Hospital-Acquired Acute Renal Failure
9
DISEASE OF THE MONTH Hospital-Acquired Acute Renal Failure CHARLES R. NOLAN and ROBERT J. ANDERSON Department of Medicine, University of Colorado Health Sciences Center and Denver Veterans Affairs Medical Center, Denver. Colorado. Acute renal failure (ARF) is the abrupt loss of renal function sufficient to decrease urinary elimination of nitrogenous waste (urea nitrogen and creatinine). Although there is consensus about this general definition, few agree on the magnitude of the rise in serum eneatinine necessary to ascribe a diagnosis of ARF (1,2). These differences in definition plus variances in methods of patient accrual, populations analyzed, and eatego- rization of causes render development of a broad-based over- view of ARF difficult. However. two generalizations about contemporary ARF are compelling. First, ARF is predomi- nantly a hospital-acquired disorder (1-3). Second, the high mortality of patients with ARF is not explained entirely by comonbid conditions. Recent data indicate that ARF per se increases the risk of development of multiple nonrenal condi- tions that lead to death and disability (4). Thus, ARF should not always be considered a treatable condition that complicates advanced disease. Together, these two generalizations prompt this review, which focuses on the causes, diagnosis, preven- tion, and management of hospital-acquired ARF. Causes and Clinical Settings of Hospital- Acquired ARF Categorization of the cause(s) of hospital-acquired ARF has traditionally involved determining which general physiologic mechanism (prerenal, postrenal, or intrarenal) is responsible for the decline of glomerulan filtration (Figure 1). This method has the advantage of providing a well accepted diagnostic framework that guides the clinician to comprehensively eon- siden most potential causes of deteriorating renal function ( 1 ,5). Prerenal factors (e.g. , extracellulan fluid volume loss and/or sequestration and impaired cardiac function) contribute to 30 to 60% of all cases of ARF. Postrenal factors (e.g., intra- or extrarenal obstruction of urine flow) are much less frequently encountered causes of hospital-acquired ARF ( 1 to 10%) but are almost always amenable to therapy. When considering renal causes of ARF, it is helpful to think of each renal anatomic compartment (vasculature, glomeruli, intenstitium, and tubules) as a potential contributor to the renal failure. Although acute vascular (e.g. , atheroemboli, vaseulitis, throm- bosis), glomerular (e.g. , glomerulonephritis), and interstitial Correspondence to Dr. Robert J. Anderson, University of Colorado Health Sciences Center. Box B 180. 4200 East Ninth Avenue. Denver. CO 80262. 1046-6673/09()4-07 l0$03.00/0 Journal of the American Society of Nephrology Copyright 0 1998 by the American Society of Nephrology (e.g. , allergic interstitial nephritis) processes occasionally cause hospital-acquired ARF, the major cause is acute tubular injury. This tubular damage is most often due to either is- ehemia (e.g., prolonged prerenal insult) or a nephrotoxin. Sometimes acute tubular injury occurs in the setting of pig- mentunia (e.g. , myogbobinunia or hemogbobinuria). A recent study by Liano and Pascual provides a reasonable overview of the causes of hospital-associated ARF (3). This experience was based on more than 740 eases of ARF that were either referred to or occurred within 13 tertiary care facilities in Madrid, Spain. Of these eases, 45% were attributed to acute tubular necrosis, 21% to prenenal causes, 10% to postrenal causes, 3% to renal vascular disorders, 3% to glomerulonephri- tis, and 2% to acute interstitial nephritis (3). In the study by Brivet ci a!. drawn from 20 French multidisciplinary intensive care units (ICUs), the type of ARF was pnerenal in I 7%, renal (usually acute tubular injury) in 78%, and postrenal in 5% (6). From a more pragmatic standpoint, general hospital-ac- quired ARF is usually encountered within a relatively narrow context of settings. These settings include the postoperative state, advanced cardiovascular disease, neoplastie disease, HIV infection, multiple organ failure, systemic infection, and solid organ transplantation. The hospital-acquired ARF that occurs in these disparate settings is usually associated with one or more of three renal insults, including prerenal events (extra- cellular fluid volume defects and hemodynamie instability), exposure to nephrotoxins, and sepsis. The postoperative period is currently one of the most prey- alent settings of ARF. For example, 27% of the 748 eases of ARF reported by Liano and Pascual were encountered in the postoperative setting (3). Older studies by Charlson et a!. indicated that 25% of elective, noneardiac surgical procedures were complicated by an acute rise in serum ereatinine of 20% or greater (7). In 11% of these patients, a 50% decline in endogenous ereatinine clearance occurred (7). More recent studies by Chertow ci’ a!. , using Veterans Affairs patient data- bases, indicate that the development of ARF sufficient to require renal replacement therapy occurs in 0.4 to 7.5% of patients undergoing cardiac surgery and 0.6% of patients un- dergoing general surgery, and is dependent on a number of preoperative risk factors (8,9). What underlies the relatively high frequency of ARF that occurs in relation to elective surgical procedures? In many eases, underlying comorbidity (diabetes mellitus, chronic hy- pertension, vascular disease, congestive heart failure) leads to diminished baseline GFR and reduced renal reserve (7-9). With this background, the “surgical experience” appears to
Transcript of Hospital-Acquired Acute Renal Failure

DISEASE OF THE MONTH
Hospital-Acquired Acute Renal Failure
CHARLES R. NOLAN and ROBERT J. ANDERSON
Department of Medicine, University of Colorado Health Sciences Center and Denver Veterans Affairs Medical
Center, Denver. Colorado.
Acute renal failure (ARF) is the abrupt loss of renal function
sufficient to decrease urinary elimination of nitrogenous waste
(urea nitrogen and creatinine). Although there is consensus
about this general definition, few agree on the magnitude of the
rise in serum eneatinine necessary to ascribe a diagnosis of
ARF (1,2). These differences in definition plus variances in
methods of patient accrual, populations analyzed, and eatego-
rization of causes render development of a broad-based over-
view of ARF difficult. However. two generalizations about
contemporary ARF are compelling. First, ARF is predomi-
nantly a hospital-acquired disorder (1-3). Second, the high
mortality of patients with ARF is not explained entirely by
comonbid conditions. Recent data indicate that ARF per se
increases the risk of development of multiple nonrenal condi-
tions that lead to death and disability (4). Thus, ARF should not
always be considered a treatable condition that complicates
advanced disease. Together, these two generalizations prompt
this review, which focuses on the causes, diagnosis, preven-
tion, and management of hospital-acquired ARF.
Causes and Clinical Settings of Hospital-Acquired ARF
Categorization of the cause(s) of hospital-acquired ARF has
traditionally involved determining which general physiologic
mechanism (prerenal, postrenal, or intrarenal) is responsible
for the decline of glomerulan filtration (Figure 1). This method
has the advantage of providing a well accepted diagnostic
framework that guides the clinician to comprehensively eon-
siden most potential causes of deteriorating renal function ( 1 ,5).
Prerenal factors (e.g. , extracellulan fluid volume loss and/or
sequestration and impaired cardiac function) contribute to 30 to
60% of all cases of ARF. Postrenal factors (e.g., intra- or
extrarenal obstruction of urine flow) are much less frequently
encountered causes of hospital-acquired ARF ( 1 to 10%) but
are almost always amenable to therapy. When considering
renal causes of ARF, it is helpful to think of each renal
anatomic compartment (vasculature, glomeruli, intenstitium,
and tubules) as a potential contributor to the renal failure.
