House&Staff&Orientaon& - Northwell Health Medical... · House&Staff&Orientaon&...
23
House Staff Orienta/on Department of Pharmacy Raisa Telis, PharmD Nicholas Zerilli, PharmD Paul Nowierski, Director of Pharmacy Lenox Hill Hospital Department of Pharmacy June 21, 2013
Transcript of House&Staff&Orientaon& - Northwell Health Medical... · House&Staff&Orientaon&...

House Staff Orienta/on Department of Pharmacy
Raisa Telis, PharmD Nicholas Zerilli, PharmD
Paul Nowierski, Director of Pharmacy
Lenox Hill Hospital Department of Pharmacy
June 21, 2013

2
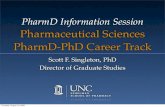
Director of Pharmacy Paul T. Nowierski
Manager, Pharmacy IT C. Emerson – PharmD
Assistant Director of Pharmacy I. Usherenko, PharmD
Pharmacy Supervisor A.Krasnoff, PharmD
Pharmacists Pharmacy Assistants Messengers Pharmacy
Interns
Advanced PracQce Clinical Pharmacists
J. Slavin PharmD
N. Zerilli PharmD
R. Telis PharmD
Manager, Purchasing M. Wozny -‐ Non RPh Manager-‐ Oncology
K. Bui, PharmD
Assistant Director of Pharmacy (64th Street) K. Talisman , PharmD
ExecuQve Assistant
Pharmacy Supervisor E. Gyuratz, PharmD
L. Nisanyan PharmD
Pharmacy Residents: Atrik Aryan & Anya Yudchyts

Pharmacy Phone Numbers • Inpa/ent Pharmacy Department (IPD) § 4-‐3226, 4-‐5731, 4-‐5730
• IV Room: 4-‐5507 • TPN: 4-‐5383 • Chemotherapy: 4-‐3181
§ Kenny Bui, PharmD • IT: 4-‐3261
§ Chris Emerson, PharmD § Pager: (917) 356-‐1247
Clinical Pharmacists • Julia Slavin, PharmD
§ 4-‐2530 § Pager: (917) 845-‐4337
• Raisa Telis, PharmD § 4-‐3185 § Pager: (917) 871-‐0003
• Nicholas Zerilli, PharmD § 4-‐2192 § Pager: (917) 785-‐7505
• Lori Nisanyan, PharmD § 4-‐3183 § Pager: (917) 205-‐8047
3

Pharmacy Residency Program
• Goal: develop a pharmacist into a more highly trained, competent, and confident health system prac//oner
• Two pharmacy residents: one year program consis/ng of core rota/ons
• Rota/ons include internal medicine, cardiology, medical & neonatal intensive care, emergency medicine, infec/ous disease, informa/cs, an/coagula/on, & administra/on
• Precepted by Clinical Pharmacists-‐Advanced Prac/ce • Work with members of an inter-‐disciplinary team to achieve op/mal pa/ent outcomes
4

College of Pharmacy Affilia/on Arnold & Marie Schwartz College of Pharmacy -‐
Long Island University § Pharmacists precept pharmacy students for various types of experiences
§ Medical residents are asked to take pharmacy students on their medicine teams
§ No more than 1 pharmacy student will be assigned to each medicine team
§ Students are here for 5 week rota/ons
5

College of Pharmacy Affilia/on • Your responsibili/es:
§ Let the students know when and where rounds are or how you can be reached to join the team
§ Provide the students with the names of the pa/ents that the team is following
• Pharmacy students: § Make recommenda/ons to op/mize a pa/ent’s drug therapy
§ Serve as a resource for drug informa/on ques/ons
§ Can perform discharge counseling if needed
6

LHH Formulary • Formulary: list of approved medica/ons that are regularly
stocked and available for use at the hospital
• The formulary is reviewed and updated by the Pharmacy & Therapeu/cs Commigee (P&T) on a con/nual basis
• Only drugs approved by P&T shall be used in the treatment of pa/ents with the following excep/ons:
– The appropriate non-‐formulary process has been completed (policy discussed later)
– The pa/ent provides their own medica/on (policy discussed later)
– The drugs have been approved for clinical inves/ga/ons at LHH
7

Non-‐Formulary Drug Policy • Non-‐formulary: medica/ons that are not on the LHH formulary and are
not rou/nely stocked by the pharmacy
• An item’s LHH formulary status can be viewed online through Lexi-‐Comp Online (icon available on desktop of all computers)
– Search for drug
– On leh side under “Lenox Hill Hospital,” it will indicate status
– If it states “No occurrences,” it is a non-‐formulary agent
– If it states “item name” [RESTRICTED], the agent has restric/ons
– If it states “item name,” the item is formulary with no restric/ons
• Prior to reques/ng a non-‐formulary agent, consider other formulary alterna/ves in the same therapeu/c class
8

