
HIV infection for the General Physician
37
HIV infection for the General Physician Dr.Andrew Carmichael Infectious Diseases Service Addenbrooke’s Hospital
Transcript of HIV infection for the General Physician

HIV infection for the General Physician
Dr.Andrew Carmichael
Infectious Diseases Service
Addenbrooke’s Hospital

Overview
• Unmodified natural history of HIV infection
• Principles of anti-HIV treatment
HIV as a chronic disease with a really good prognosis
UK prevalence of HIV 78,900 + 10,400 undiagnosed
incidence HIV 5,200 per year
AIDS 280 per year
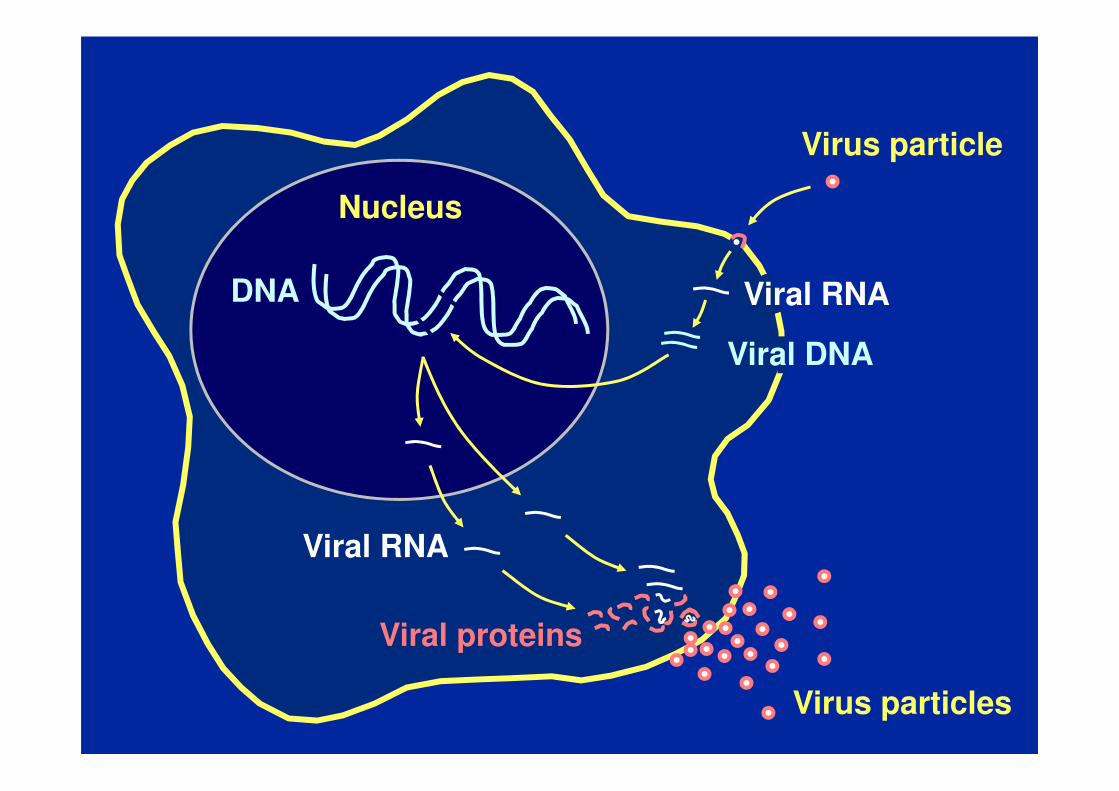
DNA
Viral proteins
Viral RNA
Nucleus
Viral DNA
Virus particle
Viral RNA
Virus particles
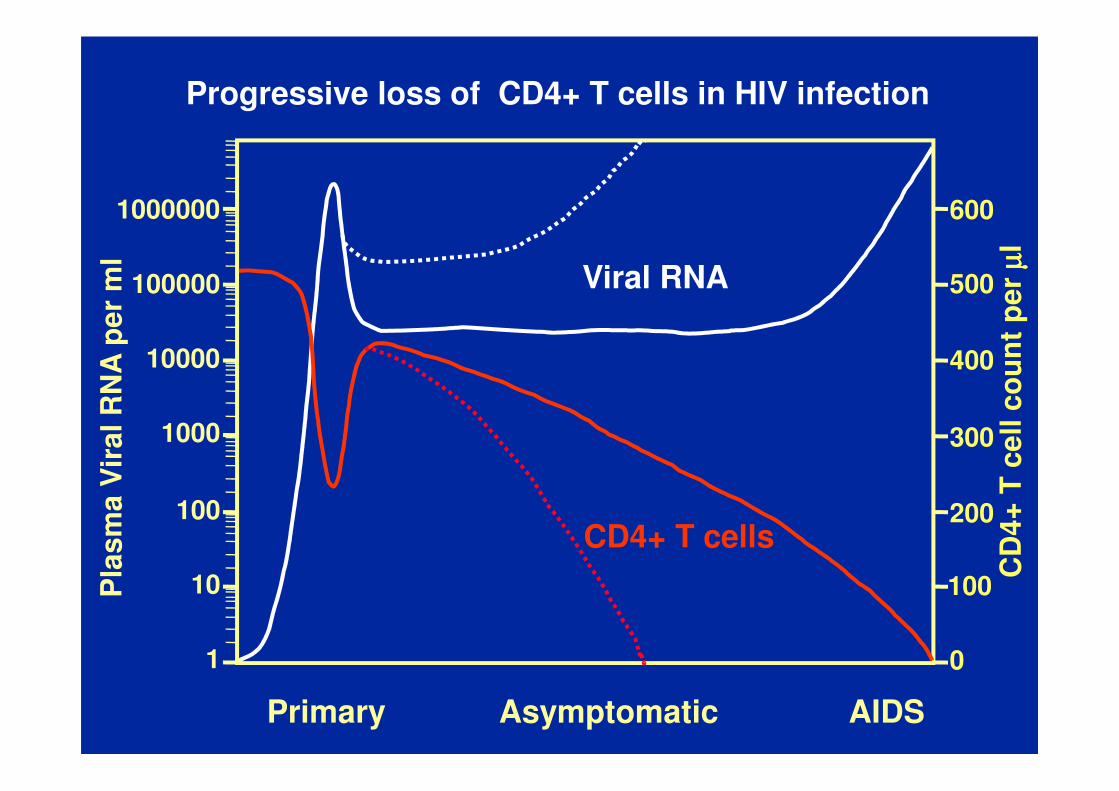
Primary Asymptomatic AIDS
Progressive loss of CD4+ T cells in HIV infection
1000000
100000
10000
1000
100
10
1
Pla
sm
a V
ira
l R
NA
pe
r m
l
Viral RNA
CD
4+
T c
ell
co
un
t p
er
µµ µµl
600
500
400
300
200
100
0
CD4+ T cells

