HIV Cases “What to Start”
20
HIV Cases “What to Start” Dr Anton Pozniak Chelsea and Westminster Hospital London
description
HIV Cases “What to Start”. Dr Anton Pozniak Chelsea and Westminster Hospital London. Case-SP. A 57 year old caucasian man presented to the emergency department with progressive difficulty in swallowing over the last 4 weeks. - PowerPoint PPT Presentation
Transcript of HIV Cases “What to Start”

HIV Cases“What to Start”
Dr Anton PozniakChelsea and Westminster Hospital
London

Case-SP• A 57 year old caucasian man presented to the emergency
department with progressive difficulty in swallowing over the last 4 weeks.
• He is hypertensive and has diet controlled diabetes and asthma and takes inhaled B2 agonists and inhaled steroids
• He had seen his family practitioner who saw oral thrush and thought it was related to his diabetes/ inhalers and gave him amphotericin lozenges
• He had been diagnosed with HIV a year before but had not attended any clinics as he “felt well”

Case-SP• He had extensive oral thrush and had severe dysphagia• BP 145/90 mmHg• He was admitted and treated with fluconazole
• Social History– Lives alone is MSM– Smokes 15 a day– Alcohol 20 units a week, no recreational drugs
• Drugs– Salbutamol inhaler – Fluticasone Inhaler– Amlodopine– St Johns Wort for depression

Case-SP• Labs• STD screen negative • FBC,U and Es, LFTs Normal ,• Cr CL 69 mls/min, Urine protein +no glucose• CD4 33 cells/uL• VL 365000 copies/ml• Hep B immune • Hep C negative • STS negative• Resistance test and HLA B5701 awaited• Framingham 10 year risk risk 18%

You decide to start ARVs Regimen DHHS[1] IAS[2] EACS[3]
EFV/TDF/FTC Preferred Recommended RecommendedATV/RTV + TDF/FTC Preferred Recommended RecommendedDRV/RTV + TDF/FTC Preferred Recommended RecommendedRAL + TDF/FTC Preferred Recommended RecommendedLPV/RTV + TDF/FTC Alternative Alternative Recommended
EFV + ABC/3TC Alternative Alternative Recommended
ATV/RTV + ABC/3TC Alternative Alternative Recommended
DRV/RTV + ABC/3TC Alternative Alternative Recommended
NVP + TDF /FTC Acceptable Alternative Recommended
MVC + TDF/FTC Acceptable Alternative Alternative
RPV + TDF /FTC Alternative No recommendation No recommendation
RAL + ABC/3TC Alternative No recommendation No recommendation
1. DHHS Guidelines, March 2012. 2. T. JAMA. 2012;304:321-333. 3. EACS Guidelines, November 2011.

You decide to start ARVs
What is your choice of main agent?• NNRTI• PI/r• Integrase• other

Difficulties in choosing-which 3rd agent?
• NNRTI-– may have transmitted dug resistance– RPV may not be effective in High viral load
• Integrase– BD – and may have NRTI transmitted dug resistance
• PI/r– drug interactions,– diabetes, lipids

NNRTI/NRTI and Prevalence of Transmitted Drug Resistance
2.5%2.9%
5.0%
8.9%
0.8% 0.4%
0%
2%
4%
6%
8%
10%
12%
Any class NRTI NNRTI PI Multi DrugRestistance (2
classes)
Multi DrugResistance (3
classes)
prev
alen
ce o
f mut
atio
ns
Eacs 2011 SPREAD

If you decide to give a boosted PIDrug Interactions
• What Drugs have significant interactions with a boosted PI?
1 St Johns Wort 2 Fluticasone 3 Amlodopine 4 None5 all

What NRTI back bone?
• AZT/3TC• ABC/3TC• TDF/FTC• DDI/3TC• OTHER

Difficulties in choice of NRTI
• AZT-– lipodystrophy– BD
• ABC– High Viral load– Cardiovascular risk(smoker and diabetic and BP)
• TDF– Renal changes,– Bone changes

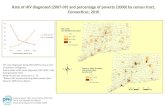
CVD – Do drugs matter? D:A:D: Recent and/or cumulative ARV exposure and risk of MI
Adapted from Lundgren JD, et al. CROI 2009. Oral presentation 44LB.
RR
of c
umul
ativ
e ex
posu
re/y
ear
95%
CI
# PYFU: 138,109 74,407 29,676 95,320 152,009 53,300 39,157# MI: 523 331 148 405 554 221 139
RR
of r
ecen
t* e
xpos
ure
yes/
no95
%C
I
1.9
1.51.2
1.0
0.8
0.6ZDV ddI ddC d4T 3TC ABC TDF
# PYFU: 68,469 56,529 37,136 44,657 61,855 58,946# MI: 298 197 150 221 228 221
IDV NFV LPV/RTV SQV NVP EFV
PI† NNRTI1.2
1.13
1.0
1.1
0.9
1.9
1.51.2
1.0
0.8
0.6
*Current or within past 6 months; †Approximate test for heterogeneity: p=0.02; **not shown due to low number of patients receiving ddC
RR
of c
umul
ativ
e ex
posu
re/y
ear
95%
CI
NRTI
CVD=cardiovascular disease; ARV=antiretroviral; MI=myocardial infarction; RR=relative risk; NRTI=nucleoside reverse transcriptase inhibitor; PI=protease inhibitor; NNRTI=nonnucleoside reverse transcriptase inhibitor; PYFU=patient years of follow up
**

