HIV & Children
41
HIV & Children Dr Emma Rutland Consultant in GU & HIV Medicine
-
Upload
samantha-horton -
Category
Documents
-
view
25 -
download
2
description
HIV & Children. Dr Emma Rutland Consultant in GU & HIV Medicine. Prevalence & demographics Adult HIV Paediatric HIV Consequences of undiagnosed HIV Testing Paediatric HIV management. Prevalence & demographics Adult HIV Paediatric HIV Consequences of undiagnosed HIV Testing - PowerPoint PPT Presentation
Transcript of HIV & Children

HIV & Children
Dr Emma RutlandConsultant in GU & HIV Medicine
• Prevalence & demographics– Adult HIV– Paediatric HIV
• Consequences of undiagnosed HIV• Testing• Paediatric HIV management
• Prevalence & demographics– Adult HIV– Paediatric HIV
• Consequences of undiagnosed HIV• Testing• Paediatric HIV management

HIV in the UK: how big a problem?
• Number of HIV+ve living in UK = 91,500*• 24% of HIV+ve people are unaware of their infection*
*HPA: HIV in the united kingdom; 2011 report.

The UK national guidelines for testing advocate the offer and recommendation to accept an HIV test to all adults registering in general practice and general medical admissions patients in areas where diagnosed HIV prevalence is greater than 2 per 1,000 population.
Prevalence of diagnosed HIV infection, UK: 2009
HPA: HIV in the united kingdom; 2010 report. http://www.hpa.org.uk

Estimated number of people living with HIV infection: United Kingdom, 2010
Total with HIV = 91,500 (85,400 − 99,000)
Total diagnosed = 69,250 (67,800 − 70,800)
Total undiagnosed = 22,200 (16,350 − 29,650)
HPA: HIV in the UK; 2010 report. http://www.hpa.org.uk

Prevalence rates of HIV: United Kingdom, 2010
People with diagnosed or undiagnosed HIV infection/1000 population
All 1.5
Men 2.0
Women 0.9
MSM 47
Black African 47
HPA: HIV in the UK; 2010 report. http://www.hpa.org.uk

Distribution of people receiving HIV care by age group: United Kingdom, 2001 and 2010
HPA: HIV in the UK; 2010 report. http://www.hpa.org.uk
MTCT• No intervention =
*Townsend et al AIDS 2008, 22:973-81

MTCT• No intervention = 25.6%
*Townsend et al AIDS 2008, 22:973-81

MTCT• No intervention = 25.6%• Breast feeding =
*Townsend et al AIDS 2008, 22:973-81

MTCT• No intervention = 25.6%• Breast feeding = 14%
*Townsend et al AIDS 2008, 22:973-81

MTCT• No intervention = 25.6%• Breast feeding = 14%
Transmission rates UK and Ireland 2000-2006* • Overall MTCT = 1.2% (n=5151)• AZT monotherapy & Caesarean section = 0% (n=464)• HAART & planned Caesarean section = 0.7% (n=2286)• HAART & planned vaginal delivery = 0.7% (n=559)• HAART & VL<50 copies/mL = 0.1% (n=2117)
(= 3 transmissions. 2 of these babies had evidence of in utero transmission)
*Townsend et al AIDS 2008, 22:973-81

CHIPS Cohort (up to March 2011)• N = 1190 children who are alive and in active follow-up • 48% born UK/Ireland, 51% born abroad • Ethnicity:
• Diagnosis of maternal infection (N=1158 vertically infected):
n %
White 70 (6%)
Black African 944 (79%)
Black other 14 (1%)
Indian SC 17 (1%)
Mixed 123 (10%)
Other 13 (1%)
Not known 9 (1%)
n %
Known after delivery 977 (84%)
Known before delivery 146 (13%)
Not known 35 (3%)
National Study of HIV in pregnancy and Childhood http://www.nshpc.ucl.ac.uk/ Collaborative HIV Paediatric study http://www.chipscohort.ac.uk

Age at diagnosis
• Most HIV infected children will become ill in the 1-2 years of life.
• However, a significant number of young people with vertically acquired HIV infection are surviving childhood, without treatment, to be diagnosed in adolescence.

