
How research Strengthens HIV care and prevention in resource constraint settings: Optimization of...
28
How research Strengthens HIV care and prevention in resource constraint settings: Optimization of HIV Care Yazdan Yazdanpanah 1 , Serge Paul Eholié 2 1-Service des maladies infectieuses et tropicales, Hôpital Bichat Claude Bernard, INSERM, Atip/avenir U738, Paris 2-Service des maladies infectieuses et tropicales, Hôpital Treichville, Site PACCI- ANRS, Abidjan, Côte d’Ivoire
-
Upload
buddy-wilcox -
Category
Documents
-
view
216 -
download
0
Transcript of How research Strengthens HIV care and prevention in resource constraint settings: Optimization of...

How research Strengthens HIV care and prevention in resource
constraint settings: Optimization of HIV Care
Yazdan Yazdanpanah1, Serge Paul Eholié2
1-Service des maladies infectieuses et tropicales,Hôpital Bichat Claude Bernard, INSERM, Atip/avenir U738, Paris 2-Service des maladies infectieuses et tropicales,Hôpital Treichville, Site PACCI- ANRS, Abidjan, Côte d’Ivoire

The debate in 2000
• “Is antiretroviral therapy possible in severely resource-constrained environments?”

“Setting realistic priorities for AIDS control in less-developed countries”
“HAART •Not affordable •Poor people could not adhere: non-compliance •Health systems in poor countries could not support: erratic supplies of drugs •Not cost-effective•Spread of drug-resistant strains of HIV•Highly inequitable”
Lancet 2000
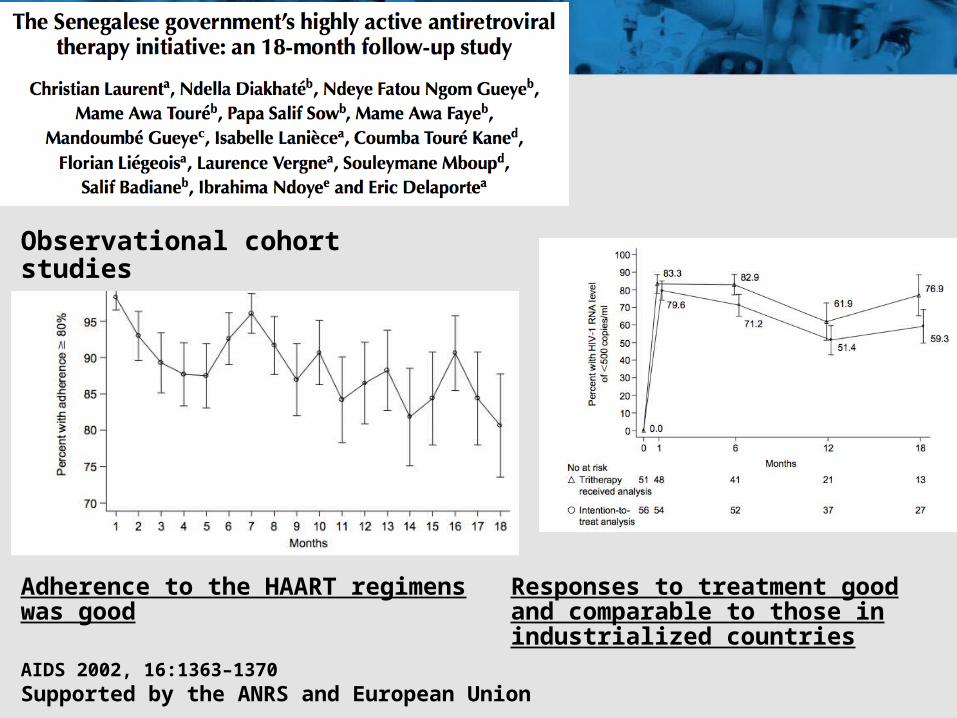
AIDS 2002, 16:1363–1370Supported by the ANRS and European Union
Observational cohort studies
Adherence to the HAART regimens was good
Responses to treatment good and comparable to those in industrialized countries

in North American Studies in African Studies
Mills EJ, JAMA 2006
Concerns about sub- optimal adherence are not supported by the data and such concerns should not contribute to delayed access to care

• The prevalence of resistant viruses = 11.8%
AIDS 2003, 17 (suppl 3):S31–S38Supported by the ANRS and European Union
Observational cohort studies

