Honeycomb Lung: History and Current Conceptssudhirstomorrow.yolasite.com/resources/Honeycomb...
10
AJR:196, April 2011 773 [5], who used the term “bronchiolar emphy- sema,” considered their cases to be a special type of pulmonary emphysema. The term “honeycomb lung” first appeared in the English literature in 1949 in a study by Oswald and Parkinson [9]. Sixteen clinical cases of honeycomb lung were presented in de- tail. The cases included, as interpreted by cur- rent medical knowledge, Langerhans cell histi- ocytosis, lymphangioleiomyomatosis (LAM), and probable chronic interstitial pneumonia, which was not a disease diagnosed in that era [9] (Fig. 2). In the definition by Oswald and Pakinson, honeycomb lung was “descriptive of the appearance of the cut surface of the lungs” as being “thin-walled cysts distributed uni- formly throughout the substance of both lungs, varying in sizes up to a maximum of 1 cm in diameter.” A more comprehensive report with a pathologic description followed in 1956 by Heppleston [10], who in his practice dealt with a wide variety of diseases and clinical back- grounds (32 patients were coal workers). In this report, most cases were probable chron- ic interstitial pneumonia, which also included a small number of those with sarcoidosis, be- rylliosis, eosinophilic granuloma, LAM, giant cell interstitial pneumonia, scleroderma, and even tuberculous bronchopneumonia. Thus, before the 1960s, honeycomb lung was considered the macroscopic appearance of lung diseases comprising various histo- pathologic processes and causes, partly be- cause physicians had little idea of identify- Honeycomb Lung: History and Current Concepts Hiroaki Arakawa 1 Koichi Honma 2 Arakawa H, Honma K 1 Department of Radiology, Dokkyo Medical University, 880 Kita-Kobayashi, Mibu, Tochigi, 3210293 Japan. Address correspondence to H. Arakawa ([email protected]). 2 Department of Cancer Center Pathology, Dokkyo Medical University, Tochigi, Japan. Cardiopulmonary Imaging • Review AJR 2011; 196:773–782 0361–803X/11/1964–773 © American Roentgen Ray Society T he term “honeycomb lung” origi- nated in the 19th century in Ger- many where medicine was highly developed in that era. We can go back as far as 1858 when Kessler described a case of congenital bronchiectasis [1]. Since then, the honeycomb appearance of the lung was named, variously by different authors, Wabenlunge (honeycomb lung), Zystenlunge (cystic lung), Schwammlunge (spongy lung), and Sacklunge (sacculated lung) [1, 2]. In the German literature, honeycomb lung was usu- ally considered a congenital malformation or anomalous development of the lung with bron- chiectasis [2] (Fig. 1). It seems that the term “honeycomb lung” was not applied to chronic interstitial pneumonia in Germany. In the first half of the 20th century, the idea of idiopathic pulmonary fibrosis (IPF) was not yet established, and only occasional case reports were found, in which the authors called their cases different names or only re- ported the clinical and pathologic findings [3–6]. The famous report by Hamman and Rich [3], which initially appeared in 1935, did not use the term “honeycomb lung.” In the subsequent English literature, cases of presumed IPF were reported under the name bronchiolar emphysema [5], pulmonary muscular hyperplasia [4], or cystic pulmo- nary cirrhosis [6]. Originating in the Ger- man literature, these names were translated into English and were discussed as a rare and new disease entity [7, 8]. Sibert and Fisher Keywords: CT, honeycomb lung, idiopathic interstitial pneumonia, interstitial lung disease DOI:10.2214/AJR.10.4873 Received April 29, 2010; accepted after revision August 28, 2010. OBJECTIVE. Originally used to describe the macroscopic appearance of various patho- logic processes with multiple cysts, honeycomb lung is now the term used to describe end- stage pulmonary fibrosis. The purpose of this article is to discuss the history and imaging of honeycomb lung. CONCLUSION. Honeycomb lung is considered one of the important CT findings in usual interstitial pneumonia. An additional challenge for radiologists is that different patho- logic processes can mimic honeycomb lung. Therefore, a precise understanding of honey- comb lung is necessary. Arakawa and Honma Imaging of Honeycomb Lung Cardiopulmonary Imaging Review Downloaded from www.ajronline.org by 175.38.202.175 on 02/02/15 from IP address 175.38.202.175. Copyright ARRS. For personal use only; all rights reserved
Transcript of Honeycomb Lung: History and Current Conceptssudhirstomorrow.yolasite.com/resources/Honeycomb...
AJR:196, April 2011 773
[5], who used the term “bronchiolar emphy-sema,” considered their cases to be a special type of pulmonary emphysema.
The term “honeycomb lung” first appeared in the English literature in 1949 in a study by Oswald and Parkinson [9]. Sixteen clinical cases of honeycomb lung were presented in de-tail. The cases included, as interpreted by cur-rent medical knowledge, Langerhans cell histi-ocytosis, lymphangioleiomyomatosis (LAM), and probable chronic interstitial pneumonia, which was not a disease diagnosed in that era [9] (Fig. 2). In the definition by Oswald and Pakinson, honeycomb lung was “descriptive of the appearance of the cut surface of the lungs” as being “thin-walled cysts distributed uni-formly throughout the substance of both lungs, varying in sizes up to a maximum of 1 cm in diameter.” A more comprehensive report with a pathologic description followed in 1956 by Heppleston [10], who in his practice dealt with a wide variety of diseases and clinical back-grounds (32 patients were coal workers). In this report, most cases were probable chron-ic interstitial pneumonia, which also included a small number of those with sarcoidosis, be-rylliosis, eosinophilic granuloma, LAM, giant cell interstitial pneumonia, scleroderma, and even tuberculous bronchopneumonia.
Thus, before the 1960s, honeycomb lung was considered the macroscopic appearance of lung diseases comprising various histo-pathologic processes and causes, partly be-cause physicians had little idea of identify-
Honeycomb Lung: History and Current Concepts
Hiroaki Arakawa1
Koichi Honma2
Arakawa H, Honma K
1Department of Radiology, Dokkyo Medical University, 880 Kita-Kobayashi, Mibu, Tochigi, 3210293 Japan. Address correspondence to H. Arakawa ([email protected]).
2Department of Cancer Center Pathology, Dokkyo Medical University, Tochigi, Japan.
Cardiopulmonar y Imaging • Review
AJR 2011; 196:773–782
0361–803X/11/1964–773
© American Roentgen Ray Society
The term “honeycomb lung” origi-nated in the 19th century in Ger-many where medicine was highly developed in that era. We can go
back as far as 1858 when Kessler described a case of congenital bronchiectasis [1]. Since then, the honeycomb appearance of the lung was named, variously by different authors, Wabenlunge (honeycomb lung), Zystenlunge (cystic lung), Schwammlunge (spongy lung), and Sacklunge (sacculated lung) [1, 2]. In the German literature, honeycomb lung was usu-ally considered a congenital malformation or anomalous development of the lung with bron-chiectasis [2] (Fig. 1). It seems that the term “honeycomb lung” was not applied to chronic interstitial pneumonia in Germany.
In the first half of the 20th century, the idea of idiopathic pulmonary fibrosis (IPF) was not yet established, and only occasional case reports were found, in which the authors called their cases different names or only re-ported the clinical and pathologic findings [3–6]. The famous report by Hamman and Rich [3], which initially appeared in 1935, did not use the term “honeycomb lung.” In the subsequent English literature, cases of presumed IPF were reported under the name bronchiolar emphysema [5], pulmonary muscular hyperplasia [4], or cystic pulmo-nary cirrhosis [6]. Originating in the Ger-man literature, these names were translated into English and were discussed as a rare and new disease entity [7, 8]. Sibert and Fisher
Keywords: CT, honeycomb lung, idiopathic interstitial pneumonia, interstitial lung disease
DOI:10.2214/AJR.10.4873
Received April 29, 2010; accepted after revision August 28, 2010.
