HIV, AGING and the LIVER - Virology...
35
Presented at the 6 th International Workshop on HIV & Hepatitis Co-infection, 31 May – 2 June 2010, Tel Aviv, Israel HIV, AGING and the LIVER Marie Marie - - Louise C. Louise C. Vachon Vachon , M.D., , M.D., M.Sc M.Sc . . Infectious Diseases / Liver Diseases Infectious Diseases / Liver Diseases Mount Sinai School of Medicine Mount Sinai School of Medicine
Transcript of HIV, AGING and the LIVER - Virology...
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
HIV, AGING and the LIVER
MarieMarie--Louise C. Louise C. VachonVachon, M.D., , M.D., M.ScM.Sc..Infectious Diseases / Liver DiseasesInfectious Diseases / Liver Diseases
Mount Sinai School of MedicineMount Sinai School of Medicine
Presenter
Presentation Notes
Aging is becoming a hot topic in HIV. We used to say the liver did not age, well we now have evidence that this is not the case. So for the next 30 minutes or so, I will review with you some of what we know occurs in the liver of aging HIV persons.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
The HIV-Infected Population is Aging
Increasing number of persons 50 years and older among new HIV infections1
44% in1995 vs
6% in 2000 vs
15% in 2005
Increasing number of persons 50 years and older living with HIV/AIDS in the US4From 2004 to 2007, the prevalence of persons living
with HIV/AIDS increased the most in those aged 40- 49 years old
In 2005, persons 50 years and older accounted for 35% of all deaths of persons living with AIDS.
1. CDC 2007. HIV/AIDS surveillance report, 2005.
Presenter
Presentation Notes
To start, some interesting numbers about the aging HIV population This is in part due to the increased survival in the post ART era.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
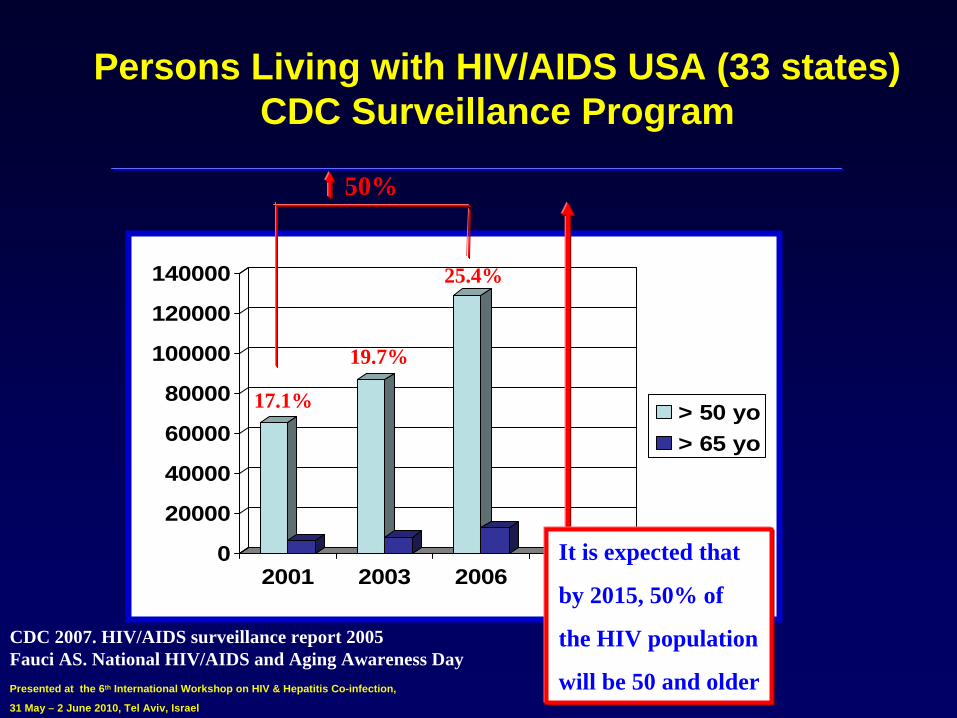
Persons Living with HIV/AIDS USA (33 states) CDC Surveillance Program
0
20000
40000
60000
80000
100000
120000
140000
2001 2003 2006
> 50 yo> 65 yo
17.1%
19.7%
25.4%
50%
CDC 2007. HIV/AIDS surveillance report 2005Fauci AS. National HIV/AIDS and Aging Awareness Day
It is expected that
by 2015, 50% of
the HIV population
will be 50 and older
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Complex Interactions between HIV and Aging Result in Accelerated Age-related Conditions
4Development of frailty, muscle wasting4 Insulin resistance, diabetes and cardiovascular disease4Chronic kidney disease4Bone disease4Cognitive impairment and dementia4HIV-related and unrelated malignancies
4Liver disease and HCC
Effros RB et al. Clin Infect Dis 2008
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Consequences of HIV, Aging and the Liver
Clinical manifestations of aging HIV and the liver4Chronic elevations of liver enzymes4Steatosis/steatohepatitis4 Increased drug-related toxicity4More severe liver disease in aging patients with hepatitis
B and C
Mortality associated with liver disease is high among HIV-infected patients1
42nd
cause of death
in HIV-infected patients after AIDS-
related complications44-fold increase
in morbidity and mortality due to liver
diseases among older patients1. Weber R. et al. arch Intern Med 2006.
