Hospital Medicine Pearls, VA ACP Meeting 2014
87
Best Papers in 2013: Hospital Medicine Edition Jon Sweet, MD, FACP Carilion Clinic & Virginia Tech Carilion School of Medicine
-
Upload
jon-sweet -
Category
Healthcare
-
view
92 -
download
2
Transcript of Hospital Medicine Pearls, VA ACP Meeting 2014

Best Papers in 2013:Hospital Medicine Edition
Jon Sweet, MD, FACPCarilion Clinic &
Virginia Tech Carilion School of Medicine
Objectives
• Analyze recent studies regarding rational transfusion strategies in different patient populations
• Appraise the recent literature regarding common inpatient situations (e.g., hepatic encephalopathy, severe alcoholic hepatitis, penicillin allergy)
• Apply recent evidence to the care of patients with acute ischemic stroke
• Disclosures: none

Case 1
• 67 yo man admitted withnon-purulent leg cellulitisrefractory to outpatientmanagement.
• Improving with cefazolin IV but SBP consistently in the 160 range (similar to outpatient measurements). Periumbilical and femoral bruits are present.
• Meds: chlorthalidone 25 mg, lisinopril 20 mg, carvedilol 25 mg BID.
• Cr stable at 2.1, K 5.1• Renal artery duplex suggest a high-grade proximal
stenosis of the right• What is the next best step?

What is the next best step?
A. Do nothing
B. Add amlodipine
C. Add spironolactone
D. Increase lisinopril
E. Renal artery stenting


CORAL Trial• Third large trial showing no benefit patients with RAS
– ASTRAL– STAR
• N = 947– Resistant hypertension or CKD stage ≥3– Atherosclerotic RAS (mean stenosis, 73%)– Median follow-up 43 months
• Optimal medical therapy alone versus optimal medical therapy with stenting
• No difference in any endpoint– Composite of death from cardiovascular or renal causes– AMI, stroke, heart failure– Renal insufficiency or need for permanent renal replacement therapy
• Secondary analysis– No benefit among patients with >80% stenosis

Pearl #1
• For patients with atherosclerotic RAS, don’t stent the beans.
Case 2
• 65 yo woman with very severe COPD (FEV1 28%) admitted to a telemetry unit for a COPD exacerbation for the 4rd time in 12 months. She continues to smoke 1 ppd. She endorses increasing URI symptoms for the past 3 days. Last hospitalization 2 months (7 days)
• Temp 98.9, BP 160/80, HR 112, RR 32. She is in moderate respiratory distress but can converse. Diffuse wheezes with markedly prolonged expiratory phase.
• pH 7.36, pCO2 62, paO2 50 mm Hg on her usual 2L oxygen via NC, glucose 160 and most recent HgbA1c 6.7%
• She is treated with albuterol, tiotropium, fluticasone-salmeterol (all baseline medications), azithromycin and guaifenesin
• What should be added to her regimen?

What should be added to her regimen?
A. Prednisone 40 mg PO daily x 5 d
B. Prednisone 40 mg PO x 14 days
C. Methylprednisolone 60 mg IV Q 6 hrs
D. Methylprednisolone 125 mg IV Q 8 hrs
E. Simply continue her inhaled fluticasone

JAMA. June 6, 2013
• Optimal dose and duration of steroids not known• N = 314 (92% admitted)• Prednisone 40 mg daily x 5 days versus 14• No difference
– Time to death– Time to exacerbation, death, or both– Recovery of lung function
• More steroids in the conventional group (793 mg vs 379 mg, P.001

Pearl #2
• It’s time to REDUCE our steroids for COPD exacerbations. Longer
courses are of no benefit.

Case 3A
• 78 yo woman is admitted foran UGIB
• 1 episode of hematemesis and 3-4 episodes of melena in the past 24 hours. No dyspnea, angina, presyncope or abdominal pain
• PMH: stable CAD s/p stent 2008, HTN, T2DM• Meds: ASA, clopidrogrel, chlorthalidone,
metoprolol, atorvastatin, metformin, glipizide. Recent ibuprofen for knee pain
• BP 110/78, HR 82, RR18• Hgb 7.8, Plt 276, BUN 42, Cr 1.3

What is the best treatment strategy?
A. IV normal saline
B. IV normal saline + IV PPI
C. Transfuse 2 units PRBC
D. Transfuse 2 units PRBC + IV PPI