Although acute vascular (e.g. , atheroemboli, vaseulitis, throm-
bosis), glomerular (e.g. , glomerulonephritis), and interstitial
Correspondence to Dr. Robert J. Anderson, University of Colorado HealthSciences Center. Box B 180. 4200 East Ninth Avenue. Denver. CO 80262.
1046-6673/09()4-07 l0$03.00/0Journal of the American Society of Nephrology
Copyright 0 1998 by the American Society of Nephrology
(e.g. , allergic interstitial nephritis) processes occasionally
cause hospital-acquired ARF, the major cause is acute tubular
injury. This tubular damage is most often due to either is-
ehemia (e.g., prolonged prerenal insult) or a nephrotoxin.
Sometimes acute tubular injury occurs in the setting of pig-
mentunia (e.g. , myogbobinunia or hemogbobinuria).
A recent study by Liano and Pascual provides a reasonable
overview of the causes of hospital-associated ARF (3). This
experience was based on more than 740 eases of ARF that were
either referred to or occurred within 13 tertiary care facilities in
Madrid, Spain. Of these eases, 45% were attributed to acute
tubular necrosis, 21% to prenenal causes, 10% to postrenal
causes, 3% to renal vascular disorders, 3% to glomerulonephri-
tis, and 2% to acute interstitial nephritis (3). In the study by
Brivet ci a!. drawn from 20 French multidisciplinary intensive
care units (ICUs), the type of ARF was pnerenal in I 7%, renal
(usually acute tubular injury) in 78%, and postrenal in 5% (6).
From a more pragmatic standpoint, general hospital-ac-
quired ARF is usually encountered within a relatively narrow
context of settings. These settings include the postoperative
state, advanced cardiovascular disease, neoplastie disease, HIV
infection, multiple organ failure, systemic infection, and solid
organ transplantation. The hospital-acquired ARF that occurs
in these disparate settings is usually associated with one or
more of three renal insults, including prerenal events (extra-
cellular fluid volume defects and hemodynamie instability),
exposure to nephrotoxins, and sepsis.
The postoperative period is currently one of the most prey-
alent settings of ARF. For example, 27% of the 748 eases of
ARF reported by Liano and Pascual were encountered in the
postoperative setting (3). Older studies by Charlson et a!.
indicated that 25% of elective, noneardiac surgical procedures
were complicated by an acute rise in serum ereatinine of 20%
or greater (7). In 1 1 % of these patients, a 50% decline in
endogenous ereatinine clearance occurred (7). More recent
studies by Chertow ci’ a!. , using Veterans Affairs patient data-
bases, indicate that the development of ARF sufficient to
require renal replacement therapy occurs in 0.4 to 7.5% of
patients undergoing cardiac surgery and 0.6% of patients un-
dergoing general surgery, and is dependent on a number of
preoperative risk factors (8,9).
What underlies the relatively high frequency of ARF that
occurs in relation to elective surgical procedures? In many
eases, underlying comorbidity (diabetes mellitus, chronic hy-
pertension, vascular disease, congestive heart failure) leads to
diminished baseline GFR and reduced renal reserve (7-9).
With this background, the “surgical experience” appears to

Figure 1. Acute renal failure.
Hospital-Acquired ARF 71 1
potentially induce afferent arteriolar renal vasoconstrietion and
diminished GFR (10,1 1). If an additional renal insult is en-
countered, clinical ARF occurs (7-9). These additional renal
insults are often referred to as “second hits” and include
reoperation, sepsis, nephrotoxin exposure, circulatory/volume
deficits, and heart failure (7-9).
A high percentage of contemporary hospital-acquired ARF
occurs in patients in the ICU. For example, 27% of the 748
eases of ARF reported by Liano and Pascual were encountered
in the ICU (3), and the frequency of ARF in patients admitted
to ICUs ranges from 6 to 23% (reviewed in reference 1). In
most eases of ICU-acquired ARF, the ARF occurs in the
setting of multiple organ failure. For example, more than 90%
of cases of ICU-aequired ARF have failure of one or more
additional organ systems, and the failure of these other systems
nearly always precedes the development of ARF (reviewed in
reference 1). In the recent ICU experience of Brivet ci’ a!.,
failure of another organ system was nearly uniformly present in
patients with ARF (6). In all series of ICU-associated ARF,
hemodynamie instability, nephrotoxins, and sepsis are eon-
comitantly present in more than two-thirds of all patients
(1-3,6).
ARF is commonly encountered in patients with HIV infee-
tion (12). Valeri and Neusy found that more than half of 246
HIV-infeeted patients had one or more episodes of a rise in
serum ereatinine of 0.3 mg/dl or greater ( 1 2). The causes of
ARF in the HIV population are diverse and include prerenal
conditions, postrenal failure (due to either intratubular micro-
crystallization from sulfa drugs/protease inhibitors or ureterie
obstruction from lymphoma), and renal disorders, including
thrombotie mieroangiopathy, HIV-associated nephropathy,
gbomerulopathy, interstitial nephritis, and acute tubular injury
occurring in the setting of sepsis and/or nephrotoxins (12,13).
Patients with neoplastie disease are also at high-risk for
hospital-acquired ARF (1,14). The frequency of development
of ARF in patients with hematobogic malignancies may be up
to 40% in some series (14). Sepsis, tumor-lysis syndrome,
hyperealeemia, hyperunicemia, nephrotoxins, and prerenal fac-
tons are the predominant causes of ARF in patients with ma-
lignancies. Less commonly encountered causes include tumor
infiltration, obstructive uropathy, and glomerubopathy.
Two of the most common conditions predisposing to hospi-
tab-acquired ARF are sepsis and nephrotoxin exposure. A ease-
control study identified sepsis as the single factor associated
with the greatest risk of developing hospital-acquired ARF
(15), and sepsis was the most common factor (48% of eases)
predisposing to development of ICU-associated ARF in the
study of Brivet ci’ a!. (6). Not only is hospital-acquired sepsis
often linked to ARF, but community-acquired sepsis is also
commonly associated with ARF (I 6). The experience of
Rayner et a!. found that 24% of 239 patients with community-
acquired bacteremia doubled their serum ereatinine coneentra-
tions (16).