OBJECTIVE. Originally used to describe the macroscopic appearance of various patho-logic processes with multiple cysts, honeycomb lung is now the term used to describe end-stage pulmonary fibrosis. The purpose of this article is to discuss the history and imaging of honeycomb lung.
CONCLUSION. Honeycomb lung is considered one of the important CT findings in usual interstitial pneumonia. An additional challenge for radiologists is that different patho-logic processes can mimic honeycomb lung. Therefore, a precise understanding of honey-comb lung is necessary.
Arakawa and HonmaImaging of Honeycomb Lung
Cardiopulmonary ImagingReview
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
774 AJR:196, April 2011
Arakawa and Honma
ing the diseases in the way we do now and partly because of the macroscopic similar-ity of various cystic lung diseases. It was not until 1965 that honeycomb lung was limited to chronic interstitial pneumonia when Mey-er and Liebow [11] suggested honeycombing
as “the end-stage of chronic interstitial pneu-monia no matter what the etiology.”
Pathologic DescriptionIn the initial detailed description of honey-
comb lung, Heppleston [10] stated that the es-
sential change is the obliteration of bronchioles by fibrosis or granulomata and compensatory dilatation of neighboring bronchioles, which forms the honeycomb appearance [10]. These changes were the consistent pathologic finding of honeycomb lung, irrespective of the cause.
A
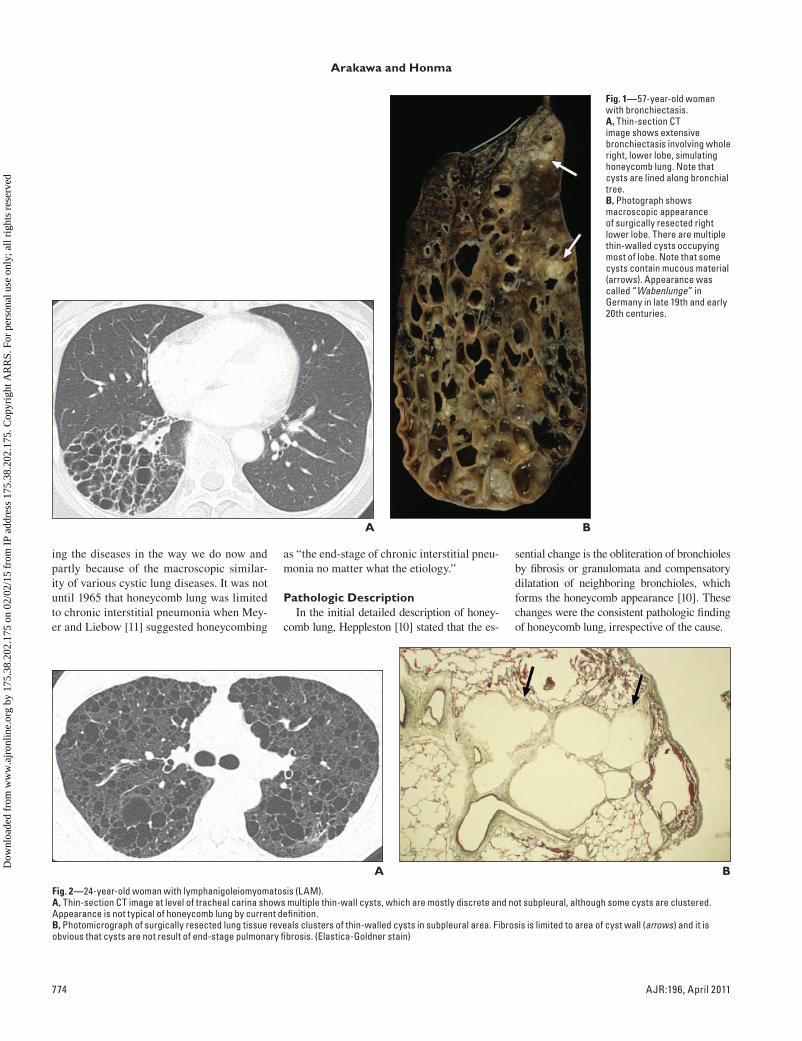
Fig. 1—57-year-old woman with bronchiectasis.A, Thin-section CT image shows extensive bronchiectasis involving whole right, lower lobe, simulating honeycomb lung. Note that cysts are lined along bronchial tree.B, Photograph shows macroscopic appearance of surgically resected right lower lobe. There are multiple thin-walled cysts occupying most of lobe. Note that some cysts contain mucous material (arrows). Appearance was called “Wabenlunge” in Germany in late 19th and early 20th centuries.
B
A
Fig. 2—24-year-old woman with lymphanigoleiomyomatosis (LAM).A, Thin-section CT image at level of tracheal carina shows multiple thin-wall cysts, which are mostly discrete and not subpleural, although some cysts are clustered. Appearance is not typical of honeycomb lung by current definition.B, Photomicrograph of surgically resected lung tissue reveals clusters of thin-walled cysts in subpleural area. Fibrosis is limited to area of cyst wall (arrows) and it is obvious that cysts are not result of end-stage pulmonary fibrosis. (Elastica-Goldner stain)
BDow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:196, April 2011 775
Imaging of Honeycomb Lung
In another study, honeycomb lung in scle-roderma, dermatomyositis, Langerhans cell histiocytosis, tuberculosis, lipoid pneumo-nia, sarcoidosis, and IPF was studied by con-tinuous sections of three resected lungs and eight autopsy lungs, which were displayed in three dimensions through photographic re-construction [12]. The authors found that the pathologic process in the honeycomb area was independent of the original disease and was fundamentally diffuse saccular or cystic bronchiolectasis involving the whole lobule, especially the terminal and respiratory bron-chioles. The other bronchioles showed ab-normal changes in direction, branching pat-tern, and abrupt amputation, and there were anastomoses between anatomically indepen-dent bronchioles. These authors insisted that the primary abnormality of honeycomb lung is the fibrous or granulomatous process of al-veoli and ducts, which causes the bronchi-oles to dilate or amputate.
Radiologic DescriptionThe early radiologic description of honey-
comb lung also indicated the various causes and pathophysiology [13]. Honeycomb lung, defined by “visualization of multiple lucent shadows from 2 to 10 mm in size” on a chest radiograph, included not only diffuse inter-stitial fibrosis but also bronchiectasis and even bullous emphysema [13]. The radiolog-ic concept changed later than the patholog-ic one. In the 1970s, the concept gradually changed. Reed and Reeder [14] listed cys-tic bronchiectasis, eosinophilic granuloma,
pneumoconiosis, and sarcoidosis in addition to idiopathic pulmonary fibrosis (Hamman-Rich) as the common lung diseases in their gamut of honeycomb lung. However, Felson [15] emphasized interstitial fibrosis as the basis of honeycomb lung and excluded cys-tic bronchiectasis and bullous emphysema from its definition. Genereux [16] discussed honeycomb lung from the standpoint of the end stage of interstitial lung disease of vari-ous causes. This idea coincides with that of Meyer and Liebow [11], who believed that the lung can respond only in a stereotyped manner to a variety of insults. Therefore, various lung diseases can result in end-stage lung (honeycomb lung), which is “charac-terized by cystic spaces of variable size and extent and is caused by alveolar septal dis-solution, bronchiolectasis, and obstructive
emphysema.” Significantly, these descrip-tions were in the era of the chest radiograph, when the macroscopic appearance of the lung was imaged imprecisely and thus had substantial limitations.