Presenter
Presentation Notes
We see an increasing number Even in the HAART era
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Clinical case: Michelle
48 yo, AA woman
Referred in 2002 for suspicion of cirrhosis4HIV diagnosed in 1989 (nadir CD4+
T-cell: 220)
4No HBV/HCV co-infection4On didanosine + stavudine /PI, HIV RNA
undetectable4BMI 20, severe lipoatrophy4Thrombocytopenia (plt=80) and CT-SCAN of the
abdomen showed signs of portal hypertension
Presenter
Presentation Notes
This is one of our patients who was referred to us in 2002
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Complex interactions between aging, HIV, the immune system and the liver: role of
microbial translocation
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Aging, HIV and the Immune System: Interactions
Early immune senescence in HIV disease1
4Aging and HIV seem to share common mechanisms by which they alter cellular immunity
4 Immune activation and inflammation are characteristic of both aging and HIV infection
4 In HIV infection, microbial translocation might contribute to premature aging by promoting immune activation –
And may have direct effects on the liver2
1. Desai S and Landay A. Curr HIV/AIDS Rep 2010; 2. Balagopal A. et al. Gastroenterology 2008.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
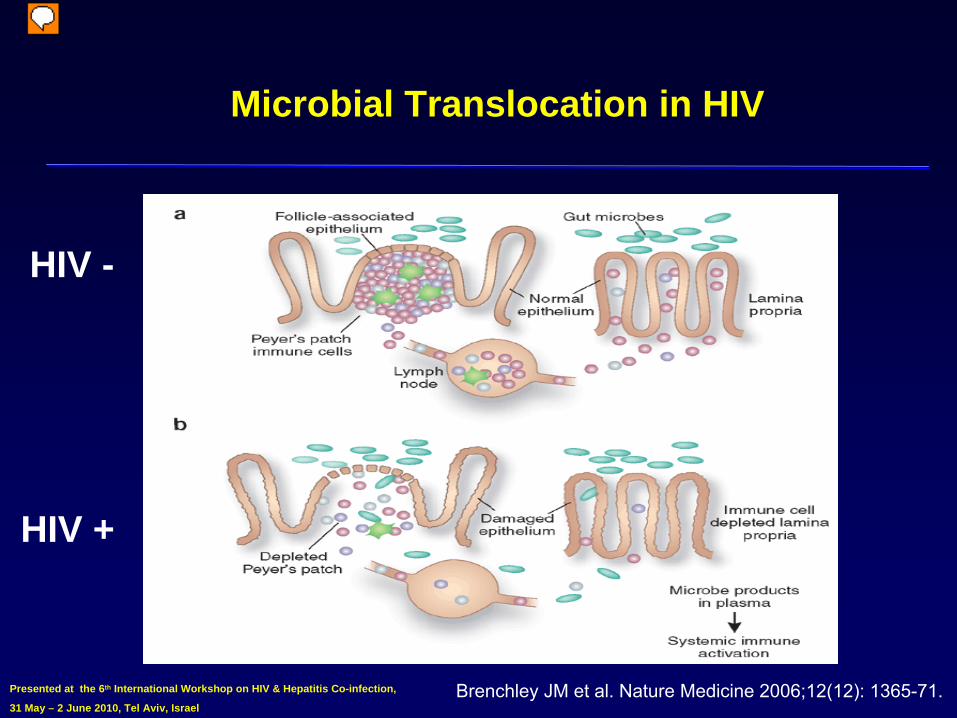
Microbial Translocation in HIV
HIV +
Brenchley
JM et al. Nature Medicine 2006;12(12): 1365-71.
HIV -
Presenter
Presentation Notes
HIV infection leads to CD4+ T cell depletion and this predominantly takes place in the GALT or gut associated lymphoid tissue which is the main reservoir of T-cells. Th-17 cells, the host defense against bacterial infections, are preferentially lost and this results in increase permeability of the gut membrane, the leaky gut. Microbes and microbial products can translocate and reach the portal and systemic circulation. This is measured by serum LPS. Microbial translocation is a cause of chronic immune activation.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
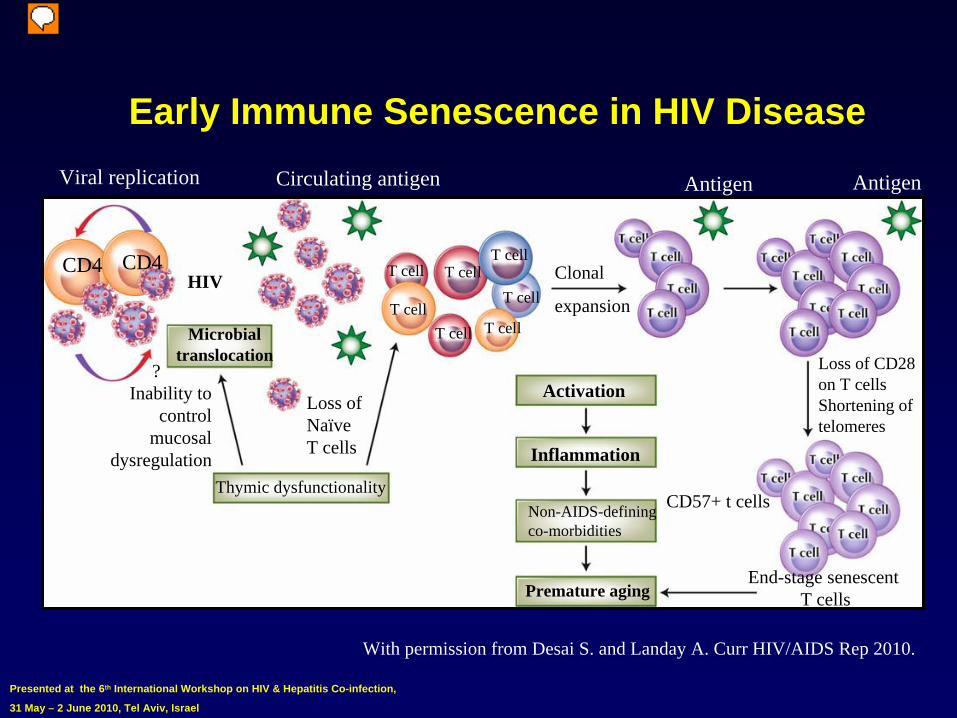
Early Immune Senescence in HIV Disease
CD4 CD4
T cell
T cell
T cell
T cell
T cell
T cell
T cell
Viral replication Circulating antigen
Clonal
expansion
Antigen Antigen
Microbialtranslocation
?Inability to
controlmucosal
dysregulation
Loss of NaïveT cells
HIV
Thymic dysfunctionality
Activation
Inflammation
Non-AIDS-definingco-morbidities
Premature aging
CD57+ t cells
Loss of CD28on T cellsShortening of telomeres
End-stage senescent T cells
With permission from Desai S. and Landay A. Curr HIV/AIDS Rep 2010.
