his.diva-portal.org › smash › get › diva2:1095143 › FULLTEXT01.pdf · The S.A.R.E.K...
18
Teknisk rapport HS-IIT-TR-17-001 Editor: Per Backlund 2017-05-12 The S.A.R.E.K Simulation Environment Technical description of a flexible training environment for prehospital care.
Transcript of his.diva-portal.org › smash › get › diva2:1095143 › FULLTEXT01.pdf · The S.A.R.E.K...
Teknisk rapport HS-IIT-TR-17-001 Editor: Per Backlund 2017-05-12
The S.A.R.E.K Simulation Environment Technical description of a flexible training environment for prehospital care.


Authors
Per Backlund (University of Skövde)
Henrik Engström (University of Skövde)
Mikael Johannesson (University of Skövde)
Mikael Lebram (University of Skövde)
Magnus Danielsson (Ambulance support unit at Skaraborgs hospital)
Magnus Hagiwara (University of Borås)
Lars Lundberg (University of Borås)
Hanna Maurin Söderholm (University of Borås)
Additional material:
http://edugamelab.hosting.his.se/sarek2/dokumentation/
https://www.youtube.com/watch?v=CO-mWrZcAPs
https://www.youtube.com/watch?v=R-o5m0COA0M
https://www.youtube.com/watch?v=enB0whmB5Ng

EXECUTIVE SUMMARY
This report contains a technical description of the result of the S.A.R.E.K (Simulation – Ambulance – Research – Education - Kinship) collaboration project and the Sim2020 project. The projects are collaborations between researchers in healthcare and IT, and prehospital care practitioners, with the aim to design, develop and test a contextualized simulation environment for prehospital care. We built a simulation environment representing the full depth and width of a prehospital care process. Breadth refers to including all phases of a prehospital mission, from dispatch to handover; while depth refers to detailed representations and recreation of artefacts, information and context for each of these phases. This report outlines the details of the overall design, all equipment and practical solutions used to create this.
Apart from the installation which is described in this report we have also developed methods and carried out a variety of tests and experiments which are reported elsewhere. The focus of this report is the system and its components.
Table of contents 1 A simulation environment for role-playing training in prehospital care ......................................... 1
2 System Description .......................................................................................................................... 2
2.1 Driving unit and transportation area ....................................................................................... 4
2.2 Scene room .............................................................................................................................. 5
2.3 Control room ........................................................................................................................... 6
2.4 Observation/debriefing room ................................................................................................. 6
3 Representation of Information ....................................................................................................... 7
4 Simulated Scenarios with Width and Depth ................................................................................... 9
4.1 Scenario width ......................................................................................................................... 9
4.2 Scenario depth......................................................................................................................... 9
4.2.1 Alarm: Receiving the call and transport to the scene of incident ................................. 10
4.2.2 On scene assessment .................................................................................................... 10
4.2.3 On scene treatment ....................................................................................................... 10
4.2.4 Scene departure and transport ..................................................................................... 11
4.2.5 Patient handover ........................................................................................................... 11
4.2.6 Reflection ....................................................................................................................... 11
5 References ..................................................................................................................................... 11


S.A.R.E.K Ambulance Training Environment
1
1 A simulation environment for role-playing training in prehospital care
The S.A.R.E.K Ambulance Training Environment was created to support contextualized enactment of patient care in live role-playing scenarios in a simulated prehospital environment. Patients can be simulated either by volunteer extras or by a patient simulator. So far we have mainly used a SimMan 3G (http://www.laerdal.com/se/SimMan3G) manikin to simulate patients. However, there is no restriction to this product in the set-up of the environment and it is outside the scope of this report to give a closer description of the manikin itself. The building blocks of S.A.R.E.K form an integrated simulation environment, consisting of physical parts, i.e. standard [facilities] and equipment, and a software part developed in-house. The overall vision of the system is to make it possible to enact realistic full scenarios covering all phases and aspects of prehospital care work, i.e. medical treatment, teamwork and communication throughout the entire prehospital process. The S.A.R.E.K Ambulance Training Environment supports flexible creation and visualization of physical environments as well as support for documentation and analysis of enacted training scenarios.