Restrictive Transfusion Strategy in UGIB (for Hgb <7)
• Restrictive strategy– Lower mortality (45% relative risk reduction in mortality at 6 wks)
• NNT 25– Lower rebleeding rates– Reduced need for rescue therapies– Fewer complications– Fewer transfusions
• 60% fewer transfusions• Only 50% of patients transfused (vs. 86% in the liberal strategy)
– Shorter LOS
• Exclusions: shock or massive bleeding• How about LOWER GI bleed?
– Don’t know, but a restrictive strategy would seem to be sensible

Case 3B
• 65 yo woman with dyspnea• Admitted for NSTEMI, acute exacerbation
of heart failure and pneumonia• PMH: colon cancer currently undergoing
XRT (discovered after she had LGIB on ASA/clopidrogrel)
• Hgb 7.8, Trop 5.4, NT-pro-BNP 5800

Should one transfuse or not?
A. Do not transfuse
B. Transfuse 2 units PRBC

• Meta-analysis of 10 studies
• JAMA IM 1/28/13
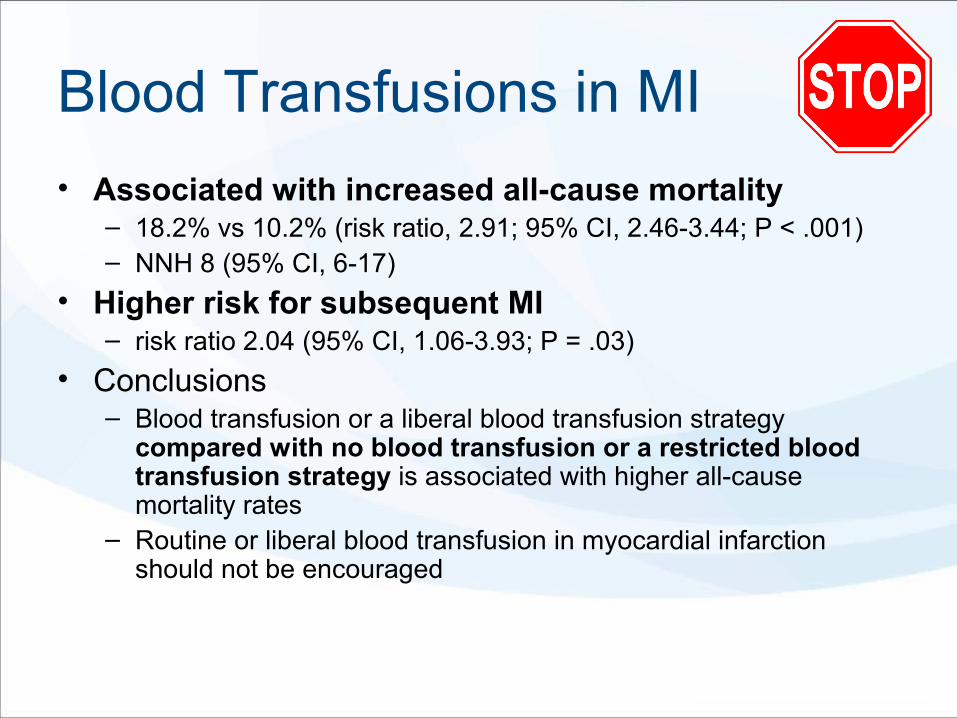
Blood Transfusions in MI
• Associated with increased all-cause mortality– 18.2% vs 10.2% (risk ratio, 2.91; 95% CI, 2.46-3.44; P < .001)– NNH 8 (95% CI, 6-17)
• Higher risk for subsequent MI– risk ratio 2.04 (95% CI, 1.06-3.93; P = .03)
• Conclusions– Blood transfusion or a liberal blood transfusion strategy
compared with no blood transfusion or a restricted blood transfusion strategy is associated with higher all-cause mortality rates
– Routine or liberal blood transfusion in myocardial infarction should not be encouraged

• Metaanalysis 3 tirals, 2364 patients with critical illness or bleeding• Transfusion trigger <7 reduced
– In-hospital mortality (RR, 0.74; ci, 0.60-0.92)– Total mortality (RR, 0.80; ci, 0.65-0.98)– Rebleeding (RR, 0.64; ci, 0.45-0.90)– Acute coronary syndrome (RR, 0.44; ci, 0.22-0.89)– Pulmonary edema (RR, 0.48; ci, 0.33-0.72)– Bacterial infections (RR, 0.86; ci, 0.73-1.00)
• NNT to prevent 1 death = 33
AJM. Feb 2014