Presenter
Presentation Notes
Even with ART, there is residual ongoing replication that continues to activate immune cells. Microbial translocation adds to circulating antigen. This immune activation is central in the HIV aging pathway.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Aging, HIV and the liver: interactions
Aging and the liver1,2
4
Decrease in liver volume
4
Impaired hepatic blood flow
4
Decreased amount of surface endoplasmic reticulum (SER)
4
Decline in regenerative response of hepatocytes
following liver injury
HIV and the liver3,4,5,6
4
Several liver cell types can be productively infected with HIV
4
Replication of HIV in hepatic stellate
cells by detection of
p24 ag
and HIV mRNA–
Pro-fibrogenic
(collagen I)
–
Pro-inflammatory (MCP-1)
1. Schmucker DL. Exp Gerontol. 2005; 2. Maclean AJ et al. J Pathol 2003; 3. Housset et al. Res Virol 1990; 4. Banerjee et al. AIDS 1992; 5. Blackard JT et al. J viral hepat. 2008; 6. Hong F et al. Hepatology 2010.
Presenter
Presentation Notes
We used to think that the liver was not aging because of its regenerative capacity, now we have evidence that it does. The liver SER is the principal site of drug metabolism. Decreased amount of SER coupled with an overall decrease in P450 activity contribute to the decline in phase I drug metabolism seen with aging and partly explains the increased susceptibility to drug-induced liver injury (DILI) in this group.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Clinical Manifestations of Aging Liver in HIV
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Chronic Elevation of Liver Enzymes in HIV
Abnormal liver enzymes are frequently seen in HIV infected patients (15-43%)1,2,3,4
Risk factors4 Increased BMI, hypertension, ART exposure, severe
alcohol use, HIV RNA level, low CD4 cell count, and age
No studies have compared the prevalence of liver enzymes elevation in younger vs
older HIV-infected
patients
1. Pol S et al. Clin Infect Dis 2004; 2. Maida I et al. J Acquir Immune Defic Syndr 2006; 3. Sterling RK et al. Dig Dis Sci 2008; 4. Kovari H et al. Clin Infect Dis 2010;
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Chronic Elevation of Liver Enzymes in HIV
Steatosis/steatohepatitis
is an emerging cause of chronic liver enzymes elevations in HIV1,2
430 HIV-infected patients on ART with transaminase elevation (> 6 months) were biopsied1
–
Mean age 46, duration of HIV infection 13 years–
18/30 had steatosis, 16/30 had steatohepatitis
–
Associated with insulin resistance424 HIV-infected patients were biopsied2
–
Mean age 50, duration of HIV infection 17 years, mean duration of ART 12 years
–
9/24 had steatohepatitis
(37.5%)
1. Ingiliz P et al. Hepatology 2009; 2. Morse C. et al. CROI 2009, abstract #748
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Steatosis and Steatohepatitis
67/216 (31%) of HIV-infected patients with NAFLD based on US examination2
4
Mean age 40 years, 94% male, mean duration of HIV 10 years, 65% on ART
165 patients with elevated liver enzymes and/or
steatosis
suggested at US4
55 underwent a liver biopsy–
20 of them (36%) had biopsy-proven steatosis
and 6 also had steatohepatitis
83/225 (37%) of HIV patients with NAFLD based on CT-
scans1
4
Mean age 48 years, 72% male, mean duration of HIV 13 years
Factors associated with steatosis4
Elevated ALT/AST, male sex, elevated waist circumference, and cumulative NRTI exposure
