HIV infection in Pregnancy. Natural history The principal target=T lymphocytes The principal...
45
HIV infection in HIV infection in Pregnancy Pregnancy รรรรรรรรรรรรรร รรร รรรรรรรรรรรรรร รรร รรรรร รรรรรรร รรรรรรร รรรรร รรรรรรร รรรรรรร รรรรรรรรรรรรรรรรร รรรรรรรรรรรรรรรรร รรรรรรรรรรร รรรรรรรรรรร รรรรรรรรรรรรร รรรรรรรรรรร รรรรรรรรรรรรร รรรรรรรรรรร รรรรรรรรรร รรรรรรรรรร
-
Upload
angelina-williams -
Category
Documents
-
view
220 -
download
5
Transcript of HIV infection in Pregnancy. Natural history The principal target=T lymphocytes The principal...

HIV infection in HIV infection in PregnancyPregnancy
รองศาสตราจารย์ นาย์แพทย์ อต�รองศาสตราจารย์ นาย์แพทย์ อต�วุ�ทธ กมุ�ทมุาศวุ�ทธ กมุ�ทมุาศ
สาขาส�ต�ศาสตรและนร�เวุชวุ�ทย์าสาขาส�ต�ศาสตรและนร�เวุชวุ�ทย์าคณะแพทย์ศาสตร มุหาวุ�ทย์าล ย์คณะแพทย์ศาสตร มุหาวุ�ทย์าล ย์
ธรรมุศาสตรธรรมุศาสตร

NaturalNatural historyhistory The principal target=T lymphocytesThe principal target=T lymphocytes Specific at CD4 surface antigen (receptor Specific at CD4 surface antigen (receptor
for the virus)for the virus) Monocyte-macrophages may be infectedMonocyte-macrophages may be infected Incubation period ; days to weeksIncubation period ; days to weeks Acute retroviral syndrome ; fever, night Acute retroviral syndrome ; fever, night
sweats, fatigue, rash, headache, sweats, fatigue, rash, headache, lymphadenophathy, pharyngitis, myalgias, lymphadenophathy, pharyngitis, myalgias, arthralgias, nausea, vomiting, diarrhea ; arthralgias, nausea, vomiting, diarrhea ; lasts < 10 dayslasts < 10 days

After symptoms abate ; chronic viremiaAfter symptoms abate ; chronic viremiaMedian time = 10 years --- AIDSMedian time = 10 years --- AIDSAIDS; generalized lymphadenopathy, AIDS; generalized lymphadenopathy,
oral hairy leukoplakia, aphthous ulcer, oral hairy leukoplakia, aphthous ulcer, thrombocytopenia, opportunistic thrombocytopenia, opportunistic infections (candida, HSV, TB, CMV, HPV, infections (candida, HSV, TB, CMV, HPV, PCP, toxo), Kaposi sarcoma, non-PCP, toxo), Kaposi sarcoma, non-Hodgkin lymphomaHodgkin lymphoma
Death Death

44
Number of People with Number of People with HIV/AIDS by RegionHIV/AIDS by Region
North America 890,000
Caribbean 330,000
Latin America1.4 million
Western Europe500,000
Sub-Saharan Africa
22.5 million
Eastern Europe &Central Asia
270,000 East Asia & Pacific560,000
South and South East Asia
6.7 million
Australia and New Zealand 12,000
North Africa &Middle East
210,000
Source: UNAIDS/WHO 1998.

VirologyVirology DNA retrovirusDNA retrovirus HIV-1 , HIV-2HIV-1 , HIV-2 Transmission - sexually transmittedTransmission - sexually transmitted
- blood-contaminated - blood-contaminated (e.g., (e.g., blood blood transfusions, shared transfusions, shared needles, needles, contaminated contaminated instruments)instruments)
- maternal to child- maternal to child
-vertical 15-40%-vertical 15-40%
-breast feeding 30-40%-breast feeding 30-40%

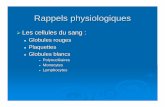
Maternal to child transmission Maternal to child transmission (MTCT)(MTCT)
<14 wk
14-36 wk
36 wk-labor
Intrapartum
1 4 12 8
75 %
uninfected
25 %
infected
4% 16% 50% 30%
Kourtis and colleagues, 2001