Pearl #3
• Avoid blood transfusions in hemodynamically stable UGIB
(and probably LGIB), AMI, and ICU patients with Hgb >7.0 g/dL

Case 4A
• 72 yo woman with cirrhosis due to NASH is admitted for the first time with hepatic encephalopathy.
• The is no evidence of infection, medication noncompliance or other precipitating factors.
• NH3 97, urinalysis normal, ascites PMN 47
• What is the best treatment approach?

What is the best treatment approach?
A. Lactulose
B. Rifaximin
C. Lactulose + rifaximin
D. Lactulose + neomycin
E. Lactulose + BCAA
• RCT, N = 120 with overt HE• Lactulose 30-60 mL TID (to effect 2-3 semisoft
BM daily) vs lactulose + rifaximin 400 mg TID• Primary endpoint: complete reversal of HE• Secondary endpoints: mortality, LOS
Am J Gastroenterol. September 2013.

West Haven Encephalopathy Grade
Grade 1 • Trivial lack of awareness• Euphoria or anxiety• Shortened attention span• Impaired performance of addition
Grade 2 • Lethargy or apathy• Minimal disorientation for time or place• Subtle personality change• Inappropriate behavior• Impaired performance of subtraction
Grade 3 • Somnolence to semi-stupor, but responsive to verbal stimuli• Confusion, gross disorientation
Grade 4 • Coma

Lactulose + Rifaximin for HE
• 84% of patients: alcohol, HCV, HBV• Child-Pugh Class: B (31%), Class C (69%).
Mean MELD 25• Encephalopathy grade (West Haven): 2 (18%), 3
(33%), 4 (48%)
Outcome Lac + Rif Lac alone NNT
Complete Reversal HE
76% 44% 4
Mortality 24% 49% 4
LOS (d) 5.8 8.2

Case 4B
• 42 yo woman with alcoholism is admitted with severe alcoholic hepatitis
• AST 187, ALT 94, total bilirubin 20.2 (direct 12.6), PT 18.5 (INR 1.6), lipase 67, Cr 0.4
• Neg HCV, HBV, HIV• She is treated with IV vitamins, IV fluids and symptom-
triggered lorazepam as needed.• Abdominal US shows increased hepatic echotexture
without gallstones, ductal dilatation or pancreatitis• What is the best strategy to improve her 6-month
survival?

What else, if anything, should be added?
A. Meticulous supportive care alone
B. Prednisone 40 mg QD
C. Prednisolone 40 mg QD
D. Prednisolone + pentoxifylline
E. Acetylcysteine days 1-5

Severe Alcoholic Hepatitis
• Mortality at 6 months is 30-40%
• Maddrey Discriminant Function ≥32– MDF = 4.6 × [PT – control] + serum bilirubin
• Our patient– 4.6 (18.5 – 13.5) + 20.2 = 47.8

