Ho Teaching- Acute Cholecystitis
26
Acute cholecystiti s
-
Upload
essa-renandra-virginia -
Category
Documents
-
view
23 -
download
3
description
acute cholecystitis
Transcript of Ho Teaching- Acute Cholecystitis
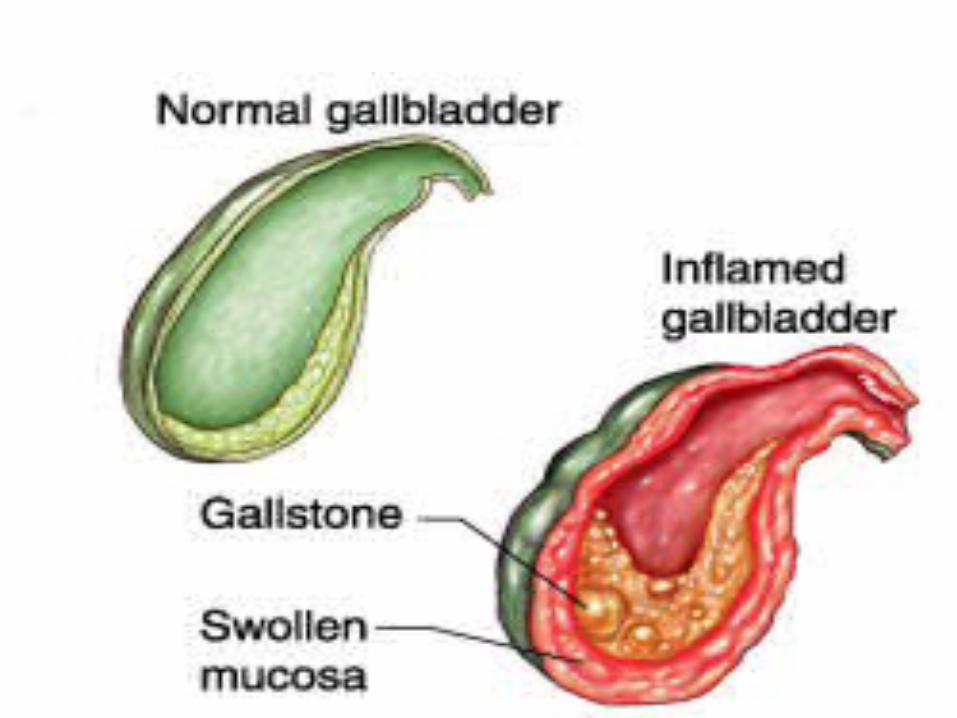
Acute cholecystitis
Inflammation of gallbladder Types:
Calculous 90% of cases
Acalculous
Calculous
• Cholesterol• Pigment (brown/black)
– Less than 30% cholesterol– Black (insoluble bilirubin pigment layers+calcium+Chole)– Brown (calcium+cholesterol)
• Mixed stones
US/Europe 80% cholesterol/mixed stonesAsia80% pigment stones
Acalculous
• Seen in pt with prolong immobilisation• 30% mortality rate, rapid progress• Secondary to– Decrease mesenteric blood flow– Bile stasis– Salmonella infection

Risk Factors 6F
Female Fat Fertile Forty Fatty food intolerance Flatulence
Presenting complain Acute right upper quadrant pain