Recent Definition of Honeycomb LungPathology
The Fleischner Society has recently re-vised its glossary terms, in which the patho-logic definition of honeycomb lung follows that of Genereux [16] as “destroyed and fi-brotic lung tissue containing numerous cystic airspaces with thick fibrous walls, represent-ing the late stage of various lung diseases, with complete loss of acinar architecture” [17]. Katzenstein [18] stated that honeycomb lung “has a characteristic gross appearance, with relatively uniformly sized cysts…that
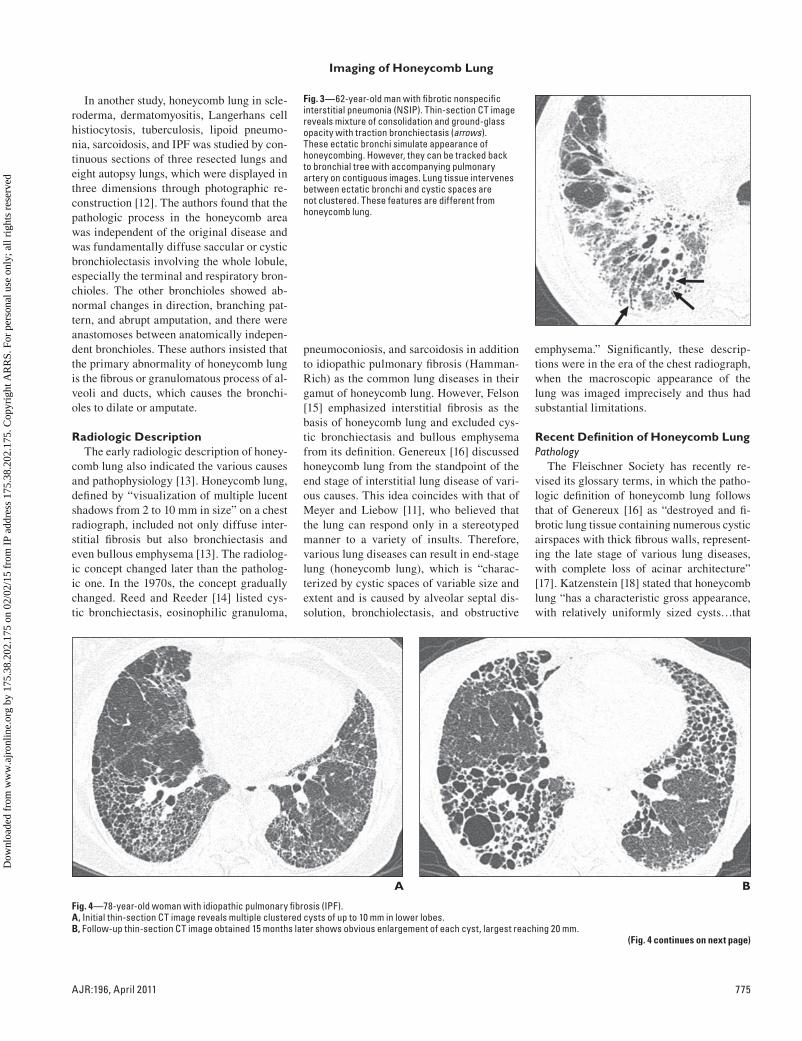
Fig. 3—62-year-old man with fibrotic nonspecific interstitial pneumonia (NSIP). Thin-section CT image reveals mixture of consolidation and ground-glass opacity with traction bronchiectasis (arrows). These ectatic bronchi simulate appearance of honeycombing. However, they can be tracked back to bronchial tree with accompanying pulmonary artery on contiguous images. Lung tissue intervenes between ectatic bronchi and cystic spaces are not clustered. These features are different from honeycomb lung.
A
Fig. 4—78-year-old woman with idiopathic pulmonary fibrosis (IPF).A, Initial thin-section CT image reveals multiple clustered cysts of up to 10 mm in lower lobes.B, Follow-up thin-section CT image obtained 15 months later shows obvious enlargement of each cyst, largest reaching 20 mm.
(Fig. 4 continues on next page)
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
776 AJR:196, April 2011
Arakawa and Honma
C
E
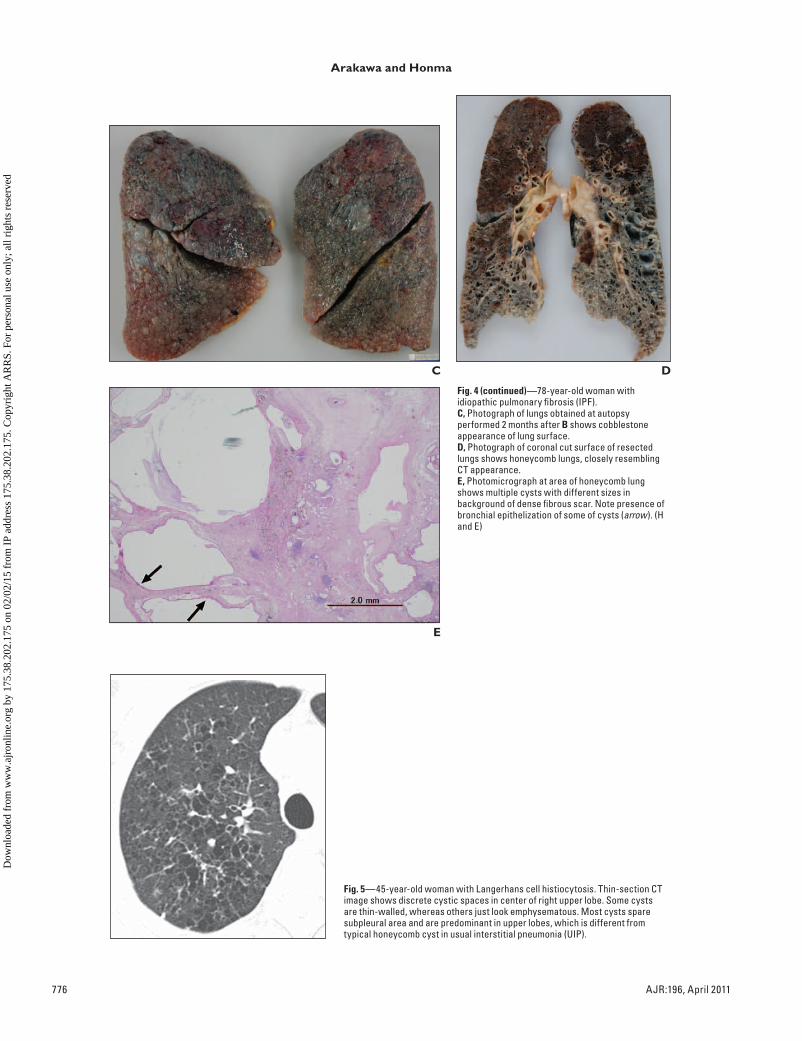
Fig. 4 (continued)—78-year-old woman with idiopathic pulmonary fibrosis (IPF).C, Photograph of lungs obtained at autopsy performed 2 months after B shows cobblestone appearance of lung surface.D, Photograph of coronal cut surface of resected lungs shows honeycomb lungs, closely resembling CT appearance.E, Photomicrograph at area of honeycomb lung shows multiple cysts with different sizes in background of dense fibrous scar. Note presence of bronchial epithelization of some of cysts (arrow). (H and E)
D
Fig. 5—45-year-old woman with Langerhans cell histiocytosis. Thin-section CT image shows discrete cystic spaces in center of right upper lobe. Some cysts are thin-walled, whereas others just look emphysematous. Most cysts spare subpleural area and are predominant in upper lobes, which is different from typical honeycomb cyst in usual interstitial pneumonia (UIP).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:196, April 2011 777
Imaging of Honeycomb Lung
are set in a background of dense scarring” and “microscopically…honeycomb lung is characterized by enlarged airspaces sur-rounded by fibrosis and lined by bronchio-lar or hyperplastic alveolar epithelium. The combination of parenchymal collapse…and collagen deposition accounts for the major manifestation of this lesion.” According to Katzenstein, honeycomb lung is nonspecific as to cause, and a diverse group of diseas-es can lead to honeycombing (idiopathic in-terstitial pneumonia [IIP], diffuse alveolar damage, asbestosis, interstitial granuloma-tous diseases, and eosinophilic granuloma), which corresponds to the previous under-standing [11, 18]. In another pathology book, Churg [19] described honeycomb lung as “a
variable combination of thick-walled cysts…, which may range from a few millimeters to a few centimeters in diameter, and intervening solid fibrous tissue.” He continued, “In ad-dition to specific diffuse diseases, localized scars of many causes can appear as honey-combed lung,” which indicates a rather non-specific pathologic condition [19].