• Blinded RCT, 23 hospitals in France• N = 270 patients, mean age 52, Maddrey score >32, all had liver biopsy• Exclusions: HRS, HCC, uncontrolled bacterial infection or GI bleed in past 4 days, other causes
of hepatitis• Interventions
– Prednisolone 40 mg daily x 28 days– Prednisolone (same dose) + pentoxifylline 400 mg PO TID x 28 days
• Primary endpoint: mortality at 6 mo• Secondary endpoints: Hepatorenal syndrome, early responders at 7 days (Lille model)
JAMA. September 11, 2013
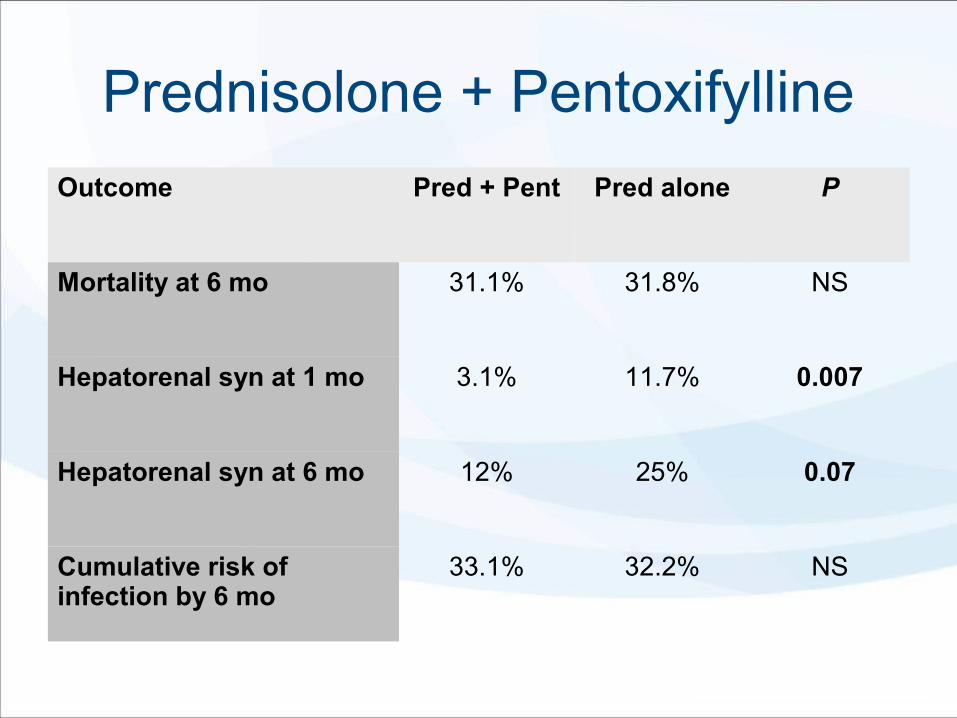
Prednisolone + Pentoxifylline
Outcome Pred + Pent Pred alone P
Mortality at 6 mo 31.1% 31.8% NS
Hepatorenal syn at 1 mo 3.1% 11.7% 0.007
Hepatorenal syn at 6 mo 12% 25% 0.07
Cumulative risk of infection by 6 mo
33.1% 32.2% NS

NEJM. November 10, 2011

Prednisolone + IV NAC
• Unblinded, 11 university hospitals in France• N = 180 patients, mean age 52, Maddrey score
>32, all had liver biopsy• Exclusions: HRS, HCC, uncontrolled bacterial
infection in past 7 days, other causes of hepatitis• Interventions
– Prednisolone 40 mg daily x 28 days– Prednisolone (same dose) + IV NAC 100 mg/kg/d*
(days 1-5)• Primary endpoint: mortality at 6 mo• Secondary endpoints: mortality at 1 months

Prednisolone + IV NAC
Outcome Pred + NAC Pred alone NNT
Mortality at 6 mo 27% 38% NS
Mortality at 1 mo 8% 24% 11
Hepatorenal syn at 6 mo 12% 25% 8
Infection at 6 mo 19% 42% 5
Pearls #4
• Adding rifaximin to lactulose is more effective than lactulose alone in the
treatment of overt hepatic encephalopathy
• Adding pentoxifylline or acetylcysteine to prednisolone does not improve 6-month
survival, but adding IV NAC might improve short-term mortality
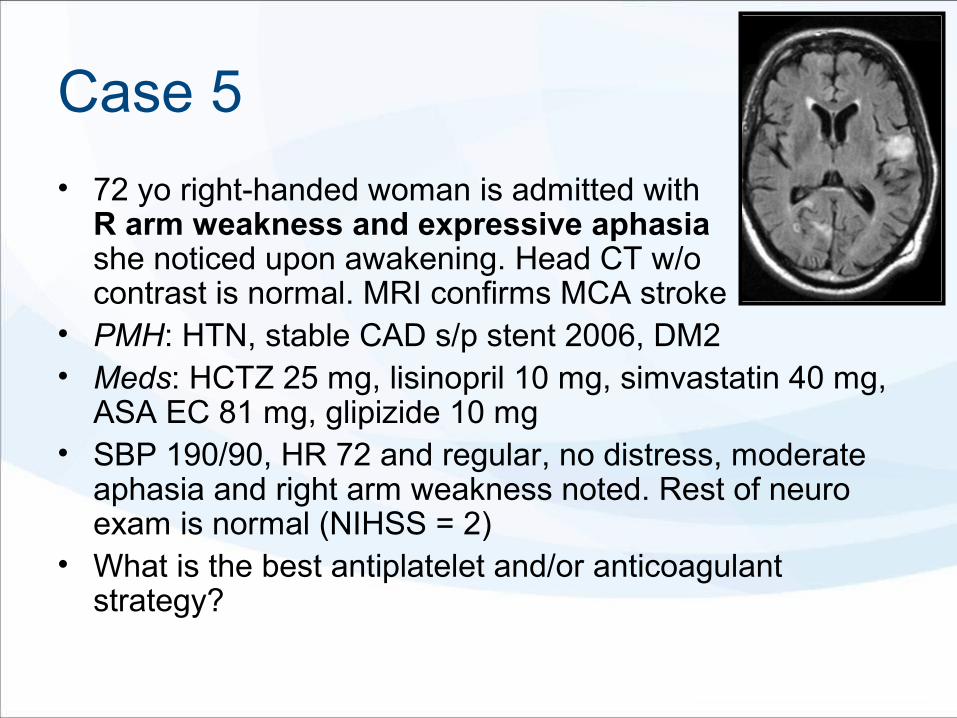
Case 5
• 72 yo right-handed woman is admitted with R arm weakness and expressive aphasiashe noticed upon awakening. Head CT w/o contrast is normal. MRI confirms MCA stroke
• PMH: HTN, stable CAD s/p stent 2006, DM2• Meds: HCTZ 25 mg, lisinopril 10 mg, simvastatin 40 mg,
ASA EC 81 mg, glipizide 10 mg• SBP 190/90, HR 72 and regular, no distress, moderate
aphasia and right arm weakness noted. Rest of neuro exam is normal (NIHSS = 2)
• What is the best antiplatelet and/or anticoagulant strategy?