1. Guaraldi G. et al. Clin Infect Dis 2008. 2. Crum-Cianflone N et al. J Acquir Immune Defic Syndr 2009.
Presenter
Presentation Notes
Data on prevalence of steatosis and steatohepatitis among HIV-infected patients are limited mostly b/c HIV mono-infected patients don’t usually undergo a liver biopsy. Data from a cross sectional study identified steatosis in 31% of 216 patients based on US examination. In this study, factors associated with steatosis on ultrasound examination included increased waist circumference, elevated TG levels, and lower HDL. This is consistent with prevalence rates of steatosis in the general population of about 17-33% (this is US data), however, the mean age of the general population in these studies is higher than in the studies of HIV-infected patients.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
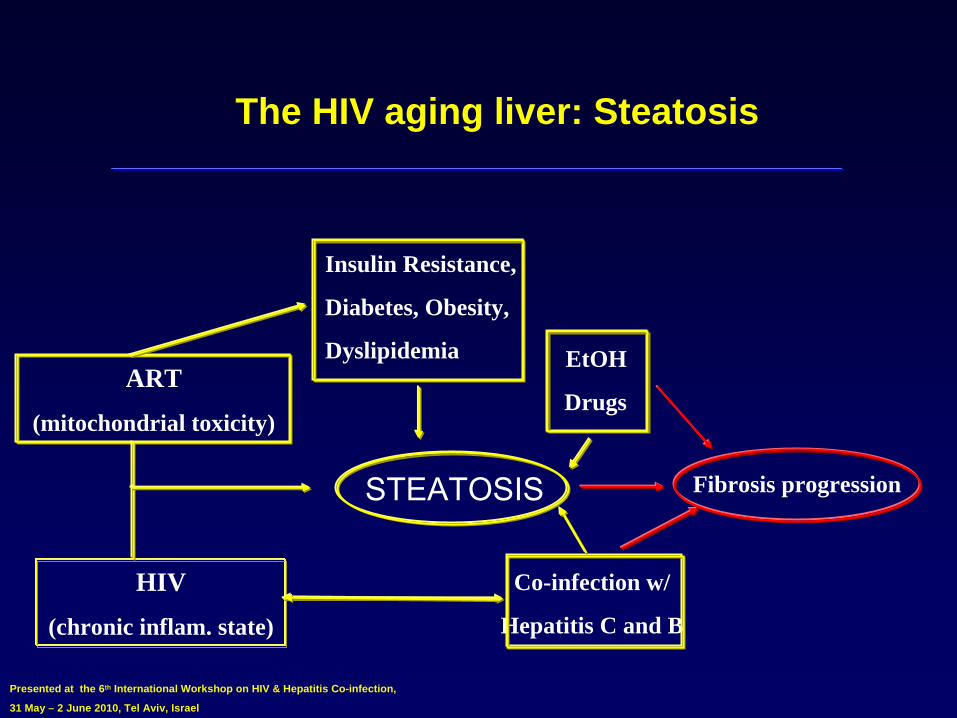
The HIV aging liver: Steatosis
STEATOSIS
HIV
(chronic inflam. state)
ART
(mitochondrial toxicity)
Fibrosis progression
Insulin Resistance,
Diabetes, Obesity,
Dyslipidemia EtOH
Drugs
Co-infection w/
Hepatitis C and B
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Drug-induced Toxicity
In the post ART era, drug-induced toxicity has become a major problem in the management of HIV1
4Mitochondrial toxicity and microvesicular
steatosis with NRTIs
4Liver enzyme elevations with NNRTIs
and PIs
Aging increases susceptibility to drug toxicity2,3
4 amount of SER + in P450 activity–
Decline in phase I drug metabolism
Increase pill burden in older HIV patients 4 Increased drug interactions and toxicity
1. Jain MK. Clin Liver Dis 2007; 2. Schmucker DL. Exp Gerontol. 2005; 3. Maclean AJ et al. J Pathol 2003
Presenter
Presentation Notes
The liver SER is the principal site of drug metabolism. Decreased amount of SER coupled with an overall decrease in P450 activity contribute to the decline in phase I drug metabolism seen with aging and partly explains the increased susceptibility to drug-induced liver injury (DILI) in this group.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Non Cirrhotic Portal Hypertension: Long-Term Liver Complication of ART
Case-series of HIV mono-infected patients with cryptogenic liver disease1,2,3,4
4Signs and symptoms of portal hypertension–
Thrombocytopenia
–
Hepatosplenomegaly–
Esophageal
varices (EV) / EV bleeding
–
Encephalopathy4Liver enzymes usually normal. INR, bilirubin
and
albumin normal4Prolonged exposure to ddI
and median duration of
HIV > 10 years1. Maida I et al. J Acquir Immune Defic Syndr 2006; 2. Mallet V. et al. AIDS 2007; 3. Schiano T. et al. Am J Gastroenterol 2007; 4. Stebbing J. et al. J Acquir Immnue Defic Syndr 2009.