Pathologically, the Fleischner Society defi-nition indicates, “the cysts range in size from a few millimeters to several centimeters in diameter,” so they are macroscopically iden-tifiable [17]. Some researchers use the term “microscopic honeycombing” to describe 1- to 2-mm dilated bronchioles surrounded by airless fibrotic lung on a pathologic specimen [20]. On thin-section CT images, the area cor-
responds to markedly increased lung attenua-tion with dilated bronchioles and is therefore different from the macroscopic honeycomb lung. Whether the pathologic process that oc-curs in the “microscopic honeycombing” has a similar clinical and pathophysiologic signif-icance to that of (macroscopic) honeycomb lung is still to be determined.
RadiologyA recent definition of honeycomb lung in
radiology is based on thin-section CT, which can image the lungs close to their macroscopic appearance [21]. The initial definition by the Fleischner Society, which was published in 1984, stated that honeycomb lung is “a num-ber of closely approximated ring shadows
A
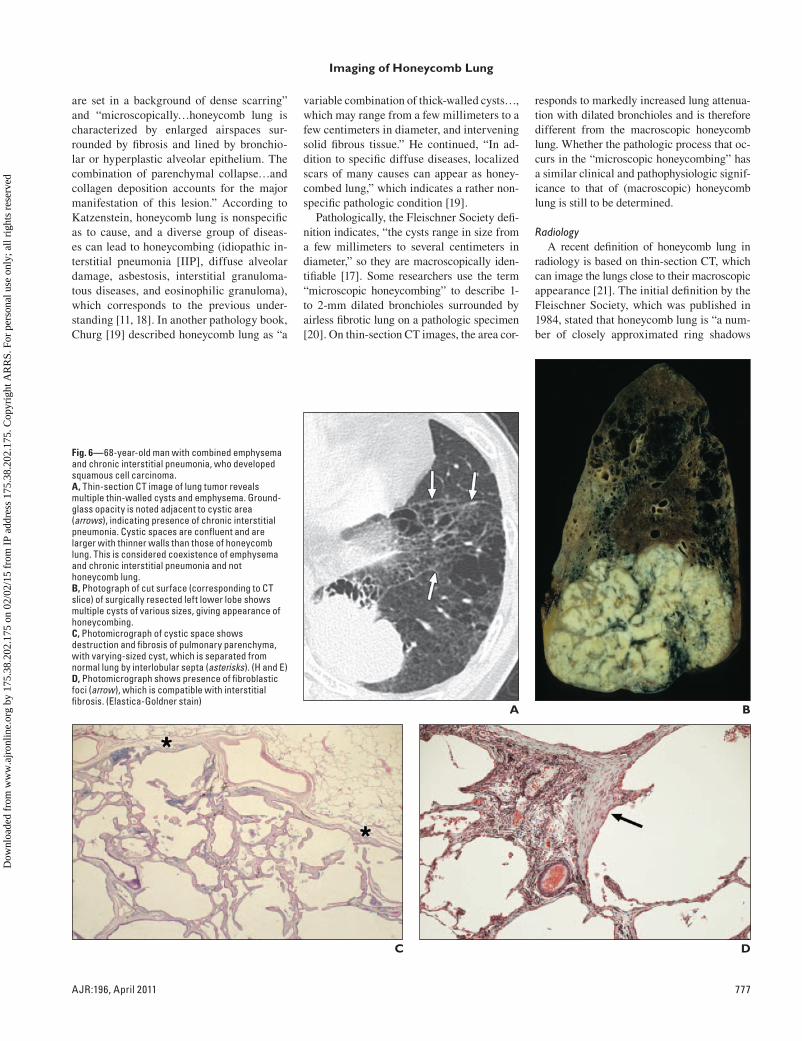
Fig. 6—68-year-old man with combined emphysema and chronic interstitial pneumonia, who developed squamous cell carcinoma.A, Thin-section CT image of lung tumor reveals multiple thin-walled cysts and emphysema. Ground-glass opacity is noted adjacent to cystic area (arrows), indicating presence of chronic interstitial pneumonia. Cystic spaces are confluent and are larger with thinner walls than those of honeycomb lung. This is considered coexistence of emphysema and chronic interstitial pneumonia and not honeycomb lung.B, Photograph of cut surface (corresponding to CT slice) of surgically resected left lower lobe shows multiple cysts of various sizes, giving appearance of honeycombing.C, Photomicrograph of cystic space shows destruction and fibrosis of pulmonary parenchyma, with varying-sized cyst, which is separated from normal lung by interlobular septa (asterisks). (H and E)D, Photomicrograph shows presence of fibroblastic foci (arrow), which is compatible with interstitial fibrosis. (Elastica-Goldner stain)
B
C D
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

778 AJR:196, April 2011
Arakawa and Honma
representing air spaces 5–10 mm in diameter with walls 2–3 mm thick…whose occurrence implies end-stage lung” [22], which is in con-cert with the statement by Meyer and Liebow [11] and Genereux [16]. The second statement by the Fleischner Society, which was published in 1996, said, “Clustered cystic air space, usu-ally of comparable diameters on the order of 0.3–1.0 cm but as much as 2.5 cm, usually is subpleural and characterized by well-defined walls, which are often thick—a CT feature of diffuse pulmonary fibrosis” [23]. These earlier definitions, which were in the era of the chest radiograph in the first version and of CT in the second version, are almost the same except for the size and location. In the latest version from the Fleischner Society, honeycomb lung is defined as “clustered cystic air spaces, typi-cally of comparable diameters on the order of 3–10 mm but occasionally as large as 2.5 cm…usually subpleural and characterized by well-defined walls” [17]. The size and wall thick-ness of the cysts vary among the authors who use the term. However, “the cystic air spaces of honeycomb lung tend to share walls” [24]. This means that traction bronchiolectasis with intervening lung should not be called honey-combing (Fig. 3). Because of the small size of the cyst, diagnosis should be performed with thin-section CT [25]. Although different dis-ease processes result in the same pathologic and radiologic appearance, recent understand-ing indicates that “honeycombing is often con-sidered specific for pulmonary fibrosis and is an important criterion in the diagnosis of usu-al interstitial pneumonia (UIP),” and thus “the term should be used with care [because] it may directly impact patient care” [17].
