How different surgical methods of performing right upper lobectomy contribute to postoperative...
4
Surg Today Jpn J Surg (1999) 29:610–613 bifurcation consisting of the RUL bronchus (RULB) and intermediate bronchus (IB). The bronchial stump is closed at the incised orifice with string sutures (Fig. 1A). Lobectomies may now be performed with video- assisted thoracotomy, following which the bronchus is often closed with a mechanical stapler. 1 When the orifice of the RULB is closed with a stapler, the an- astomotic line is two or three rings distal from the bifurcation due to the width of the stapler (Fig. 1B). Postoperative bronchofiberscopic examination usually reveals a pocket formation at the closed stump (Fig. 2B); however, when the stump is closed by hand suturing, this pocket formation rarely occurs (Fig. 2A). In recent years, other bronchoplastic procedures, including sleeve and wedge lobectomy, have achieved prominence in the treatment of lung diseases. 2,3 Following RU lobectomy, the right thoracic space becomes filled by the displacement and distortion of the remaining right middle lobe (RML) and the right lower lobe (RlL); therefore, some bending and rotation of the RML bronchus (RMLB) is a common postoperative phenomenon. 4 The present study was conducted to determine whether various surgical methods used in RU lobectomy, such as closure by hand suturing versus mechanical stapling, and wedge or sleeve broncho- plasty, affect the degree of postoperative bronchial de- formity. If so, the root cause would be associated with variations in the postoperative length of the stump of the RULB. We also evaluated the relationship between various surgical methods and postoperative bronchial deformity using an in situ bronchial casting model in rabbits. 5 Materials and Methods All animals received humane care in compliance with the Principles of Laboratory Animal Care formulated Reprint requests to: M. Nonaka Presented at the 97th Annual Meeting of the Japan Surgical Society, held in Kyoto, Japan, April 9–11, 1997 (Received for publication on Apr. 13, 1998; accepted on Nov. 6, 1998) How Different Surgical Methods of Performing Right Upper Lobectomy Contribute to Postoperative Bronchial Branching Deformity: An Experimental Study Makoto Nonaka, Mitsutaka Kadokura, Tetsuro Michihata, Koichi Inoue, and Toshihiro Takaba First Department of Surgery, Showa University School of Medicine, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo 142-8666, Japan Abstract: It has been suggested that postoperative bronchial deformity is a complication of surgery and that the surgical methods employed may play a role in its development. We studied the relationship between postoperative bronchial branching deformity and various surgical methods, including hand suturing or mechanical stapling of right upper (RU) lobectomy, versus wedge or sleeve bronchoplasty with RU lobectomy. We used an in situ bronchial casting model in rabbits and measured the branching angles between: the tra- chea and the right main bronchus (RMB); the trachea and the left main bronchus; the RMB and the intermediate bronchus (IB); the IB and the right middle lobe bronchus (RMLB); and the RMLB and the coronal plane. In the mechanical stapling group, the angle between the RMB and the IB was wider than in the hand suturing group, and the RMLB diverged more laterally. In the wedge plasty group, the angle between the trachea and the RMB was wider, while that between the IB and the RMLB was narrower than in the hand suturing group. In the sleeve plasty group, the angle between the RMB and the IB and that between the IB and the RMLB were wider than in the hand suturing group. The findings of this experiment clearly demonstrate that postoperative deformity of the distal bronchus varies according to the surgical methods used. Key Words: right upper lobectomy, bronchoplasty, sleeve lobectomy, wedge lobectomy, mechanical stapling Introduction In the case of right upper (RU) lobectomy, the RU lobe (RUL) of the bronchus is incised at the level of the
-
Upload
makoto-nonaka -
Category
Documents
-
view
214 -
download
0
Transcript of How different surgical methods of performing right upper lobectomy contribute to postoperative...

