
HIV in Paediatrics - RAFTraft.g2hp.net/files/2015/07/150722_HIV-GSK-E... · HIV in Paediatrics...
63
HIV in Paediatrics 22.07.15 Juan Ambrosioni, Noémie Wagner
Transcript of HIV in Paediatrics - RAFTraft.g2hp.net/files/2015/07/150722_HIV-GSK-E... · HIV in Paediatrics...

HIV in Paediatrics
22.07.15
Juan Ambrosioni, Noémie Wagner

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• HIV: Human immunodeficiency Virus
– HIV-1: Pandemic
– HIV-2: Endemic in West Africa
• AIDS: Acquired immunodeficiency
syndrome
• ART: Antiretroviral therapy
Definitions

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• First cases of AIDS described in early1980s
• Since then, more than 30 millions deaths
• In 2013: 35 million people infected
– Sub-saharian Africa: 1/20 adult is infected
• In 2013: 3,2 million children infected
• Since 1995: 14 million lives saved thanks to ART
WHO /UNAIDS 2013
Epidemiology

• Carte du monde avec prévalence HIV

Epidemiology: HIV-2
-Geographically restricted
-Less transmissible
-Less aggressive
-Some antiretroviral drugs (NNRTI, see later), not active
Nicolas et al. ERAIT 2015

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

Risk of getting infected with HIV (blood, body fluids):
•Transfusion: close to 100%
•MTCT (untreated mother): 30% (< 1% on ART and
undetectable VL)
•Vaginal/anal intercourse: 0,01 à 8 %
•Almost cero for oral sex (except menses or ejaculation)
•Needle injury: 0,3 %
☛ risk related to VL!!! ↗↗ during primary infection !!!
☛ circumcision: 40% decrease of risk (women to men)
☛sexual intercourse: Increased risk if local inflammation, (genital ulcer: x 10!)
Transmission

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• The virus can infect:
- CD4 lymphocytes
- Dendritiques cells
- Monocytes and monocytes-derived cells
• HIV is also neurotropic and infect CNS!!!
Attachment of viral particles
(gp120) to CD4 and co-
receptors (CCR5, CXCR4)
Pathogenesis

1) Transmission through the mucosae (genital tract/rectum/placenta/digestive tract)
2) Depletion of lymphoid tissue in digestive tract (GALT)
=> translocation of bacterial products
☛ INCREASED IMMUNE ACTIVATION
3) progressive decrease of CD4 cell count and immune
collapse due to: - ↗ in CD4 cell turn-over
- ↗ destruction of CD4 cells
=> collapse of immune system
☛ OPPORTUNISTIC INFECTIONS (final step)
Pathogenesis (2)

Pathogenesis(3)

• Effect on the immune system
– ↗ HIV infection (the virus infect preferably activated cells)
– ↗ Increased T cell turnover immune collapse
– Fibrosis of lymphoid tissue dysfunction
• Effect on the organism (inflammation and increased replication)
– ↗ CV risk
– Neurological, bone and kidney involvement
– Increased risk of non-AIDS defining tumors
Frailty and Immune senescence =
development of typical complication of
uninfected population 10-20 years older
➤ Chronic increased immune activation
Pathogenesis (3)

Evolution clinique naturelle de
-A newborn infected in-uterus can progress much faster
-Since adolescence, clinical presentation is similar to that of adults
Natural history of HIV infection in adults

Evolution clinique naturelle de Viral markers kynetics

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• Clinical presentation varies according to age
• Frequently the same pathogens than in HIV-neg
patients but:
– More frequently or repeated
– More severe
• Some diseases, highly specific of HIV-infected
children, e.g.:
– Pneumocystis jirovecii pneumonia (PCP)
– Esophagic candidiasis
– Lymphoid interstitial pneumonia (LIP)
– Kaposi Sarcoma
– Severe CMV infections
Clinical presentation in children (1)

Type of evolution in untreated children:
•Category 1 (25 – 30%): in general, infection acquired in-utero
• Very rapid disease progression
• Death before one year of life
•Cateegory 2 (50 – 60%)
• Symptomes appear during first years of life
• Death between 3 to 5 years old
•Cateegory 3 (5 – 25%): « long term survivors »
• children living without treatment beyond 8-y.o.
Clinical presentation in children(2)

• PCP
• LIP
• Delayed growing and repeated diarrheal episodes
• Lymphadenopathies, liver and spleen increase
• CMV Infection
• Hepatitis, retinitis, pneumonia, digestive disease,
encephalopathy, haematological involvement
• HIV-encephalopathy
• Tuberculosis
• Toxoplasmosis
• BCG-itis
Clinical presentation: infants (1)