Presenter
Presentation Notes
Parenchymal liver function is normal
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
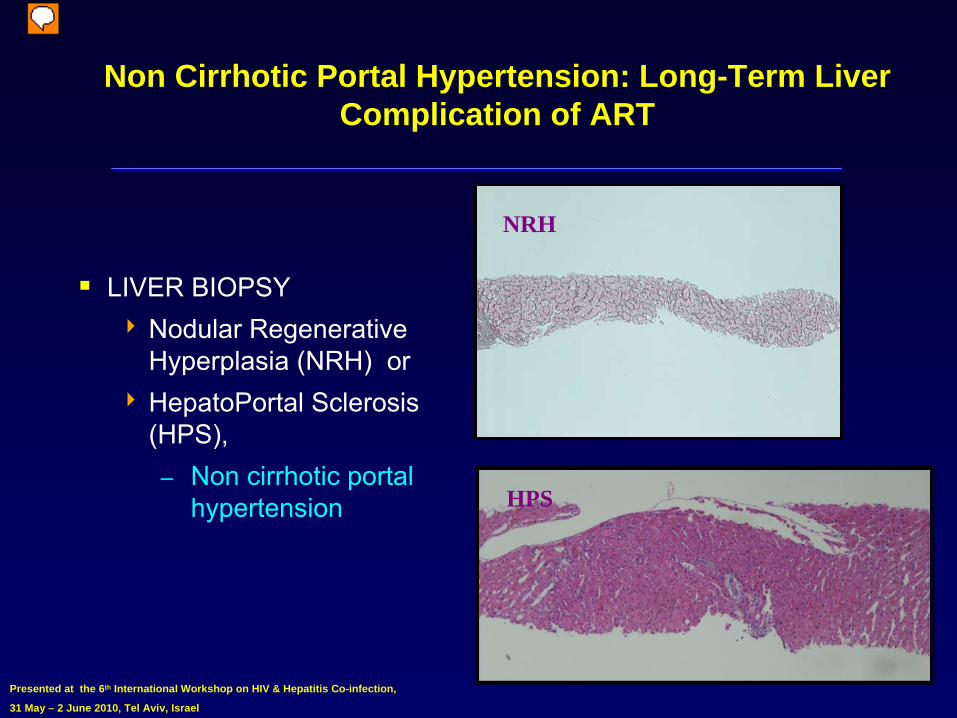
Non Cirrhotic Portal Hypertension: Long-Term Liver Complication of ART
LIVER BIOPSY4
Nodular Regenerative Hyperplasia (NRH) or
4
HepatoPortal
Sclerosis
(HPS),–
Non cirrhotic portal hypertension
NRH
HPS
Presenter
Presentation Notes
NRH and HPS may be part of a spectrum reflecting chronological progression of a single disease
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Non Cirrhotic Portal Hypertension: Long-Term Liver Complication of ART
In January of 2010, the United States Food and Drug Administration issued a statement that patients using Didanosine are at risk for a rare but potentially fatal liver disorder, non-cirrhotic portal hypertension
Presenter
Presentation Notes
Non cirrhotic portal hypertension is the topic of the next presentation by Dr Vincent Soriano so I will leave it to him to explain the details about this relatively new clinical entity.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
HCV Co-Infected Patients Are Aging
1st
cause of non-AIDS-related-deaths: LIVER1
4Risk factors for liver deaths: lower CD4+
T cell count,
IVDU, HCV, HBV and age (RR 1.3 per 5 years older)
Patients with chronic HCV get older2
4A recent multiple cohort model of HCV prevalence and disease progression (in the US) estimated the burden of HCV and cirrhosis for the next decades
1. Weber R et al. Arch Intern Med 2006; 2. Davis GL et al. Gastroenterology 2010; 3. Balagopal A et al. Gastroenterology 2008
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
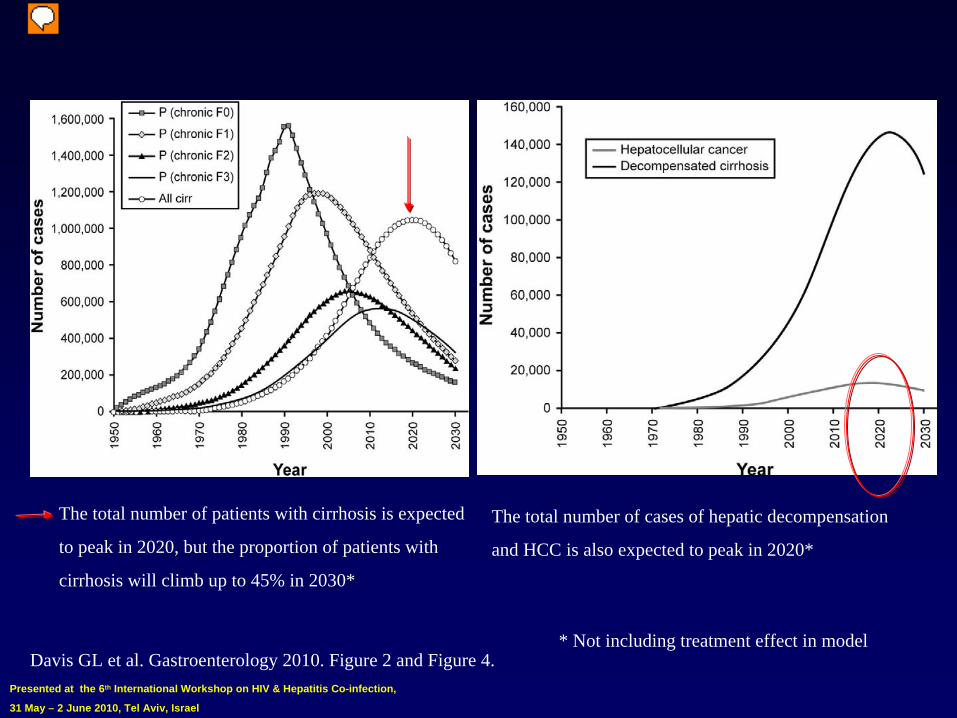
The total number of patients with cirrhosis is expected
to peak in 2020, but the proportion of patients with
cirrhosis will climb up to 45% in 2030*
The total number of cases of hepatic decompensation
and HCC is also expected to peak in 2020*
Davis GL et al. Gastroenterology 2010. Figure 2 and Figure 4.* Not including treatment effect in model
Presenter
Presentation Notes
When treatment effect of new HCV treatment is included in the model (assuming 80% chance of response and ½ of the patients treated), the model estimated that cirrhosis would be reduced by 15% after 10 years, or 30% if all would receive treatment. This is for HCV mono-infected patients, such a model was not done in coinfected.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
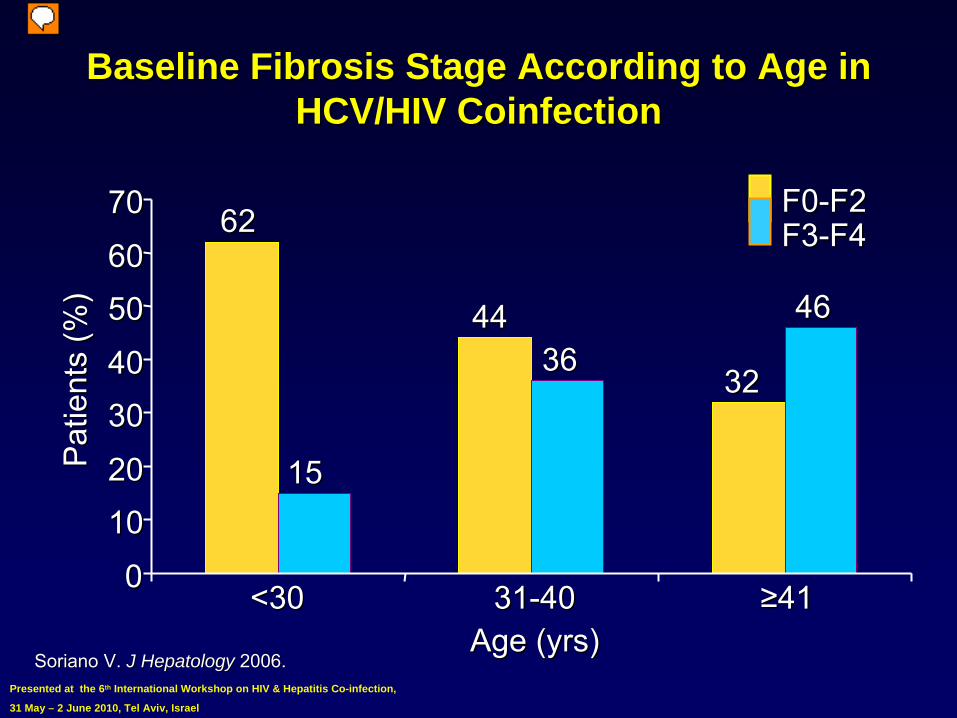
Baseline Fibrosis Stage According to Age in Baseline Fibrosis Stage According to Age in HCV/HIV HCV/HIV CoinfectionCoinfection
