
How Public Health Can Appear Inside an EHR
61
How Public Health Can Appear Inside an EHR K.D. Pool, MD Terese Finitzo, PhD
-
Upload
aquila-hicks -
Category
Documents
-
view
30 -
download
0
description
How Public Health Can Appear Inside an EHR. K.D. Pool, MD Terese Finitzo, PhD. Public Health and The EHR. Why would we want to be “inside”? How could we get “inside”? Who’s in control? Why not? Now what can we do?. Forms. Why do we love them? - PowerPoint PPT Presentation
Transcript of How Public Health Can Appear Inside an EHR

How Public Health Can Appear Inside an EHRK.D. Pool, MD
Terese Finitzo, PhD

Public Health and The EHR
• Why would we want to be “inside”?
• How could we get “inside”?
• Who’s in control?
• Why not?
• Now what can we do?

Forms
• Why do we love them?
• We can create a form that gathers all of the data we need for a topic.
• We can change them.
• They meet the needs of the agency that needs data.
Forms
• Do providers love forms?
• Not so much.
• They are not fun to fill out.
• They take time away from doing whatever it is that providers do when they are not filling out forms.
EHR
• A place to record point-of-care data.
• Organized around a patient.
• Designed to make it easy to document and review data about a patient.
• They are becoming ubiquitous.
• This is where providers “work”.

Interoperability
• Send data from one system to another.
• Standardized processes so the sender and the receiver both know how to make the exchange.
• Standardized structured data so the receiver knows something about the data it receives.

Landscape
• Forms == data related to a topic that I need from the provider at the point-of-care.
• EHR == place where provider records point-of-care data.
• Interoperability == way to move data

Landscape
• So we just specify the data we need based on interoperability content standards;
• The EHR can then pull out the data and package it up and send it to us; and
• We receive the data and go do our job.

Landscape
• We get the data we need;
• Provider doesn’t have to spend time filling out a form;
• Life is good….
• So what is the hold up here?

Interoperability
• Send data from one system to another.
• Standardized processes so the sender and the receiver both know how to make the exchange.
• Standardized STRUCTURED data so the receiver knows something about the data it receives.

Structured Data
• Not all data in an EHR is structured.
• Not all data needed by public health forms is structured.
• So we can’t exchange reliably.
• SO JUST WRITE A NEW STANDARD.

Structured Data Standards
• The nuisance about standards is we have to agree on them or at the very least tell people what they are.
• Developing a new standard is not easy and not fast.
• THEN THEY HAVE TO BE IMPLEMENTED.
• And then if we need to change we start over.

Structured Data Standards
• It can take 1-2 years to develop a new standard (getting shorter).
• Current standards implementation backlog for many EHR systems is measured in years.
• Not everyone will implement our standard.
Back to the drawing board…
• Paper Forms
– Create the form
– Print and distribute it
– Fill it out
– Ship it back
– Transcribe the data

Back to the drawing board…
• Web forms
– Create the form
– Put it on our website
– Fill it out
– Form sends us the data the way we need it
Web Forms beat Paper Forms
• Deployment – saves trees (and dollars)
• Deployment – provider doesn’t have to keep a stash of forms (nor do we)
• Version–change in version is instantaneous
• Data - we don’t have to transcribe to get data
Web Forms: The dark side
• Even though a lot of the data we need is in the EHR as structured data providers have to re-enter those data into our form.
• Providers have to “go to” our website (giving them an excuse not to report).
What if?
• Could get benefits of web form AND
• Be able also get the data from the EHR that is structured AND
• Be “inside” the EHR so the provider doesn’t have to go to our web site.
• THAT IS RFD.
RFD
• Is a web form that appears “inside” the EHR
• Can be updated and deployed at will
• Can get the data for our program electronically
• Can “use” the structured data that is in the EHR.

RFD?
• Retrieve
• Form for
• Data Capture
• IHE Standard
• Originally developed by CDISC
RFD: What are the parts?
• Form Filler
• Form Manager
• Form Receiver
• Form Archiver
• Form
• User