steady and severe pain, worsened by movement and deep breathing
May radiate to the back Fever Flatulence Nausea and vomiting anorexia
Physical examination Usually appears ill, febrile and tachycardic Jaundice in few cases Guarding Tenderness more over RHC Positive murphy's sign
Investigation
• FBC, LFT, amylase Findings
Leukocytosis Slight elevation of liver enzymes
IMAGING STUDIES (TO CONFIRM DIAGNOSIS)
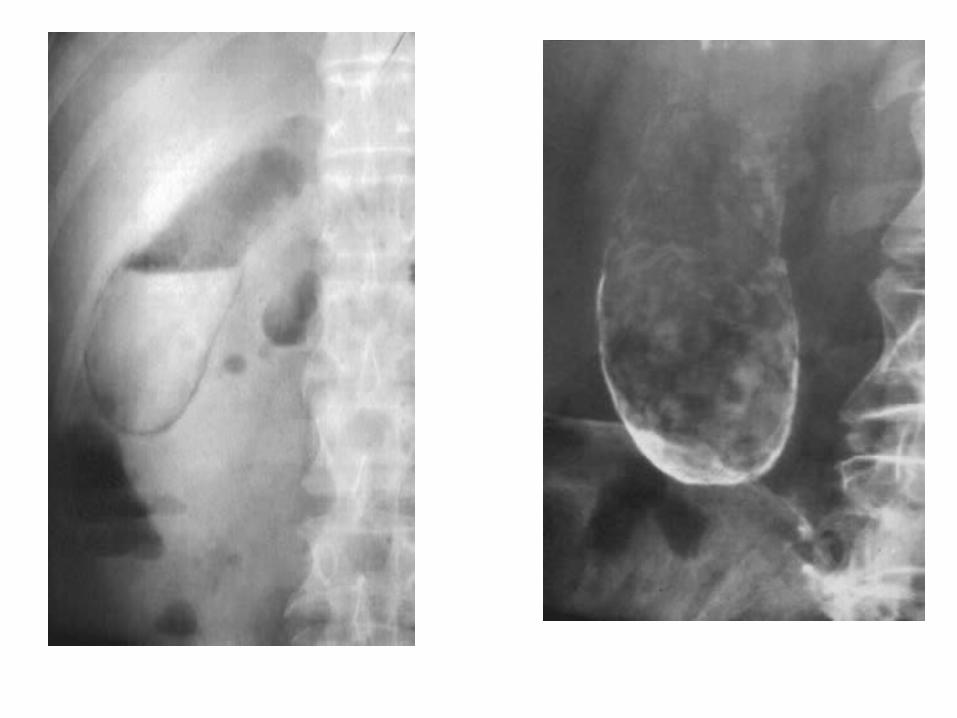
Xrays
• Abdominal radiographs demonstrate 10% of all gallstones
• enlarged GB shadow• Radio-opaque: calcium• Radiolucent: cholesterol stones
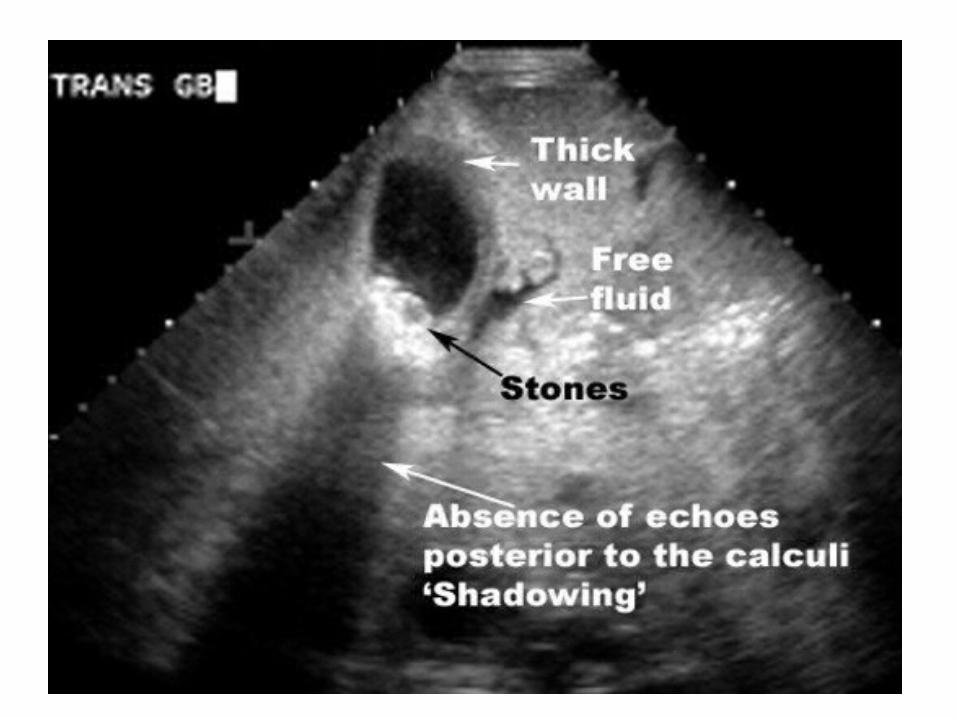
Ultrasound
• Operator dependant• Sensitivity: 96% Specificity: 95%• Suboptimal in fat pt• Findings–+ Murphy’s sign–wall thickening (> 4-5mm)–wall edema

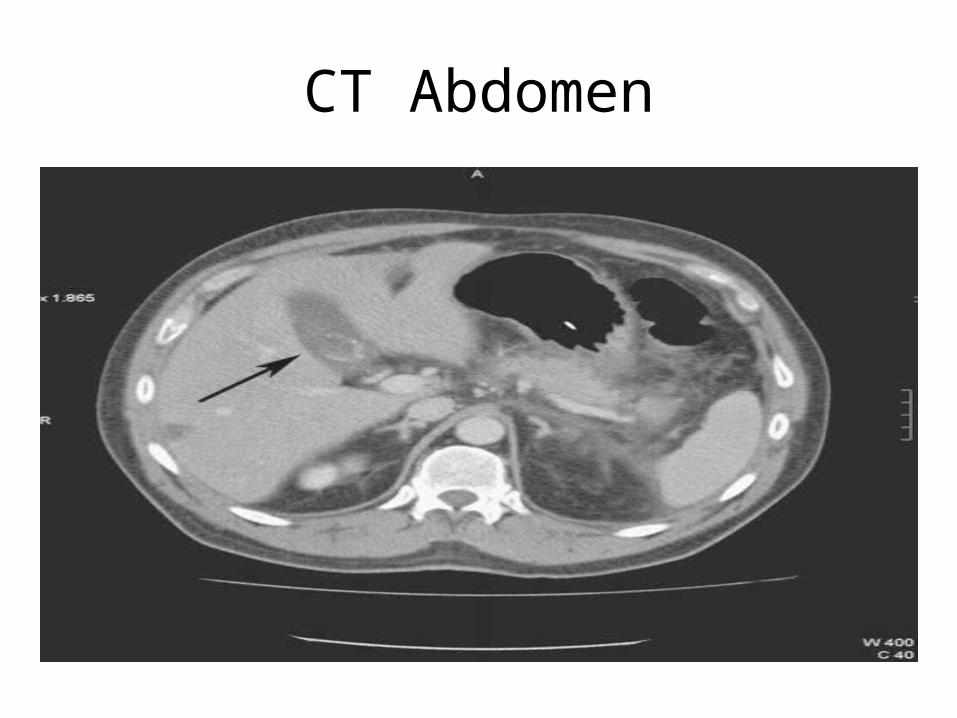
CT Abdomen