The latest definition emphasizes the im-portance of honeycombing as the diagnostic criterion of UIP. This emphasis originated from the recent consensus statement about idiopathic pulmonary fibrosis published in 2000 by American Thoracic Society and Eu-ropean Respiratory Society, which empha-sized the clinical relevance of discriminating UIP from other IIP [25]. Among idiopathic interstitial pneumonia, IPF is a progressive disease, often with acute exacerbation, and shows far worse prognosis than other chronic interstitial pneumonia [26]. Although a new antifibrotic drug has emerged as a possible treatment option for IPF [27], the prognosis is still regarded as poor [28].
Progression of Honeycomb LungBecause honeycomb lung is the end stage
of interstitial pneumonia, there must be an ab-normality that precedes it. In the case of UIP, honeycomb lung is preceded by the presence of patchy ground-glass opacity and reticu-lation within a secondary lobule [29]. Over time, intralobular reticulation increases and traction bronchiolectasis gradually appears in the area of the ground-glass opacity while the ground-glass opacity diminishes and finally results in honeycombing [29, 30]. The earliest CT abnormality of UIP is poorly understood. In one report of 14 cases of silicosis that de-veloped chronic interstitial pneumonia with honeycombing, the earliest abnormality was faint ground-glass opacity or, less frequently, coarse reticulation [30]. However, this study was performed with 10-mm slice thickness.
The speed of progression of honeycomb lung is poorly understood. In a series of 29 IPF
patients, the progression of honeycomb lung ranged from 0% to 11% of the lungs per month (median, 0.4%) and was fastest in the low-er lobes [29]. In another series of 14 patients with chronic interstitial pneumonia and silico-sis observed for a median of 15.4 years, nor-mal or near-normal lung progressed to hon-eycomb lung within a median of 12.1 years (range, 3.7–19.1 years) [30]. It is presumed that a long asymptomatic period exists before honeycomb lung develops and the patient be-comes symptomatic. With the common use of CT examinations in this era of MDCT, cases of IPF without honeycomb lung are expected to be increasingly found, which challenges radiologists in CT diagnosis.
Although most cases of honeycomb lung are seen in chronic lung disease, it can also occur in a minority of patients with acute interstitial pneumonia and diffuse alveolar damage [31, 32]. This disease is progressive by the day or week, and the result is often fa-tal. Honeycomb lung is not the initial feature, but it can occur as early as 1 week after the onset of symptoms [31].
The size of the honeycomb cyst usually in-creases during follow-up [33]. In two autopsy series of patients with honeycombing of UIP, stenosis or abrupt angulations of bronchiole and slitlike structures between the cysts and bronchioles were found, which were regard-ed as the causes of progressive enlargement of honeycomb cysts [12, 33] (Fig. 4). In another study of 97 patients with end-stage lung dis-ease, patients underwent paired inspiratory and expiratory volume scanning of the lung, and the size of honeycomb cysts was evaluated using multiplanar reformation [34]. The large
A
Fig. 7—56-year-old man with emphysema who developed interstitial pneumonia during follow-up.A, Thin-section CT image shows emphysema in periphery of right lower lobe. There is minimum increase in lung attenuation associated with emphysematous area.B, Thin-section CT image obtained 5 years later shows cluster of multiple cysts in area of previous emphysema. This appearance mimics honeycomb lung. However, it is not end-stage of chronic fibrosing interstitial pneumonia but superimposition of ground-glass opacity on emphysema.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
AJR:196, April 2011 779
Imaging of Honeycomb Lung
honeycomb cysts (mean, 20.6 mm; SD, 10.7 mm) tended to have thinner walls and did not communicate with the airways and thus did not change in size during forced exhalation, whereas the small cysts (mean, 2.7 mm; SD, 4.3 mm) did have communication with the air-ways and their size changed on expiration [34]. The data suggest that the progressive enlarge-ment of honeycomb cysts is partly due to air trapping by the check-valve mechanism.
Honeycomb Lung as the CT Criterion of UIPHoneycombing is often considered spe-
cific to pulmonary fibrosis and is an impor-
tant criterion in the diagnosis of UIP [17]. By definition, however, it is not the specific CT finding of UIP, although honeycombing is the common finding of UIP.
In previous literature, honeycombing was identified in 41–100% of UIP, depending on the reported series [35–44]. In one report of 168 cases of suspected IIP, the sensitivity and specificity of the presence of honeycombing in the diagnosis of UIP were 90% and 86%, respectively [45]. Nonspecific interstitial pneumonia (NSIP) and desquamative intersti-tial pneumonia (DIP), which are the chronic interstitial pneumonias of IIP and are the im-
portant differential diagnostic considerations, show honeycombing in 0–30% and 4.3–39%, respectively [37, 38, 46–48]. In acute intersti-tial pneumonia, the frequency is lower, rang-ing from 6% to 14% [31, 32, 49].
Honeycomb lung in UIP is usually subpleu-ral and is predominant in posterior and lower lobes [29, 35, 50]. This characteristic distri-bution distinguishes UIP from other diseases with honeycomb lung. In a study of 61 various end-stage lung diseases (26 UIP, nine sarcoido-sis, eight Langerhans cell histiocytosis, five as-bestosis, four silicosis, four chronic hypersensi-tivity pneumonitis, three LAM, one berylliosis,
A
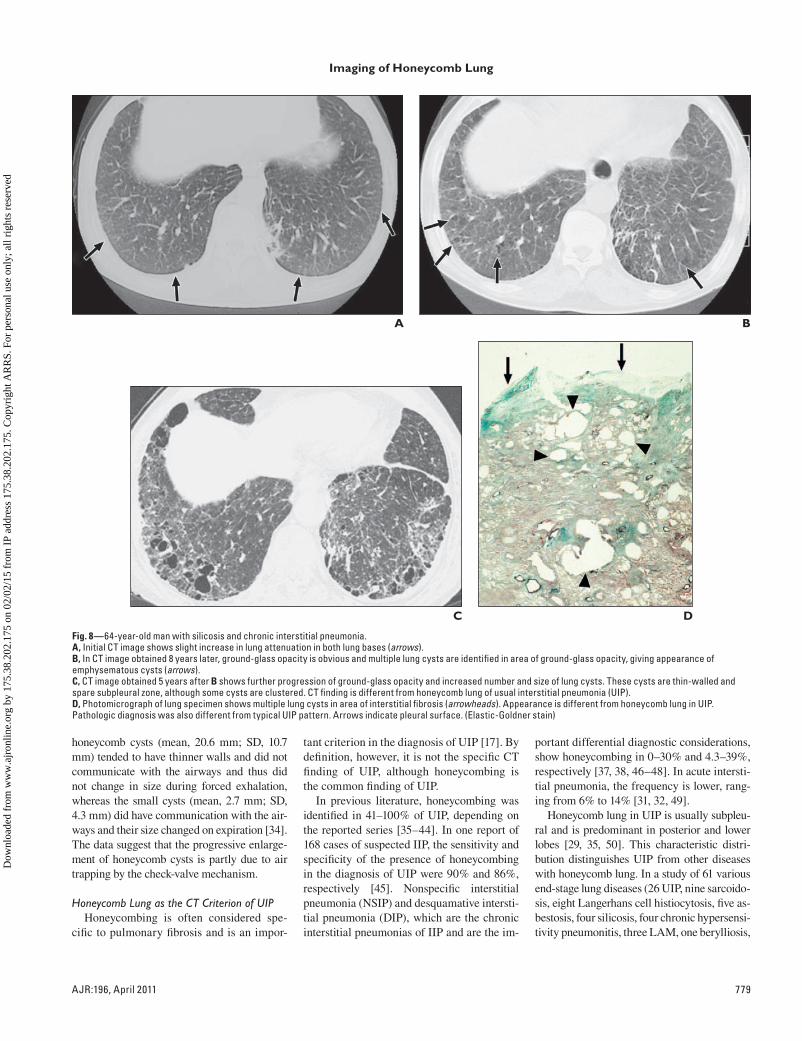
Fig. 8—64-year-old man with silicosis and chronic interstitial pneumonia.A, Initial CT image shows slight increase in lung attenuation in both lung bases (arrows).B, In CT image obtained 8 years later, ground-glass opacity is obvious and multiple lung cysts are identified in area of ground-glass opacity, giving appearance of emphysematous cysts (arrows).C, CT image obtained 5 years after B shows further progression of ground-glass opacity and increased number and size of lung cysts. These cysts are thin-walled and spare subpleural zone, although some cysts are clustered. CT finding is different from honeycomb lung of usual interstitial pneumonia (UIP).D, Photomicrograph of lung specimen shows multiple lung cysts in area of interstitial fibrosis (arrowheads). Appearance is different from honeycomb lung in UIP. Pathologic diagnosis was also different from typical UIP pattern. Arrows indicate pleural surface. (Elastic-Goldner stain)
B
C D
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved
780 AJR:196, April 2011
Arakawa and Honma
and one talcosis), the characteristic distribution of honeycombing made it possible to diagnose UIP in 88% of the cases, with a high degree of confidence in 67% [51] (Fig. 5).