Example of natural progression of HIV infection in an adult individual over time
Time Post Infection
1000
500
200
2 4 6 2 3 4 5 6 7 8 9 10 11 12
(weeks) (years)
CD
4 C
ou
nt
(cel
ls/m
m3 )
Both AIDS and low CD4 counts are
markers of long-standing infection
(prior to treatment)
Diagnosis can be made at any time
AIDS event and diagnosis becomes increasingly likely
Data source: Health Protection Agency CD4 surveillance

Age at diagnosis
• 2009 analysis of children diagnosed >13 years old in UK:– 42 young people were located – 20% were at an advanced stage of disease at diagnosis– 50% had CD4 <200 cells/μl– 50% were asymptomatic
Judd A, Ferrand R, Jungmann E et al. Vertically acquired HIV diagnosed in adolescence and early adulthood in the UnitedKingdom and Ireland: findings from national surveillance. HIV Med, 2009, 10, 253–256.
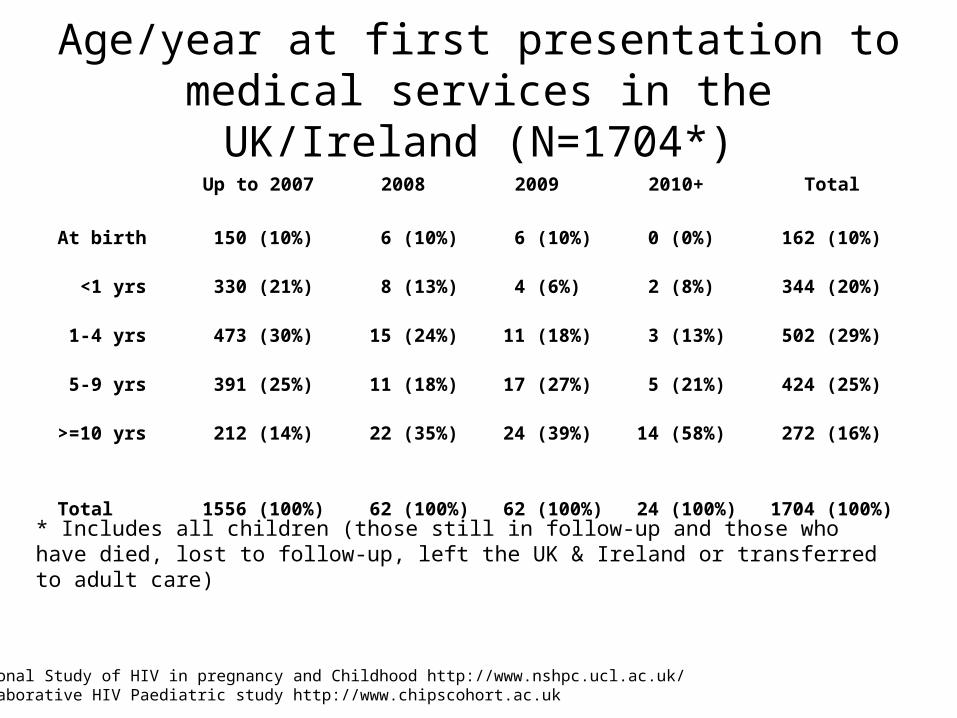
Age/year at first presentation to medical services in the UK/Ireland (N=1704*)
Up to 2007 2008 2009 2010+ Total
At birth 150 (10%) 6 (10%) 6 (10%) 0 (0%) 162 (10%)
<1 yrs 330 (21%) 8 (13%) 4 (6%) 2 (8%) 344 (20%)
1-4 yrs 473 (30%) 15 (24%) 11 (18%) 3 (13%) 502 (29%)
5-9 yrs 391 (25%) 11 (18%) 17 (27%) 5 (21%) 424 (25%)
>=10 yrs 212 (14%) 22 (35%) 24 (39%) 14 (58%) 272 (16%)
Total 1556 (100%) 62 (100%) 62 (100%) 24 (100%) 1704 (100%) * Includes all children (those still in follow-up and those who have died, lost to follow-up, left the UK & Ireland or transferred to adult care)
National Study of HIV in pregnancy and Childhood http://www.nshpc.ucl.ac.uk/ Collaborative HIV Paediatric study http://www.chipscohort.ac.uk

Age/year at first presentation to medical services in the UK/Ireland (N=1704*)
Up to 2007 2008 2009 2010+ Total
At birth 150 (10%) 6 (10%) 6 (10%) 0 (0%) 162 (10%)
<1 yrs 330 (21%) 8 (13%) 4 (6%) 2 (8%) 344 (20%)
1-4 yrs 473 (30%) 15 (24%) 11 (18%) 3 (13%) 502 (29%)
5-9 yrs 391 (25%) 11 (18%) 17 (27%) 5 (21%) 424 (25%)
>=10 yrs 212 (14%) 22 (35%) 24 (39%) 14 (58%) 272 (16%)
Total 1556 (100%) 62 (100%) 62 (100%) 24 (100%) 1704 (100%) * Includes all children (those still in follow-up and those who have died, lost to follow-up, left the UK & Ireland or transferred to adult care)
National Study of HIV in pregnancy and Childhood http://www.nshpc.ucl.ac.uk/ Collaborative HIV Paediatric study http://www.chipscohort.ac.uk