What is the best antiplatelet and/or anticoagulant strategy?
A. Continue ASA 81 mg
B. Increase ASA to 325 mg
C. Change to ASA-DP ER or clopidrogrel
D. Add clopidrogrel and stop ASA after 3 weeks
E. Switch to warfarin or other oral anticoagulant

NEJM. July 4, 2013

CHANCE Trial
• RCT 114 sites in China• N = 5,170 with
– Minor stroke (NIHSS ≤3) or– High-risk TIA (ABCD2 ≥4)
• Interventions– Clopidrogrel 75 mg* + ASA 75 mg x 21 days,
then clopidrogrel alone (*300 mg load day 1)– ASA 75 mg daily
• Outcome: new stroke at 90 days

ABCD2 Score
ABCD2 Risk Factor Value Score
Age • ≥60 1
Blood pressure • SBP >160 or DBP >90 1
Clinical symptoms • Unilateral weakness• Speech disturbance w/o weakness
21
Duration • >60 minutes• 10-59 minutes
21
Diabetes • Oral medication or insulin 1
90-day Risk of Stroke
1-3 4 5 6 7
<10% 20% 26% 37% 43%

CHANCE trial
• Median age 62, women 34%
• Medical history– HTN: 66%– Smokers (current or former): 43%– DM: 21%
• Qualifying event– TIA: 28%– Minor stroke: 72%

CHANCE: ResultsOutcome Clopidogrel/ASA ASA NNT
Stroke at 90d 8.2% 11.7% 29
Stroke, MI or CV death 8.4% 11.9% 29
Hemorrhagic stroke 0.3% 0.3% NS
• No difference in MI, TIA, death, bleeding• Differences in Chinese patients?
– Death rate from stroke 5X higher than U.S– Less DM/HTN/Hypercholesterolemia– More large artery intracranial atherosclerosis
• Stay tuned for NIH POINT trial – very similar (600 mg)

Pearl #5
• Although long-term DAPT for secondary stroke prophylaxis is not
effective, short-term DAPT with clopidrogrel-ASA after TIA of minor
stroke might be
Case 6A
• 66 yo woman with cirrhosis admitted with dyspnea, fevers, leukocytosis and a pleural effusion. Spontaneous bacterial empyema (infection of hepatic hydrothorax) is suspected
• WBC 13, Hgb 10.1, Plt 44 000, PT 19.0, INR 1.7, Alb 2.5, TBili 2.9, Cr 1.1
• What should be done prior to diagnostic and therapeutic thoracentesis?