- Severe infections / mild recurrent infections
- Chronic bilateral parotiditis
- Severe presentation of childhood infections (VZV)
- Herpes Zoster
-Repeated, extender cutaneous Infections
-HEENT recurrent Infections (Otitis, sinusitis)
-Lymphadenopathies, liver and spleen increase
☛ involution of lymphoid organs with advanced HIV infection
-Tuberculosis
Also frequent:
- Delayed puberty
- Delayed cognitive development (1/3 des patients)
Penta course, Rome 2013
Clinical presentation: children
THINK ABOUT HIV!!!!!!!!!!!!!

• Congenital infections can be evident only at that
time!!!!!!
• HIV/AIDS complications have the same clinical
presentation than in adults
Clinical presentation: adolescents
• Remember that a mononucleosis-
like syndrome can be a primary HIV
infection!!!

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• The most frequent clinical presentation
• In general < 12 months (peak 4 – 6 months)
• Frequently associated with other infections (CMV!)
• 20-30% of mortality rate
Clinical presentation:
•Non-productive cough
and respiratory distress
•Fever (can be absent)
Radiography:
Interstitial bilateral
infiltrates
(although RX can be
normal in up to 20% of
cases)
PCP (1)

Treatment of PCP
– Start Co-trimoxazol orally or, if available, IV for
three weeks (dose 15mg/kg/d of TMP, tid or qid)
– Add prednisone 1-2 mg/kg (first week, then
decrease progressively, total 15-20 days) if
pO2<70mmHg, or clear respiratory insufficiency
– Start ART during the first two weeks of PCP
treatment
– Continue secondary prophylaxis with Co-
trimoxazol until CD4 T cell improvement
PCP (2)

•20% of infected infants, generally at the end of first year of life
•Related to EBV infection
•Exclusion Diagnosis
Clinical presentation:
Persistent cough
Bilateral Parotiditis
Persistent generalised lymphadenopathies
Hepatomegaly and other signs of cardiac insufficiency
TxRx: interstitial reticulonodular infiltrates
Interstitial Lymphoid Pneumonia (1)

Treatment ILP
• Antibiotics-Co-trimoxazole (exclude infectious causes)
• Once antimicrobials started and in presence of at least
one of the following:
• Respiratory distress
• Cyanosis
• Saturation < 90%
Add prednisone (1-2 mg/kg/d during 2 weeks, then decreasing doses)
• Start ART, if still not done
Interstitial Lymphoid Pneumonia(2)

ILP
•Hiliar Lymphadenopathy and more central infiltrates
PCP
PCP and/or ILP?

• Think TB in every HIV + patient!!
• Frequently difficult to confirm
• If immunity not compromised:
– Same clinical presentation than HIV negative children
• If advanced immunedeficiency:
– Frequently disseminated or meningeal TB
• Start 4 drugs as soon as possible
• Start ART asap, once tolerated
(within 2 weeks if severe immunodeficiency, and no more than 8
weeks after in every case for less immunosuppressed patients)
Tuberculosis (1)

Tuberculosis (2)
NCBI bookshelf
Miliary TB

– Severe delayed neurological development affecting
up to 10% of HIV infected infants
– Dysfonction similar to CP
– Motor disorders (spastic diplegia) +/- cognitive disorders
HIV-related encephalopathy