610 M. Nonaka et al.: Right Upper Lobectomy and Bronchial DeformitySurg TodayJpn J Surg (1999) 29:610–613
bifurcation consisting of the RUL bronchus (RULB)and intermediate bronchus (IB). The bronchial stump isclosed at the incised orifice with string sutures (Fig. 1A).Lobectomies may now be performed with video-assisted thoracotomy, following which the bronchus isoften closed with a mechanical stapler.1 When theorifice of the RULB is closed with a stapler, the an-astomotic line is two or three rings distal from thebifurcation due to the width of the stapler (Fig.1B). Postoperative bronchofiberscopic examinationusually reveals a pocket formation at the closedstump (Fig. 2B); however, when the stump is closed byhand suturing, this pocket formation rarely occurs(Fig. 2A). In recent years, other bronchoplasticprocedures, including sleeve and wedge lobectomy,have achieved prominence in the treatment of lungdiseases.2,3
Following RU lobectomy, the right thoracic spacebecomes filled by the displacement and distortion of theremaining right middle lobe (RML) and the right lowerlobe (RlL); therefore, some bending and rotation of theRML bronchus (RMLB) is a common postoperativephenomenon.4 The present study was conducted todetermine whether various surgical methods used inRU lobectomy, such as closure by hand suturing versusmechanical stapling, and wedge or sleeve broncho-plasty, affect the degree of postoperative bronchial de-formity. If so, the root cause would be associated withvariations in the postoperative length of the stump ofthe RULB. We also evaluated the relationship betweenvarious surgical methods and postoperative bronchialdeformity using an in situ bronchial casting model inrabbits.5
Materials and Methods
All animals received humane care in compliance withthe Principles of Laboratory Animal Care formulated
Reprint requests to: M. NonakaPresented at the 97th Annual Meeting of the Japan SurgicalSociety, held in Kyoto, Japan, April 9–11, 1997(Received for publication on Apr. 13, 1998; accepted onNov. 6, 1998)
How Different Surgical Methods of Performing Right UpperLobectomy Contribute to Postoperative Bronchial BranchingDeformity: An Experimental Study
Makoto Nonaka, Mitsutaka Kadokura, Tetsuro Michihata, Koichi Inoue, and Toshihiro Takaba
First Department of Surgery, Showa University School of Medicine, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo 142-8666, Japan
Abstract: It has been suggested that postoperative bronchialdeformity is a complication of surgery and that the surgicalmethods employed may play a role in its development. Westudied the relationship between postoperative bronchialbranching deformity and various surgical methods, includinghand suturing or mechanical stapling of right upper (RU)lobectomy, versus wedge or sleeve bronchoplasty with RUlobectomy. We used an in situ bronchial casting model inrabbits and measured the branching angles between: the tra-chea and the right main bronchus (RMB); the trachea and theleft main bronchus; the RMB and the intermediate bronchus(IB); the IB and the right middle lobe bronchus (RMLB); andthe RMLB and the coronal plane. In the mechanical staplinggroup, the angle between the RMB and the IB was widerthan in the hand suturing group, and the RMLB divergedmore laterally. In the wedge plasty group, the angle betweenthe trachea and the RMB was wider, while that between theIB and the RMLB was narrower than in the hand suturinggroup. In the sleeve plasty group, the angle between the RMBand the IB and that between the IB and the RMLB werewider than in the hand suturing group. The findings of thisexperiment clearly demonstrate that postoperative deformityof the distal bronchus varies according to the surgical methodsused.
Key Words: right upper lobectomy, bronchoplasty, sleevelobectomy, wedge lobectomy, mechanical stapling
Introduction
In the case of right upper (RU) lobectomy, the RU lobe(RUL) of the bronchus is incised at the level of the

611M. Nonaka et al.: Right Upper Lobectomy and Bronchial Deformity
by the National Society for Medical Research, and theGuide for the Care and Use of Laboratory Animalsprepared by the Institute of Laboratory AnimalResources and published by the National Institutes ofHealth (NIH publication no. 86-23, revised 1985).
A total of 40 New Zealand white rabbits weighingfrom 2.0 to 3.0 kg, with a mean weight of 2.3kg, wereused. All the animals were anesthetized and euthanizedwith sodium pentobarbital. After the animals had beenplaced in the left lateral position, a standard posterolat-eral thoracotomy was performed through the inter-costal muscle of the fifth intercostal space, and the rightchest wall was opened.
These rabbits were divided into four groups of tenrabbits each (Fig. 3). Group 1 was a hand suturingmodel in which the RULB was incised at the level of thebifurcation consisting of the RULB and IB, followingby closure of the stump at the incised orifice with 6-0monofilament sutures. Group 2 was a mechanical sta-pling model in which the RULB was incised three ringsdistal from the bifurcation consisting of the RULB andIB followed by closure of the stump at the incised end.Group 3 was a wedge bronchoplasty with lobectomy ofthe RUL model in which half of the right main bronchus(RMB) circumference was resected. Group 4 was a RUlobectomy with a sleeve resection model in which theproximal bronchotomy was made one ring distal formthe carina, while the distal incision was made one ringproximal from the bifurcation consisting of the RMLBand RLL bronchus (RLLB), followed by bronchoplastyperformed with an end-to-end anastomosis. In all fourgroups, the bronchial anastomosis was subsequentlychecked for airtightness. A chest tube was inserted intothe thoracic cavity and the chest was closed layer tolayer.