Supported the use and funding of a generic fixed-dose in developing countries
Lancet 2004; 364: 29–34

Goldie et al. N Engl J Med 2006
Supported by the ANRS, NIAID, Doris Duke Charitable Foundation
Cost-effectiveness of cART = $ 1180/YLS
< 3 x Côte d’Ivoire GDP/capita (708 $) = “cost-effective”

The Research Agenda• What to start with?• When to start?• How should we monitor ART efficacy and what criteria
for switching ART regimens?• How should we improve
– HIV testing (patients unaware of their status), – Linkage to care– Adherence interventions
• How should we avoid– Loss to follow-up– Medication stockout
While scaling-up : how best to utilize available resources?

What to start with?
PI-based regimen was not superior to NNRTI at week 96
However, NNRTI-NRTI regimen was associated with a significantly higher rate of virologic failure and higher incidence of resistance mutations
NNRTI vs. PI for HIV treatment (Low cost, FDC, tolerance vs. genetic barrier, emergence of resistance)
Clumeck et al. CROI 2012
Lubumbashi trial,

Randomised controlled trials not always ideal
• Short term evaluation vs. Long term evaluation

• In the case of two available regimens, the model inherently favored initiating with a NNRTI-based regimen and using a boosted PI-regimen subsequently.– NRTI options limited – the second PI- or NNRTI-based regimen efficacy
similar to the addition of a single drug to an already resistant NRTI backbone.
– PI monotherapy greater efficacy than NNRTI monotherapy
AIDS 2007, 21:973–982
Supported by the ANRS, NIAID, Doris Duke Charitable Foundation

d4T vs Tenofovir (cost issue)
Using tenofovir as part of first-line ART in India will improve survival, is cost-effective by international standards
Clin Infect Dis 2010 AIDS 2011

When to start?
CD4 cell count 200-350 vs. < 200 CD4 cell count 350-550 vs. < 250

Trials exploring the benefits and risks of initiating ART at very high CD4 cell counts make more sense in low-resource than in rich countries.
Clin Infect Dis 2012;54(5):714–23
Supported by the ANRS

Essai Temprano ANRS 12136 (N=2075); http://www.clinicaltrials.gov/ct2/show/NCT00495651
France, USA..., guidelines
Essai START; http://www.clinicaltrials.gov/ct2/show/NCT00867048
Ongoing trials (Temprano, START)
?
CD4 threshold to initiate ART in asymptomatic patients
WHO guidelines « for a public health approach »

Strategies to monitor ART efficacy
Lancet 2008
Archives Intern Med 2008
J AIDS 2010

19
Lancet Infect Dis 2011; 11: 825–33
13 participants (6%) in the LAB group switched to second-line regimens whereas no participants in the CLIN group did so (p<0·0001)
Supported by the ANRS

Viral load sites (South Africa, n = 18 706)
Nonviral load sites (Zambia and Malawi,
n = 80937)
Failure on 1st line but no switch
1,3% 3,7%
Switch to 2nd line therapy
9,8% 2,1%
Loss to follow up 9,2% 15,3%
Deaths 4,3% 6,3%
AIDS 2011

• Clinical trials : Substantial benefits for key outcomes favoring Biol vs. Clin
• Observational studies : more frequent switching, earlier switching, and switching at higher CD4 counts when comparing Biol vs. Clin
Low to very low-quality of evidence

Clinical Infectious Diseases 2012;54(8):1187–95

HIV care optimization
• HIV testing (patients unaware of their status)
• Linkage to care• Pre-ART loss to follow-up
Reduce the delay to start ART

AIDS 2011

• Oral supervised self-testing was highly acceptable and accurate,
Plos Med 2011
Promote HIV testing

Plos Med 2011

After the introduction of point-of-care CD4, the proportion of loss to follow-up before initiation of antiretroviral treatment fell from 64% to 33%
(OR 0·27, 95% CI 0·21-0·36)

HIV care optimization
• Adherence• Loss to follow-up
J Acquir Immune Defic Syndr 2011;56:e39–e44

• “An old African proverb states that the growth of a deep-rooted tree cannot be stopped. Our tree - representing care and support for people living with HIV in LMIC – is well rooted in existing field experience and is therefore expected to grow.”
Serge Paul Eholié


