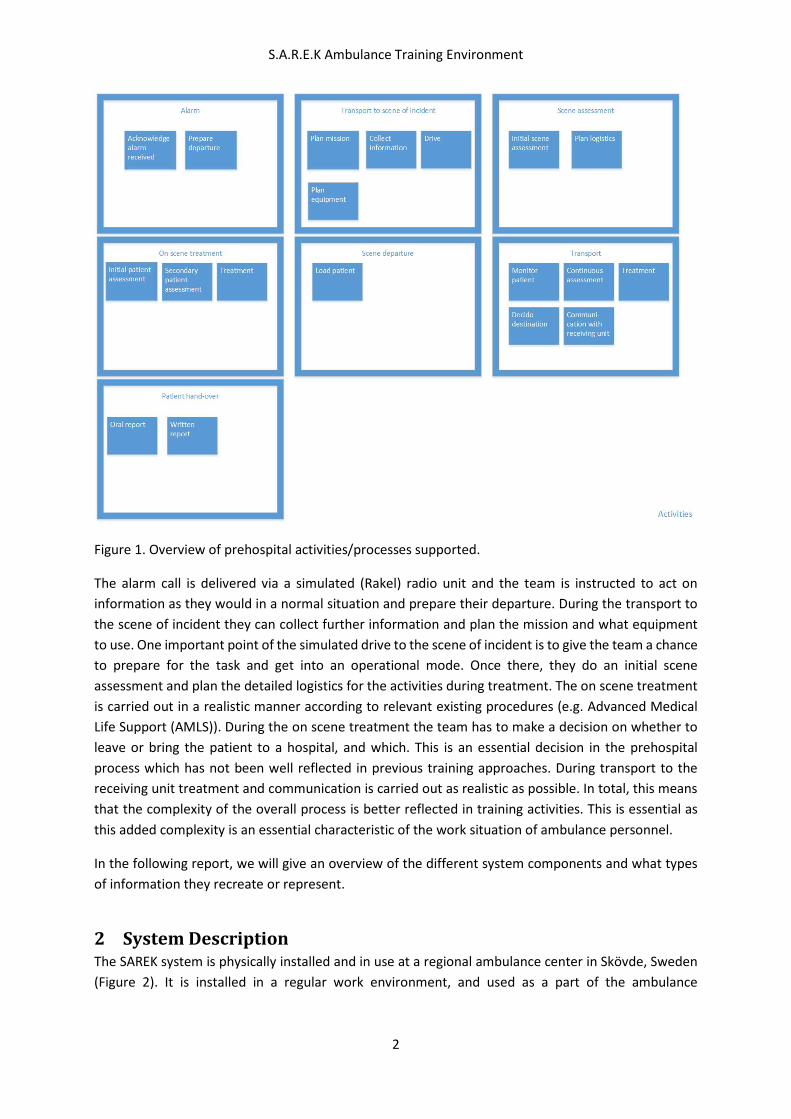
Coverage of the entire prehospital process and all its aspects is at the core of the philosophy behind the SAREK Ambulance Training Environment (Söderström, van Laere, Backlund and Maurin Söderholm, 2014). The need to support training activities throughout the process and to also capture aspects of prehospital care outside the scope of medical treatment was identified early on in the project. We refer to this as scenario width. In order to become relevant to the field of practice we have derived phases of the prehospital process from previous research in prehospital medicine (Jensen, Croskerry and Travers, 2011; Carter and Thompson, 2015): alarm, transport to the scene of incident, scene assessment, on scene treatment, scene departure, transport and patient hand-over (Figure 1). We created a work systems model (Söderström et al., 2014) to make a detailed account for the activities in the different phases and map them to training needs.
S.A.R.E.K Ambulance Training Environment
2
Figure 1. Overview of prehospital activities/processes supported.
The alarm call is delivered via a simulated (Rakel) radio unit and the team is instructed to act on information as they would in a normal situation and prepare their departure. During the transport to the scene of incident they can collect further information and plan the mission and what equipment to use. One important point of the simulated drive to the scene of incident is to give the team a chance to prepare for the task and get into an operational mode. Once there, they do an initial scene assessment and plan the detailed logistics for the activities during treatment. The on scene treatment is carried out in a realistic manner according to relevant existing procedures (e.g. Advanced Medical Life Support (AMLS)). During the on scene treatment the team has to make a decision on whether to leave or bring the patient to a hospital, and which. This is an essential decision in the prehospital process which has not been well reflected in previous training approaches. During transport to the receiving unit treatment and communication is carried out as realistic as possible. In total, this means that the complexity of the overall process is better reflected in training activities. This is essential as this added complexity is an essential characteristic of the work situation of ambulance personnel.
In the following report, we will give an overview of the different system components and what types of information they recreate or represent.
2 System Description The SAREK system is physically installed and in use at a regional ambulance center in Skövde, Sweden (Figure 2). It is installed in a regular work environment, and used as a part of the ambulance
S.A.R.E.K Ambulance Training Environment
3
organization’s regular facilities for training and certification. This demonstrates the feasibility of the concept in practice.