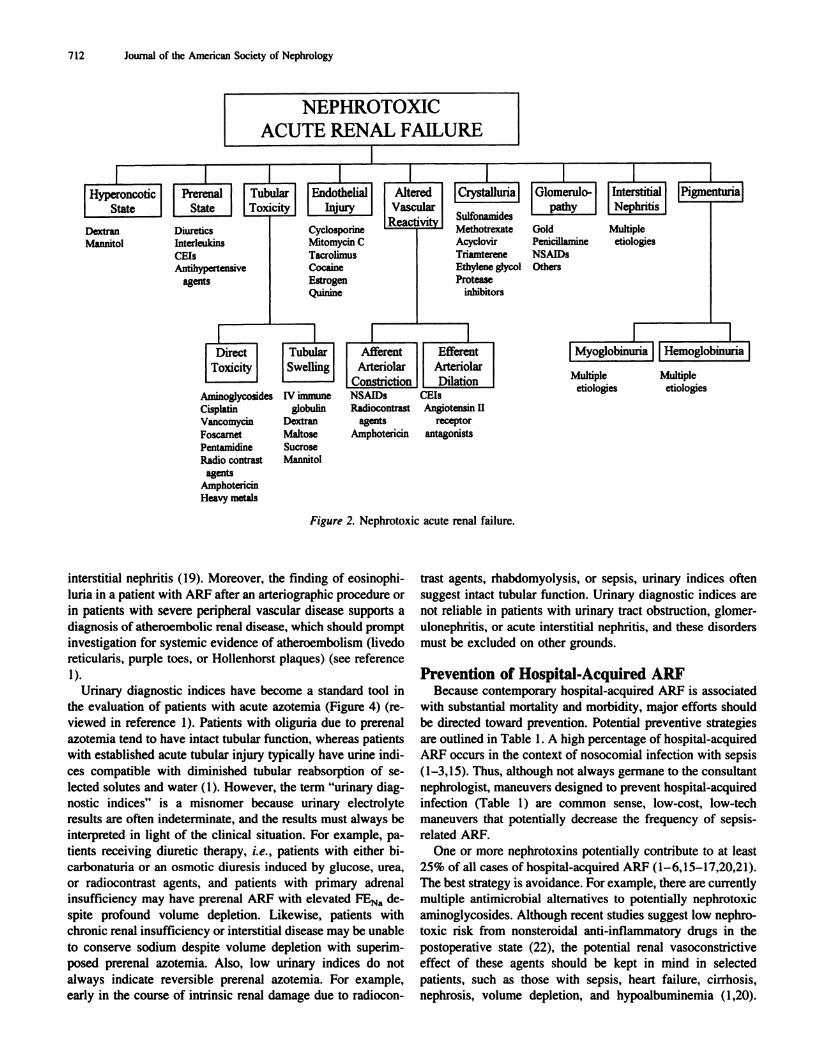
In every analysis, nephrotoxie agents have been found to
contribute to hospital-acquired ARF (1-4,17). The number of
potential nephrotoxins is large, and the mechanisms by which
nephrotoxins contribute to ARF are diverse (Figure 2). More-
over, new agents (e.g. , protease inhibitors, immune globulin,
tacrolimus) are continually being added to the ever-expanding
list of foods, plants, animal venoms, and diagnostic and then-
apeutic drugs capable of inducing ARF, emphasizing the need
for a comprehensive review of medication/exposure history in
each ease (1,17,18).
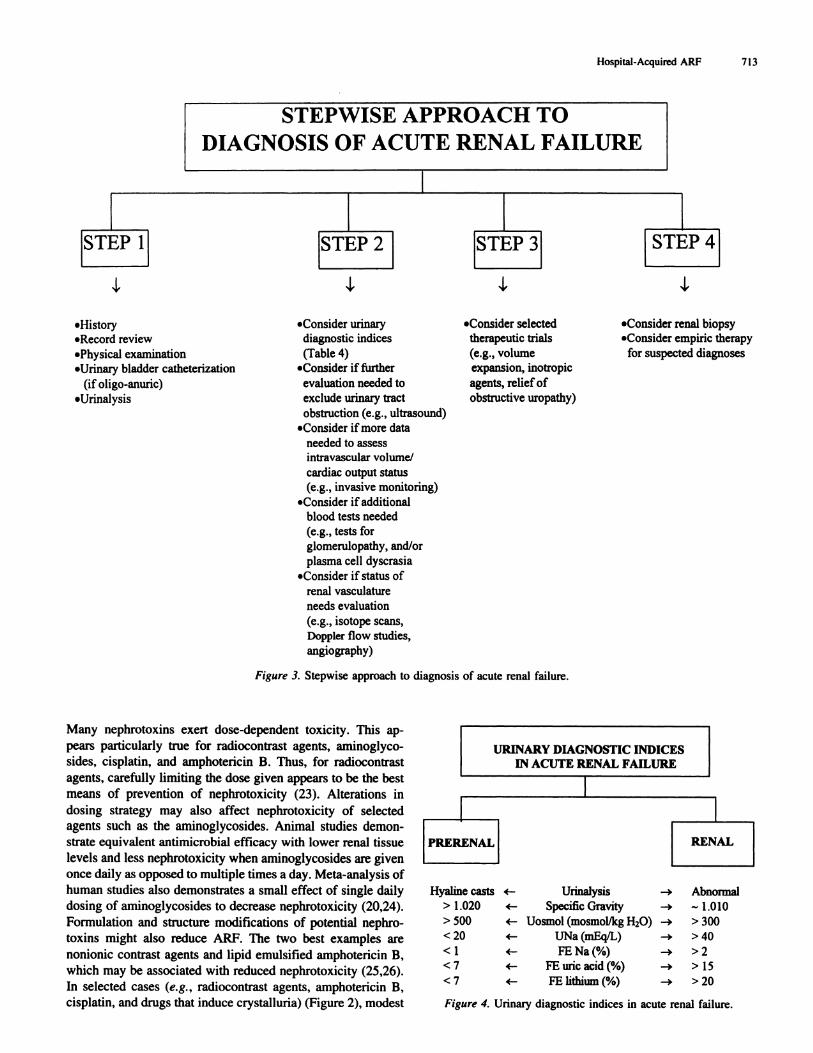
Diagnosis of Hospital-Acquired ARFThe time-honored approach to evaluating a patient with ARF
is to exclude prerenal and postrenal causes and then, if neces-
sary, initiate an examination to determine potential renal eti-
obogies. We favor a four-step approach to this process, as
outlined in Figure 3. In our experience, the cause(s) of ARF is
usually apparent after step 1 . A thorough review of the medical
record is mandatory to identify potential nephnotoxie drugs on
other insults, such as volume depletion, hypotension, radiocon-
trast studies, or surgical interventions. A careful historical and
physical examination for clues to volume status is imperative,
because prerenal azotemia is a correctable condition, and care-
ful volume repletion may be of value even in established ARF.
Occasionally, hemodynamie monitoring, i.e., noting changes in
cardiac output, capillary wedge pressure, or urine output in
response to a trial of either volume expansion or inotropie
agents, may be useful in the process of excluding prerenal
azotemia.
Urinalysis performed by the physician is usually a key tool
in the diagnostic evaluation of ARF. A normal urinalysis is
most compatible with pre- or postrenal forms of ARF. Numen-
ous pigmented granular casts or the finding of abundant tubular
epithelial cells helps support a diagnosis of isehemia/nephro-
toxin-induced ARF. The detection of heme-pigment by dip-
stick screening, which is out of proportion to the number of
erythrocytes on microscopic examination, suggests the pres-
ence of pigmentunia due to rhabdomyolysis on intravascular
hemolysis. Significant proteinuria, hematunia, on the finding of
red blood cell casts suggests an underlying gbomerubonephnitis
or vasculitis. White blood cell casts may be seen in the setting
of acute pyebonephritis, interstitial nephritis, or gbomerulone-
phritis. The finding of eosinophiluria by Hansel’s stain sug-
gests that the ARF is not due to acute tubular injury. However,
in the absence of systemic signs of an allergic reaction (fever,
rash, peripheral eosinophilia), the finding of eosinophiluria is
suggestive, but clearly not diagnostic, of drug-induced acute
NEPHROTOXIC
ACUTE RENAL FAiLURE
DextranMannitol
DiureticsInterleukinsCEIsAntihypertensive
agents
CyclosponineMitomycin CTacrolimusCocaineEstrogenQuinine
MethotrexateAcyclovirTniamtereneEthylene glycolProtease
inhibitors
GoldPenicillamineNSAIDsOthers
Multipleetiologies
AminoglycosidesCisplatinVancomycinFoscarnetPentamidineRadio contrast
agentsAmphotenicinHeavy metals
IV immuneglobulin
DextranMaltoseSucroseMannitol
NSAIDs
Radiocontrastagents
Amphotenicin
CEIsAngiotensin II
receptorantagonists
Multipleetiologies
Multipleetiologies
712 Journal of the American Society of Nephrology
Figure 2. Nephnotoxic acute renal failure.