Risk factors for vertical Risk factors for vertical transmissiontransmission
1. Preterm birth1. Preterm birth(3.7 relative risk for intrapartum (3.7 relative risk for intrapartum transmission ; Kuhn and assoc 1999)transmission ; Kuhn and assoc 1999)
2. Prolonged membrane rupture2. Prolonged membrane rupture(increase rate from 15 to 25% in ROM > (increase rate from 15 to 25% in ROM > 4 hr ; Landesman and co-workers 1996)4 hr ; Landesman and co-workers 1996)
3. Placental inflammation, 3. Placental inflammation, chorioamnionitis, concurrent syphylis chorioamnionitis, concurrent syphylis (Mwanyumba 2002)(Mwanyumba 2002)

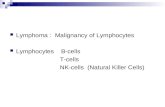
4. Maternal plasma HIV RNA level 4. Maternal plasma HIV RNA level
0
5
10
15
20
25
30
35
1st Qtr 400-30003000-40000 40000-
100000
>100000
1
Most important factor,
HIV RNA viral load > 100000 copies/ml : risk > 30 %
HIV RNA viral load < 400 copies/ml : risk 1 %

5. Stage of disease5. Stage of disease
6. CD4+ T-cell count6. CD4+ T-cell count
7. Mode of delivery7. Mode of delivery
cesarean section vs vaginal deliverycesarean section vs vaginal delivery
8. Breast feeding8. Breast feeding (risk 30-40%)(risk 30-40%)

PregnancyPregnancy on on HIV infectionHIV infection
Pregnancy Pregnancy : slightly : slightly immunosuppressiveimmunosuppressive
: minimal effect on CD4 : minimal effect on CD4 countcount
: minimal effect on HIV : minimal effect on HIV RNA level RNA level
: does not have : does not have significant effect on the significant effect on the clinical or immunological clinical or immunological course of HIV infection course of HIV infection (Minkoff 2003)(Minkoff 2003)
Maternal morbidity and Maternal morbidity and mortalitymortality
: not increased : not increased
HIV infection on pregnancy
•Slightly increase rate of preterm birth
•Slightly increase rate of IUGR
•Slightly increase rate of PROM
•Fetal and neonatal infection
varies from 25-40 percent

Adverse Pregnancy Outcomes and Adverse Pregnancy Outcomes and Relationship to HIV InfectionRelationship to HIV Infection
Pregnancy Pregnancy OutcomeOutcome
Relationship to HIV InfectionRelationship to HIV Infection
Spontaneous Spontaneous abortionabortion
Limited data, but evidence of possible Limited data, but evidence of possible increased riskincreased risk
StillbirthStillbirth No association noted in developed countries; No association noted in developed countries; evidence of increased risk in developing evidence of increased risk in developing countriescountries
Perinatal Perinatal mortalitymortality
No association noted in developed countries, No association noted in developed countries, but data limited; evidence of increased risk in but data limited; evidence of increased risk in developing countriesdeveloping countries
Newborn Newborn mortalitymortality
Limited data in developed countries; evidence Limited data in developed countries; evidence of increased risk in developing countriesof increased risk in developing countries
Intra-uterine Intra-uterine growth growth retardationretardation
Evidence of possible increased riskEvidence of possible increased risk
Anderson 2001.

Adverse Pregnancy Outcomes and Adverse Pregnancy Outcomes and Relationship to HIV Infection (continued)Relationship to HIV Infection (continued)
Pregnancy Pregnancy OutcomeOutcome
Relationship to HIV InfectionRelationship to HIV Infection
Low birth weightLow birth weight Evidence of possible increased riskEvidence of possible increased risk
Preterm deliveryPreterm delivery Evidence of possible increased risk, Evidence of possible increased risk, especially w/ more advanced diseaseespecially w/ more advanced disease
Pre-eclampsiaPre-eclampsia No dataNo data
Gestational diabetesGestational diabetes No dataNo data
AmnionitisAmnionitis Limited data; more recent studies do not Limited data; more recent studies do not suggest an increased risk; some earlier suggest an increased risk; some earlier studies found increased histologic placental studies found increased histologic placental inflammation, particularly in those with inflammation, particularly in those with preterm deliveriespreterm deliveries
OligohydramniosOligohydramnios Minimal dataMinimal data
Fetal malformationFetal malformation No evidence of increased riskNo evidence of increased risk Anderson 2001.