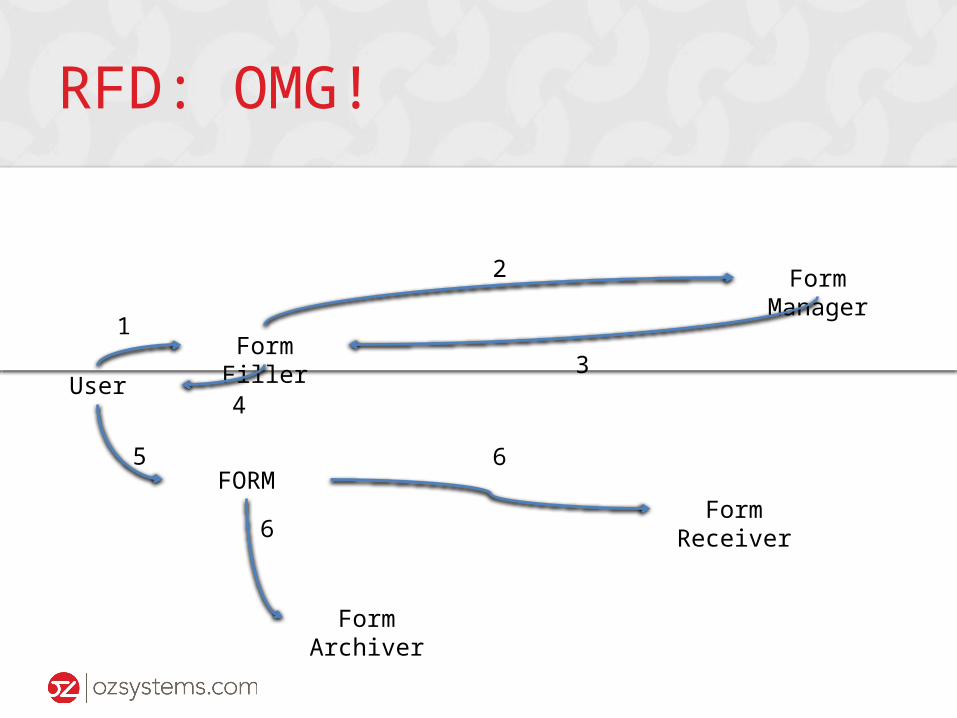
RFD: How does it work?
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
1
2
3
4
5
6
6
RFD: OMG!
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
1
2
3
4
5
6
6

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Clicks button

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Builds document with structured data

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Sends document and which form is needed
RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
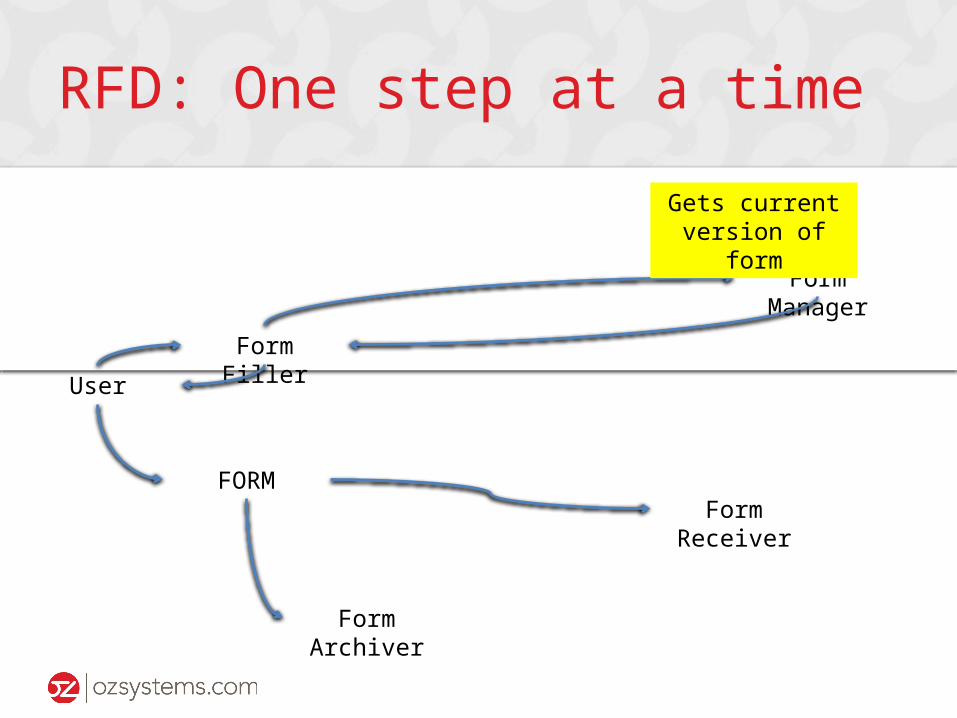
Gets current version of form