interstitial nephritis ( I 9). Moreover, the finding of eosinophi-
lunia in a patient with ARF after an arteriographie procedure or
in patients with severe peripheral vascular disease supports a
diagnosis of atheroembolic renal disease, which should prompt
investigation for systemic evidence of atheroembolism (livedo
reticulanis, purple toes, or Hollenhonst plaques) (see reference
I ).
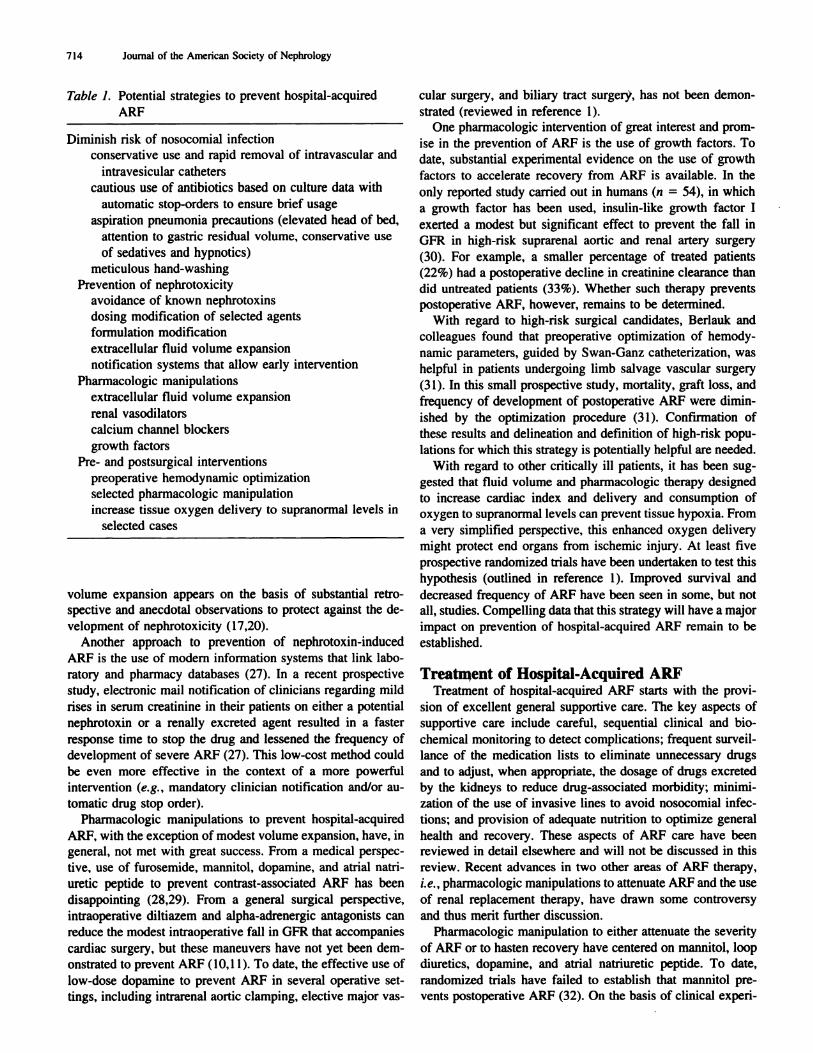
Urinary diagnostic indices have become a standard tool in
the evaluation of patients with acute azotemia (Figure 4) (re-
viewed in reference 1 ). Patients with oliguria due to prerenal
azotemia tend to have intact tubular function, whereas patients
with established acute tubular injury typically have urine mdi-
ces compatible with diminished tubular reabsorption of Se-
bected solutes and water ( I ). However, the term “urinary diag-
nostie indices” is a misnomer because urinary electrolyte
results are often indeterminate, and the results must always be
interpreted in light of the clinical situation. For example, pa-
tients receiving diuretic therapy, i.e. , patients with either bi-
earbonaturia or an osmotic diuresis induced by glucose, urea,
on nadiocontrast agents, and patients with primary adrenal
insufficiency may have prenenal ARF with elevated FENa de-
spite profound volume depletion. Likewise, patients with
chronic renal insufficiency on interstitial disease may be unable
to conserve sodium despite volume depletion with superim-
posed prerenal azotemia. Also, low urinary indices do not
always indicate reversible prerenal azotemia. For example,
early in the course of intrinsic renal damage due to radiocon-
trast agents, rhabdomyolysis, or sepsis, urinary indices often
suggest intact tubular function. Urinary diagnostic indices are
not reliable in patients with urinary tract obstruction, gbomer-
ubonephnitis, or acute interstitial nephritis, and these disorders
must be excluded on other grounds.
Prevention of Hospital-Acquired ARFBecause contemporary hospital-acquired ARF is associated
with substantial mortality and morbidity, major efforts should
be directed toward prevention. Potential preventive strategies
are outlined in Table I . A high percentage of hospital-acquired
ARF occurs in the context of nosocomial infection with sepsis
(1-3,15). Thus, although not always germane to the consultant
nephrologist, maneuvers designed to prevent hospital-acquired
infection (Table 1 ) are common sense, low-cost, low-tech
maneuvers that potentially decrease the frequency of sepsis-
related ARF.
One or more nephrotoxins potentially contribute to at least
25% of all cases of hospital-acquired ARF ( I -6,15-17,20,21).
The best strategy is avoidance. For example, there are currently
multiple antimicrobial alternatives to potentially nephrotoxie
aminoglycosides. Although recent studies suggest low nephro-
toxic risk from nonsteroidal anti-inflammatory drugs in the
postoperative state (22), the potential renal vasoconstrietive
effect of these agents should be kept in mind in selected
patients, such as those with sepsis, heart failure, cirrhosis,
nephrosis, volume depletion, and hypoalbuminemia (1,20).
rSTEP 1� STEP 2 � STEP 3� � STEP�
URINARY DIAGNOSTIC INDICESIN ACUTE RENAL FAILURE
PRERENAL RENAL
Hyaline casts +- Urinalysis
> 1.020 +- SpecificGravity
> 500 �- Uosmol (mosmol/kg H2O)
< 20 �- UNa (mEq/L)
<1 �- FENa(%)
<7 4- FEuricacid(%)
<7 4- FElithium(%)
-3 Abnormal
-3 -.1.010
-+ >300
-3 >40
-3 >2
-4 >15
-). >20
Hospital-Acquired ARF 713
Figure 4. Urinary diagnostic indices in acute renal failure.