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

Stade 1 Asymptomatic or generalized adenopathies
Stade 2 Recurrent HEENT infections
HPV and molluscum extended infections. Nails mycoses.
Zoster (1 dermatome)
Chronic parotiditis
Stade 3 Moderate malnutrition
Recurrent pulmonary Infections
Recurrent oral candidiasis
TB (lungs, lymph nodes)
Chronic ILP
Unexplained haematological involvements (anemia,
thrombopenia, leucopenia)
Unexplained fever and/or diarrhea
Stade 4 Severe malnutrition
Recurrent severe bacterial infections
Oesophagic candidiasis
TB (extrapulmonary, entranodal)
PML
Zoster (multi-metameric)
PCP, CMV organ diseases
Kaposi
WHO 2006: Clinical classification (abstract)
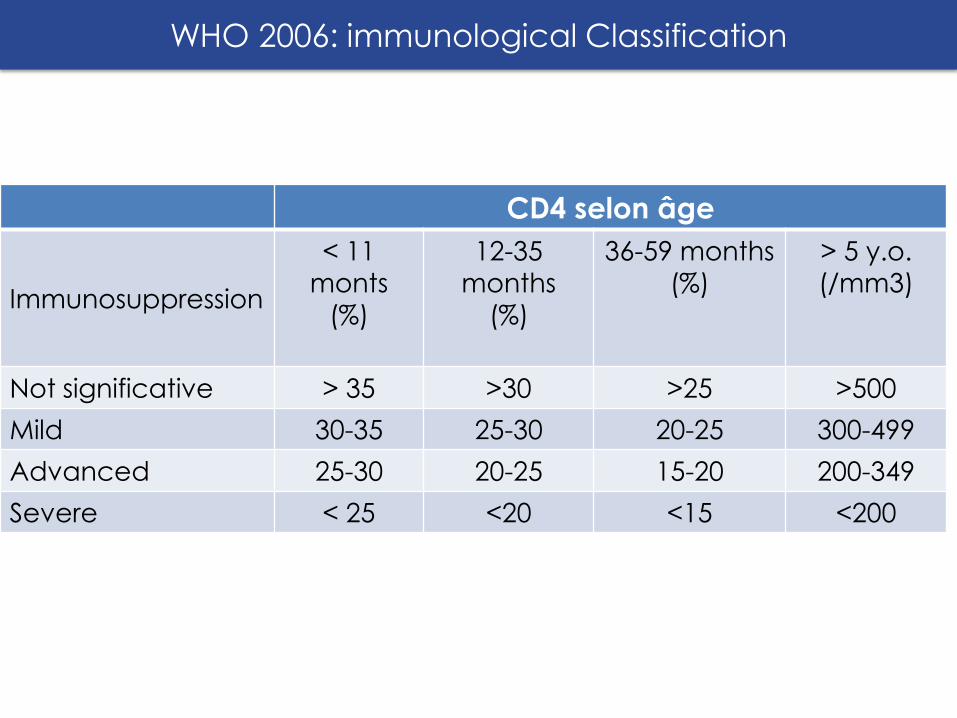
CD4 selon âge
Immunosuppression
< 11
monts
(%)
12-35
months
(%)
36-59 months
(%)
> 5 y.o.
(/mm3)
Not significative > 35 >30 >25 >500
Mild 30-35 25-30 20-25 300-499
Advanced 25-30 20-25 15-20 200-349
Severe < 25 <20 <15 <200
WHO 2006: immunological Classification

The European collaborative study
PIDJ, 1992
Proportion of CD4 cells in
uninfected children (born from
HIV-infected mothers)
CD4 cells in healthy children (2)

The European collaborative study PIDJ,
1992
CD4 cells in healthy children(1)

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• HIV infection in adults is based on Ab
detection +/- viral Ag P24 detection:
Diagnosis

Serologic tests according to generation:
• Tests of 1st, 2nd, 3rd generation: Only
detection of Ab (3rd G more sensitive,
pos around 4-6 weeks post-infection)
• Test of 4th generation: Simultaneous
detection of Ab and P24 Ag (pos
around 3-4 weeks post-infection)
Diagnosis

• In newborns, diagnosis cannot be based in Ab detection,
due to maternal IgGs
• IgM not useful either
Diagnostic
• Diagnosis in then based in direct detection of the virus
(genome) and the lost of maternal Abs (See later MTCT)

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

ART: targeting the replication cycle steps

• Every children < 5 y.o.
• Every children ≥ 5 y.o. with:
– CD4 < 500
–Clinical stages 3 & 4
Indications for ART (WHO 2013)

• ART: always combined therapy(SOC, three drugs)
Avoid resistance development
• First line drugs in children -Nucleoside RT inhibitors(NRTI)
-Non-Nucleoside RT inhibitors(NNRTI)
-Protease inhibitors (PI)
-Integrase inhibitors and entry inhibitors (very poor availability in Africa, thus not recommended by WHO in first line regimens)
Classic regimens:
• 2 NRTI + 1 NNRTI
• 2 NRTI + 1 PI
ART: regimens

• Choice according to:
- Age (authorized? Paediatric formulation?)
- Risk of resistance development
- Simplicity
- Side effects
- Limited experience with the more recently
developed molecules
ART : choice of regimen

Class Drug
NRTI zidovudine (AZT)
abacavir (ABC)
tenofovir (TDF)
lamivudine (3TC)
Emtricitabine (FTC)
NNRTI efavirenz (EFV)
Nevirapine (NVP)
PI Lopinavir (LPV)
Ritonavir (/r)
First line drugs in children