A tracheotomy was performed, and casting material,in the form of methacrylate resin, 7ml/kg, was intro-duced into the airway. The lung-heart bloc was removedthrough a sternotomy and floated in a solution of potas-sium hydroxide for tissue digestion. The branchingangles between the trachea and the RMB (a°), the tra-chea and the left main bronchus (LMB) (b°), the RMBand the IB (c°), the IB and the RMLB (d°), and theRMLB and the coronal plane (e°) were measured usingthe bronchial casts as previously described.5
All results are presented as the mean 6 standarderror of the mean. Differences in means between stratawere tested by Student’s unpaired t-analysis. For a dif-ference to be significant, the error probability wasrequired to be 0.05 or less.
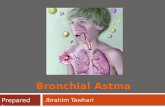
Fig. 2A,B. Bronchofiberscopic find-ings at the closed stump followingright upper lobectomy with A handsuturing and B mechanical stapling,in humans. A pocket formation at theclosed stump can be seen in B, butnot in A
Fig. 1. Methods of closure by hand suturig (A) and mechani-cal stapling (B) after right upper lobectomy. With mechanicalstapling, the anastomotic line is made two or three rings distalfrom the bifurcation due to the width of the stapler. RMB,right main bronchus; RULB, right upper lobe bronchus; IB,intermediate bronchus

612 M. Nonaka et al.: Right Upper Lobectomy and Bronchial Deformity
Discussion
After RU lobectomy, some bending and rotation of theRMLB, which is usually narrow and long, is common.As bronchial secretions can cause atelectasis of theRML, bronchial suctioning may be necessary during theearly postoperative period after RU lobectomy. Someauthors have reported early postoperative complica-tions, such as atelectasis and pneumonia,6 which may becaused by preoperative respiratory dysfunction, dimi-nution of pulmonary arterial perfusion, postoperativewound pain, and granulation of the anastomotic site.6–8
We speculate that these complications are partlyattributable to the postoperative bronchial deformityand suggest that the methods of bronchial closure orbronchoplasty have a significant impact on the degree ofthis deformity. Others have reported that the length ofthe remaining closed stump may affect the postopera-tive deformity of the distal bronchus, but no one hasstudied the relationship between the surgical methodsof performing RU lobectomy and the postoperativebranching angles.
In our mechanical stapling model, the anastomoticline was three rings distal from the bifurcation involvingthe RULB and the IB, and the angle between the RMBand the IB (c°) was wider than that in the hand suturingmodel. Although we had speculated that the straight-ened angle between the RMB and the IB (c°) wouldcause a sharpened angle between the IB and the RMLB(d°), we found that the angle between the IB and theRMLB (d°) did not differ in the mechanical stapling andhand suturing models. On the other hand, the RMLBdiverged more laterally in the mechanical staplingmodel than in the hand suturing model. Therefore, if apatient has a weakened bronchial wall, caused by adisorder such as bronchial malasia, or a narrow RMLbronchial pedicle, this lateral divergence will result inthe orifice of the RMLB becoming stenotic, due torotation of the RMB and IB.
In the case of wedge bronchoplasty, it was speculatedthat the sharpened angle between the RMB and the IB
Results
The branching angles are shown in Table 1. In group 2,the angle between the RMB and the IB (c°) was wider(P , 0.01), while that between the RMLB and thecoronal plane (e°) was narrower (P , 0.01) than ingroup 1. The angles between the IB and the RMLB (d°)were not significantly different between groups 1 and 2.In group 3, the angle between the trachea and the RMB(a°) was wider (P , 0.01), while that between the IBand the RMLB (d°) was narrower (P , 0.05) than ingroup 1. A fold formation on the opposite side of theanastomosis between the RMB and IB after wedge RUlobectomy was observed in four of the group 3 lungs. Ingroup 4, the angle between the trachea and the RMB(a°) was narrower (P , 0.01) than in group 1, while thatbetween the RMB and the IB (c°), and that between theIB and the RMLB (d°) were wider (P , 0.01) than ingroup 1.