SorianoSoriano
V. V. J J HepatologyHepatology 2006.2006.
3131--4040<30<30 ≥≥4141Age (yrs)Age (yrs)
Pat
ient
s (%
)P
atie
nts
(%)
F0F0--F2F2F3F3--F4F46262
4444
3232
1515
36364646
001010202030304040505060607070
Presenter
Presentation Notes
Baseline Fibrosis Stage According to Age in HCV/HIV Coinfection These data are from a retrospective analysis of baseline biopsies from HIV-infected patients who were not receiving any HCV therapy during the analyzed trials. More rapid liver disease progression is seen in this population, leading to cirrhosis and end-stage liver disease complications (including hepatocellular carcinoma) at younger ages, and justifying HCV therapy as a priority in HCV/HIV coinfected patients. Reference Soriano V. Treatment of chronic hepatitis C in HIV-positive individuals: selection of candidates. J Hep. 2006;44:S44-S48.�
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Liver fibrosis is accelerated in HIV/HCV co- infected patients
Why?4Decreased immunity4HIV replication in stellate
cells
4ART toxicity?4Steatosis/steatohepatitis4Liver disease progression may be associated
with microbial translocation1
1. Balagopal A. et al. Gastroenterology 2008.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
HIV-related Microbial Translocation and Progression of Hepatitis C1
HIV-related CD4+ T-cell depletion associated with microbial translocation2