0-3 y.o. 3 - 10 y.o. >10 y.o. (> 35 kg)
Back-
bone ABC + 3TC
Alternative:
-AZT + 3TC
ABC + 3TC
Alternative:
-AZT + 3TC
-TDF + 3TC (or FTC)
TDF + 3TC (or
FTC)
Alternative:
-AZT + 3TC
-ABC + 3TC
3rd
agent LPV/r
Alternative: NVP
EFV
Alternative: NVP
EFV
Alternative: NVP
ART in children: 1st line regimens
WHO guidelines 2013

• NNRTI
– More paediatric formulations available
– Lower genetic barrier (resistance easily selected)
– Co-formulation
• PI
– Higher genetic barrier (‘resistant to resistance’)
– Fewer paediatric formulations available
NNRTI or PI based-regimens?

– Paradoxical worsening of clinical symptoms of a pre-
existent disease (diagnosed or not!!!), following
immunity improvement
– Up to 25% of cases following ART initiation
– More frequently seen with mycobacteria and some
fungi (crypto)
– Coud be fatal (E.g. Crypto, PML)
– Never stop ART!!! Provide anti-inflammatory treatment
IRIS (immune reconstitution inflammatory syndrome )

Age Indication
Infants of HIV-pos mothers Every child since 4-6 weeks until exclusion of
HIV infection
Infected children 0 - 5 y.o. all
≥ 5 y.o. Stage WHO 3 or 4
Or
CD4 < 350
Some experts recommend PCP prophylaxis
for every infected children in poor-resource
settings and high morbidity-mortality
countries
PCP prophylaxis
WHO guidelines 2014

• In untreated patients, production of millions virions per day
• Mutation rate 1/1000, most not functional, some potentially
resistant to drugs
• Risk of development in patients with poor adherence or low
drug exposure
• Resistant strains can also be transmitted!!!!
ART: Resistance(1)

• △ An acquired resistance will never be lost
• Every effort must be made to avoid the onset of
resistance
Drug adherence!!!!!!
• △ Resistance can be seen only under drug pressure
→ Always consider previous genotypes
ART: Resistance

ART resistance
Detection requires molecular techniques (genome amplification
and sequencing, followed by interpretation of mutations found)

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content
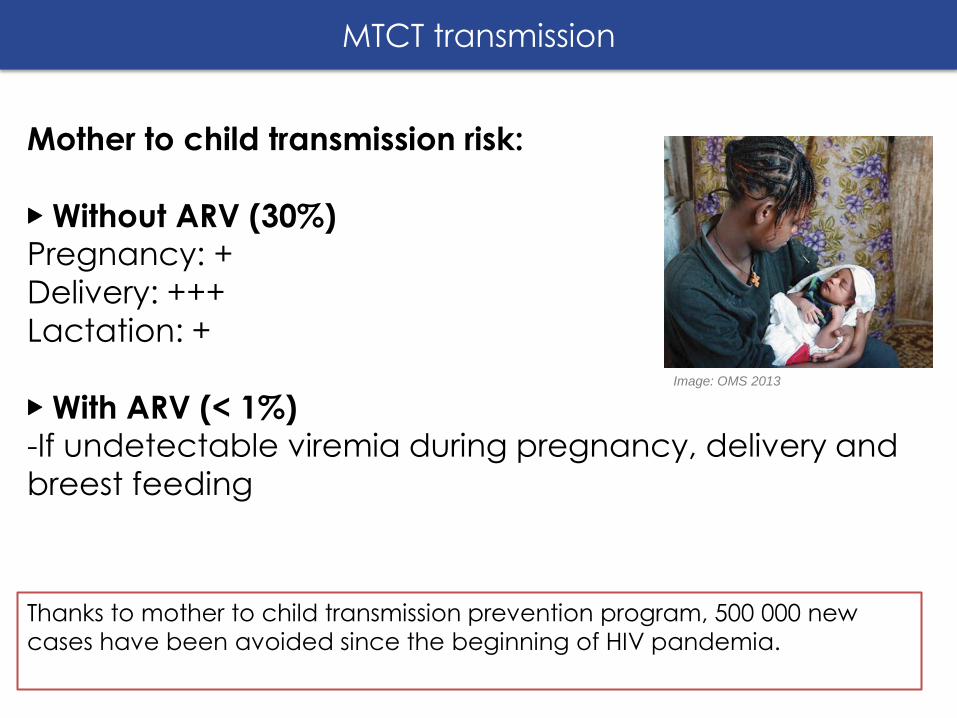
Mother to child transmission risk:
▶ Without ARV (30%) Pregnancy: +
Delivery: +++
Lactation: +
▶ With ARV (< 1%) -If undetectable viremia during pregnancy, delivery and
breest feeding
Thanks to mother to child transmission prevention program, 500 000 new
cases have been avoided since the beginning of HIV pandemia.
MTCT transmission
Image: OMS 2013