What should be done prior to thoracentesis?
A. Nothing
B. Infuse platelets
C. Infuse FFP
D. Infuse platelets and FFP
E. Infuse FFP and vitamin K

• Mild coagulation abnormalities have been shown to NOT increase bleeding risk with thoracentesis, yet transfusions of FFP or platelets is common– McVay PA, Toy PT. Transfusion. 1991;31(2):64-71. – Patel MD, Joshi SD. AJR Am J Roentgenol. 2011;197(1):W164-8.
• 1009 consecutive US-guided thoracenteses, men 53%, mean age 67• INR >1.6, platelet <50 x 109/L, or both• Performed by radiologists, radiology residents or fellows
Chest. August 2013

Thoracentesis with Abnormal Coagulation Parameters
• Transfusion decision and dose up to clinician and/or radiologist
Group 1(Not Corrected)
Group 2(Transfused FFP and/or Plt)
# Procedures 706 303
Mean INR 1.9 1.8
INR >1.6 88% 66%
Platelets <50 x 109/L 17% 45%
Fluid removed (mean) 888 mL 914 mL
Hemorrhage 0 4 (1.3%)

Case 6B
• The procedure goes well without apparent complication.
• 1200 mL straw-colored fluid removed
• Patient endorses rather marked improvement in dyspnea
• Should you order a post-procedure CXR?

Should you order a post-procedure CXR?
A. Yes
B. No

• Prospective cohort study• 278 procedures, mean age 66• Inpatients (44%) and outpatients (56%
– 10/1995-1/1998– Not on positive pressure ventilation– Diagnostic (45%), therapeutic (22%), both (32%)– US guidance (13%)– Malignant (42%), parapneumonic/empyema (16%), CHF (13%)
• CXR done at discretion of provider
Chest. April 2000

Limited Utility of CXR after Thoracentesis
• Operators– Non-radiology staff (51%), pulm fellow (36%), resident/student (13%)– PTX rates: 6%, 5%, 11%, respectively (overall 6.5%)
• PTX suspected in 6% due to aspiration of air - CXR obtained– PTX confirmed 69% of time
• CXR obtained 36% of time despite no suspected complication– PTX found in 3 patients– Vacuum bottles used in all cases
• No CXR obtain in the rest– 3 small PTX identified on subsequent imaging (CT in 2, CXR in 1)– No intervention was required
• New findings (e.g., atelectasis) after thoracentesis were rare (<4%) and did not affect management.
• No re-expansion pulmonary edema was seen• Vacuum bottles associated w/ increase PTX risk (OR 4.5, p<0.01)• If vacuum bottles are used, clinically significant immediate PTX was
always identified by the aspiration of free air
Pearls #6• Hemorrhagic complications after thoracentesis are
uncommon• Correction of abnormal INR or thrombocytopenia
before thoracentesis is unlikely to confer benefit.
• In the absence of a suspected complication, routine CXR after thoracentesis is not warranted and does not identify relevant new findings.
• Vacuum bottles should be avoided.

Case 7
• A 52 yo man arrives to the ED 120 minutes after the sudden onset of extremity weakness (R > L) and global aphasia. CT head demonstrates bilateral MCA dense vessel signs, L > R.
• PMH: T1DM s/p kidney-pancreas transplant 2008, recurrent DVT/PE with prothrombin mutation, HTN
• Meds: tacrolimus, mycophenolate, prednisone, warfarin, lisinopril
• BP 170/80, HR 86 and regular. Global aphasia. Dense right hemiparesis
• INR 1.2, Cr. 1.3• What is the best treatment option?


What is the best treatment option?
A. Aspirin 325 mg
B. Alteplase 90 mg IV
C. Alteplase followed 90 minutes later w/ endovascular management
D. Endovascular management



Endovascular Studies• IMS III (<3 hrs) [NINDS]
– N=656; 58 sites. – IV t-PA (<3 hours) vs IV t-PA followed by endovascular
therapy EVT) if a treatable occlusion was identified• Merci, Penumbra, Solitaire FR, EKOS microcatheter
– No difference in outcomes: debility, death or symptomatic ICH• SYNTHESIS Expansion (<4.5 hrs) [Italian Medicines Agency]
– N=362; 24 sites– IV t-PA vs EVT (IA t-PA +/- various mechanical devices)– No difference in outcomes– Start of treatment: IV t-PA (2h 45m), EVT (3h 45 m)
• MR RESCUE (<8 hrs) [NINDS]– N=127; 22 sites– Standard care vs mechanical EVT (Merci or Penumbra)– No difference in outcomes– Favorable penumbra pattern did not predict those who might benefit from
EVT
Merci
Penumbra

Pearl #7
• Endovascular management of acute stroke remains unproven

Case 8
• 47 yo man withHTN is admitted withacute ischemic stroke, confirmed by MRI
• UDS is negative; LDL 112• Rhythm: normal sinus• Carotids: no significant stenosis• Echo: EF 55%, PFO is demonstrated with RL shunting
during Valsalva• Well’s DVT score = 0• What is the best long-term therapy for this patient?