Markers of microbial translocation were strongly associated with HCV-related liver disease progression4Levels of LPS were elevated prior to recognition of
cirrhosis
1. Balagopal A et al. Gastroenterology 2008; 2. Brenchley JM et al. Nature Medicine 2006;12(12): 1365- 71
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
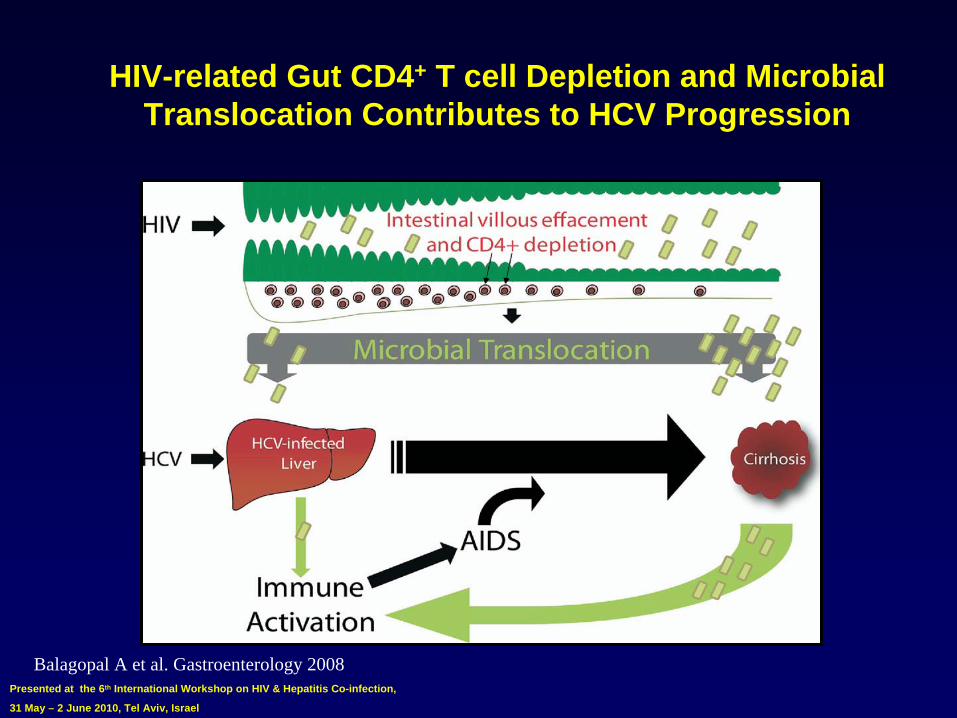
HIV-related Gut CD4+ T cell Depletion and Microbial Translocation Contributes to HCV Progression
Balagopal A et al. Gastroenterology 2008
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
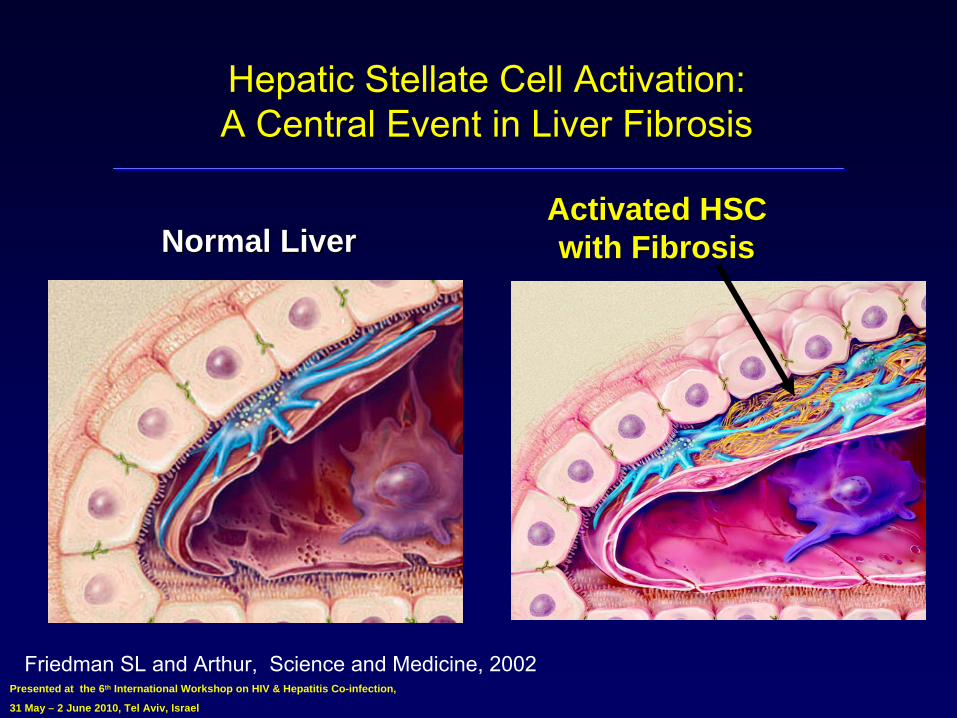
Hepatic Hepatic StellateStellate
Cell Activation: Cell Activation: A Central Event in Liver FibrosisA Central Event in Liver Fibrosis
Normal LiverNormal LiverActivated HSC Activated HSC with Fibrosiswith Fibrosis
Friedman SL and Arthur, Science and Medicine, 2002
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
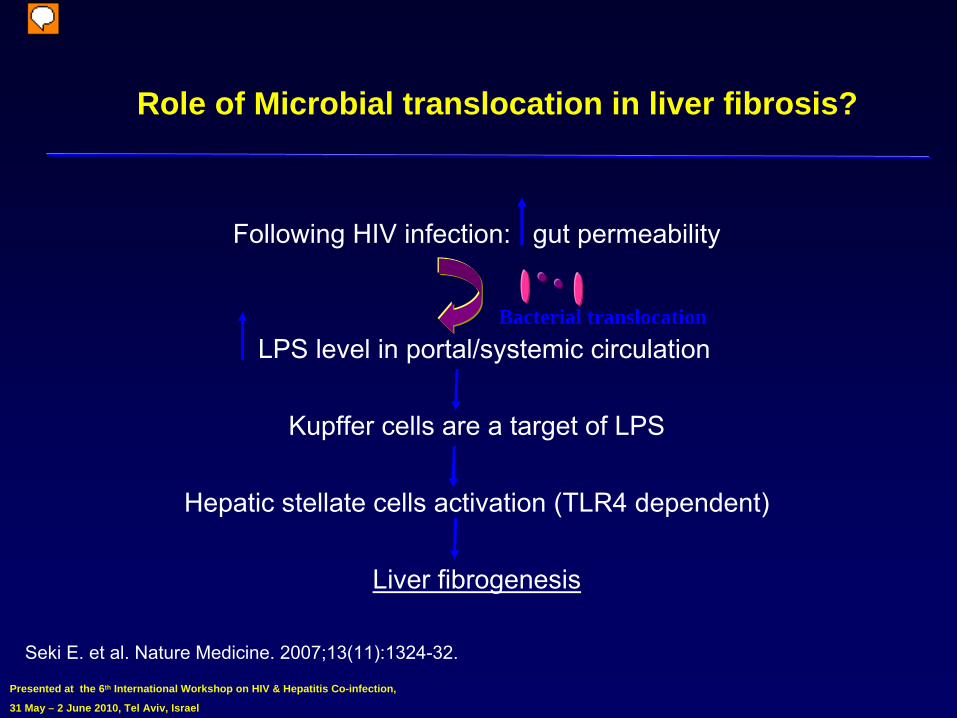
Role of Microbial translocation in liver fibrosis?
Following HIV infection: gut permeability
LPS level in portal/systemic circulation
Kupffer
cells are a target of LPS
Hepatic stellate
cells activation (TLR4 dependent)
Liver fibrogenesis
Seki E. et al. Nature Medicine. 2007;13(11):1324-32.
Bacterial translocation
Presenter
Presentation Notes
In the study referenced here, mice that were treated with antibiotics had a decrease in plasma LPS and significant reduction in hepatic fibrosis.