Pregnant or breastfeeding
women HIV exposed infant
Treatment for all
TDF + 3TC (or FTC) + EVF
Breastfeeding Replacement
feeding
6 weeks ofNVP 4-6 weeks of NVP or AZT
• Option B+: Provide lifelong ART to all pregnant and
breastfeeding women with HIV regardless WHO staging or
CD4 count.
Option B: After delivery and lactation, continue ART only for
those meeting treatment eligibility criteria.
Mother to child prevention recommandations
WHO guidelines 2013

• ART for all breastfeeding mother
• Exclusive breastfeeding for the first 6 months of life
• Introduction of appropriate complementary foods
after 6 months and continued breastfeeding for the
first 12 months of life.
• Stop breastfeeding only once a nutritionally adequate
and safe diet without breast-milk can be provided
Breastfeeding recommandation

• Maternal HIV antibodies can persist in the child up to 15–
18 months of age
• A positive antibody test in a child < 18 months old is not
reliable to diagnose HIV infection
• HIV infection can only be definitively confirmed using
virological test (PCR) in children < 18 months
• In case of a positive virological test, start ART without
delay and repeat the virological test to confirm the
infection
HIV diagnosis in children < 18 mois
WHO guidelines 2013

HIV
-exp
ose
d in
fan
t o
r ch
ild <
18
mo
nth
s
Infected
In case of positive viral test - Start ART - Repeat viral test to confirm HIV infection
Uninfected. Remains at risk
until breastfeeding cessation
Infected
PCR at 1 month Antibodies
test at 9 months
Viral test
Antibody test at 18 months of age and/or 6 weeks after cessation of
breastfeeding
uninfected
+
-
+
+
-
- +
-
Infant diagnosis (virological –PCR- test available)
Uninfected. Remains at risk
until breastfeeding cessation
WHO guidelines 2013

Probable infection
periodic clinical monitoring
Antibodies
test at 9 months
Antibody test at
18 months of age and/or 6 weeks after cessation of
breastfeeding
Antibodies test
- Start ART. - Check antibodies at 9 months. If positive, repeat antibody test at 18 months of age and/or 6 weeks after cessation of breastfeeding
- Assume infected if sick - Assume uninfected if well
Possible infection
Start ART
-
+
+ -
+
-
Infant diagnosis (virological –PCR- test available) H
IV-e
xpo
sed
infa
nt
or
child
<1
8 m
on
ths
Uninfected. Remains at risk
until breastfeeding cessation
uninfected
Infected
WHO guidelines 2013

1. Definitions
2. Epidemiology
3. Transmission
4. Pathogenesis
5. Clinical presentation in paediatrics
- Presentation according to age
- Some selected diseases
6. WHO classification
7. Diagnosis
8. Antiretroviral therapy and resistance
9. Mother to child transmission
10. Take-home messages
Content

• HIV is frequent in Africa
• Think about HIV in case of repeted, severe or
uncommun infection(s)
• The standard ART is based on a combination of 2 NRTI
and 1 NNRTI or PI.
• Be aware of resistance risk. An acquired resistance will
never diseapear.
• Mother to child transmisison prevention:
– Mother ARV treatement + NVP (or AZT) in infant
during 6 weeks + exclusive breatfeeding
– Rule out infection in all exposed infant
Take-home messages

• G. Maartens, C. Celum, S. lewin. HIV infection: epidemiology,
pathogenesis, treatment and prevention Lancet 2014; 384:
258–71
• Penta Course, Roma 2013
• Consolidated guidelines on the use of antiretroviral drugs for
treating and preventing hiv infection (WHO 2013)
• Guidelines on post-exposure prophylaxis for HIV and the use of
co-trimoxazole prophylaxis for HIV-related infections among
adults, adolescents and children (WHO 2014)
• Pocket book of hospital care for children (Second edition): guidelines for the management of common childhood
illnesses (WHO 2013)
Bibliography


