• Prevalence & demographics– Adult HIV– Paediatric HIV
• Consequences of undiagnosed HIV• Testing• Paediatric HIV management

The consequences of undiagnosed HIV in children
• Increased morbidity and mortality (particularly high risk of rapid HIV progression and death in infancy)
• Increased admissions, including ITU and transfer to specialist centres
• Increased health care related costs• Poorer response to antiretroviral medication• Public health issue of onward transmission


• Prevalence & demographics– Adult HIV– Paediatric HIV
• Consequences of undiagnosed HIV• Testing• Paediatric HIV management


Who to test
• All children where a parent or sibling is known to have HIV or may have died of an HIV associated condition
• Where no documentation of the childʼs previous negative HIV test result is provided
• Children with signs and symptoms consistent with an HIV diagnosis

ClClinical Indicator diseases for paediatric HIV infectionHIV testing guidelines 2008
http://www.bhiva.org/documents/Guidelines/Testing/GlinesHIVTest08.pdf

Who to test
• All children where a parent or sibling is known to have HIV or may have died of an HIV associated condition
• Children whose father has HIV and motherʼs HIV status is unknown.• Where no documentation of the childʼs previous negative HIV test
result is provided• Children with signs and symptoms consistent with an HIV diagnosis• Children being investigated for a congenital immunodeficiency• Children newly arrived in the UK from high-prevalence areas (they
may be unaccompanied minors)• Children who are presented for fostering/adoption where there is
any risk of blood borne infections.• Children at risk of non-vertically acquired infection including cases
of sexual abuse

Barriers to testing - Parents
• The child is well (perceived as incompatible with HIV infection)
• The parent may be newly diagnosed and not fully accepting their own diagnosis.
• Fear of disclosure of own status• Fear of rejection from children / partner• Parental experience of / or perception of stigma• The inability to cope with a positive diagnosis• The fear of feeling guilty if the child was diagnosed positive

Barriers to HIV testing – health care professionals
• Perception that teenage children would have presented symptomatically by now
• Lack of experience with HIV, lack of confidence
• Not considering it in the differential diagnosis
• Not considering child at risk
• Concerns about ‘making judgements’
• Fear of having to give positive result
• Concerns about confidentiality, child protection issues
• Lack of incentives to test
Timeline for testingThe Asymptomatic child• 6-12 months from initial discussion with parents before referral to
social services • Parents will have to engage with relevant healthcare services (e.g.
GP, Paediatric HIV Team, HIV counsellor..)
The acutely ill / symptomatic child.• Immediate testing required • Discussion with local specialist paediatric services
Young infants (0–1 year)• Timescale is more urgent as the risk of disease progression in the
first year of life is high.
For sexually active young people• The possibility of onward transmission makes testing urgent

Consent to test
Consent to testing: infants and younger children• Consent required from person with parental responsibility • Full disclosure of parents HIV diagnosis not always appropriate or necessary
Consent to testing: older children• Older children may consent if they are considered to be Gillick competent• Can be challenging if the parent does not want to disclose their diagnosis • Parents should strongly be encouraged to discuss the test with their child• Work with the parents to find a way forward • A plausible explanation could be; ‘as you were born abroad, we would like
to test you for a variety of bloodborne viruses which are more common where you were born, such as hepatitis B (the importance of that is that it can affect your liver); HIV (which can be treated); and a full blood count (to see if you’re anaemic)’.

Pre-test discussion – older competent child
– Benefits for testing (prognosis, treatment available in UK, risks of transmission, )
– Consequences for not testing (i.e. risks of becoming unwell, death)
– When possible, a full history of childʼs health including birth and country of origin, breastfeeding, past medical history, transfusions, etc
– Any concerns raised by the family (e.g. disclosure to the child or partner, fears of positive result, family issues…)
– Details of how the result will be given
• Document in the patients notes with any relevant discussion• Written consent from patient is unnecessary

Which test to use?
• Children < 18 months should be tested for genomic evidence of HIV by PCR
• Children > 18 months should have an HIV antibody test

Parental refusal to consent to testing
The rights of the child• Children Act 1989• Working together to Safeguard
Children 2006• UN Convention on the Rights of the
Child.• Article 2 or 6 - the right to life.• Article 24 – the right to the highest
attainable standard of health.
The rights of the parent• Disclosure of a parents HIV status
infringes his/her right to medical confidentiality.
• It also infringes his/her right to respect for his private life under article 8 (European Convention on Human Rights, 1954).
If a parent refuses to allow the child to be tested or if a Gillick competent child refuses to be tested, appropriate legal advice should be sought and as a last resort the case will need to be referred to the courts.