In addition to the distribution, the extent of honeycomb cyst is another important con-sideration when diagnosing UIP. It has been reported that the extent of honeycombing ranged from 3% to 21% of the lung parenchy-ma in UIP [35–44]. On the other hand, the extent of honeycombing in NSIP and DIP is reported as 0.3–3.7% and 0.7–10% of the lung parenchyma, respectively [37, 38, 46–48]. In these reports, both the frequency and extent are significantly higher in UIP than in DIP or NSIP, although there seems to be no threshold that discriminates UIP from other IIP.
Problems in Diagnosing Honeycomb Lung
There are several difficulties in the diagno-sis of honeycomb lung. One is the definition of the terminology and the others are asso-ciated with radiographic diagnosis with CT. The problem of diagnosis originates from the historical change of the concept and the dif-ferent circumstances in which it is made. In the previous literature, honeycombing meant nonspecific cystic pulmonary conditions, in-cluding bronchiectasis and congenital cystic lung disease. However, in the recent litera-ture, its use is limited mostly to the end-stage lung with interstitial fibrosis.
Other problems affect the CT diagnosis of honeycomb lung in cases with chronic intersti-tial pneumonia [52]. Although the definition is straightforward, diagnosing honeycomb lung in IPF or UIP is sometimes not easy for radi-ologists. For instance, in a study of 314 cases
of IPF, the interobserver agreement regarding the presence of honeycomb lung ranged from 0.21 to 0.31, which indicates rather poor agree-ment [36]. This variation could originate from the varied appearance of cystic structures in chronic interstitial pneumonia, in which there can be traction bronchiolectasis, subpleural cysts or bulla, and emphysema, especially of the paraseptal type. Located in the subpleu-ral area, all these structures appear cystic and often have walls. The coexistence of emphy-sema is reported in the subset of patients with IPF, which is rather a common phenomenon because both diseases are associated with cig-arette smoking [53–56]. Although emphyse-ma is pathologically defined as loss of lung parenchyma without fibrosis, fibrosis can co-exist in the area with emphysema [57] (Fig. 6). Although such fibrosis may be different from UIP [58], the presence of this fibrosis can be a risk factor of acute exacerbation during cy-totoxic drug treatment [59] and after pulmo-nary surgery [60].
Emphysema and cystic spaces can be challenging in the presence of overlapping ground-glass opacity [47]. In a study of 34 patients with either UIP or NSIP and em-physema, emphysematous lung or cystic ar-eas were misdiagnosed as honeycombing in three cases [47]. This situation can oc-cur with pneumonia in emphysematous lung but more problematic is the development of chronic interstitial pneumonia in emphyse-matous lung during follow-up (Fig. 7). NSIP and DIP, which show predominantly ground-glass opacity, might show a honeycomb ap-pearance if the abnormality involves the em-physematous area and thus would likely be misdiagnosed as UIP [47].
Furthermore, emphysema and interstitial fibrosis develop and progress simultaneously in the same lung area [61] (Fig. 8). The end result is similar to honeycomb lung, which is often relatively thin walled and presents a di-agnostic challenge to radiologists.
Finally, paraseptal emphysema, which is one of the types of emphysema, has definite walls, is located subpleurally, and is often clustered (Fig. 9). Pathologically, paraseptal emphyse-ma is often accompanied by fibrosis in its walls [62]. There are cases that show paraseptal em-physema in the upper and middle lobes, al-though there is typical honeycomb lung in the lower lobes. In these cases, these differ-ent pathologic processes are often continuous with each other in the subpleural zone. Thus, differentiating the two is almost impossible.
It should be kept in mind that honeycomb lung is the end stage of pulmonary fibrosis. Thus, the development of ground-glass opac-ity in the area of emphysema should not be called honeycomb lung. However, in cases of the simultaneous progression of fibrosis and airspace enlargement, it might be difficult to reject the term honeycomb lung.
Future of CT Diagnosis of Honeycomb Lung
Because the term “honeycomb lung” is close-ly linked with the concept of the disease and with the classification of idiopathic interstitial pneumonia, the definition and clinical mean-ing of honeycomb lung have changed and may change from the present definition in the future. In the meantime, it is important to use the term in consensus, and when it is used, interpreters should have a unanimous opinion and image of what is meant by honeycomb lung.