• 4 chapters of the microbiology text book :
mycobacteria, yeasts, protozoa, persistent DNA viruses
• reactivation of persistent intra-cellular infections
high density of organisms & lack of host immune response
• concurrent or sequential infections are common
• some infections are human-adapted & difficult to eradicate,
may require long-term suppressive anti-microbial treatment
until the immune system improves with anti-HIV treatment
• the Microbiology lab will not look for these organisms
unless you ask them to
Opportunistic infections in advanced HIV = AIDS

Classical AIDS presentation 1
white man, age 30-65
sub-acute 2-3 weeks dry cough (NO sputum)
worsening breathlessness
fever
weight loss
on examination pulse 110/min
resp 22/min
surprisingly clear lungs
pulse oximetry at rest 94% after exercise, only 89%

Pneumocystis pneumonia (PCP)

Classical AIDS presentation 3
Black African man or woman, age 25-65
works as a carer in a nursing home
sub-acute 4 weeks productive cough
fever
weight loss
on examination pulse 100/min
resp 20/min
scattered lung crackles
painless 2cm lymphadenopathy

Disseminated tuberculosis
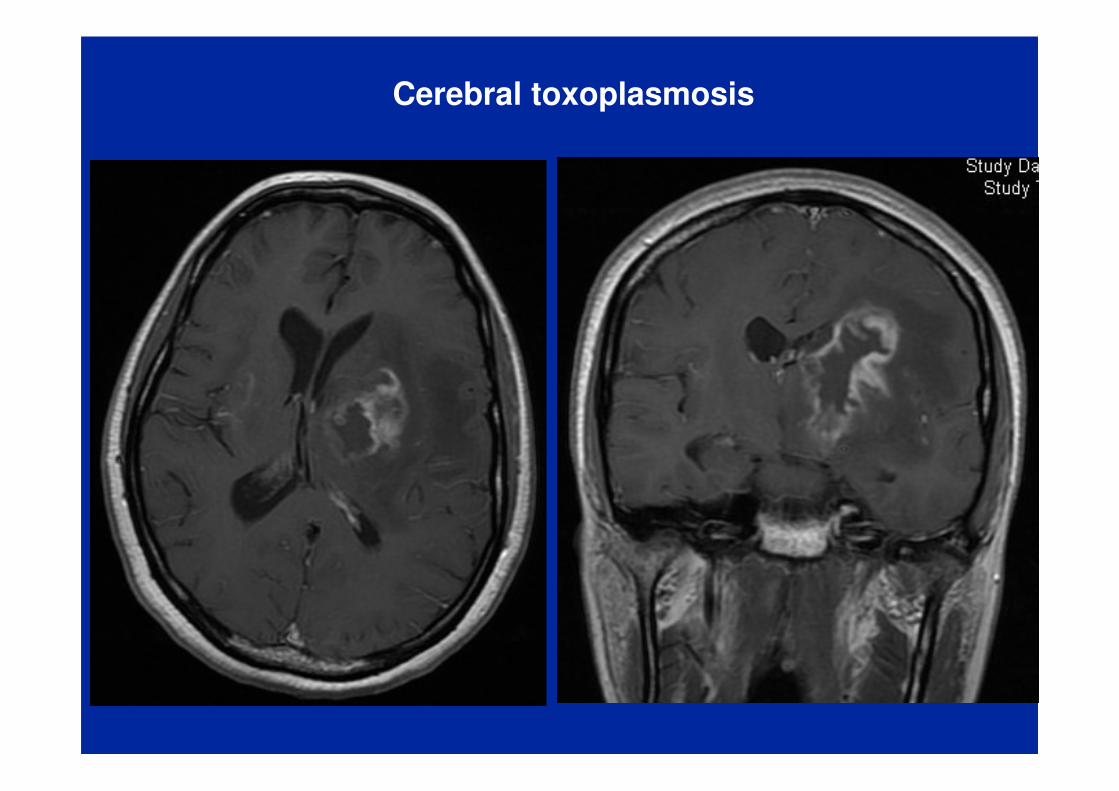
Cerebral toxoplasmosis

Progressive multifocal leucoencephalopathy

Cytomegalovirus retinitis

Delayed diagnosis of HIV leads to avoidable fatalities & disability
infectionadults newly diagnosed with HIV in the UK in 2015
late CD4 count 350-200 17%
very late CD4 count < 200 21%} 38%
8%1 year
7%
6%
5%
4%
3%
2%
1%
0
CD4 count < 350
CD4 count > 350
15-24Age 25-34 35-49 50-64 65+
mortality rate

Diagnosed HIV prevalence (per 1,000 population aged 15 to 59 years)
England, 2016

HIV prevalence rate per 1000 adults age 15-59
KwaZulu Natal 390.0 per 1000
Extremely high > 5 per 1000 Lambeth 16.4 per 1000
High prevalence 2-5 per 1000 Luton 4.1 per 1000
Low prevalence < 2 per 1000 Cambridgeshire 1.1 per 1000
Lincolnshire 0.7 per 1000

Certain groups have a higher prevalence of HIV infection
infection
HIV prevalence in adults age 15-59, UK 2014
Men Women
Men who have sex with men 5.9%
(London or Brighton 12.5%)
Heterosexual
Black African ethnicity 4.1% 7.1%
Caucasian ethnicity 0.06% 0.06%
Injecting drug users 0.9% 0.9%

%

ESR 50-100 (CRP < 10)Polyclonal increase IgG

Seeking consent for an HIV test
We would like you to have an HIV test - HIV is the virus that can
lead to the disease AIDS.
There is now very effective treatment for HIV, so it is important
to find out if a person has the virus in time.
If the first blood test looks positive, we will test a second blood
sample to make sure that the laboratory gets the correct result.
This is confidential - I will tell you the result.
If a person does have HIV, we give support and practical advice
about relationships, work, insurance and travel. We do tests to
find out how much or how little the immune system is affected.