• Prevalence & demographics– Adult HIV– Paediatric HIV
• Consequences of undiagnosed HIV• Testing• Paediatric HIV management

Paediatric HIV• N = 1190 children who are alive and in active follow-up (up to March 2011)
• ‘Ageing cohort’ - the proportion of the cohort aged ≥10 years increased from 11% to 70% in last 15 years
• Aims of treatment– Viral load suppression– Immune reconstitution– Reduction HIV related complications (OI, HIV encephalopathy,
malignancies)– Maintain adherence to minimise risk of drug resistance
Collaborative HIV Paediatric study http://www.chipscohort.ac.uk

ARV therapy in children• Indication to start is age dependant:
– All infants under 1 year should be treated– All children with symptomatic HIV should be treated– Children >5 years are treated according to adult CD4 criteria
• Choice of ARV limited by lack of safety data• Additional factors to be considered in children include pill burden,
swallowing tablets, likely adherence patterns• Age appropriate education and adherence programmes vital for success
• 15% ARV naive• 82% had undetectable viral load after starting ARV (85% in adults)
• Average age for transition to adult services is 17 years old
Collaborative HIV Paediatric study http://www.chipscohort.ac.uk SOPHID 2011 data www.hpa.org.uk

Summary
• Most HIV infected children in the UK are vertically infected, and half were born abroad.
• Many will become symptomatic within the first 1–2 years of life; however, some may remain asymptomatic well into adolescence.
• Parents may have major concerns about testing their children for HIV• HIV testing of children is clearly in the medical interests of the child and,
in the majority of cases, is straightforward. However, if the parents consistently refuse it may become a child-protection issue and need to involve the courts.
• A clear pathway of referral between health and social care needs to be identified to manage cases where parents refuse testing
Useful websites for guidelines:www.chiva.org.ukwww.bhiva.org.uk
WHO clinical staging of HIV/AIDS for children with confirmed HIV infection (2006)
Clinical Stage 1AsymptomaticPersistent generalized lymphadenopathy
Clinical Stage 2Unexplained persistent hepatosplenomegalyPapular pruritic eruptionsExtensive wart virus infectionExtensive molluscum contagiosumFungal nail infectionsRecurrent oral ulcerationsUnexplained persistent parotid enlargementLineal gingival erythemaHerpes zosterRecurrent or chronic upper respiratory tract infections (otitis media,
otorrhoea, sinusitis, tonsillitis)

WHO clinical staging of HIV/AIDS for children with confirmed HIV infection (2006)
Clinical Stage 3Unexplained* moderate malnutrition not adequately responding to standard
therapyUnexplained persistent diarrhoea (14 days or more)Unexplained persistent fever (intermittent or constant, > 1 month)Persistent oral candidiasis (after first 6–8 weeks of life)Oral hairy leukoplakiaAcute necrotizing ulcerative gingivitis/periodontitisLymph node TBPulmonary TBSevere recurrent bacterial pneumoniaSymptomatic lymphoid interstitial pneumonitisChronic HIV-associated lung disease including bronchiectasisUnexplained anaemia , neutropenia or chronic thrombocytopenia

WHO clinical staging of HIV/AIDS for children with confirmed HIV infection (2006)
Clinical Stage 4Unexplained severe wasting, stunting, severe malnutrition not responding to standard
therapyPneumocystis pneumoniaRecurrent severe bacterial infections (e.g. empyema, bone or joint infection, meningitis)Chronic HSV infection; (orolabial or cutaneous for > 1 month or visceral at any site)Extrapulmonary/disseminated tuberculosisDisseminated non-tuberculous mycobacteria infectionKaposi’s sarcomaOesophageal candidiasis (or candidiasis of trachea, bronchi or lungs)CNS Toxoplasmosis (after 1 month of life)HIV encephalopathyCMV retinitis or CMV infection affecting another organExtrapulmonary cryptococcosis (including meningitis)Disseminated endemic mycosis (extrapulmonary histoplasmosis, coccidiomycosis,)Chronic cryptosporidiosis, Chronic isosporiasisHIV associated tumours including cerebral or B cell non-Hodgkin lymphomaProgressive multifocal leukoencephalopathySymptomatic HIV-associated nephropathy or HIV-associated cardiomyopathy