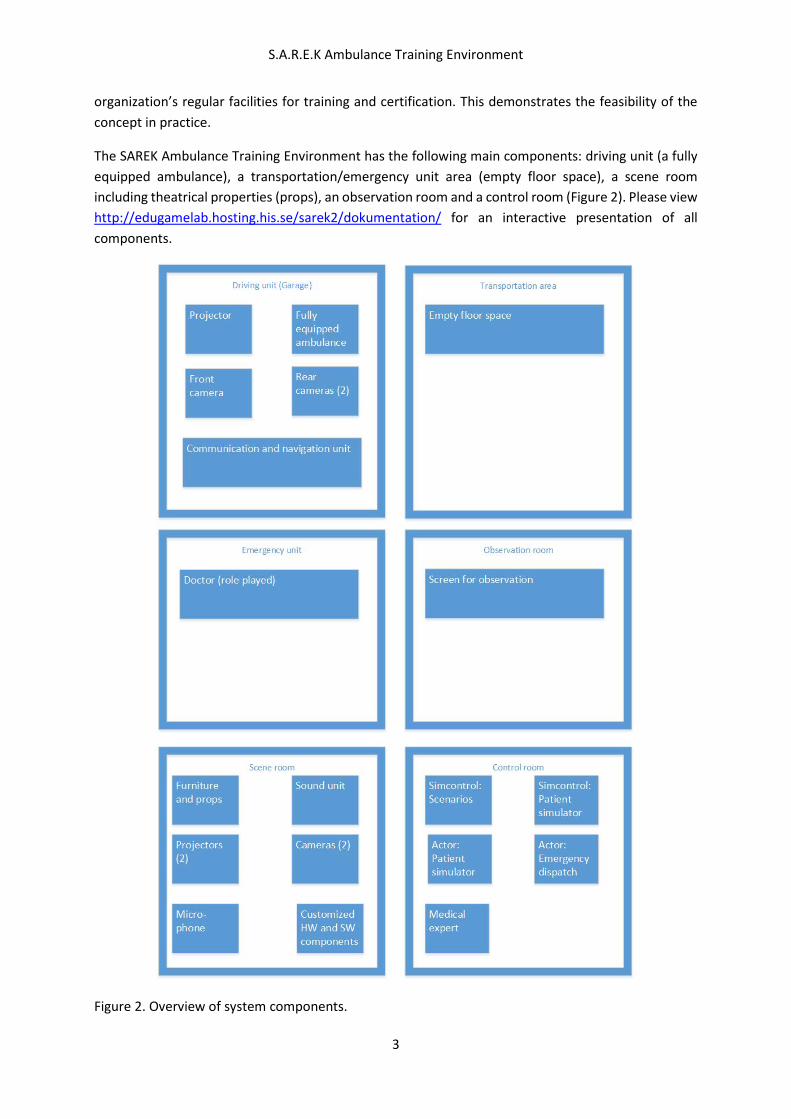
The SAREK Ambulance Training Environment has the following main components: driving unit (a fully equipped ambulance), a transportation/emergency unit area (empty floor space), a scene room including theatrical properties (props), an observation room and a control room (Figure 2). Please view http://edugamelab.hosting.his.se/sarek2/dokumentation/ for an interactive presentation of all components.
Figure 2. Overview of system components.
S.A.R.E.K Ambulance Training Environment
4
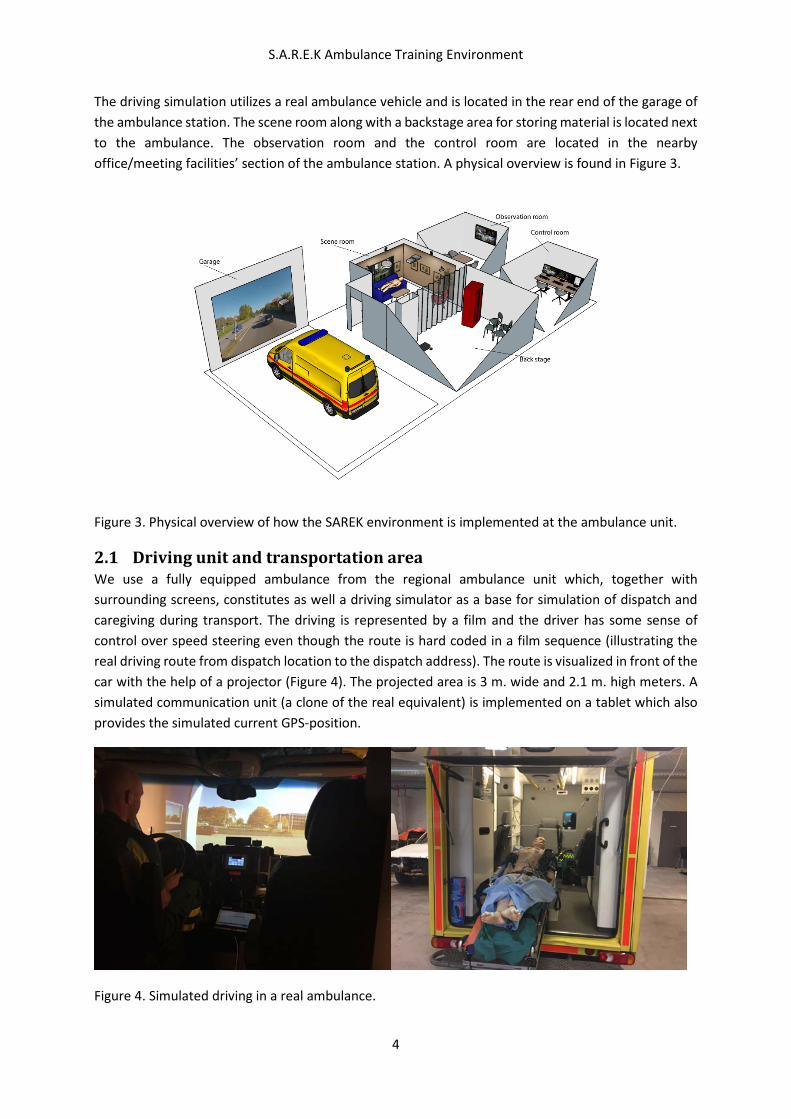
The driving simulation utilizes a real ambulance vehicle and is located in the rear end of the garage of the ambulance station. The scene room along with a backstage area for storing material is located next to the ambulance. The observation room and the control room are located in the nearby office/meeting facilities’ section of the ambulance station. A physical overview is found in Figure 3.
Figure 3. Physical overview of how the SAREK environment is implemented at the ambulance unit.
2.1 Driving unit and transportation area We use a fully equipped ambulance from the regional ambulance unit which, together with surrounding screens, constitutes as well a driving simulator as a base for simulation of dispatch and caregiving during