STEPWISE APPROACH TO
DIAGNOSIS OF ACUTE RENAL FAILURE
#{149}History
#{149}Recordreview
#{149}Physical examination
#{149}Uninarybladder catheterization
(if oligo-anuric)
#{149}Uninalysis
#{149}Consider urinary
diagnostic indices
(Table 4)
#{149}Considerif further
evaluation needed to
exclude urinary tract
obstruction (e.g., ultrasound)
#{149}Consider ifmore data
needed to assess
intravascular volume/
cardiac output status
(e.g., invasive monitoring)
#{149}Consider if additional
blood tests needed
(e.g., tests for
gbomerubopathy, and/or
plasma cell dyserasia
#{149}Considen if status of
renal vasculature
needs evaluation
(e.g., isotope scans,
Doppler flow studies,
angiography)
‘Consider selectedtherapeutic trials
(e.g., volume
expansion, inotropic
agents, reliefof
obstructive uropathy)
‘Consider renal biopsy
#{149}Consider empiric therapy
for suspected diagnoses
Figure 3. Stepwise approach to diagnosis of acute renal failure.
Many nephrotoxins exert dose-dependent toxicity. This ap-
pears particularly true for radiocontrast agents, aminoglyco-
sides, cisplatin, and amphotericin B. Thus, for nadiocontrast
agents, carefully limiting the dose given appears to be the best
means of prevention of nephrotoxieity (23). Alterations in
dosing strategy may also affect nephrotoxieity of selected
agents such as the aminoglycosides. Animal studies demon-
strate equivalent antimicrobial efficacy with lower renal tissue
levels and less nephrotoxicity when aminoglycosides are given
once daily as opposed to multiple times a day. Meta-analysis of
human studies also demonstrates a small effect of single daily
dosing of aminoglycosides to decrease nephrotoxieity (20,24).
Formulation and structure modifications of potential nephro-
toxins might also reduce ARF. The two best examples are
nonionie contrast agents and lipid emulsified amphotericin B,
which may be associated with reduced nephrotoxieity (25,26).
In selected eases (e.g. , radiocontrast agents, amphotericin B,
cisplatin, and drugs that induce erystalluria) (Figure 2), modest
714 Journal of the American Society of Nephrology
Table I. Potential strategies to prevent hospital-acquired
ARF
Diminish risk of nosocomial infection
conservative use and rapid removal of intravascular and
intravesiculan catheters
cautious use of antibiotics based on culture data with
automatic stop-orders to ensure brief usage
aspiration pneumonia precautions (elevated head of bed,
attention to gastric residual volume, conservative use
of sedatives and hypnotics)
meticulous hand-washing
Prevention of nephrotoxieity
avoidance of known nephrotoxins
dosing modification of selected agents
formulation modification
extracellular fluid volume expansion
notification systems that allow early intervention
Pharmacologic manipulations
extracellular fluid volume expansion
renal vasodilatons
calcium channel blockers
growth factors
Pre- and postsungieal interventions
preoperative hemodynamic optimization
selected pharmacologic manipulation
increase tissue oxygen delivery to supranormal levels in
selected eases
volume expansion appears on the basis of substantial retro-
speetive and anecdotal observations to protect against the de-
vebopment of nephrotoxieity (17,20).
Another approach to prevention of nephrotoxin-induced
ARF is the use of modern information systems that link labo-
ratory and pharmacy databases (27). In a recent prospective
study, electronic mail notification of clinicians regarding mild
rises in serum ereatinine in their patients on either a potential
nephrotoxin or a nenally excreted agent resulted in a faster
response time to stop the drug and lessened the frequency of
development of severe ARF (27). This low-cost method could
be even more effective in the context of a more powerful
intervention (e.g. , mandatory clinician notification and/or au-
tomatie drug stop order).
Pharmacologic manipulations to prevent hospital-acquired
ARF, with the exception of modest volume expansion, have, in
general, not met with great success. From a medical perspec-
tive, use of furosemide, mannitol, dopamine, and atnial natni-
uretic peptide to prevent contrast-associated ARF has been
disappointing (28,29). From a general surgical perspective,
intraopenative diltiazem and alpha-adrenengic antagonists can
reduce the modest intnaoperative fall in GFR that accompanies
cardiac surgery, but these maneuvers have not yet been dem-
onstrated to prevent ARF (10, 1 1 ). To date, the effective use of
low-dose dopamine to prevent ARF in several operative set-
tings, including intrarenal aortic clamping, elective major vas-
eular surgery, and biliary tract surgery, has not been demon-
strated (reviewed in reference 1).
One pharmacologic intervention of great interest and prom-
ise in the prevention of ARF is the use of growth factors. To
date, substantial experimental evidence on the use of growth
factors to accelerate recovery from ARF is available. In the
only reported study earned out in humans (n = 54), in which
a growth factor has been used, insulin-like growth factor I
exerted a modest but significant effect to prevent the fall in
GFR in high-risk supranenal aortie and renal artery surgery
(30). For example, a smaller percentage of treated patients
(22%) had a postoperative decline in ereatinine clearance than
did untreated patients (33%). Whether such therapy prevents
postoperative ARF, however, remains to be determined.
With regard to high-risk surgical candidates, Berlauk and
colleagues found that preoperative optimization of hemody-
namie parameters, guided by Swan-Ganz catheterization, was
helpful in patients undergoing limb salvage vascular surgery
(3 1). In this small prospective study, mortality, graft loss, and
frequency of development of postoperative ARF were dimin-
ished by the optimization procedure (3 1). Confirmation of
these results and delineation and definition of high-risk popu-
lations for which this strategy is potentially helpful are needed.
With regard to other critically ill patients, it has been sug-
gested that fluid volume and pharmacologic therapy designed
to increase cardiac index and delivery and consumption of
oxygen to supranormal levels can prevent tissue hypoxia. From
a very simplified perspective, this enhanced oxygen delivery
might protect end organs from isehemie injury. At least five
prospective randomized trials have been undertaken to test this
hypothesis (outlined in reference 1 ). Improved survival and
decreased frequency of ARF have been seen in some, but not
all, studies. Compelling data that this strategy will have a major
impact on prevention of hospital-acquired ARF remain to be
established.
Treatment of Hospital-Acquired ARFTreatment of hospital-acquired ARF starts with the provi-
sion of excellent general supportive care. The key aspects of
supportive care include careful, sequential clinical and bio-
chemical monitoring to detect complications; frequent surveil-
lance of the medication lists to eliminate unnecessary drugs
and to adjust, when appropriate, the dosage of drugs excreted
by the kidneys to reduce drug-associated morbidity; minimi-
zation of the use of invasive lines to avoid nosocomial infec-
tions; and provision of adequate nutrition to optimize general
health and recovery. These aspects of ARF care have been
reviewed in detail elsewhere and will not be discussed in this
review. Recent advances in two other areas of ARF therapy,
i.e. , pharmacologic manipulations to attenuate ARF and the use
of renal replacement therapy, have drawn some controversy
and thus merit further discussion.