Reques/ng a Non-‐Formulary Agent • Most non-‐formulary items CANNOT be entered into the CPOE
(Computerized Prescriber Order Entry) system by prescribers and pharmacy must be contacted to order these items
• To place an order for a non-‐formulary item: • Call pharmacy (4-‐3226)
• No/fy the pharmacist which drug you are reques/ng and the reason for using the non-‐formulary agent
• The pharmacist and pharmacy supervisor or clinical pharmacist will review the request
• If approved, receipt of non-‐formulary items can take up to 72 hours
• If a delay is an/cipated beyond 72 hours, the physician and nurse will be no/fied
9

An/microbial Stewardship • Purpose
– To prevent the development of resistant organisms, control drug cost, and to prevent the indiscriminate use of an/microbial agents when alternate treatments are formulary based
• Formulary Unrestricted
– Agents generally available to all members of the medical staff to order for the prophylaxis and treatment of infec/ous diseases
• Formulary with Guidelines
– Require approval by a Clinical Pharmacist or an Infec/ous Disease (ID) Physician if used outside of the approved guidelines for use
– Approved indica/ons for use are part of a pull-‐down menu during the order entry process
10

An/microbial Stewardship • Formulary Restricted to Infec/ous Diseases Physicians
– An/microbial agents that can only be ordered directly by an ID physician
– Stocked by the pharmacy
• Non-‐Formulary An/microbials – Designated as any other an/microbial agent available in the United
States but not on formulary
– These agents will NOT be stocked by the pharmacy and would require special ordering that may delay treatment
– Please contact the Infec/ous Disease Agending on-‐call
11

An/bio/cs -‐ Formulary Unrestricted • Amphotericin B • Ampicillin Inj & Caps &
Suspension • Amoxicillin Caps &
Suspension • Azithromycin Tabs &
Suspension • Cefaclor Suspension • Cefazolin Inj • Cefuroxime Tabs • Cehriaxone Inj • Cephalexin Caps &
Suspension • Ciprofloxacin Tabs • Clarithromycin Tabs &
Suspension • Clindamycin Inj & Caps
• Dapsone Tabs • Dicloxacillin Caps &
Suspension • Doxycycline Inj & Tabs • Erythromycin Inj & Tabs &
Suspension • Fluconazole Tabs • Gentamicin Inj • Itraconazole Inj & Caps &
Solu/on • Kanamycin Inj • Ketoconazole Tablet • Levofloxacin Tabs • Metronidazole Tabs • Nafcillin Inj • Neomycin Tabs • Nitrofurantoin Caps &
suspension • Oxacillin Inj • Paromomycin Caps • Penicillin G Procaine Inj • Penicillin G Benzathine Inj • Penicillin G Sodium Inj • Penicillin VK Tabs &
Suspension • Pentamidine Inj • Piperacillin Inj • Sulfadiazine Tabs • Tetracycline Tabs • Trimethoprim/
Sulfamethoxazole Inj & Tabs & Suspension
• Tobramycin Inj
12

An/bio/cs -‐ Formulary With Guidelines • Amikacin • Amoxicillin/clavulanate • Ampicillin/sulbactam • Azithromycin Inj • Aztreonam • Cefixime • Cefotaxime • Cehazidime • Ciprofloxacin Inj • Dalfopris/n-‐quinupris/n Inj • Daptomycin • Fluconazole Inj • Imipenem-‐cilasta/n Inj • Levofloxacin Inj
• Linezolid Inj/PO • Metronidazole Inj • Piperacillin/tazobactam • Polymyxin B Joint solu/on • Vancomycin Inj • Vancomycin oral suspension
13

An/bio/cs -‐ Restricted • Amphotericin B Liposomal Inj (Ambisome & Abelcet) • Caspofungin Inj • Chloramphenicol Sodium Inj • Doripenem Inj • Meropenem Inj • Moxifloxacin Inj & Tablet • Polymyxin B Inj • Posaconazole Suspension • Rifaximin Tablet • Streptomycin Inj • Ticarcillin/Clavulanate Inj • Tigecycline Inj • Tobramycin Nebulizer Solu/on • Voriconazole Inj and Tablet
14

An/coagula/on • An/coagulants are considered “High-‐Alert Medica/ons” due
to the risk of pa/ent harm when used inappropriately • LHH has developed policies and procedures for the safe use of
these medica/ons.
– On every desktop:
HealthPort à Policies à LHH à Medica/on Management
– Unfrac/onated heparin, enoxaparin, direct thrombin inhibitors (IV and po), and warfarin
• Clearly specifying indica/on for use, therapeu/c goals, and appropriate documenta/on is essen/al for providing safe and effec/ve therapy.
15