What is the best long-term therapy?
A. Aspirin
B. Warfarin
C. Rivaroxaban
D. Percutaneous PFO closure
E. Surgical PFO closure


PFO Closure Trials:Is it PC not to RESPECT CLOSURE?
• CLOSURE 1 (NEJM 3/15/12)– STARFlex device– N=909; 2 yr follow-up– No benefit: stroke, TIA, embolism
• PC Trial [St. Jude Medical]– Amplatzer PFO Occluder– N=414; 29 European sites; 4 yr follow-up– No benefit: stroke, embolism, death
• RESPECT [St. Jude Medical]– Amplatzer PFO Occluder– N=980; 69 US/Canadian sites; 2.5 yr follow-up– ITT analysis: No benefit: stroke, embolism, death– Per protocol: 0.46 per 100 patient-years in the
closure group and 1.30 in the medical group)• Meta-analyses
– No benefit over medical therapy

• PFO does not increase the 2-year risk of stroke compared to those w/o PFO
• Warfarin was not more effective than ASA
• PFO size or presence of atrial septal aneurysm did not affect outcomes
• ACCP9 (Feb 2013) recommends ASA
PICSS study. Circ 6/4/2002

Pearl #8
• Percutaneous closure of PFO has not yet been proven superior to aspirin
• Patients offered PFO closure should be part of a study or registry

Case 9
• 64 yo man admitted for weakness due to acute exacerbation of systolic HF. Meds were adjusted several weeks ago by his nephrologist, but patient cannot recall details
• Meds: furosemide 40 mg, lisinopril 40 mg, carvedilol 25 mg BID, losartan 50 mg, glipizide ER 10 mg daily
• 125/70, 74 (regular), RR 24, afebrile. JVD, crackles, S3 and edema are present
• Recent EF 25%-30%, NT-PBNP 12 000, Cr 2.0 (baseline 1.8) K 5.6, urine protein/creatinine 0.56 (down from 1.5)
• In addition to IV diuresis, which is the next best step in management?

In addition to IV diuresis, which is the next best step in management?A. Add spironolactone
B. Add hydralazine and isosorbide
C. Stop losartan
D. Restrict sodium to <2 gm/d
E. Repeat echocardiogram

• Losartan + lisinopril vs losartan alone• T2DM with proteinuria and GFR >30• Stopped early due to harms (AKI and
hyperkalemia)
• 33 RCT with >68,000 patients– 22 trials: ACEI + ARB vs monotherapy– 11 trials: Aliskiren + (ACEI or ARB) vs monotherapy
• Dual blockade did not improve all-cause or CV mortality • Outcomes of dual therapy
– 18% reduction in admissions for HF– 55% increase in hyperkalemia– 66% increase in risk of hypotension– 41% increase in risk of renal failure– 27% increase in withdrawal due to adverse events
• Efficacy and safety results were relatively consistent in various cohorts
Makani H, et al.

Pearl #9
• Dual RAS inhibition is not appropriate
• JNC8 (JAMA 2/5/2014): “Do not use an ACEI and an ARB together in the same patient.”

Case 10
• You are consulted to see a 71 yo woman in inpatient rehab for a UTI with bacteremia due to ESBL-producing Enterobacter sensitive only to piperacillin-tazobactam, imipenem and carbapenem.
• She confirms she is allergic to penicillin “hives,” but this was decades ago.
• What would be the best strategy?

What would be the best strategy?
A. Treat empirically with colistin
B. Treat empirically with polymixin
C. Treat with meropenem and observe closely
D. Test for penicillin allergy
E. Desensitize to penicillin

ESBL Organisms
• ESBL– R to most cephalosporins except cefoxitin
– R to most penicillins except pip-tazo– R to aztreonam
• Carbapenems are the usual drugs of choice

J Allergy Clin Immunol Pract, May 2013.