Pharmacologic manipulation to either attenuate the severity
of ARF on to hasten recovery have centered on mannitol, loop
diuretics, dopamine, and atrial natriuretic peptide. To date,
randomized trials have failed to establish that mannitol pre-
vents postoperative ARF (32). On the basis of clinical experi-
Hospital-Acquired ARF 715
enee and retrospective studies, however, many experienced
nephrologists continue to use mannitol in an effort to attenuate
ARF, especially pigment-associated ARF (I). With regard to
loop diuretics, prospective randomized trials, undertaken in
patients with advanced, well established ARF, fail to demon-
strate a beneficial effect on duration of azotemia, dialysis
requirement, or mortality (32,33). Although some of these
studies demonstrate that loop diuretics increase urine output, it
is not clear whether oligurie ARF patients with a loop diuretic-
induced increase in urine flow have the same, more favorable
prognosis than do ARF patients that are spontaneously nono-
liguric. Nonetheless, because of the generally low complication
rate associated with loop diuretics, many clinicians administer
loop diuretics to patients with ARF who continue to be oliguric
despite optimization of renal perfusion and exclusion of post-
renal factors.
Low-dose (<3 to 5 p.g/kg per mm) dopamine is widely used
in ARF, especially in oligurie patients. A large study, using
each patient as his or her own control, has clearly established
that low-dose dopamine can render many oligurie patients
nonoliguric (34). This nonoligurie state, however, does not
necessarily appear to reflect a rise in GFR. In a recent analysis
of 256 patients with ARF in which dopamine was administered
nonrandomly at the discretion of the treating physician, the
relative risk of death or dialysis associated with low-dose
dopamine administration, after adjustment for several van-
ables, was 0.95 (95% confidence interval, 0.58 to 1.58; refer-
ence 35). Because there was no statistically significant differ-
ence in outcome in patients treated with low-dose dopamine,
the authors concluded that the routine use of low-dose dopa-
mine in ARF should be discouraged until a prospective, ran-
domized, placebo-controlled trial establishes its safety and
efficacy. Other researchers, however, believe that the docu-
mented potential diuretic effect and nonthreatening side-effect
profile of low-dose dopamine mandate its continued use, es-
pecially in oligurie ARF.
Atnial natriuretic peptide is known to increase GFR by
dilation of afferent arterioles and constriction of efferent arte-
rioles. Several experimental and uncontrolled clinical trials
suggest clinical benefit from both intranenal and intravenous
atrial natriuretic peptides in established ARF. In a recent mul-
ticenter, randomized, double-blind, placebo-controlled clinical
trial of anaritide in 504 critically ill patients with acute tubular
necrosis, patients received a 24-h infusion of either anaritide
(0.2 �tg/kg per mm) on placebo (36). The primary end point
was dialysis-free survival for 2 1 d after treatment. The rate of
dialysis-free survival was not significantly different between
the two groups (47% in the placebo group and 43% in the
ananitide group, P = 0.35). However, in a subgroup of 120
patients with oliguria, dialysis-free survival was 8% in the
placebo group (five of 60 patients) and 27% in the anaritide
group ( 16 of 60 patients, P = 0.008). Anaritide-treated patients
who became nonoliguric after treatment seemed to benefit the
most. A subsequent, similarly designed study that enrolled only
patients with oligunic acute tubular necrosis failed to demon-
strate a benefit of anaritide administration. Drug company
development of ananitide, however, has been suspended. The
suspension was prompted by a low probability that a positive
outcome could be obtained with respect to the primary clinical
end point of dialysis-free survival (Robin Allgnen, personal
communication).
There are several arguable issues regarding renal replace-
ment therapy (RRT) for ARF. These issues include: when to
begin, what membrane and modality to use, and what level of
intensity is sufficient? With regard to commencement of RRT,
there has been a general trend in recent years toward earlier
initiation. This aggressive approach does not necessarily
equate with an improvement in therapy. To our knowledge, no
study in the modern era has adequately addressed timing of
initiation of RRT. One study of 132 critically ill ARF patients
found an inverse relationship between serum eneatinine con-
centration at initiation of hemodialysis and mortality (37).
Although these data are subject to at least two interpretations
(early dialysis is deleterious versus patients dialyzed earlier are
sicker with more fluid overload and electrolyte disturbances),
they do raise concerns. Moreover, intermittent hemodialysis
may be associated with hemodynamie instability, which, with
potential impairment of renal autoregulatory responses that can
occur in ARF, may lead to enhanced isehemie injury (38). Few
would argue that volume overload and hypenkalemia refractory
to medical therapy, as well as uremie symptoms and compli-
eations, merit RRT. As far as the level of azotemia is eon-
cerned, little data support prophylactic RRT for blood urea
nitrogen (BUN) levels <200 mg/dl (37).
The choice of RRT modality is also a subject of debate. One
issue involves the type of membrane. It has recently become
apparent that biocompatibility of dialysis membranes may be
an important determinant of survival and recovery of renal
function in patients with ARF (39,40). The polysacchanide
structure of cellulosie (bioincompatible) membranes provides a
trigger for complement activation via the alternative pathway,
which leads to the liberation of anaphylotoxins and activation
of leukocytes. The potential induction of a systemic inflamma-
tory reaction during each dialysis treatment with bioincompat-
ible dialysis membranes could conceivably cause further is-
ehemia or inflammatory changes within the previously injured
renal microcireulation.
In a recent study of 72 patients with ARF, patients were
randomized to intermittent dialysis treatment with either bioin-
compatible Cuprophane dialysis membranes, which activate
the complement system and leukocytes, on to dialysis with a
biocompatible membrane composed of polymethyl methacry-
late, which has a less marked effect on complement and leu-
kocytes (39). The two dialysis membranes chosen for the study
had similar clearance and ultrafiltration characteristics and the
patient groups were similar. Fifty-seven percent of patients on
dialysis with biocompatible membranes survived, compared
with 37% of those dialyzed with Cuprophane membranes (P =
0. 1 1 ). Recovery of renal function occurred in 62% of those
dialyzed with a biocompatible membrane, compared with 37%
of those who underwent dialysis with Cuprophane membranes
(P = 0.04). The time to recovery of renal function after
initiation of dialysis was also significantly shorter in the bio-
compatible membrane group compared with the Cuprophane
716 Journal of the American Society of Nephrology
group: five dialysis treatments over I 1 d versus 17 dialysis
treatments over 33 d, respectively. Subgroup analysis revealed
that the benefits of biocompatible membrane dialysis were
evident only in patients who were nonoligunic before the mi-
tiation of dialysis. These results suggest that use of the bio-
compatible dialysis membrane increases the likelihood of me-
covery of renal function and survival of patients with ARF.
Other studies have confirmed and extended these observations
to include other biocompatible dialysis membranes, including
polysulfone and polyacrylonitnile membranes (40). However,
this issue may not be quite as clear-cut as these two studies
suggest. For example, in the most recent prospective random-
ized study (ii = 1 33) of patients with severe ARF who were
concomitantly undergoing mechanical ventilation and contin-
uous, high-flux dialysis, the type of membrane did not influ-
ence survival in those patients undergoing continuous high-
flux dialysis (41).
The modality of RRT for ARF is also debatable, with
proponents of both intermittent hemodialysis (IHD) and con-
tinuous modes of RRT (CRRT) (42,43). Surveys of nephrolo-
gists in the United States reveal that IHD is the most common
modality used for treating ARF, followed by CRRT and then
penitoneal dialysis (43). The IHD modality has been in wide-
spread use for the past four decades for the treatment of ARF.