ManagementManagement during during pregnancypregnancy
Therapeutic goals Therapeutic goals ; maximal suppression of viral load and ; maximal suppression of viral load and restoration of immunological functionrestoration of immunological function; prevention of maternal to child transmission; prevention of maternal to child transmission
ARV therapy should be offered to all HIV ARV therapy should be offered to all HIV infected pregnant women regardless of CD4 cell infected pregnant women regardless of CD4 cell count or HIV RNA levelcount or HIV RNA level
To treat the mother as well as to reduce the risk To treat the mother as well as to reduce the risk of perinatal transmissionof perinatal transmission
Holistic care : antepartum / intrapartum / Holistic care : antepartum / intrapartum / postpartumpostpartum
: mother / fetus-baby: mother / fetus-baby : psycho / bio / social: psycho / bio / social

Antepartum careAntepartum care1.1. Posttest counseling / psychological supportPosttest counseling / psychological support2.2. History taking History taking 3.3. Physical examinationPhysical examination4.4. Per vaginal examinationPer vaginal examination5.5. Oral health examinationOral health examination6.6. Ophthalmic examinationOphthalmic examination7.7. Lab testsLab tests8.8. Tuberculin testTuberculin test9.9. Chest X-rayChest X-ray10.10. Prenatal care in high risk clinicPrenatal care in high risk clinic11.11. Nutrition support / vitamin supplementationNutrition support / vitamin supplementation12.12. Ultrasound Ultrasound 13.13. Prevention of opportunistic infectionPrevention of opportunistic infection14.14. ImmunizationImmunization15.15. Anteretroviral administration Anteretroviral administration

Intrapartum careIntrapartum care
1.1. ARV during labor period ; minimum viral loadARV during labor period ; minimum viral load2.2. Mode of deliveryMode of delivery3.3. Labor augmentation is used when needed to Labor augmentation is used when needed to
shorten the interval to delivery / but avoid shorten the interval to delivery / but avoid ARMARM
4.4. Minimize operative obstetrics : scalp Minimize operative obstetrics : scalp electrode, fetal scalp blood sampling, forceps electrode, fetal scalp blood sampling, forceps extraction, vacuum extractionextraction, vacuum extraction
5.5. Universal precautionUniversal precaution ; percutaneous ; percutaneous exposure of needle=0.3%, mucous exposure of needle=0.3%, mucous membrane exposure=0.09%, atraumatic membrane exposure=0.09%, atraumatic needle, absorbable suture, non-touch needle, absorbable suture, non-touch technique, 0.5% sodium hypochloride, room technique, 0.5% sodium hypochloride, room for isolation for isolation

Cesarean section ; decrease vertical Cesarean section ; decrease vertical transmission transmission one-halfone-half compared with compared with vaginal deliveryvaginal delivery (metaanalysis of 15 (metaanalysis of 15 prospective cohort studies by the prospective cohort studies by the international perinatal HIV group 1999)international perinatal HIV group 1999)
Combined cesarean section with ARV Combined cesarean section with ARV reduced the risk 87 %reduced the risk 87 %
ACOG 2000 ; recommended C/S when HIV ACOG 2000 ; recommended C/S when HIV RNA viral loads > 1000 copies/mlRNA viral loads > 1000 copies/ml
Scheduled C/S is recommended at 38 wkScheduled C/S is recommended at 38 wk If viral load < 1000 copies/ml ; data If viral load < 1000 copies/ml ; data
insufficient to estimate benefit of C/S insufficient to estimate benefit of C/S (ACOG 2000)(ACOG 2000)