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Reads document with structured data
RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
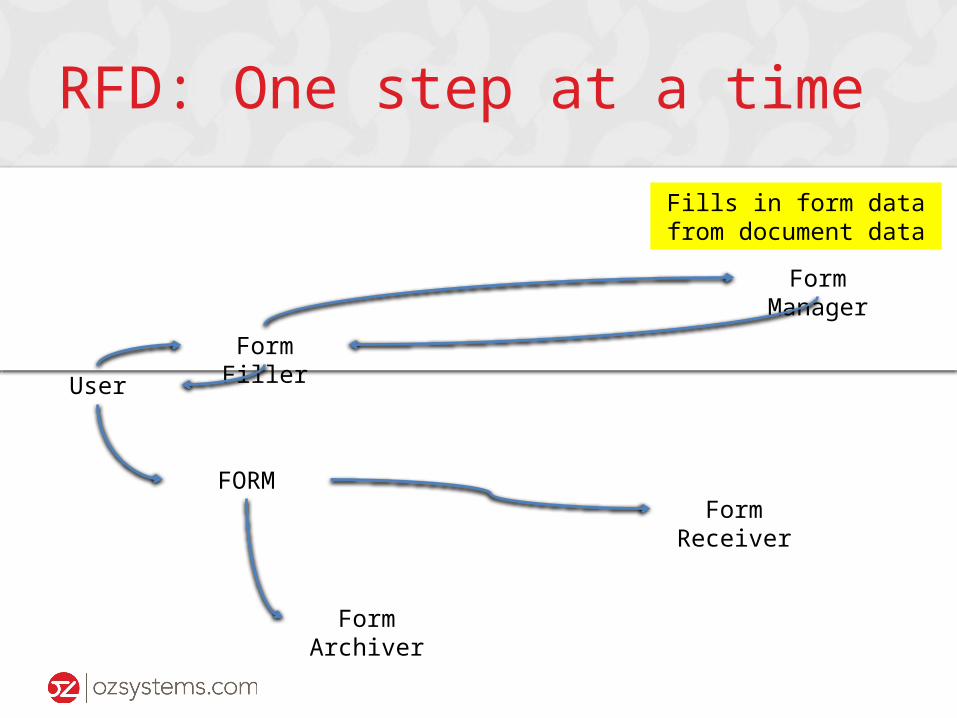
Fills in form data from document data

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Returns web form with filled in data

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Displays form for user

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Fills in remaining data

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Clicks SUBMIT

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Gets data entered and sends it to archiver

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Gets data and puts it in the archive
RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
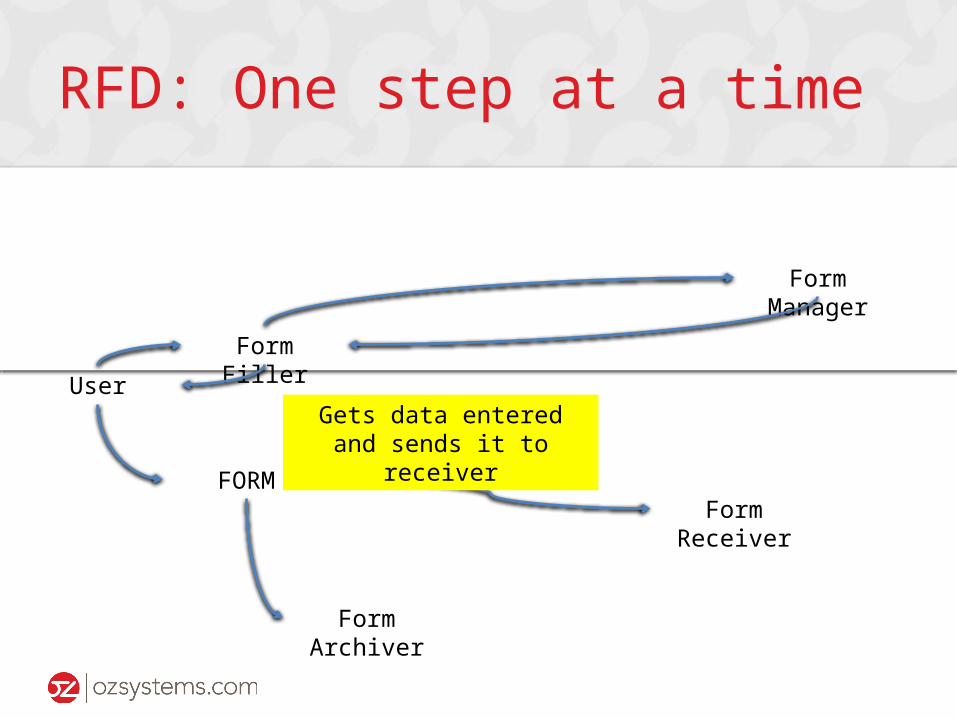
Gets data entered and sends it to receiver