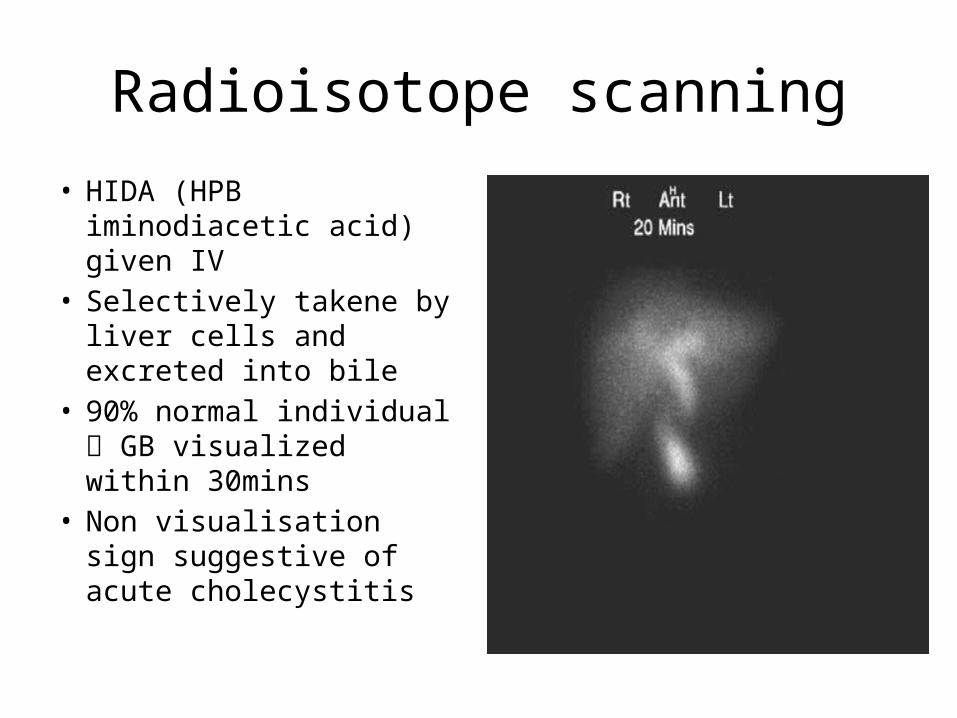
Radioisotope scanning
• HIDA (HPB iminodiacetic acid) given IV
• Selectively takene by liver cells and excreted into bile
• 90% normal individual GB visualized within 30mins
• Non visualisation sign suggestive of acute cholecystitis
Differentials Acute peptic ulcer Acute cholecystitis Acute appendicitis Acute pancreatitis Acute pyelonephritis Pneumonia Fitz-Hugh-curtis syndrome
Treatment
• Symptoms subsides in 90% of cases withh conservative measure
• Four principles–NBM and IVD–Analgesics–Antibiotics–Subsequent Mx
Antibiotics
• The current Sanford guide recommendations include – piperacillin/tazobactam (Zosyn, 3.375 g IV q6h or
4.5 g IV q8h)– ampicillin/sulbactam (Unasyn, 3 g IV q6h)– meropenem (Merrem, 1 g IV q8h)– third-generation cephalosporin plus
metronidazole (Flagyl, 1 g IV loading dose followed by 500 mg IV q6h).