Postpartum carePostpartum care1. ARV1. ARV
Mother:Mother: AIDS, HIV infection with CD4<200 ; continue ARV AIDS, HIV infection with CD4<200 ; continue ARV
treatmenttreatment CD4 200-350 ; controversial for ARVCD4 200-350 ; controversial for ARV CD4 > 350 ; stop ARV , monitoring CD4 CD4 > 350 ; stop ARV , monitoring CD4
Baby: ARV 1 / 6 weeksBaby: ARV 1 / 6 weeks
If delivery occurs before treatment is given, the new If delivery occurs before treatment is given, the new born can receive prophylaxis for born can receive prophylaxis for66 weeks with zidovu weeks with zidovu dine, or in some cases combination antiretroviral trea dine, or in some cases combination antiretroviral trea
tmenttment
2. Contraceptives ; condom + OCP2. Contraceptives ; condom + OCP points of interest ; TR, injectable, norplant, IUDpoints of interest ; TR, injectable, norplant, IUD

3. Breast feeding3. Breast feedingNot recommendedNot recommendedAfrica ; breast feeding with Africa ; breast feeding with
continuation of ARV prophylaxiscontinuation of ARV prophylaxis
4. Postpartum clinic and pap smear ; 6 4. Postpartum clinic and pap smear ; 6 mo / 1 yearmo / 1 year

1. Classes of ARV drugs1. Classes of ARV drugs
By FDA pregnancy category classificationBy FDA pregnancy category classification
e-text McGrawHille-text McGrawHill Cunningham FG, Leveno KJ, Bloom SL, Cunningham FG, Leveno KJ, Bloom SL,
Hauth JC, Gilstrap III L, Wenstrom KD. Hauth JC, Gilstrap III L, Wenstrom KD. Williams Obstetrics. 22nd ed. New York: Williams Obstetrics. 22nd ed. New York: McGRAW-HILL; 2005.McGRAW-HILL; 2005.
Guidelines for ARV in pregnancyGuidelines for ARV in pregnancy

Drug Category
Nucleoside reverse transcriptase inhibitors Abacavir Didanosine Emtricitabine Lamivudine Stavudine Tenofovir Zalcitabine ZidovudineNon-nucleoside reverse transcriptase inhibitors Delavirdine Efavirenz NevirapineProtease inhibitors Amprenavir Atazanavir Fosaprenavir Indinavir Lopinavir/ritonavir Nelfinavir Ritonavir SaquinavirFusion inhibitors Enfuvirtide
CBBCCBCC
CCC
CBCCCBBB
B

NRTI/ NNRTI
FI
PI

2. Regimens2. RegimensNNRTI-basedNNRTI-basedPI-basedPI-basedTriple NRTI-basedTriple NRTI-basedFI-basedFI-based
http://AIDSinfo.nih.govhttp://AIDSinfo.nih.gov

3. Monitoring3. Monitoring CD4 count at initiation then CD4 CD4 count at initiation then CD4
count every 3 monthscount every 3 monthsHIV RNA levels at 4 weeks after HIV RNA levels at 4 weeks after
initiation of treatment then HIV RNA initiation of treatment then HIV RNA levels monthly until undetectable, levels monthly until undetectable, then every 3 monthsthen every 3 months
HIV RNA level at GA 36 weeksHIV RNA level at GA 36 weeks

4. Heavy, Light, or Medium4. Heavy, Light, or Medium
HeavyHeavy Medium Medium Light Light
Short course AZTShort course AZT
NVP-single doseNVP-single dose
Short course Short course AZT+SD NVPAZT+SD NVP
AZT+3TCAZT+3TC
AZT+3TC+NVPAZT+3TC+NVP
AZT+3TC+PIAZT+3TC+PI

Short course ZDV / SD NVPShort course ZDV / SD NVP35
30
20
11.8
6.32.1
4.63.80
5
10
15
20
25
30
35
No ARV HIVNET012 PHPT-2+ZDV28wk
MASHI+ZDV34wk
HIVNET012 ; Guay, Lancet 1999;354:795-802.
PHPT-2; Lallemant, NEJM 2004; 351: 217-8.
MASHI; Shpiro , AIDS 2006; 20: 1281-8. Short course AZT ; TR 8% TR 8% (ACTG076)(ACTG076)
Short course ZDV
NVP-NVP
P-P
NVP-P
NVP-NVP P-NVP