In recent years, the development of bicarbonate-based dialy-
sate and volumetrically controlled machines for precise control
of ultrafiltration has made IHD a safer procedure in the h�mo-
dynamically unstable ICU patient with multiorgan failuk. In
most centers in the United States, the standard approach to IHD
for ARF uses moderate blood flow rates (200 to 250 ml/min)
and dialysate flow rates of 500 mllmin. In contrast to the
situation for treatment of chronic renal failure, there are no
well established guidelines for defining IHD adequacy in ARF.
Dialysis frequency and intensity are usually determined em-
pinically based on the patient’s volume status, associated elm-
ical events, BUN levels, and other blood chemistries.
The most common reasons cited for preferential choice of
IHD are efficacy, ease of use, and familiarity of the dialysis
and ICU nursing personnel with the procedure. CRRT tends to
be reserved for patients who are hemodynamically unstable or
hypereatabolie. or for those with large fluid burdens due to
aggressive nutritional support (42). The minority of nephrobo-
gists who administer peritoneal dialysis cite the absence of a
need for anticoagulation and better hemodynamie stability as
the main reasons for using this technique. For rapid correction
of life-threatening electrolyte or acid-base disorders, IHD is
probably the best choice, given both the efficacy and rapidity
of response. On the other hand, if fluid removal is the primary
objective, hemodynamic instability may limit aggressive ultra-
filtration during a 3- to 4-h IHD treatment. Thus, for hyper-
catabolic patients receiving nutritional support with a high
nitrogen content, even daily hemodialysis may provide made-
quate urea clearance. CRRT modalities, especially hemofiltra-
tion techniques that combine dialysis with significant ultrafil-
trate volumes to enhance solute clearances, may provide the
more intensive treatment necessary to control azotemia in
catabolic ICU patients receiving high protein content nutrition
(42). The major disadvantage of CRRT is the need for well
trained ICU nursing personnel to perform the procedure. A
lack of detailed understanding of the CRRT flow sheets and the
computations necessary to determine replacement fluid vol-
umes can lead to disaster due to significant volume depletion.
Occasionally, lactate-based replacement fluid may result in
lactate accumulation and worsening acid-base status if the
patient has liver disease and is unable to metabolize lactate as
a source of base. On-site formulation of custom bicarbonate-
containing replacement fluid is costly and time consuming.
Ambulation and physical therapy may be difficult while the
patient is receiving CRRT.
The issue of dialysis intensity in ARF also remains contro-
versial. In one study, patients with ARF were matched by
etiology and randomly assigned to either an intensive treatment
group (dialysis to maintain BUN <60 mg/dl and ereatinine <5
mg/dl) or to a nonintensive group (dialysis to maintain BUN
< 100 mg/dl and creatinine <9 mg/dl; reviewed in reference
37). Seven of 17 (41 %) patients in the intensive group survived
compared with nine of 17 (53%) in the nonintensive group.
Complications such as hemorrhage (24% versus 59%) and
septicemia (47% versus 65%) were less common in the inten-
sive treatment group. Although none of the differences be-
tween groups reached statistical significance, this study has
been criticized because of insufficient power to detect a dif-
ference in survival (37). It has been postulated that a random-
ized clinical trial capable of identifying an absolute risk redue-
tion of 10% would require a sample size in excess of 750
matched patients (37). In general, once RRT is initiated, most
nephrologists aim to keep BUN and serum creatinine at levels
<80 to 100 and 8 to 10 mg/dl, respectively.
Outcome of Hospital-Acquired ARFThe outcome of hospital-acquired ARF depends on the site
(ward or ICU), comonbidity, cause, and severity of the renal
failure. As a general estimate, contemporary survival of hos-
pital-aequired ARF severe enough to be dialyzed averages 10
to 50% ( I ). The development of even mild hospital-acquired
ARF sufficient to cause a 25% increase in serum creatinine to
at least 2 mg/dl increased mortality fivefold in a recent case
control cohort analysis of contrast-associated ARF (4).
New developments have been reported in three areas with
regard to ARF outcome. First, some analyses suggest that the
outcome of severe hospital-acquired ARF, although generally
dismal, may be improving. An excellent retrospective study
found that ICU-associated ARF is associated with significantly
lower mortality in the more modern era versus two decades ago
despite comparable or more severe comorbidity (44). In the
Mayo Clinic study, there was a 20% increase in hospital
survival and a 9% increase in 1-yr survival when ICU patients
with ARF who required dialysis from the period 1977 to 1979
were compared with comparable patients from the period 1991
to 1992 (44). Second, substantial effort is being placed on the
application of existing severity of illness and outcome predie-
tion models, as well as the development of new models, to
patients with ARF (reviewed in references I and 45). These
prediction models are useful to stratify and assign patients for
Hospital-Acquired ARF 717
prospective studies, as well as to compare risk-adjusted out-
comes across several sites. However, to date, they remain
insufficiently predictive to be routinely used in clinical deci-
sion-making with regard to level of care in many cases.
Finally, reasonable cost-effectiveness analyses are being
done regarding RRT in critically ill patients with hospital-
acquired ARF (46). A recent prospective cohort study from
five geographically diverse teaching hospitals included 490
patients with ARF requiring dialysis (46). Median survival was
32 d, and 27% survived 6 mo. Survivors were dependent for at
least one activity of daily life (bathing, moving, toileting,
feeding, or dressing), but 62% rated their quality of life as
good. The estimated cost per quality-adjusted life-year saved
by initiating dialysis was $274, 100 for the 103 patients in the
worst prognostic category and $61 ,900 for the 94 patients in
the best prognostic category. These costs somewhat exceed
$50,000 per quality-adjusted life-year, which has been arbi-
trarily defined as the threshold for cost-effective care.
References1 . Anderson Ri, Schrier RW: Acute renal failure. In: Diseases of
the Kidney, edited by Schrier RW, Gottshalk CW, Boston, Little,
Brown and Co., 1997, pp 1069-1 113
2. Elasy TA, Anderson RI: Changing demography of acute renal
failure. Semin Dial 9: 438-443, 1996
3. Liano F, Pascual I: Epidemiology of acute renal failure: A
prospective, multicenter community-based study. Kidney mt 50:
811-818, 1996
4. Levy EM, Viscoli CM, Horwitz RI: The effect of acute renal
failure on mortality: A cohort analysis. JAMA 275: 1489-1494,
1996
5. Mindell IA, Chertow GM: A practical approach to acute renal
failure.Med Clin North Am 81: 731-748, 1997
6. Brivet FG, Kleinknecht DI, Loirat P. Landais P1: Acute renalfailure in intensive care units-causes, outcome and prognostic
factors of hospital mortality: A prospective, multicenter study.
Crit Care Med 24: 192-198, 1996
7. Charlson ME, MacKenzie CR, Gold JP, Shines GT: Postopera-
tive changes in serum creatinine: When do they occur and how
much is important? Ann Surg 209: 328-338, 1989
8. Chertow GM, Lazarus IM, Christiansen CL, Cook EF, Hammer-
meister KE, Grover F, Daley I: Preoperative renal risk stratifi-
cation. Circulation 95: 878-884, 1997
9. Chertow GM, Henderson W, Khuni S. Hun K, Daley I: Acute
renal failure after non-cardiac surgery: Results from the national
VA surgical risk study. J Am Soc Nephrol 8: l23A, 1997
10. Kulka P1, Tryba M, Zeng M: Preoperative a2-adnenengic recep-
ton agonists prevent the deterioration of renal function aftercardiac surgery: Results of a randomized, controlled trial. Crit
Care Med 24: 947-952, 1996
1 1 . Amano I, Suzuki A, Sunamari M, Tofukiyi M: Effect of calcium
antagonist diltiazem on renal function in open heart surgery.