Subsequent Mx
• If inflammation subsiding-> start feeding accordingly
• USG• MRCP for jaundice pt• CT if suspected perforation• Cholecystectomy done electively. High risk pt
can proceed with percutaneous transhepatic cholecystostomy drainage
• Conservative mx to be abandoned if pain and tenderness increase
• Cholecystectomy to be done if pt becoming more septic
Cholecystectomy
• Open and laparascopic• Study done in "Virgen de la Arrixaca" University Hospital,
El Palmar (Murcia), Spain. 1998• Patients 114 underwent LC, and 110 underwent OC• Results
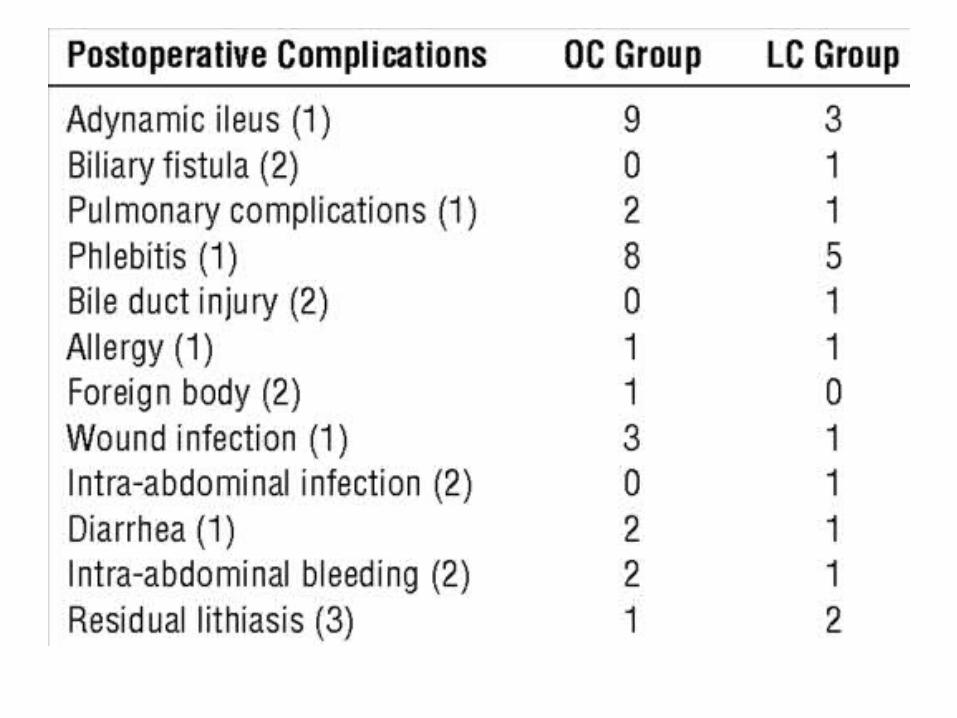
– Conversion from LC to OC was necessary in 15% op.– Complications occurred in 14% of the patients in the LC group
and in 23% of the patients in the OC group, with no significant differences between the 2 groups (P=.06)
– The length of the hospital stay averaged 8.1 days for the OC group and 3.3 days for the LC group (P<.001).
References
• Bailey’s & Love Short Practice of Surgery• UpToDate• Lecture noter General Surgery- Ellis, Harold,
Calne, Roy, Watson, Cristopher• Surgery A Competency Based Companion-
Mann, Barry D• Oxford Handbook of Clinical Surgery• Medscape