When you diagnose a patient as having HIV
Please remember confidentiality
Please telephone your regional Infectious Diseases unit
to discuss the clinical condition of the patient
and appropriate investigations
to decide where the patient should be cared for

Treatment of HIV infection
• anti-retroviral drug therapy
- start early, as soon as feasible
- inhibitors of viral enzymes - reverse transcriptase
- protease
- integrase
- drug combinations are used to prevent viral resistance
- adherence to treatment is essential
- regular monitoring of HIV viral load
• prophylaxis against opportunistic infections
• psychological / social support

Anti-HIV drugs
Nucleoside RT Non-nucleoside RT Protease inhibitor
Abacavir Efavirenz Atazanavir
Tenofovir Nevirapine Darunavir
Lamivudine Etravirine Lopinavir
Emtricitabine Rilpivirine Ritonavir
Zidovudine Saquinavir
Stavudine Fosamprenavir
Didanosine Tipranavir
Entry inhibitor Integrase inhibitor
Enfuvirtide Raltegravir
Maraviroc Elvitegravir
Dolutegravir

Primary Asymptomatic
1000000
100000
10000
1000
100
10
1
Pla
sm
a V
ira
l R
NA
pe
r m
l
Viral RNA
CD
4+
T c
ell
co
un
t p
er
µµ µµl
600
500
400
300
200
100
0
CD4+ T cells
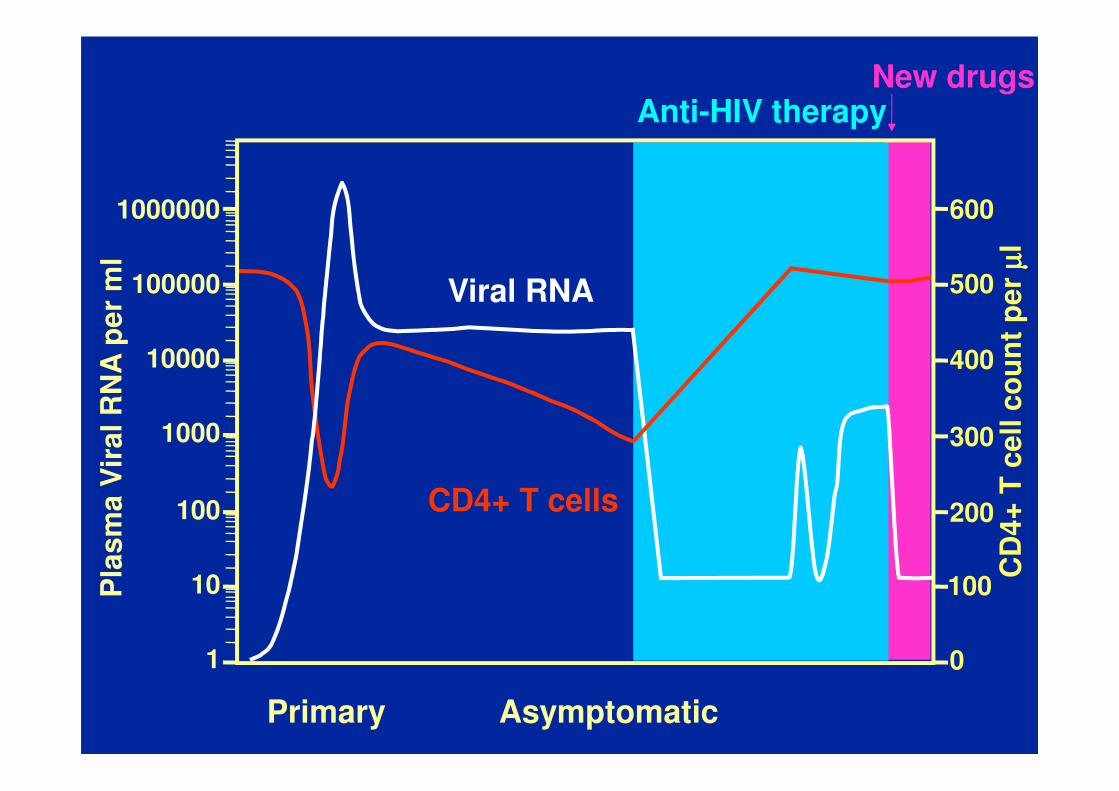
Anti-HIV therapy