NVP concentration after SD-NVP concentration after SD-NVPNVP
•Median T1/2 = 61.3 hours
•Drug can be detected up to 19 days
•Lower limit assay quantification 50 ng/ml ; 3-4 weeks postpartum
Cressey TR. JAIDS 2005; 38: 283-8.
•SD NVP covering the tail ; ZDV/3TC 7 days : reduce resistance from 60 % to 10-12 %
TOPH Trial, SA

Two drugs regimenTwo drugs regimen
Short course AZT (28 week)+SD Short course AZT (28 week)+SD NVP : TR 6.3% (PHPT-2)NVP : TR 6.3% (PHPT-2)
AZT+ddI (36 wk to 1 wk PP) : TR AZT+ddI (36 wk to 1 wk PP) : TR 6.9% (SIMBA trial)6.9% (SIMBA trial)
AZT+3TC 32 wk add SD NVP : TR AZT+3TC 32 wk add SD NVP : TR 4.7% (Ditrame Plus)4.7% (Ditrame Plus)
AZT 36 wk + SD NVP : TR 6.5%AZT 36 wk + SD NVP : TR 6.5%

HAARTHAART
Depend on immune status of motherDepend on immune status of mother
-low CD4 <200 ; start for maternal health-low CD4 <200 ; start for maternal health
-high CD4 ; consider-high CD4 ; consider
-pro ; low TR (PACTG316, TR 1.5%)-pro ; low TR (PACTG316, TR 1.5%)
-con ; high risk of NVP toxicity, -con ; high risk of NVP toxicity, increase risk of GDM with PI, risk of increase risk of GDM with PI, risk of preterm delivery (controversial)preterm delivery (controversial)
Which HAART?Which HAART?
-NNRTI based HAART-NNRTI based HAART
-PI based HAART -PI based HAART

Toxicities concernedToxicities concerned
NVPNVP-rash ; women>men (3.7 x)-rash ; women>men (3.7 x)-more common with high CD4 > 250 (10X -more common with high CD4 > 250 (10X increase in women)increase in women)
HepatotoxicityHepatotoxicity-symptomatic hepatotoxicity ; CD4 -symptomatic hepatotoxicity ; CD4 <250 :0.5-1.7%, CD4 > 250: 10.0-11.3%<250 :0.5-1.7%, CD4 > 250: 10.0-11.3%-fetal hepatic events ; CD4 250-400 : 0.42%, -fetal hepatic events ; CD4 250-400 : 0.42%, CD4 >400 : 1.1%)CD4 >400 : 1.1%)-TRC cohort ; low : high CD4 2.9% versus -TRC cohort ; low : high CD4 2.9% versus 7.7%7.7%


5. Factors for selection5. Factors for selection
Mother
Child Medical services

Action reports fromAction reports from Thammasat Hospital Thammasat Hospital

ท�มุงานท�มุงาน
อาย์�รแพทย์ อาย์�รแพทย์ ((ออ..อน�ชาอน�ชา)) ส�ต�แพทย์ ส�ต�แพทย์ ((ออ..อต�วุ�ทธอต�วุ�ทธ)) ก�มุารแพทย์ ก�มุารแพทย์ ((ออ..อ จฉราอ จฉรา)) ท�มุพย์าบาลหน#วุย์เอดสธรรมุศาสตร ท�มุพย์าบาลหน#วุย์เอดสธรรมุศาสตร
((ค�ณกรองท�พย์ค�ณกรองท�พย์)) ท�มุอาสาสมุ ครผู้�&ต�ดเช'(อ ท�มุอาสาสมุ ครผู้�&ต�ดเช'(อ ((ค�ณวุ นใหมุ#ค�ณวุ นใหมุ#)) เภส ชกรเภส ชกร น กส งคมุสงเคราะหน กส งคมุสงเคราะห อ'+น ๆอ'+น ๆ