0.27
0.21
0.51
1.16
-0.26
-0.43
-0.45
-0.53
0.008
-0.11
0.03
0.31
-0.8 -0.4 0 0.4 0.8 1.2
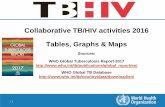
Mantel-Haenszel Risk Difference % (95% CI)
All Trials n=26
GSK Trials n=16
NIH Trials n=5
Academic Trials n=5
Created from Ding X, et al. CROI 2011. Poster presentation 808.
• Meta-analysis of Phase II–IV RCTs including ABC – Mean follow up 1.6
person-years per subject– Patients: 80% male (mean
age=39 years)• Limitations
– Young adults, so underlying MI risk low
– Other CV risk factors usually unknown
– Unvalidated MIs– Some studies had a PI
control group
CVD: Do drugs matter?FDA meta-analysis of abacavir and MI
CVD=cardiovascular disease; FDA=Food and Drug Administration; MI=myocardial infarction; RCTs=randomised controlled trials; CV=cardiovascular; PI=protease inhibitor

Chronic renal disease: ART risk factors
• 6,843 patients (5,136 male), median age 43 yrs, 90.1% exposed to cART, CD4 450 cells/mm3, 21.7% hypertension, 4.9% diabetes
• Median follow up 3.7 years• 2-fold increased risk if hepatitis C RNA+
Adapted from Mocroft A, et al. AIDS. 2010;24:1667–8.
Multivariate analysis
IRR/ year p
Tenofovir 1.16 <0.0001Indinavir 1.12 <0.0001Atazanavir 1.21 0.0003Lopinavir/r 1.08 0.030%
pro
gre s
sed
to C
KD
Incidence: 1.05 (0.91–1.18)/100 PYFU
MonthsART=antiretroviral therapy; PYFU=patient years follow up; IRR=incidence rate ratio

1. Adapted from McComsey G, et al. JID. 2011;203:1791–801.
ACTG 5224 & SMART: BMD loss with ART initiation ~2-4% at 1-2 yrs1
Low bone density/fracture: Relationship to ART
NRTI ComponentPrimary Analysis
NNRTI/PI ComponentSecondary Analysis
TDF/FTCABC/3TC
p=.004*
0-1
-2-3
-4-5Spi
ne B
MD
per
cent
cha
nge
from
wee
k 0
0 24 48 96 144 192Visit Week from Randomization
No. of subjectsTDF/FTC 128 111 105 97 87 53
130ABC/3TC 122 106 101 80 53
* - two-sample t-testNo significant interaction of NRTI and NNRTI/PI components (p=0.63)
Visit Week from RandomizationNo. of subjects
EFVATV/rtv
133 117 109 107 86 58125 116 102 91 81 48
EFVATV/rtv
p=.035*
0-1
-2-3
-4-5
0 24 48 96 144 192
p=.004*
ART=antiretroviral therapy; BMD=bone mineral density; DC=drug conservation; VS=viral suppression; NRTI=nucleoside reverse transcriptase inhibitor; NNRTI=nonnucleoside reverse transcriptase inhibitor; PI=protease inhibitor; DXA=dual-energy X-ray absorptiometry

Case-SP
• Resistance was wild type
• He starts EFV TDF FTC

Case AP
• 35 year old Asian women presents with• Night sweats, weight loss and cough• CXR - RUL cavity and infiltrates• AAFB - smear positive and started on RZHE• Had an HIV test and was positive CD4 was 35
cells/uL

Case AP• As her CD4 was<50 cells/uL she was offered
ARVs within 2 weeks of starting and tolerating her TB meds
What ARV combination would you offer her? What is your choice of main agent?
• NNRTI-Efavirenz• PI/r-Lopinavir/r• Integrase-Raltegravir• other

Case AP
• Started Efavirenz but couldn't tolerate it• What would you offer her?
• NNRTI-Nevirapine• PI/r-Lopinavir/r• Integrase-Raltegravir• other

Case AP• What would you offer her?• NNRTI-Nevirapine-less efficacy ? Drug
interaction• PI/r-Lopinavir/r major interaction with
rifampicin so switch to rifabutin or double dose lopinavir/r or high dose ritonavir 400mg bd
• Integrase-Raltegravir 400 or 800mg bd• Other-4 nucleosides