Pa/ent’s Own Medica/ons • When a pa/ent arrives at LHH with their own medica/on,
the nurse will reconcile the medica/ons presented.
• The physician will determine the medica/ons that the pa/ent will con/nue while hospitalized.
• If a medica/on is available at LHH, the pa/ent is not permiged to use his/her own medica/on, including nutri/onal supplements and herbal products.
• The pa/ent’s own medica/ons should be returned to the family or guardian whenever possible.
16

Pa/ent Own Medica/ons • In the situa/on where the medica/on(s) is/are not available from the
Pharmacy, the pa/ent may take his/her own medica/on(s) – Appropriate instances include:
• Oral contracep/ves • Inves/ga/onal drugs and/or • Non-‐formulary medica/ons not rou/nely stocked by LHH Pharmacy
– The pa/ent’s own medica/on must be sent to the pharmacy department to be iden/fied, labeled, and returned to the nursing unit.
– Pharmacy will only verify medica/ons in either the original labeled container or prescrip/on bogle. Unlabeled medica/ons (i.e. loose medica/ons in pill boxes) will not be accepted.
– Remaining medica/on must be returned to the pa/ent upon discharge. • In the event the pa/ent’s medica/on is a controlled substance, the
medica/on will be assigned a drawer in the Omnicell by Pharmacy.
17

Automa/c Stop Order Policy • Orders placed for medica/ons will be reviewed and renewed if
needed based on the following automa/c stop order dates approved by the Medical Board:
– Enoxaparin (Cardiac indica/on) – 72 hours
– Enoxaparin (Non-‐cardiac indica/on) – 7 days
– Hypertonic Saline (NaCl 3%) – up to 24 hours as specified
– Potassium Chloride IV large volume – up to 24 hours as specified
– Potassium Chloride riders – up to 3 riders as specified
– An/bio/cs -‐ 7 days
18

Automa/c Stop Order Policy
• IVs – up to midnight of the following day – Excep/ons Include:
• An/bio/cs • Oncology regimens defined by prac//oner
• Cor/costeroid regimens defined by prac//oner
• An/convulsants • Pa/ent Controlled Analgesia (PCA) as defined by prac//oner • When risk of discon/nua/on jeopardizes pa/ent care
• Total Parenteral Nutri/on (TPN) – up to 24 hours
19

Automa/c Stop Order • Controlled substances – up to 7 days (24 hours if IV drip)
– At no /me can dosage ranges or mul/ple routes of administra/on be wrigen (i.e. Percocet-‐5, 1 -‐ 2 tablets po q4h prn pain OR fentanyl 25 mcg IM x 1 [give IV] )
– If an order is wrigen for prn use, the reason for administra/on must be specified.
– If a PRN order does not contain specific administra/on /mes or frequency, i.e. morphine sulfate 8 mg IM PRN Severe pain, the drug may be administered only ONCE and the order is valid for only 72 hours
– The use of “renew”, “con/nue”, “repeat”, or “PRN” without a designated dose and frequency is unacceptable
• All other medica/ons will have an automa/c stop requiring re-‐order aher 60 days
• The physician is responsible for reviewing medica/ons and determining if the medica/on(s) is to be renewed, changed, or discon/nued. If the physician does not reorder drugs designated for automa/c stop, they will be dropped out of the system at the specified /me
20

IV to PO Automa/c Conversion • The following agents will be automa/cally converted from IV
to PO form by a Clinical Pharmacist-‐Advanced Prac/ce if criteria set forth by the P&T are met. – Famo/dine – Esomeprazole – Ciprofloxacin – Levofloxacin – Fluconazole – Voriconazole – Metronidazole – Linezolid
21

Epoe/n Alfa Usage Criteria • As per P&T and Medical Board, the use of Erythropoie/n S/mula/ng
Agents will meet certain criteria in terms of upper limit of Hgb related to indica/on for use. All orders for erythropoie/n will be discon/nued by a pharmacist if Hgb is > 11 mg/dL except where noted below.*
• Indica/on and Hgb value are required for ordering. – Treatment of anemia related to chronic renal failure in dialysis pa/ents – Treatment of anemia related to chronic renal failure in non dialysis pa/ents
– Treatment of anemia related to HIV (zidovudine) therapy
– Treatment of anemic pa/ents scheduled to undergo elec/ve, noncardiac, nonvascular surgery to reduce the need for allogeneic blood transfusion
– Treatment of anemia related to an/neoplas/c therapy
– *Other non FDA-‐approved indica/on: Hgb < 10 mg/dL
22

Ques/ons?
23