A
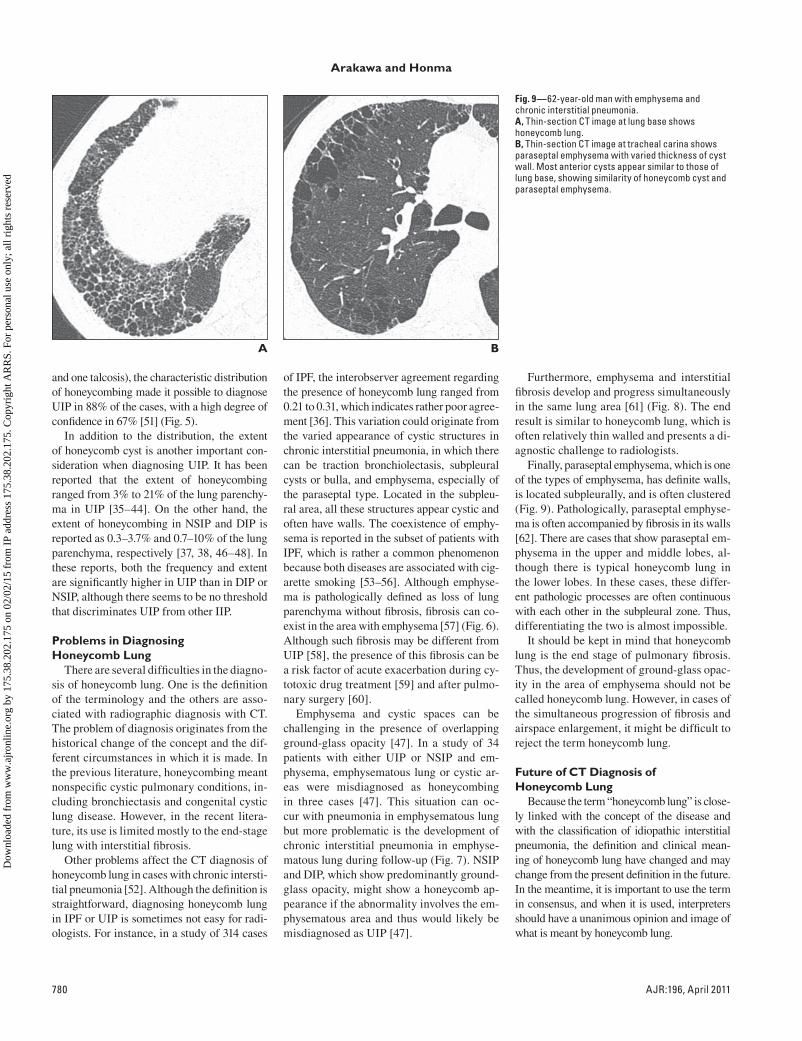
Fig. 9—62-year-old man with emphysema and chronic interstitial pneumonia.A, Thin-section CT image at lung base shows honeycomb lung.B, Thin-section CT image at tracheal carina shows paraseptal emphysema with varied thickness of cyst wall. Most anterior cysts appear similar to those of lung base, showing similarity of honeycomb cyst and paraseptal emphysema.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:196, April 2011 781
Imaging of Honeycomb Lung
Disagreement concerning the CT diagno-sis of honeycomb lung could partly be ex-plained by the lack of prespecified consensus, and thus reference images, such as the Inter-national Labor Office classification of pneu-moconiosis, are considered to improve the interobserver agreement [36]. Actually, refer-ence images should be used so that we have a unanimous CT diagnosis of honeycomb lung in diagnosing IPF. Because the final goal is to identify those patients who are likely to show progressive disease and die within sev-eral years, the prespecified pattern of honey-combing should be revised on the basis of the results of the prospective observation that will be undertaken, depending on the prespecified consensus. The revision is an urgent task for radiologists considering that the presence and extent of honeycombing is the most important thin-section CT finding in the correct diagno-sis of UIP [39–41, 43, 44, 47].
References 1. Bargon G. Zur Pathogenese der Wabenlunge. Be-
itr Pathol Anat 1955; 115:452–469
2. Otto A, Otto H. Einiges uber Zysten und Waben-
lungen. Z Gesamte Inn Med 1956; 11:505–511
3. Hamman L, Rich A. Fulminating diffuse intersti-
tial fibrosis of the lungs. Trans Am Clin Climatol
Assoc 1935; 151:154–163
4. Rubenstein L, Gutstein WH, Lepow H. Pulmo-
nary muscular hyperplasia (muscular cirrhosis of
the lungs). Ann Intern Med 1955; 42:36–43
5. Siebert FT, Fisher ER. Bronchiolar emphysema:
so-called muscular cirrhosis of the lungs. Am J
Pathol 1957; 33:1137–1161
6. Hirshfield HJ, Krainer L, Coe GC. Cystic pulmo-
nary cirrhosis (bronchiolar emphysema). Dis
Chest 1962; 42:107–110
7. von Stossel E. Uber Muskulare Cirrhose der
Lunge. Beitr Klin Tuberk 1937; 90:429–442
8. Davidsohn C. Uber Muskulare Lungencirrhose.
Berl Klinwchnschr 1907; 44:33
9. Oswald N, Parkinson T. Honeycomb lungs. QJM
1949; 18:1–20
10. Heppleston AG. The pathology of honeycomb
lung. Thorax 1956; 11:77–93
11. Meyer EC, Liebow AA. Relationship of intersti-
tial pneumonia honeycombing and atypical epi-
thelial proliferation to cancer of the lung. Cancer
1965; 18:322–351
12. Pimentel JC. Tridimensional photographic recon-
struction in a study of the pathogenesis of honey-
comb lung. Thorax 1967; 22:444–452
13. Johnson TH Jr. Radiology and honeycomb lung
disease. Am J Roentgenol Radium Ther Nucl Med
1968; 104:810–821
14. Reed JC, Reeder MM. Honeycomb lung (intersti-
tial fibrosis). JAMA 1975; 231:646–647
15. Felson B. Chest Roentgenology. Philadelphia, PA:
Saunders, 1973
16. Genereux GP. The end-stage lung: pathogenesis,
pathology, and radiology. Radiology 1975;
116:279–289
17. Hansell DM, Bankier AA, MacMahon H, McLoud
TC, Muller NL, Remy J. Fleischner Society: glos-
sary of terms for thoracic imaging. Radiology
2008; 246:697–722
18. Katzenstein AL. Idiopathic interstitial pneumo-
nia. In: Katzenstein AL. Kazenstein and Askin’s
surgical pathology of non-neoplastic lung dis-
ease. Philadelphia, PA: Saunders, 2006:51–84
19. Churg AM. Lung biopsy, lung resection, and autopsy
lung specimens. In: Churg AM, Myers JL, Tazelaar
HD, Wright JL, eds. Thurlbech’s pathology of the
lung. New York, NY: Thieme, 2005:95–108
20. Nishimura K, Kitaichi M, Izumi T, Nagai S, Ka-
naoka M, Itoh H. Usual interstitial pneumonia:
histologic correlation with high-resolution CT.
Radiology 1992; 182:337–342
21. Murata K, Khan A, Herman PG. Pulmonary pa-
renchymal disease: evaluation with high-resolu-
tion CT. Radiology 1989; 170:629–635
22. Tuddenham WJ. Glossary of terms for thoracic
radiology: recommendations of the Nomenclature
Committee of the Fleischner Society. AJR 1984;
143:509–517
23. Austin JH, Muller NL, Friedman PJ, et al. Glos-
sary of terms for CT of the lungs: recommenda-
tions of the Nomenclature Committee of the
Fleischner Society. Radiology 1996; 200:327–331
24. Webb WR, Muller NL, Naidich DP. Standardized
terms for high-resolution computed tomography
of the lung: a proposed glossary. J Thorac Imag-
ing 1993; 8:167–175
25. Idiopathic pulmonary fibrosis: diagnosis and
treatment—international consensus statement of
the American Thoracic Society and the European
Respiratory Society. Am J Respir Crit Care Med
2000; 161:646–664
26. Kondoh Y, Taniguchi H, Kawabata Y, Yokoi T,
Suzuki K, Takagi K. Acute exacerbation in idio-
pathic pulmonary fibrosis: analysis of clinical and
pathologic findings in three cases. Chest 1993;
103:1808–1812
27. Taniguchi H, Ebina M, Kondoh Y, et al. Pirfeni-
done in idiopathic pulmonary fibrosis. Eur Respir
J 2010; 35:821–829
28. Collard HR, Moore BB, Flaherty KR, et al. Acute
exacerbations of idiopathic pulmonary fibrosis.