transport. The driving is represented by a film and the driver has some sense of control over speed steering even though the route is hard coded in a film sequence (illustrating the real driving route from dispatch location to the dispatch address). The route is visualized in front of the car with the help of a projector (Figure 4). The projected area is 3 m. wide and 2.1 m. high meters. A simulated communication unit (a clone of the real equivalent) is implemented on a tablet which also provides the simulated current GPS-position.
Figure 4. Simulated driving in a real ambulance.
S.A.R.E.K Ambulance Training Environment
5
Activities inside the vehicle are monitored by three cameras: one in the front capturing the driving seat, and two in the rear capturing all events in the back of the ambulance. As the ambulance is fully equipped according to organizational standards all activities inside it can be carried out as close to normal as possible.
The transportation area and the emergency unit are mainly composed of an empty space by the ambulance. Both areas may be subject to further development to include more physical as well as virtual components.
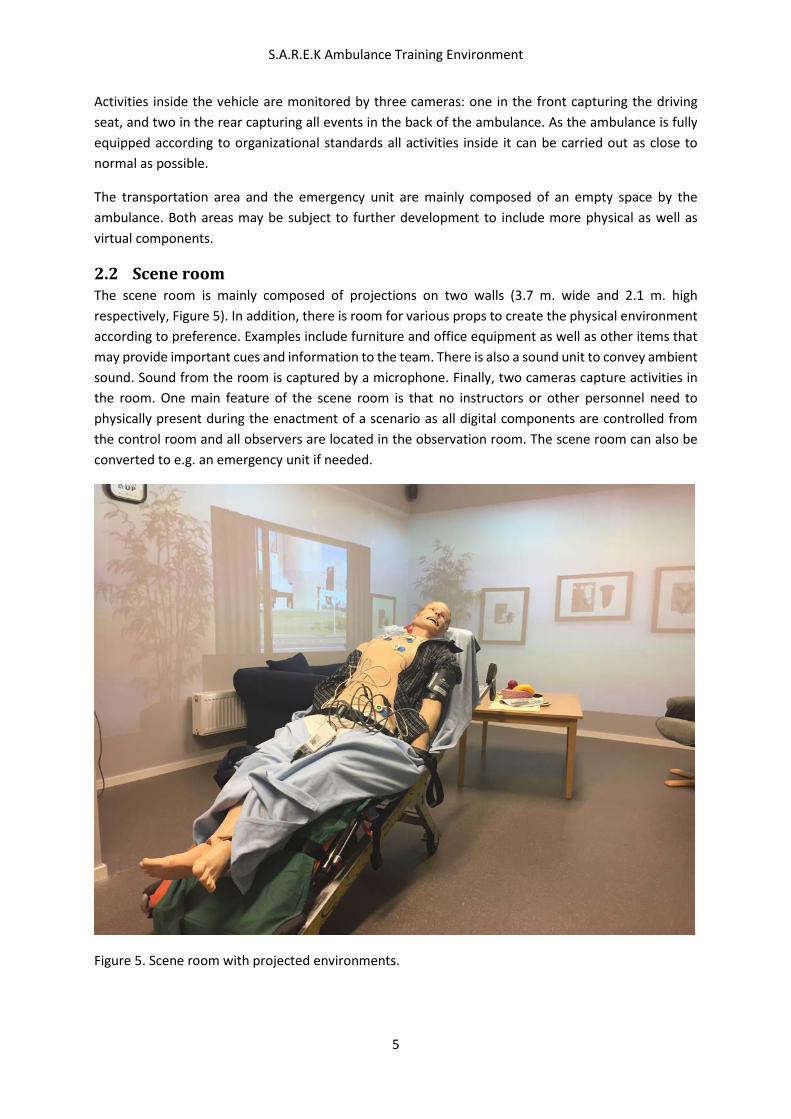