RFD: One step at a time
Form Filler
Form Manager
Form Receiver
User
FORM
Form Archiver
Gets data and….
RFD: Form Filler (think EHR)
• Generates standard document with structured data (they know how to do this)
• Sends that document to Form Manager along with a request for form X (easy to implement and doesn’t matter what form is being requested).
• Display web form (think browser window)

RFD: Form Filler Key Features
• Does essentially the same thing no matter what the form is.
• Once an EHR has implemented RFD it can support virtually any form and virtually any number of forms.
• Which means when we add or change a form we don’t have to wait for the EHR to implement the change.

RFD: Form Manager
• “Brains” of the process to capture the data.
• Manages the structured data associations between the EHR data and the form data.
• “Absorbs” the impact of changes. It is built to support change.
• Virtually unlimited potential for what a smart manager might do.
RFD: Form Archiver
• Pristine place to record what was entered in the form.
• Meant to be a “read only” copy.

RFD: Form Archiver
• Smart archivers can show
–What was “pre-filled” and left untouched
–What was “pre-filled” but user changed
–What was added by the user
–What the form looked like

RFD: Form Receiver
• By standard not very impressive
• Just receives the data
• This allows it to be very flexible

RFD: Form Receiver +
• Power is in what is done next with the data
– Use the data to “build” a document
– Save the data into a repository
– Restructure the data to match what the public health system is capable of
RFD: Form Receiver +
• Can be a distributor
– Can send the data to more than one “consumer”
–Meaning multiple public health programs can each get their own copy of the data in the way they need it
– Can “batch” up data or send in real time

RFD: Who is in charge here?
• Form Authority
– This is whoever will ultimately get the data
– Controls what data are in the form
– Controls what the form looks like
– Controls what the form does
RFD: Who is in charge here?
• Form Authority
– Controls how structured data from the EHR is used to “pre-fill” the form
– Controls who gets the form data
– Controls how the form data are delivered
– DOES NOT HAVE TO BE THE MANAGER TO BE IN CONTROL

RFD: Who is in charge?
• Form Filler
– Controls what forms can be selected by the user
– Controls when forms can be selected
– Controls what data are “disclosed” to “pre-fill” the form
– Controls the use of an archive

RFD: Who is in charge?
• User
– Controls what data are entered and sent

RFD: Who is in charge?
• Form Manager
– Controls which forms are supported
– Controls which user/EHR can access what form
– Otherwise it just follows instructions
RFD: Who is in charge?
• Form Receiver
– Isn’t in control of anything
– It just follows instructions

RFD: Who is in charge?
• Form Archiver
– It protects the data
– It controls who can see the data

RFD: Why not…
• We know all too well why paper forms aren’t a great answer.
• We know that even web forms have their drawbacks.
• We have already explored why we cannot JUST rely on EHRs generating documents with all of the data we need YET.
RFD: Why not…
• Just build the forms into the EHR?
• Sheer numbers makes this impractical
– Number of topics that there are or might be forms for
– Number of local, state, and federal variations
– Number of different EHR systems
• Cannot rely on this until all EHRs build them
• Changes will not be instantaneous or synchronized

RFD: Why not…
• Just let the EHR pre-fill the form?
• There is nothing to preclude this.
• However, pre-filling is a type of “coupling” and that makes the system less fluid and able to accommodate change.
• It makes us dependent on development priorities of EHR vendors.
• No EHR vendor currently supports this.

So what can we do with this?
• Virtually any reporting form especially if the report is about a patient.
– Reportable conditions
– Case reports
– Follow-up reports

So what can we do with this?
• Vital Records
• Program specific data
– EHDI, CCHD
–Metabolic specimen card data
– HIV/AIDS
– Immunization

So what can we do with this?
• Adverse event reporting
• Patient safety reporting
• Quality measures reporting

So else what can we do?
• Other than public health
– Clinical research forms
– Payer/claims forms
– Augment EHRs

RFD: Use with caution
• Since RFD forms are easier to access you will get more data.
• Since RFD forms take less time to complete you will get more data.
• Since RFD forms are “in” the EHR you will get data more timely.

Questions?
K.D. Pool, MD
Terese Finitzo, PhD


