Because some anti-HIV drugs have very long serum half-lives,
unplanned stopping leads to monotherapy & HIV resistance
Se
rum
dru
g c
on
ce
ntr
ati
on
Time
Patient stops all drugs
Efavirenz
Tenofovir
Emtricitabine

Primary Asymptomatic
1000000
100000
10000
1000
100
10
1
Pla
sm
a V
ira
l R
NA
pe
r m
l
Viral RNA
CD
4+
T c
ell
co
un
t p
er
µµ µµl
600
500
400
300
200
100
0
CD4+ T cells
Anti-HIV therapy
Primary Asymptomatic
1000000
100000
10000
1000
100
10
1
Pla
sm
a V
ira
l R
NA
pe
r m
l
Viral RNA
CD
4+
T c
ell
co
un
t p
er
µµ µµl
600
500
400
300
200
100
0
CD4+ T cells
Anti-HIV therapyNew drugs

Immune reconstitution inflammatory syndrome IRIS= fancy name for a paradoxical reaction
• within 6 weeks of starting anti-HIV treatment
as the number & function of CD4+ T cells improves,
a vigorous cellular immune response can develop
e.g. against a disseminated mycobacterial infection
• more likely when there are large numbers of mycobacteria
• fever, weight loss
enlarging lymph nodes
increased lung shadowing
• may require anti-inflammatory treatment (steroids)

nu
mb
er
of
dia
gn
os
es
pe
r ye
ar
New HIV diagnoses, AIDS diagnoses
& deaths in HIV infected individuals in the UK
1985
HIV
AIDS
deaths
combination anti-HIV
drug treatment
1990 1995 2000 2005 2010 2015
8000
7000
6000
5000
4000
3000
2000
1000
0
2016 UK prevalence: 78,900 diagnosed & 10,400 undiagnosed

HIV as a chronic disease - Practical stuff
• Relocation of GUM clinics from hospitals into the community
No-one in a district general hospital has training in HIV
Hospital doctors lack information about tests or treatment
• When an HIV patient is under your care, call the HIV physician
to find out the patient’s recent blood results
which anti-HIV drugs the patient is taking now
ensure the anti-HIV drugs are given on time
beware unfamiliar drug interactions
• Remember confidentiality (visitors, letters to GP)

oral Atazanavir
plasma Atazanavir
unconjugated bilirubin Atazanavir
Se
rum
bilu
rub
in
Time
Clinical pharmacology of anti-HIV drugs
UDP glucuronosyl
transferase 1A1
conjugated bilirubin
X

cytochrome P450 3A4
oral Atazanavir
plasma Atazanavir
inactive metabolites
pla
sm
a A
taza
na
vir
Time