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
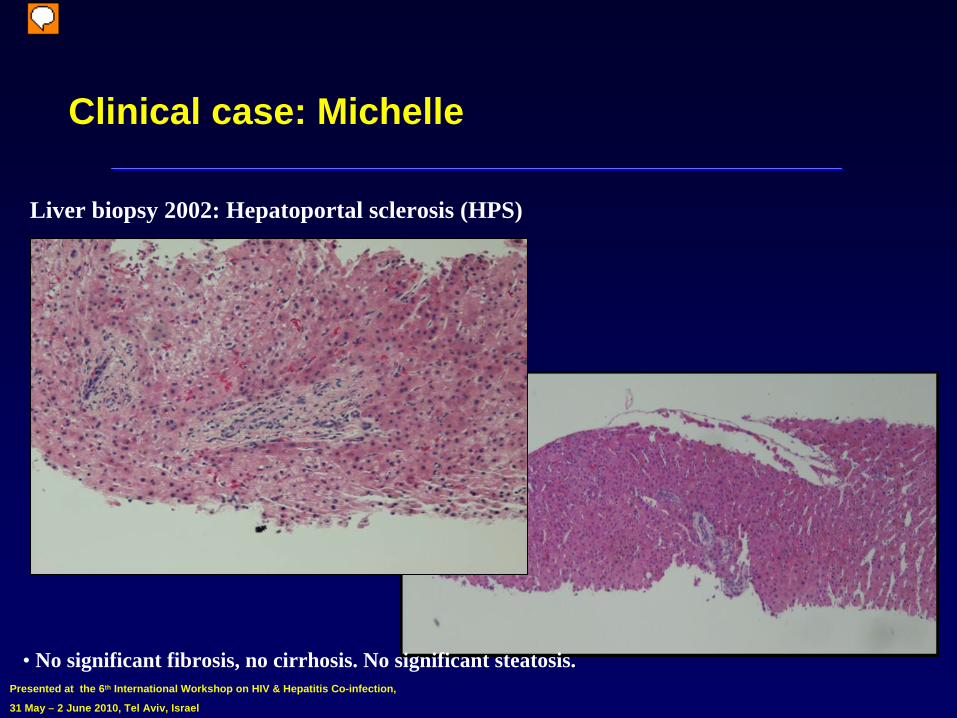
Clinical case: Michelle
• No significant fibrosis, no cirrhosis. No significant steatosis.
Liver biopsy 2002: Hepatoportal sclerosis (HPS)
Presenter
Presentation Notes
Consistent with hepatoportal sclerosis
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Dx: Non cirrhotic portal hypertension
Upper endoscopy: grade 3 varices: banded.
Trace ascites. No encephalopathy.
ART modified: tenofovir
DF + lamivudine
+ efavirenz
2 years later, ALT increases to 3X ULN
She had gained about 20 pounds in 1 year
Liver biopsy 2004
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
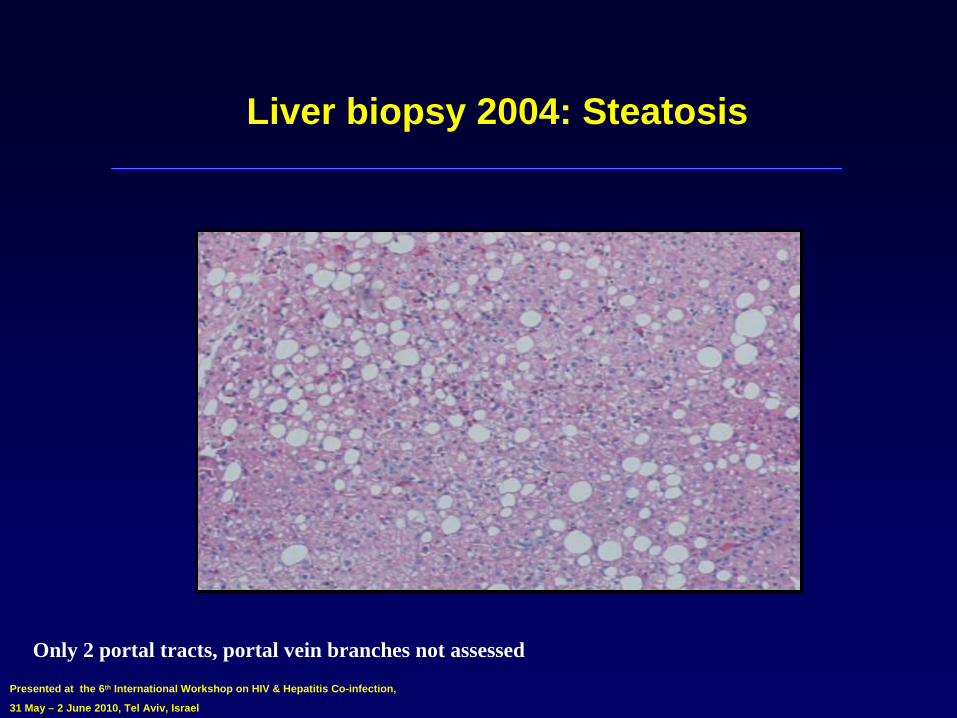
Liver biopsy 2004: Steatosis
Only 2 portal tracts, portal vein branches not assessed
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Since 2002
Still on TDF + lamivudine
+ efavirenz
Lost weight and ALT in the 30s
Bi-annual upper EGD: varices grade 1-2 in 02/2010, no bleeding, no further banding necessary
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
Conclusion
The liver is a major target of the aging process that occurs in HIV-infected patients
The causes are multiple:4Chronic immune activation4Accelerated senescence 4HIV effect on stellate
cells and liver fibrosis
4Microbial Translocation leading to progressive liver disease
4Worsening of chronic hepatitis
Recognize the clinical importance of the aging liver and tailor treatment accordingly
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel
1st International Workshop on HIV & Aging 4-5 October 2010, Baltimore, MD, USA4Abstract submission deadline August 7, 2010
Presented at the 6th International Workshop on HIV & Hepatitis Co-infection,
31 May – 2 June 2010, Tel Aviv, Israel P-35
Take care of your patients livers and they will all be Take care of your patients livers and they will all be smiling!smiling!