Chest 107: 1260-1265, 1995
12. Valeri A. Neusy AJ: Acute and chronic renal failure in hospital-
ized AIDS patients. Clin Nephrol 35: 1 10-1 18, 1991
13. Kopp JB. Miller KD, Mican IM, Feuenstein IM, Vaughan E.
Baker C, Pannell LK, Falloon I: Crystalluria and urinary tract
abnormalities associated with indinavir. Ann intern Med 127:
119-125. 1997
14. Lanore JI, Brunet T, Prichard F: Hemodialysis for acute renal
failure in patients with hematologie malignancies. Crit Care Med
19: 346-351, 1991
15. Shusterman N, Strom BL: Risk factors and outcome of hospital-
acquired acute renal failure. A,n J Med 83: 65-71, 1987
16. Rayner BL, Willeox PA, Pascoe MD: Acute renal failure in
community-acquired bacteremia. Nephron 54: 32-35, 1990
17. Choundry D, Ahmed Z: Drug-induced nephnotoxicity. Med Cliii
North Am 81: 705-717, 1997
I 8. Cayco AV, Penazella MA, Harplett IP: Renal insufficiency af-
ten intravenous immune globulin therapy: A report of two cases
and analysis of the literature. J Am Soc Nephrol 8: 1788-1794,I997
19. Nolan CR, Anger MS. Kelleher SP: Eosinophiluria: A new
method of detection and definition of the clinical spectrum.
NEnglJMed3l5: 1516-1519, 1986
20. Hock R, Anderson RI: Prevention of drug-induced nephrotoxic-
ity in the intensive care unit. J Crit Care 10: 33-43, 1995
21 . Guttham SP, Rodriguez LA, Raiford DS. Oliart AD, Romeu JR:
Nonsteroidal anti-inflammatory drugs and the risk of hospital-
ization for acute renal failure. Arch Intern Med 156: 2433-2439,
1996
22. Feldman HI, Kinman IL, Berlin IA, Hennesy 5, Kimmel SE,
Farrar J, Carson IL, Strom BL: Panenteral ketorolac: The risk foracute renal failure. Ann intern Med 126: 193-199, 1997
23. Cigarrou RG, Lange PA, Williams RH, Hatlis D: Dosing of
contrast material to prevent contrast nephropathy in patients with
renal disease. Am J Med 86: 644-650, 1989
24. Hatala R, Dinh T, Cook DI: Once-daily aminoglycoside dosing
in immuno-competent adults: A meta-analysis. Ann Intern Med
124: 717-725, 1996
25. Barrett BJ, Carliste El: Meta-analysis of the relative nephrotox-
icity of high- and low- osmolality contrast media. Radiology 188:
171-178, 1993
26. Sorkine P. Nagar H, Weinbroum A, Setton A, Israitel E, Scarlatt
A, Silbiger A, Rudick V, Kluger Y, Halpern P: Administration of
amphotenicin B in lipid emulsion decreases nephrotoxicity: Re-
sults of a prospective, randomized controlled study in critically
illpatients. Crit Care Med 24: 131 1-1315, 1996
27. Rind DV, Safran C, Phillips PS: Effect of computer-based alerts
on the treatment and outcomes of hospitalized patients. Arch
Intern Med 154: 1511-1517, 1994
28. Solomon R, Werner C, Mann D, D’Elia I, Silva P: Effects of
saline, mannitol, and furosemide on acute decreases in renal
function induced by nadiocontrast agents. N Engl J Med 33 1:1416-1420, 1994
29. Weisbeng LS, Kunnick PB, Kurnick BR: Risk of radiocontrast
nephropathy in patients with and without diabetes mellitus. Kid-
,ies. liii 45: 259-265, 1994
30. Franklin SC, Moulton M, Sicard GA, Hammerman MR. Miller
SB: Insulin-like growth factor I preserves renal function postop-
eratively. Am J Phvsiol 272: F257-F259, 1997
31. Benlauk IF, Abrams IH, Gilmour II, O’Connor SR. Knighton
DR. Cerra FB: Preoperative optimization of cardiovascular he-
modynamics improves outcome in peripheral vascular surgery.
Ann Surg 214: 289-295, 1991
32. Congen ID: Interventions in clinical acute renal failure: What are
the data? Am J Kidney Dis 26: 565-576, 1995
33. Majumdar S. Kjellstrand CM: Why do we use diuretics in acute
renal failure? Semin Dial 9: 454-459, 1996
34. Flancbaum L, Choban PS. Dasta IF: Quantitative effects of low

7 18 Journal of the American Society of Nephrology
dose dopamine on urine output in oliguric surgical intensive care
unit patients. Crit Care Med 22: 61-66, 1994
35. Chertow GM, Sayegh MH, Allgren RL, Lazarus MI: Is the
administration of dopamine associated with adverse on favorable
outcomes in acute renal failure? Am J Med 101 : 49-53, 1996
36. Allgnen RL, Marbuny TC, Rahman SN: Anaritide in acute tubular
necrosis. N Engl J Med 336: 828-834, 1997
37. Chertow GM, Lazarus JM: Intensity of dialysis in established
acute renal failure. Semin Dial 9: 476-480, 1996
38. Congen ID: Does hemodialysis delay recovery from acute renal
failure? Semi,i Dial 3: 146-150, 199039. Hakim RM, Wingard RL, Parker RA: Effect of the dialysis
membrane in the treatment of acute renal failure. N EngI J Med
331: 1338-1342, 1994
40. Himmelfarb I. Hakim RM: The importance of biocompatible
membranes in dialysis. Semun Dial 9: 481-483, 1996
41 . Jones CH, Newstead CG, Goutcher E, Will El, Dean 5G. Davi-
son AM: Continuous dialysis for ARF in the ICU: Choice of
membrane does not influence survival. J Am Soc Nephrol 8:126A, 1997
42. Forni LG, Hilton P1: Continuous hemofiltration in the treatment
of acute renal failure. N Engl J Med 336: 1303-1309, 1997
43. Mehta RL: Modalities of dialysis for acute renal failure. Semin
Dial 9: 469-475, 1996
44. McCarthy IT: Prognosis of patients with acute renal failure in the
intensive care unit: A tale of two eras. Mayo Clin Proc 7 1:
117-126, 1996
45. Douma CE, Redekop WK, Van den Meulen JH, Van Olden RW,
Hoeck I, Struijk DG, Knediet RT: Predicting mortality in inten-
sive care patients with acute renal failure treated with dialysis.
J Am Soc Nephrol 8: 1 11-1 17, 1997
46. Hamel MB, Phillips RS, Davis RB, Desbiens W, Connors AF,
Teno JM, Wenger N, Lynn I, Wu AW, Fulkenson W, Tsevat J:
Outcomes and cost-effectiveness of initiating dialysis and con-
tinuing aggressive care in seriously ill hospitalized adults. Ann
Intern Med 127: 195-202, 1997