Penicillin Allergy
• 8% of Americans report an allergy to penicillins• Major determinant
– Penicilloyl polylysine (Pre-Pen®)
• Minor determinants– Penicilloate– Penilloate– Native penicillin– Amoxicillin
• Complete panel of PCN skin tests has never been available
• Pre-Pen not available from 2000-2001 and 2004-2009 (so many physicians not familiar with testing)

Macy et al
• 500 sequential Kaiser (San Diego) patients with PCN “allergy” in the EHR– Exclusion: TEN/SJS/bullous dermatosis, hemolysis,
hepatitis, nephritis– Inclusions: anaphylaxis, respiratory problems, hives,
swelling, rash other than above, unknown
• Skin tests with Pre-Pen, pen G, amoxicillin– First: prick test– If neg: intradermal test– If neg: amoxicillin 250 mg PO and observe x 1 hr

Macy et al: Results
• 4/500 (0.8%) had a positive skin test to Pre-Pen– No reactions to pen G or amoxicillin
• 4/496 had objective reactions to oral amoxicillin– All treated with oral antihistamine and resolved within 1 hour– 15 patients (3%), all women, reported subjective symptoms only
• 11 (73%) had Multiple Drug Intolerance Syndrome (3 or more unrelated classes)
• None received treatment
• No delayed-onset reactions (possible T-cell-mediated)• 29 patients promptly treated with -lactamsẞ
– 22 patients treated in hospital– 7 treated as outpatients (for syphilis)– There were no reactions

Rimawi et al
• N = 146 with hx of PCN allergy– Urticaria 68%, edema 22%, bronchospasm 16%, anaphylaxis 14%– Medical, surgical, L&D, ICU, ED
• Exclusions– Uncertain allergy or non-IgE-mediated reaction– Hx of severe exfoliation– Anaphylaxis within last 4 weeks
• Skin testing performed by I.D. fellows– Pre-Pen, Pen G, histamine, saline prick test– If neg: intradermal (0.02 mL)– If neg: Pen VK 250 mg (or the drug to which allergy reported)
Rimawi et al
• All 146 had neg prick test• 1/146 developed urticaria, edema, pruritis
6 minutes after intradermal injection• 145 tolerated the oral challenge and
switch to -lactam antibioticẞ (PCNs, cephalosporins, carbapenems) without allergy
• Savings, better ABx choices, and avoidance of PICCs reported

Penicillin Allergy
• PRE-PEN®– Available in 0.25 mL vials
– Necessary but not sufficient for allergies to the major determinant
• Negative skin tests indicates <<< 5% chance of reaction to PCN (mostly dermatologic)

Pre-Pen®: Procedure
• Prick test– Volar forearm– Using needle (22-28 ga), place a drop on
skin, then prick through the drop– Read at 15 min (or before) for wheal,
erythema, pruritis• POS = wheal >5 mm
– If Negative, then intradermal
• Intradermal– Upper outer arm– Tuberculin syringe
• Create 3 mm (0.02 mL) blebs with PRE-PEN and saline control
– Read at 20 minutes• POS = pruritis and increase bled to >5 mm

Coding & Billing - 2014
CPT Procedure Facility Price ($) wRVU
95018 Skin testing(prick, intradermal), Report # of tests
7.05 per test 0.14 per test
95076 Oral challenge(up to 120 minutes)
73.73 1.5
ICD-9
V14.0 Personal hx of allergy to penicillin
V14.1 Personal hx of allergy to other antibiotic
http://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx

Pearl #10
• There is an epidemic of over-reported PCN allergy (>20 million Americans)
• Very few inpatients (~2%) are truly allergic to PCN
• Patients can safely use -lactams after ẞnegative skin testing and oral challenge

Summary: The Best of 2013
• Don’t stent RAS• No dual ACEI-ARB• Add rifaximin for
hepatic encephalopathy
• Avoid blood products before thoracentesis
• Restrictive transfusion strategy for UGIB/AMI
• DAPT x 3 weeks for TIA or minor stroke
• Interventional stroke mgmt remains unproven
• Antiplatelets for PFO• Prednisone 40 mg x 5
for COPD• Give -lactams after ẞ
negative skin testing
Recommended Resources
• ACP JournalWise
• DynaMed EBM Focus
• NEJM Journal Watch