< 2540 ; no ARV< 2540 ; no ARV important role of a termination of important role of a termination of pregnancypregnancy
2541-2546 ; AZT + SD NVP2541-2546 ; AZT + SD NVP
> 2547 ; HAART> 2547 ; HAART

æ µ¦¨ µ¦ ·ÁºÊ° µÂ¤n ¼n̈¼� � � � � � � � � � � (AZT)
¨� Anti HIV »¦Á¤ºÉ°°µ¥»� � 18 Áº°� �e ¦³¤µ� � � � � εª ¤µ¦ µ� � � � ANC Non - Reactive Positive Ťn¦µ� �
2541 20 9 - 11
2542 21 9 - 12
2543 17 11 1 5
2544 33 16 2 15
2545 24 12 - 12
2546 23 17 - 17
ข&อมุ�ลจาก หน#วุย์เอดสธรรมุศาสตร โรงพย์าบาลธรรมุศาสตรเฉล�มุพระเก�ย์รต�

AZT regimen AZT regimen
Prevalence of HIV infection Prevalence of HIV infection pregnancy in TUH = 1-2 percentpregnancy in TUH = 1-2 percent
AZT aloneAZT alone = infection rate 3.9 = infection rate 3.9 percentpercent
AZT regimen from other studies ; AZT regimen from other studies ; infection rate 5-8 percent, ACTG infection rate 5-8 percent, ACTG 076 protocol = 8%076 protocol = 8%
Cesarean section = beneficialCesarean section = beneficial MPH ; still using AZT regimenMPH ; still using AZT regimen

RegimensRegimens ; Pediatrics AIDS clinical trials ; Pediatrics AIDS clinical trials group, USAgroup, USA
Antepartum: 100 mg 5times/day, initiating Antepartum: 100 mg 5times/day, initiating at 14-34 wk,continueat 14-34 wk,continue throughout pregnancythroughout pregnancy (or 200 mg 3times/day, (or 200 mg 3times/day, 300 mg twice a 300 mg twice a dayday))
Intrapartum: IV Zidovudine in a 1-hr initial Intrapartum: IV Zidovudine in a 1-hr initial dose of 2 mg/kg, followed by a continuous dose of 2 mg/kg, followed by a continuous infusion of 1 mg/kg/hr until deliveryinfusion of 1 mg/kg/hr until delivery
Neonates: begin at 8-12 hr after birth, and Neonates: begin at 8-12 hr after birth, and give syrup at 2 mg/kg every 6 hr for 6 give syrup at 2 mg/kg every 6 hr for 6 weeksweeks

Regimen MPHRegimen MPH Antepartum; 300 mg twice a day, initiating Antepartum; 300 mg twice a day, initiating
at 14-34 (28) wk,continueat 14-34 (28) wk,continue throughout throughout pregnancy (regardless of CD4 count)pregnancy (regardless of CD4 count)
Intrapartum; AZT 300 mg every 3 hr and Intrapartum; AZT 300 mg every 3 hr and single dose NVP 200 mg orallysingle dose NVP 200 mg orally
Postpartum; AZT 300 mg+3TC 150 mg Postpartum; AZT 300 mg+3TC 150 mg twice a day for 2 weekstwice a day for 2 weeks
Neonates; NVP 2 mg/kg single dose and Neonates; NVP 2 mg/kg single dose and AZT 2 mg/kg every 6 hr for 6 weeksAZT 2 mg/kg every 6 hr for 6 weeks
Disadvantages (compare to HARRT) : Disadvantages (compare to HARRT) : Higher transmission rateHigher transmission rate High incidence of NVP resistanceHigh incidence of NVP resistance

HAART (AZT+3TC+NVP)HAART (AZT+3TC+NVP)
ปี/ปี/ จ0านวุนจ0านวุนมุารดามุารดา
ล�กไมุ#ต�ดล�กไมุ#ต�ดเช'(อเช'(อ
ล�กต�ดเช'(อล�กต�ดเช'(อ
25472547 3636 3535 11
25482548 4646 4646 00
25492549 3434 3333 11
25502550 5252 2121 11
25512551 4343 88 00
ข&อมุ�ลจาก หน#วุย์เอดสธรรมุศาสตร โรงพย์าบาลธรรมุศาสตรเฉล�มุพระเก�ย์รต�

Triple agents (HARRT) Triple agents (HARRT) Thammasat Hospital ; Thammasat Hospital ; transmission ratetransmission rate 1.2 %1.2 %
Other studies ; transmission rate Other studies ; transmission rate 1-1.5%1-1.5%

Regimen : TUHRegimen : TUH
1. CD41. CD4 ≤ ≤ 200 / GA 14 weeks 200 / GA 14 weeks Antepartum; AZT(300)/3TC(150) q Antepartum; AZT(300)/3TC(150) q
12 hr + NVP(200) OD for 2 wk then 12 hr + NVP(200) OD for 2 wk then AZT(300)/3TC(150) +NVP(200) q AZT(300)/3TC(150) +NVP(200) q 12 hr12 hr
Intrapartum; AZT 300 mg q 3 hr and Intrapartum; AZT 300 mg q 3 hr and AZT(300)/3TC(150) +NVP(200) q AZT(300)/3TC(150) +NVP(200) q 12 hr12 hr
Postpartum; AZT(300)/3TC(150) Postpartum; AZT(300)/3TC(150) +NVP(200) q 12 hr +NVP(200) q 12 hr
Neonates; AZT 2 mg/kg q 6 hrx6 wkNeonates; AZT 2 mg/kg q 6 hrx6 wk

2. CD42. CD4 > 200 / GA 28 weeks> 200 / GA 28 weeksAntepartum; AZT(300)/3TC(150) Antepartum; AZT(300)/3TC(150) q 12 hr + NVP(200) OD for 2 wk q 12 hr + NVP(200) OD for 2 wk then AZT(300)/3TC(150) then AZT(300)/3TC(150) +NVP(200) q 12 hr+NVP(200) q 12 hrIntrapartum; AZT 300 mg q 3 hr Intrapartum; AZT 300 mg q 3 hr and AZT(300)/3TC(150) and AZT(300)/3TC(150) +NVP(200) q 12 hr+NVP(200) q 12 hrPostpartum; AZT(300)/3TC(150) Postpartum; AZT(300)/3TC(150) q 12 hr x 14 days, stop NVPq 12 hr x 14 days, stop NVPNeonates; AZT 2 mg/kg q 6 hrx6 Neonates; AZT 2 mg/kg q 6 hrx6 wkwk

Alternative regimens;Alternative regimens; AZT/3TC/Nelfinavir(NLF) (250 mg 5 tabs q 12 AZT/3TC/Nelfinavir(NLF) (250 mg 5 tabs q 12
hr, no need for test dose, no covering tail)hr, no need for test dose, no covering tail) AZT/3TC/Efavirenz (GA>24wk)AZT/3TC/Efavirenz (GA>24wk) GPOvir(3TC/d4T/NVP)(follow the protocolGPOvir(3TC/d4T/NVP)(follow the protocol
AZT/3TC/NVP and test doses NVP for 2 wk)AZT/3TC/NVP and test doses NVP for 2 wk)In case C/SIn case C/S Start AZT with 30 cc of water since NPO then Start AZT with 30 cc of water since NPO then
NPO except medicine with water until delivery NPO except medicine with water until delivery and and postop care period 12-24 hrpostop care period 12-24 hr
For no ANC patientsFor no ANC patients Intrapartum; Intrapartum; AntiHIV statAntiHIV stat, NVP 200 mg single , NVP 200 mg single
dose (dose (immediatelyimmediately) and AZT 300 mg q 3 hr ) and AZT 300 mg q 3 hr regardless of CD4 count regardless of CD4 count
Postpartum;AZT300/3TC150 q 12 hrx14wkPostpartum;AZT300/3TC150 q 12 hrx14wk Neonates; NVP 2 mg/kg single dose + AZT 2 Neonates; NVP 2 mg/kg single dose + AZT 2
mg/kg q 6 hr x 6 wk (start mg/kg q 6 hr x 6 wk (start immediatelyimmediately))

Thank you for your attention Thank you for your attention until the end of the sessionuntil the end of the session