2.2 Scene room The scene room is mainly composed of projections on two walls (3.7 m. wide and 2.1 m. high respectively, Figure 5). In addition, there is room for various props to create the physical environment according to preference. Examples include furniture and office equipment as well as other items that may provide important cues and information to the team. There is also a sound unit to convey ambient sound. Sound from the room is captured by a microphone. Finally, two cameras capture activities in the room. One main feature of the scene room is that no instructors or other personnel need to physically present during the enactment of a scenario as all digital components are controlled from the control room and all observers are located in the observation room. The scene room can also be converted to e.g. an emergency unit if needed.
Figure 5. Scene room with projected environments.
S.A.R.E.K Ambulance Training Environment
6
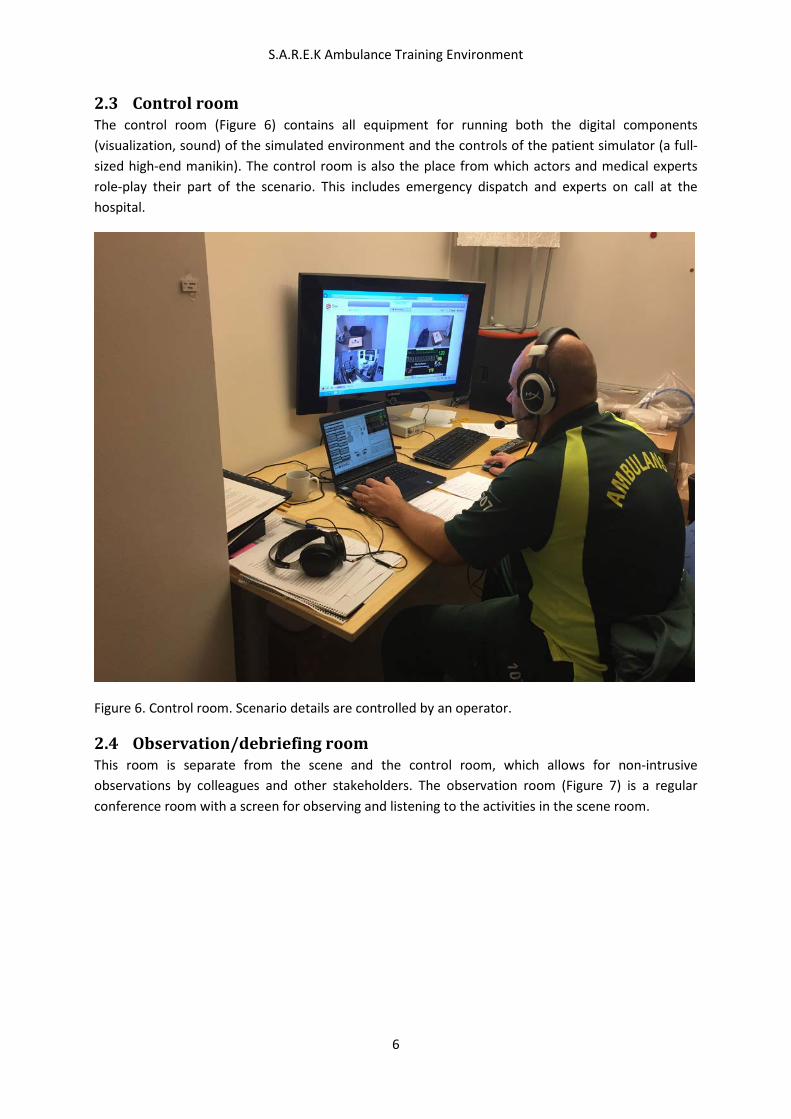
2.3 Control room The control room (Figure 6) contains all equipment for running both the digital components (visualization, sound) of the simulated environment and the controls of the patient simulator (a full-sized high-end manikin). The control room is also the place from which actors and medical experts role-play their part of the scenario. This includes emergency dispatch and experts on call at the hospital.