Fig. 3. Variations in the operative methods of performingright upper lobectomy
Table 1. Branching angles in the four groups
Angle
Group a° b° c° d° e°
1 170° 6 2° 140° 6 2° 143° 6 1° 104° 6 3° 58° 6 3°2 163° 6 3° 146° 6 2° 178° 6 1° 109° 6 4° 34° 6 3°3 192° 6 1° 147° 6 3° 157° 6 6° 90° 6 5° 50° 6 7°4 150° 6 7° 136° 6 8° 180° 6 0° 124° 6 10° 56° 6 21°
Values are expressed as means 6 SEM. Branching angles between: a°, the trachea and the rightmain bronchus (RMB); b°, the trachea and the left main bronchus; c°, the RMB and the interme-diate bronchus (IB); d°, the IB and the right middle lobe bronchus (RMLB); e°, the RMLB andthe coronal plane

613M. Nonaka et al.: Right Upper Lobectomy and Bronchial Deformity
Fig. 4. Clinical bronchofiberscopic findings in a patient whohad undergone wedge bronchoplasty with right upperlobectomy. A fold formation (F ) on the opposite side of theanastomosis (A) can be seen
the bronchus will affect the postoperative bronchialbranching deformity.
In conclusion, the results of the present experimentindicate that in the case of RU lobectomy, if the excisedand closed RULB is left longer than usual, the anglebetween the RMB and the IB (c°) will widen andthe RMLB will diverge more laterally. When wedgebronchoplasty is performed, the angle between thetrachea and the RMB (a°) is wider, and the RMLB isangled in a more upward direction than following stan-dard lobectomy. When sleeve resection is performed,the angle between the RMB and the IB is wider, but theangulation of the RMLB widens because of the cylindri-cal form of bronchial resection. It has been suggestedthat postoperative bronchial deformities may causeclinical complications, and the results of this experimentclearly demonstrate how different surgical methodsmay affect postoperative deformities of the distal bron-chus.
Acknowledgments. The authors thank Mr. Nobukazu Nishinoand Ms. Miki Taki for their technical assistance, and Ms. MisaIzumikawa for her secretarial assistance.
References
1. Takaro T (1987) Use of staplers in bronchial closure. In: Grillo HC,Eschapasse H (eds) Major challenges. Saunders, Philadelphia,pp 452–457
2. Khargi K, Duurkens VAM, Versteegh MMI, Huysmans HA,Quanjer PH, Verzijlbergen FF, Velde EA, Knaepen PJ (1996)Pulmonary function and postoperative complications after wedgeand flap reconstructions of the main bronchus. J ThoracCardiovasc Surg 112:117–123
3. Gaisser HA, Mathisen DJ, Moncure AC, Hilgenberg AD, GrilloHC, Wain JC (1996) Survival and function after sleeve lobectomyfor lung cancer. J Thorac Cardiovasc Surg 111:948–953
4. Wallace JE, Pillman R (1956) Bronchographic studies after resec-tion for pulmonary tuberculosis. Thorax 11:149–159
5. Nonaka M, Kadokura M, Tanio N, Yamamoto S, Kataoka D,Inoue K, Takaba T (1998) Changes in lung lobar volume andbronchial deformity after right upper lobectomy. Surg Today28:285–288
6. Brooks JW (1979) Complications following pulmonary lobectomy.In: Cordell AR, Ellison RG (eds) Complications of intrathoracicsurgery. Little Brown, Boston, pp 235–245
7. Kirsh MM, Rotman H, Behrindt DM, Orringer MB, Sloan H(1975) Complications of pulmonary resection. Ann Thorac Surg20:215–236
8. Bueno R, Wain JC, Wright CD, Moncure AC, Grillo HC, MathisenDJ (1996) Bronchoplasty in the management of low grade airwayneoplasms and benign bronchial stenosis. Ann Thorac Surg62:824–829
(c°) might cause a widening of the angle between the IBand the RMLB (d°); however, our experiment revealedthat the tension along the anastomotic site made “folds”on the opposite side of the anastomosis in the RMB andIB. Due to these folds, the angles between the RMB andthe IB (c°) did not differ in the wedge bronchoplastygroup and the hand suturing group. In fact, the forcedtension along the anastomotic site made the anglebetween the trachea and the RMB (a°) wider and thatbetween the IB and the RMLB (d°) narrower. Underthese conditions, bending or compression of the RMLBwould occur easily. Clinically, we encountered a patientwho developed a fold formation on the opposite side ofthe anastomosis in the RMB and IB following a wedgeRU lobectomy (Fig. 4). The incised width and lengthmay affect the postoperative deformity following thewedge resection.
In the sleeve bronchoplasty model, the angle betweenthe IB and the RMLB (d°) was wider than that in thehand suturing model. Sleeve resection may be the mostrecommended method of surgery for avoiding stenosisor obstruction of the RMLB due to bending at theorifice after RU lobectomy. In our experiment, bron-chial incision and anastomosis were performed acrossthe longitudinal axis of the remnant bronchus. Anyalternation in the angle between the incised plane and