cytochrome P450 3A4
Ritonavir
oral Atazanavir
plasma Atazanavir
inactive metabolites
X
Time
Pharmacokinetic boosting by selective inhibition of
the metabolism of HIV protease inhibitors
+ Ritonavir
pla
sm
a A
taza
na
vir
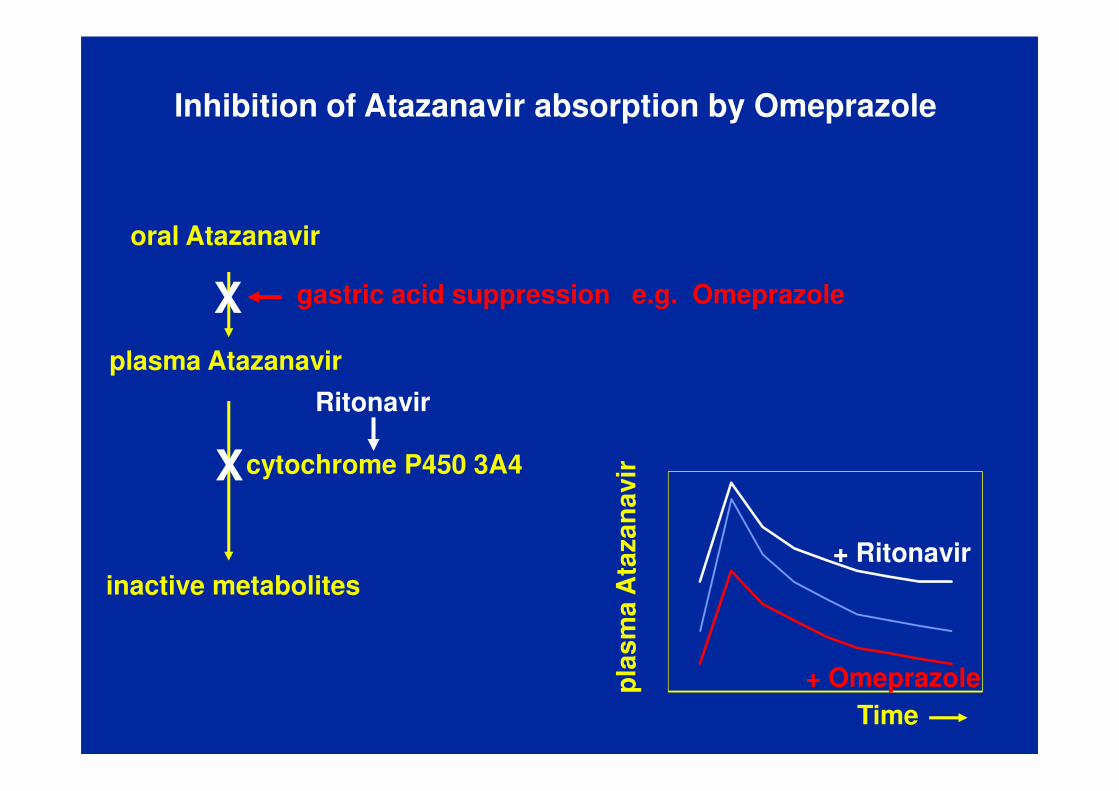
cytochrome P450 3A4
Ritonavir
oral Atazanavir
plasma Atazanavir
inactive metabolites
X
Time
gastric acid suppression e.g. OmeprazoleX
Inhibition of Atazanavir absorption by Omeprazole
+ Omeprazole
+ Ritonavir
pla
sm
a A
taza
na
vir

oral Ticagrelor
plasma Ticagrelor
cytochrome P450 3A4
inactive metabolites
Ritonavir arterial bleeding
oral Atazanavir
plasma Atazanavir
inactive metabolites
XX
Increased plasma concentration of Ticagrelor
e.g. following placement of an intra-arterial stent

inhaled Fluticasone
plasma Fluticasone
cytochrome P450 3A4
inactive metabolites
Ritonavir
Cushing’s syndrome
suppressed ACTH
adrenal atrophy
undetectable cortisol
oral Atazanavir
plasma Atazanavir
inactive metabolites
XX
Increased plasma concentration of inhaled Fluticasone

Iatrogenic inhaled Cushing’s syndrome
• Confiscate Fluticasone-containing inhaler
Prescribe Beclomethasone-containing inhaler
• Because of temporary adrenal suppression,
prescribe low dose Hydrocortisone, gradual dose weaning
• Give the patient a credit-card sized list of
his current anti-HIV medication and
the Clinic phone number
• Inform the patient’s GP and the patient

HIV infection - the key points
• anti-HIV treatment reverses the immune impairment
and greatly improves the prognosis
• early diagnosis of HIV infection is very important
2 main obstacles - failure to think of HIV infection
- reluctance to perform an HIV test
• Beware stopping anti-HIV treatment
Beware starting new drugs that interact with anti-HIV treatment
So please call an HIV physician


