Figure 6. Control room. Scenario details are controlled by an operator.
2.4 Observation/debriefing room This room is separate from the scene and the control room, which allows for non-intrusive observations by colleagues and other stakeholders. The observation room (Figure 7) is a regular conference room with a screen for observing and listening to the activities in the scene room.

S.A.R.E.K Ambulance Training Environment
7
Figure 7. Debriefing room with possibility to monitor and replay scenarios.
3 Representation of Information On the information level we describe how we represent the information content in all channels that we use (Figure 8). The aim is to convey as much as possible of the information through realistic channels. Normally, there should be no interventions from instructors or others outside in what is role-played in the scenario. Here it is worth pointing out that the ambulance team is alone throughout the scenario, and the intention is that they get all the information they need via the environment and the interactions with the patient simulator and role-play actors. In should be notated that it is a challenge to reduce the amount of instructions outside the scenario.
S.A.R.E.K Ambulance Training Environment
8
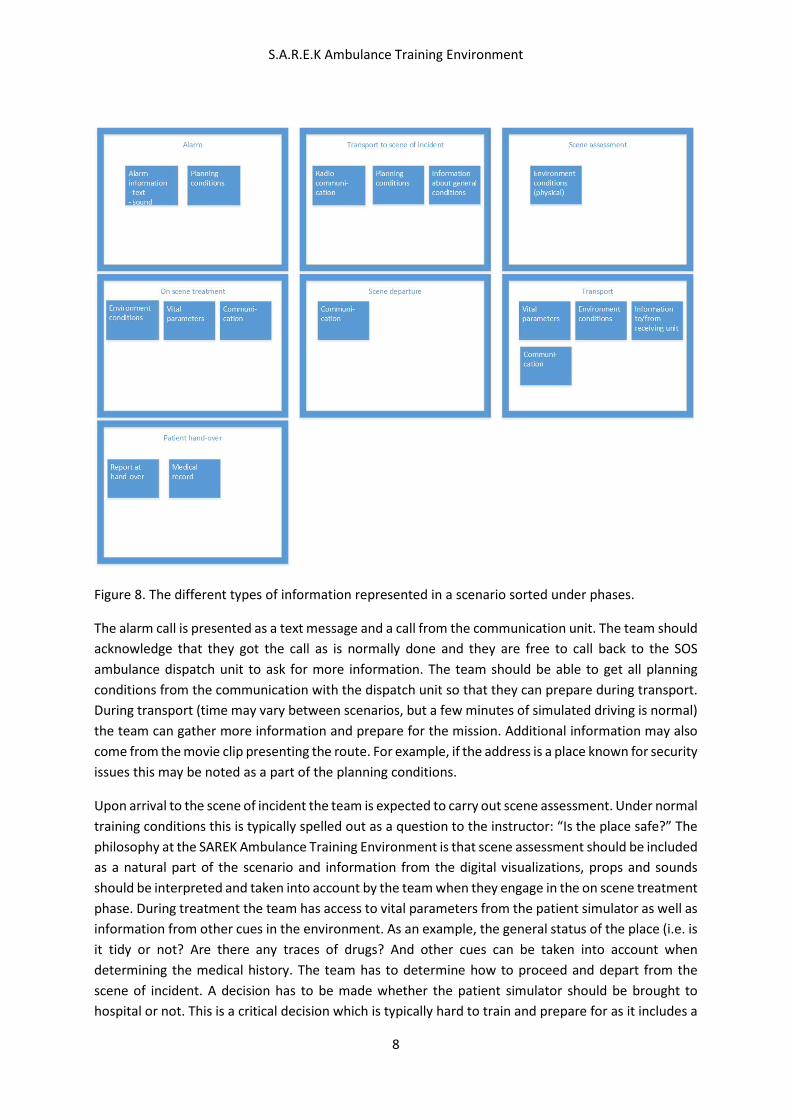
Figure 8. The different types of information represented in a scenario sorted under phases.
The alarm call is presented as a text message and a call from the communication unit. The team should acknowledge that they got the call as is normally done and they are free to call back to the SOS ambulance dispatch unit to ask for more information. The team should be able to get all planning conditions from the communication with the dispatch unit so that they can prepare during transport. During transport (time may vary between scenarios, but a few minutes of simulated driving is normal) the team can gather more information and prepare for the mission. Additional information may also come from the movie clip presenting the route. For example, if the address is a place known for security issues this may be noted as a part of the planning conditions.
Upon arrival to the scene of incident the team is expected to carry out scene assessment. Under normal training conditions this is typically spelled out as a question to the instructor: “Is the place safe?” The philosophy at the SAREK Ambulance Training Environment is that scene assessment should be included as a natural part of the scenario and information from the digital visualizations, props and sounds should be interpreted and taken into account by the team when they engage in the on scene treatment phase. During treatment the team has access to vital parameters from the patient simulator as well as information from other cues in the environment. As an example, the general status of the place (i.e. is it tidy or not? Are there any traces of drugs? And other cues can be taken into account when determining the medical history. The team has to determine how to proceed and depart from the scene of incident. A decision has to be made whether the patient simulator should be brought to hospital or not. This is a critical decision which is typically hard to train and prepare for as it includes a

S.A.R.E.K Ambulance Training Environment
9
general judgement of the situation. If the decision is to bring the patient to the hospital the patient simulator is placed on a stretcher and loaded to the ambulance. The state of the patient determines which hospital will be the destination. Vital parameters are monitored via the simulated monitor system and the ambulance nurse responsible for the medical treatment carry on activities in a normal fashion during transport. Communication is open with the hospital and medical data such as ECG can be submitted for review.
Finally, the team will make a medical report to the receiving nurse or doctor and complete the medical record.
4 Simulated Scenarios with Width and Depth With the goal to increase immersion, the project has been working both with width (involving all phases included in a typical ambulance mission) and depth (making all activities in the phases as realistic as possible). By using a number of, physical as well as procedural, system components, the ambition is also to provide a ground for so called emergent properties. The concept of emergence, in this respect, is that simple component-level behaviors often give more complex and surprising system-level behavior (Holland, 1998; Bailey and Katchabaw, 2008). According to Pfeifer (2004), emergent gameplay has the potential to create “a large amount of gameplay experiences from a much smaller set of interconnected game rules” which can lead to a better overall player experience.
4.1 Scenario width A typical ambulance mission can be divided in some well-defined phases (Jensen, Croskerry and Travers, 2011; Carter and Thompson, 2015). The project identified 6 phases which all were included in the simulation. The first phase is labeled (1) Receiving the call and last from the ambulance team receiving the call on the radio until the ambulance arrived to the address. The next phase, (2) Arriving at the scene, comprises the team arriving to the address to first patient contact. (3) On scene assessment and treatment include all activities until decision of transport. The fourth phase (4) Transport decision and departure include transport decisions, transport to the ambulance and loading the patient to the ambulance. The next phase is (5) En route assessment and treatment. This phase includes continuous assessment and treatment, documentation and notification to hospital and lasts until arrival at hospital. The last phase (6) Handover includes unloading the patient and verbal report to the receiving doctor. It is concluded by patient record writing in a digital patient record system. Carter and Thompson (2015) also include Reflection as an important aspect of the prehospital process. This phase is also included in our tests and experiments since the ambulance team was sitting down with either a doctor or a researcher to discuss their performance from different aspects. The only part of the prehospital process which is excluded from the simulation is to prepare the ambulance for the next mission. This work is done by the simulation instructors.
4.2 Scenario depth To achieve depth to the simulation, this project was using several aspects such as the use of ordinary equipment’s, the use of technology for sound and environmental simulation and an effort to reduce disturbing interaction with people not involved in the scenarios, for examples instructors and simulation technician’s. In the following, our description of activities to increase the depth is organized according to the activities described in Figure 1. The phases are derived from Jensen, et al. (2011) and Carter and Thompson (2015).

S.A.R.E.K Ambulance Training Environment
10
4.2.1 Alarm: Receiving the call and transport to the scene of incident This phase starts with a call on radio. The person making the call role-plays an ordinary call from the dispatch center. The team receives the call on the same radio device they use in ordinary work. When the team receives the call they walk to the ambulance. The ambulance is an ordinary fully equipped ambulance connected to a visualization of the route to the scene of accident. The ambulance operator space is equipped with a replica of a computer in which the ambulance team can receive more information about the mission, leave status rapports and receive directions via GPS. When the scenario starts the team sees a picture of the garage door in front of the ambulance, and when pushing the start button on the status panel, a movie playing the simulated route starts. During this phase the ambulance team can gather information of actual weather, time of the day and traffic situation. The 5 minutes of simulated driving also gives the team the possibility to gather more information by calling the dispatch central and plan the mission if they choose to do so. When the ambulance arrive at the address the movie stops and the next phase in the simulation starts.
4.2.2 On scene assessment When the team arrives at the address they have a short transfer to the actual scene of incident where the actual environment is represented by projections on two walls and some basic physical props. Upon entering the scene room, the team has to make an initial assessment of the environment (Figure 5) and use whatever cues there are to determine whether the place is safe or not before they initiate treatment.
The environment is flexible for change so the team can enact different scenarios. For example in one apartment where a drug addict lives, there are cues to raise awareness of risks specific to such an environment. Other examples are office environments and an industrial building.
The environment could be changed both through projections of film and pictures; by adding sounds such as dog barking and traffic noise; and by adding physical props specific to the environment. Setting a new environment up is a matter of a few minutes only. The goal with the more detailed environmental is to give the ambulance team opportunity to assess the scene and gather non-patient information.
4.2.3 On scene treatment The patient is an advanced simulation manikin which can simulate many physiological aspects considered important in patient assessment such as lung, heart and bowel sounds, cyanosis, chest rise and vital parameters. The manikin operator control the scenario via a computer network and all activities are captured by video and audio recording. Manikin speech is handled via radio connection by the manikin operator from the operator room. The operator has a scenario manuscript to follow but must also be flexible to changes in the scenario dependent of actions of the ambulance team. The operator is an experienced ambulance nurse with deep knowledge of the prehospital settings and patients. No instructors or operators are located at the scene during the enactment of the scenario. The ambulance team is alone with the patient apart from any extras playing additional roles. If any instructions, which cannot be represented by the patient simulator, have to be given to the team, such as a physical response to neurological examination, the results are spoken out as a “voice of God”. The “God’s voice” is distinguished by the operator speaking with a neutral voice, while delivering the response to a request: e.g. “the patient lifts both arms”.
S.A.R.E.K Ambulance Training Environment
11
The drugs in the medical bag are tagged with correct names. If the nurse, for example, wants to administrate 5 mg Morphine, he/she has to mark the syringe with the Morphine tag and fill the syringe with water and administrate the right dose. All doses are registered in the system with the use of RFID tags.
4.2.4 Scene departure and transport In this phase the ambulance teams have to decide about transport. They have their ordinary equipment to use such as the ambulance stretcher. Dependent on which simulation room used in the scenario, the distance from patient to ambulance can differ. The team has to plan the transportation and take in consideration the patient’s need of monitoring, how to transport all equipment and how to use resources on scene such as relatives. The ambulance is fully equipped and the team can choose to either work in the ambulance before departure or to start transportation at once with only one team member working with the patient during transport.
The team is informed about the transportation time to hospital. When the team has decided to initiate transport, the driver initiates the simulated drive back to the hospital. The ambulance nurse taking care of the patient continues with patient assessment and treatment with ordinary monitoring equipment and drugs.
The nurse is also able to contact the receiving hospital during transport using either phone or radio. When the team calls the hospital the instructor plays the role of the switchboard operator and they have to ask for a specific function to speak with such as stroke coordinator or ED doctor. During experiments an emergency physician plays the role of all functions at the receiving hospital.
4.2.5 Patient handover The handover phase started with unloaded the patient. In some cases the team took the patient to a simulated emergency room, other cases the physician was meeting the team in the garage. Here they were leaving a verbal report to the physician in charge. After the verbal report the team went to a PC and finished the electronic patient record.
4.2.6 Reflection The enactment of a simulation scenario is typically finished with a reflection session where the ambulance team can discuss the whole scenario with the instructor, the team observing the mission in the observation room or ambulance organizations physician. The reflection phase typically lasts for 15-20 minutes.
5 References Bailey, C. and Katchabaw, M. (2008). An emergent framework for realistic psychosocial behaviour in non player characters. FuturePlay 2008, Toronto, Ontario, Canada.
Carter H. and Thompson, J. (2015) Defining the paramedic process. Australian Journal of Primary Health. Vol. 21(1), pp. 22-6.
Holland, J. H. (1998). Emergence: From chaos to order. Addison-Wesley.

S.A.R.E.K Ambulance Training Environment
12
Jensen, J.L., Croskerry P. and Travers A.H. (2011) Consensus on paramedic clinical decisions during high-acuity emergency calls: results of a Canadian Delphi study. CJEM : Journal of the Canadian Association of Emergency Physicians. Vol. 13(5), pp. 310-8.
Pfeifer, B. (2004). Creating emergent gameplay with autonomous agents. Proceedings of the Game AI Workshop at AAAI-04.
Söderström, E., van Laere, J., Backlund, P. and Maurin Söderholm, H. (2014) Combining Work Process Models to Identify Training Needs in the Prehospital Care Process. In the Proceedings of the 13th International Conference Perspectives in Business Informatics Research, BIR 2014, pp. 375-389. Lund, Sweden, September 22–24, 2014. Lecture Notes in Business Information Processing 194, B. Johansson, B. Andersson, and N. Holmberg (Eds.), ISBN: 978-3-319-11369-2