Am J Respir Crit Care Med 2007; 176:636–643
29. Akira M, Sakatani M, Ueda E. Idiopathic pulmo-
nary fibrosis: progression of honeycombing at
thin-section CT. Radiology 1993; 189:687–691
30. Arakawa H, Fujimoto K, Honma K, et al. Progres-
sion from near-normal to end-stage lungs in
chronic interstitial pneumonia related to silica ex-
posure: long-term CT observations. AJR 2008;
191:1040–1045
31. Johkoh T, Muller NL, Taniguchi H, et al. Acute
interstitial pneumonia: thin-section CT findings
in 36 patients. Radiology 1999; 211:859–863
32. Ichikado K, Suga M, Muller NL, et al. Acute in-
terstitial pneumonia: comparison of high-resolu-
tion computed tomography findings between sur-
vivors and nonsurvivors. Am J Respir Crit Care
Med 2002; 165:1551–1556
33. Mino M, Noma S, Kobashi Y, Iwata T. Serial
changes of cystic air spaces in fibrosing alveolitis:
a CT–pathological study. Clin Radiol 1995;
50:357–363
34. Johkoh T, Muller NL, Ichikado K, et al. Respira-
tory change in size of honeycombing: inspiratory
and expiratory spiral volumetric CT analysis of 97
cases. J Comput Assist Tomogr 1999; 23:174–180
35. Hunninghake GW, Lynch DA, Galvin JR, et al.
Radiologic findings are strongly associated with a
pathologic diagnosis of usual interstitial pneumo-
nia. Chest 2003; 124:1215–1223
36. Lynch DA, David Godwin J, Safrin S, et al. High-
resolution computed tomography in idiopathic
pulmonary fibrosis: diagnosis and prognosis. Am
J Respir Crit Care Med 2005; 172:488–493
37. Silva CI, Muller NL, Hansell DM, Lee KS, Nich-
olson AG, Wells AU. Nonspecific interstitial
pneumonia and idiopathic pulmonary fibrosis:
changes in pattern and distribution of disease over
time. Radiology 2008; 247:251–259
38. Tsubamoto M, Muller NL, Johkoh T, et al. Patho-
logic subgroups of nonspecific interstitial pneu-
monia: differential diagnosis from other idiopath-
ic interstitial pneumonias on high-resolution
computed tomography. J Comput Assist Tomogr
2005; 29:793–800
39. Elliot TL, Lynch DA, Newell JD Jr, et al. High-
resolution computed tomography features of non-
specific interstitial pneumonia and usual intersti-
tial pneumonia. J Comput Assist Tomogr 2005;
29:339–345
40. Johkoh T, Muller NL, Cartier Y, et al. Idiopathic
interstitial pneumonias: diagnostic accuracy of
thin-section CT in 129 patients. Radiology 1999;
211:555–560
41. Nagai S, Kitaichi M, Itoh H, Nishimura K, Izumi
T, Colby T. Idiopathic nonspecific interstitial
pneumonia/fibrosis: comparison with idiopathic
pulmonary fibrosis and BOOP. Eur Respir J 1998;
12:1010–1019
42. Sumikawa H, Johkoh T, Colby TV, et al. Com-
puted tomography findings in pathological usual
interstitial pneumonia: relationship to survival.
Am J Respir Crit Care Med 2008; 177:433–439
43. Sumikawa H, Johkoh T, Ichikado K, et al. Usual
interstitial pneumonia and chronic idiopathic in-
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

782 AJR:196, April 2011
Arakawa and Honma
terstitial pneumonia: analysis of CT appearance
in 92 patients. Radiology 2006; 241:258–266
44. Shin KM, Lee KS, Chung MP, et al. Prognostic
determinants among clinical, thin-section CT,
and histopathologic findings for fibrotic idiopathic
interstitial pneumonias: tertiary hospital study.
Radiology 2008; 249:328–337
45. Flaherty KR, Toews GB, Travis WD, et al. Clini-
cal significance of histological classification of
idiopathic interstitial pneumonia. Eur Respir J
2002; 19:275–283
46. Travis WD, Hunninghake G, King TE Jr, et al.
Idiopathic nonspecific interstitial pneumonia: re-
port of an American Thoracic Society project. Am
J Respir Crit Care Med 2008; 177:1338–1347
47. Akira M, Inoue Y, Kitaichi M, Yamamoto S, Arai
T, Toyokawa K. Usual interstitial pneumonia and
nonspecific interstitial pneumonia with and with-
out concurrent emphysema: thin-section CT find-
ings. Radiology 2009; 251:271–279
48. Hartman TE, Primack SL, Kang EY, et al. Dis-
ease progression in usual interstitial pneumonia
compared with desquamative interstitial pneumo-
nia: assessment with serial CT. Chest 1996;
110:378–382
49. Primack SL, Hartman TE, Ikezoe J, Akira M,
Sakatani M, Muller NL. Acute interstitial pneu-
monia: radiographic and CT findings in nine pa-
tients. Radiology 1993; 188:817–820
50. Nagao T, Nagai S, Hiramoto Y, et al. Serial evalu-
ation of high-resolution computed tomography
findings in patients with idiopathic pulmonary fi-
brosis in usual interstitial pneumonia. Respiration
2002; 69:413–419
51. Primack SL, Hartman TE, Hansell DM, Muller
NL. End-stage lung disease: CT findings in 61 pa-
tients. Radiology 1993; 189:681–686
52. Galvin JR, Frazier AA, Franks TJ. Collaborative
radiologic and histopathologic assessment of fi-
brotic lung disease. Radiology 2010; 255:692–706
53. Cottin V, Nunes H, Brillet PY, et al. Combined pul-
monary fibrosis and emphysema: a distinct under-
recognised entity. Eur Respir J 2005; 26:586–593
54. Grubstein A, Bendayan D, Schactman I, Cohen
M, Shitrit D, Kramer MR. Concomitant upper-
lobe bullous emphysema, lower-lobe interstitial
fibrosis and pulmonary hypertension in heavy
smokers: report of eight cases and review of the
literature. Respir Med 2005; 99:948–954
55. Doherty MJ, Pearson MG, O’Grady EA, Pellegrini
V, Calverley PM. Cryptogenic fibrosing alveolitis
with preserved lung volumes. Thorax 1997;
52:998–1002
56. Wiggins J, Strickland B, Turner-Warwick M.
Combined cryptogenic fibrosing alveolitis and
emphysema: the value of high resolution comput-
ed tomography in assessment. Respir Med 1990;
84:365–369
57. Niewoehner DE, Kleinerman J, Rice DB. Pathologic
changes in the peripheral airways of young cigarette
smokers. N Engl J Med 1974; 291:755–758
58. Katzenstein AL, Mukhopadhyay S, Zanardi C,
Dexter E. Clinically occult interstitial fibrosis in
smokers: classification and significance of a sur-
prisingly common finding in lobectomy speci-
mens. Hum Pathol 2010; 41:316–325
59. Kudoh S, Kato H, Nishiwaki Y, et al. Interstitial
lung disease in Japanese patients with lung can-
cer: a cohort and nested case-control study. Am J
Respir Crit Care Med 2008; 177:1348–1357
60. Kawabata Y, Hoshi E, Murai K, et al. Smoking-
related changes in the background lung of speci-
mens resected for lung cancer: a semiquantitative
study with correlation to postoperative course.
Histopathology 2008; 53:707–714
61. Arakawa H, Johkoh T, Honma K, et al. Chronic
interstitial pneumonia in silicosis and mix-dust
pneumoconiosis: its prevalence and comparison
of CT findings with idiopathic pulmonary fibrosis.
Chest 2007; 131:1870–1876
62. Wright JL. Chronic airflow obstruction. In: Churg
AM, Myers JL, Tazelaar HD, Wright JL, eds.
Thurlbeck’s pathology of the lung. New York,
NY: Thieme, 2005:686–687
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
75.3
8.20
2.17
5 on
02/
02/1
5 fr
om I
P ad
dres
s 17
5.38
.202
.175
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved