
Hip and Knee Replacements - GTA Rehab Network · Guiding Principles ... Hospital or Private/Public...
32
Hip and Knee Replacements Standardized Rehabilitation Treatment Approaches across the Continuum of Care February 2014
Transcript of Hip and Knee Replacements - GTA Rehab Network · Guiding Principles ... Hospital or Private/Public...

Hip and Knee Replacements
Standardized Rehabilitation
Treatment Approaches
across the Continuum of Care
February 2014

2

3
Table of Contents
Acknowledgements ................................................................................................................. 4
Abbreviations and Definitions ................................................................................................... 5
Background & Introduction ....................................................................................................... 6
Guiding Principles ................................................................................................................... 7
Hip and Knee Replacement: Rehabilitation Pathway .................................................................. 8
Hip/Knee Joint Replacement Standard Rehabilitation Approaches .............................................. 9
Conservative Management Phase ................................................................................... 9
Pre-habilitation Phase .................................................................................................. 11
Inpatient Surgery Phase ............................................................................................... 14
Inpatient Rehabilitation Phase ....................................................................................... 17
Outpatient Rehabilitation – Hospital or Private/Public Physiotherapy Clinics ...................... 20
Community In–Home Rehabilitation Phase .................................................................... 23
Appendix A: Clinical Outcome Measures ................................................................................. 26
Appendix B: Champlain LHIN Orthopedic Physiotherapy Discharge Communication Report ........ 30

4
Acknowledgements
This document is the result of extensive
consultation and collaboration with individuals
from the Champlain LHIN region who work in
organizations across the continuum of care and
have joint replacement knowledge and experience.
These organizations include:
Carleton Place & District Memorial Hospital
Champlain Community Care Access Centre
Champlain Orthopedic Program Planning
Initiative
Cornwall Community Hospital
Kemptville District Hospital
Montfort Hospital
Ontario Physiotherapy Association
Pembroke Regional Hospital
Queensway-Carleton Hospital
Rehabilitation Network of Champlain
The Arthritis Society
The Cochrane Collaboration
The Ottawa Hospital

5
Abbreviations and Definitions
List of Abbreviations:
ADL: Activities of Daily Living
BBS (BERG): Berg Balance Scale
CCAC: Community Care Access Centre
COPPI: Champlain Orthopedic Program Planning
Initiative
CPM: Continuous Passive Motion
IM: Functional Independence Measure
IADL: Instrumental Activities of Daily Living
LEFS: Lower Extremity Functional Status
LHIN: Local Health Integration Network
LOS: Length of stay
M-HAQ: Modified Health Assessment
Questionnaire
MMSE : Mini Mental State Examination
MOCA : Montreal Cognitive Assessment
NRS: Numerical Rating Scale
OQS: Orthopaedic Quality Scorecard
RM&R: Resource Matching and Referral
RNOC: Rehabilitation Network of Champlain
ROM: Range of Motion
THR: Total Hip Replacement
TINETTI: Tinetti Balance Assessment Tool
TJAC: Total Joint Assessment Clinic
TKR: Total Knee Replacement
TUG: Timed Up and Go
VAS: Visual Analog Scale
WOMAC: Western Ontario and McMaster
Universities Osteoarthritis Index
Definitions:
Wait 1a: time from referral from primary care
provider to assessment at a Total Joint Assessment
Clinic
Wait 1b: time from assessment at a joint
assessment clinic to surgeon consultation
Wait 2: time from decision to treat (surgery) to
surgery date
Conservative Management is the episode of care
appropriate for patients with confirmed or suspected
hip or knee arthritis whose symptoms may be
managed non-surgically. This phase involves
individual and/or group evaluation and treatment.
Cryotherapy (or cold therapy) involves the
application of very low temperatures to the skin
surrounding an injury or surgical site. This can be
by means of bags of ice or specialized devices that
deliver cooled water to the area1.
Pre-habilitation is a program provided to assess
the client’s baseline functional capabilities and
safety, to provide patient education and self-
management, to maximize the client’s potential
recovering from surgery, and to optimize the
discharge process.
1 The Cochrane Collaboration. 2012. Cryotherapy following
total knee replacement (Review).

6
Background & Introduction
The Champlain LHIN recognizes that the
development of a regional approach to service
delivery can make a significant contribution to
certain patient populations and as such, has focused
on sectors of the system that have the potential to
make the biggest impact.
Orthopedic care is a high volume, high cost service
that crosses multiple sectors - thereby providing
significant opportunities for system improvement.
More than 4000 hip and knee replacements are
completed annually in the Champlain LHIN at six
different acute care sites.
The rehabilitation associated with these procedures
is provided in a variety of settings and locations
throughout the LHIN. Patients who are candidates
for a hip or knee replacement typically are referred
by their primary care provider to the Regional Hip
and Knee Program via the Central Intake Clinic.
Referrals are triaged by Central Intake staff and
assigned to the appropriate Total Joint Assessment
Clinic, based on geography or patient choice. The
patient is assessed by a physiotherapist or advanced
practice nurse to determine surgical candidacy.
Education and information is provided during the
assessment.
Conservative management options are provided. If
surgery is the treatment of choice, the patient is
referred to a surgeon according to patient
preference, geographical area or wait time.
Conservative management patients are referred to
The Arthritis Society and surgical patients are
booked for a consultation with a surgeon.
Once the decision for surgery has been made by the
surgeon and patient, the patient is booked for the
pre-habilitation phase of rehabilitation during which
the patient and family receive education, an
exercise regimen, and support to prepare for
surgery.
Once surgery has been performed the patient
recovers for 2-4 days from the acute stage on a
surgical inpatient unit where post-operative
rehabilitation is provided.
On discharge from the surgical unit, the patient
proceeds to rehabilitation either in an inpatient
rehabilitation unit, in a hospital-based outpatient
clinic, in a community based outpatient clinic or is
discharged home with rehabilitation treatment
provided by CCAC.
Standardized rehabilitation treatment approaches
for hip/knee replacement patients have been
developed for the following rehabilitation phases:
conservative management, pre-habilitation, acute
care post-operative rehabilitation, inpatient
rehabilitation, outpatient rehabilitation and
community rehabilitation.
The guidelines in this document are a result of
regional collaboration that were first developed in
2005, updated in 2008 and again in 2014 under the
direction of the Champlain Regional Orthopedic
Program and the Rehabilitation Network of
Champlain.
These standardized guidelines are intended as a tool
for practitioners to ensure rehabilitation for hip &
knee replacement patients is high quality, accessible
and efficient.

7
Guiding Principles
The rehabilitation standard approaches/guidelines
for each phase of care will:
Be patient centered
Be based on current Champlain LHIN
Rehabilitation for Hip/Knee Replacement
Framework
Be broad enough to address 80% of patients
Identify and address the rehabilitation needs of
the remaining 20%
Incorporate the following goals: access,
quality, and efficiency
Be evidenced based where there is available
evidence or based on the advice/consensus of
expert panels/practitioners

8
Hip and Knee Replacement: Rehabilitation Pathway
9
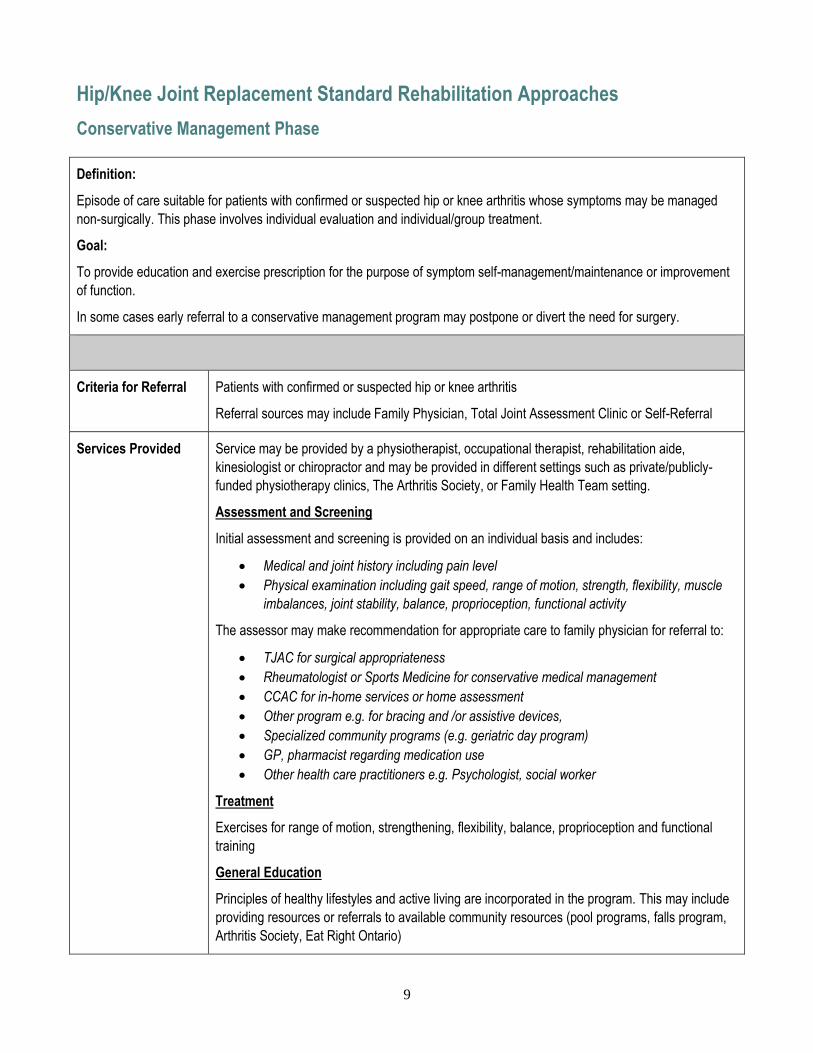
Hip/Knee Joint Replacement Standard Rehabilitation Approaches
Conservative Management Phase
Definition:
Episode of care suitable for patients with confirmed or suspected hip or knee arthritis whose symptoms may be managed
non-surgically. This phase involves individual evaluation and individual/group treatment.
Goal:
To provide education and exercise prescription for the purpose of symptom self-management/maintenance or improvement
of function.
In some cases early referral to a conservative management program may postpone or divert the need for surgery.
Criteria for Referral Patients with confirmed or suspected hip or knee arthritis
Referral sources may include Family Physician, Total Joint Assessment Clinic or Self-Referral
Services Provided Service may be provided by a physiotherapist, occupational therapist, rehabilitation aide,
kinesiologist or chiropractor and may be provided in different settings such as private/publicly-
funded physiotherapy clinics, The Arthritis Society, or Family Health Team setting.
Assessment and Screening
Initial assessment and screening is provided on an individual basis and includes:
Medical and joint history including pain level
Physical examination including gait speed, range of motion, strength, flexibility, muscle
imbalances, joint stability, balance, proprioception, functional activity
The assessor may make recommendation for appropriate care to family physician for referral to:
TJAC for surgical appropriateness
Rheumatologist or Sports Medicine for conservative medical management
CCAC for in-home services or home assessment
Other program e.g. for bracing and /or assistive devices,
Specialized community programs (e.g. geriatric day program)
GP, pharmacist regarding medication use
Other health care practitioners e.g. Psychologist, social worker
Treatment
Exercises for range of motion, strengthening, flexibility, balance, proprioception and functional
training
General Education
Principles of healthy lifestyles and active living are incorporated in the program. This may include
providing resources or referrals to available community resources (pool programs, falls program,
Arthritis Society, Eat Right Ontario)

10
Education on the following topics should be provided:
Low impact fitness alternatives (swimming, cycling)
Pacing strategies
Gait aids, bracing, assistive devices, proper footwear
Use of heat/ice
Importance of weight control
Hurt vs. harm
Typical Duration Duration and frequency: variable and is patient-specific
Discharge Criteria Patient demonstrates knowledge and tolerance of prescribed exercises
Patient has been provided with self-management strategies
Appropriate referrals to other disciplines/programs have been completed
Performance
Indicators: Clinical
and Non-Clinical
Outcome Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures (pre and post):
WOMAC
LEFS * (recommended)
VAS or NRS *(recommended)
M-HAQ
Patient Satisfaction
Clinical Objective Outcome Measures (pre and post):
Gait Speed (3 vs. 4 meter test)
range of motion
strength
flexibility
balance (BBS or TINETTI)
functional activity (TUG, Stairs)
cognition (MOCA, MMSE)
Non-clinical Indicators (Access)
access to publicly funded conservative management program (Target: 2 - 4wks)
Non-clinical Indicators (Efficiency)
number of visits per episode of care (Target: 2-8 visits)* short term focused on teaching
self-management
*Recommendation – no standard available in literature

11
Pre-habilitation Phase
Definition:
Pre-habilitation phase is defined as the period between the decision for surgery and the date of surgery.
Goal:
To assess the client’s baseline functional capabilities and safety, to provide patient education and self-management, to
maximize the client’s potential recovering from surgery, and to optimize the discharge process
Pre-habilitation includes the following elements:
An assessment/screening of the home environment for equipment and safety needs;
Education and the demonstration of exercises.
Screening for core issues which may delay recovery or timely hospital discharge
Expectation/goal setting for the pre-habilitation phase
Criteria for Referral All patients booked for hip/knee (primary or revision) are automatically referred for pre-habilitation
The referral is made as soon as consent for surgery is signed
Services Provided The pre-habilitation program is provided by a physiotherapist and/or an occupational therapist.
Additional disciplines are added as required and available eg. pharmacist, dietitian, nurse.
Assessment and Screening
Complete the hospital specific pre-habilitation tool to establish the bench-mark for client progress
and achievement of functional outcomes.
Screen to identify:
1. barriers to discharge home
2. potential post-op or discharge issues
General Education
Education on the following topics is provided:
the surgical procedure and hospital stay
precautions and joint protection post-operatively, energy conservation and pain
management techniques
assistive devices and home equipment required for the post-operative period; resources
and supply options available
demonstration of standardized exercises specific to THR and TKR with a home program
of exercises to be continued either at a gym facility or at home.

12
A client/patient information package is provided to standardize and consolidate information, to
facilitate communication for the client and health care providers, and to foster a sense of client
participation in outcomes achieved.
Goal setting and expectations are reviewed and documented.
Typical Duration Pre-habilitation takes place after decision for surgery is made and is provided in two components
one of which is in a group education format and the second component is individual based.
Component 1: 1 – 2 hour group session by a multidisciplinary team (up to 30 clients)
Component 2: 1:1 with Physiotherapist or Occupational Therapist or Social Worker
Key Activities Key Components: Total Hip or Knee Replacement
Key Activities:
General education about joint replacement surgery
Patient role and responsibility explained
Hospital specific THR or TKR clinical pathway explanation
Specific equipment requirements reviewed
Individual patient assessment completed
Instruction of exercise program for appropriate joint replacement
Pain management techniques, importance of joint protection reviewed
Lower Extremity Function Scale tool filled in by patient
List of contacts at hospital, hospital specific processes
Home care, convalescent and short term inpatient rehabilitation needs identified
Discussion & education re: equipment requirements and importance of procuring the
equipment emphasized
Home environment questionnaire completed
Review joint protection precautions
ADL assessment
MMSE as required
Outcomes:
Patient understands the type of surgery and pathways for their specific joint replacement
Patient understands their role and responsibility in the process and as part of the team.
Patient understands pain management and joint protection
Patient receives instruction in joint replacement specific exercises and understand the
need to practice these exercises before surgery
Potential post-operative rehabilitation needs identified and providers alerted
Equipment, home management, home environment plans are discussed and patient’s
individual plan for care is initiated and discussed as needed
Cognitive status evaluated as indicated

13
Discharge Criteria Patient attended program
Performance
Indicators: Clinical
and Non-Clinical
Outcome Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures:
WOMAC
LEFS * (recommended)
VAS or NRS *(recommended)
Patient Satisfaction
Clinical Objective Outcome Measures :
range of motion* (recommended)
strength* (recommended)
functional activity (TUG, Stairs)
cognition (MOCA, MMSE)
Non-Clinical Indicators (Access)
% of patients first joint specific surgery participation in pre-habilitation (Access) Target: 95%*
Non-Clinical Performance Indicators (Efficiency)
None
*Recommendation – no standard available in literature

14
Inpatient Surgery Phase
Definition:
Episode of rehabilitative care associated with the immediate post-operative period ranging from day of surgery until
discharge from acute surgical care.
Goal:
To optimize patient’s capacity which will allow the patient to be discharged to the most appropriate care setting by:
assisting patient to mobilize post operatively
reinforcing post-operative exercise regimen
preparing patient for discharge by assessing knowledge and confirming that safety needs are addressed,
ensuring that a longer term rehabilitation plan is in place post hospital discharge
Criteria for Referral All patients undergoing hip or knee replacement (partial or total/primary or revision) will receive
post-operative rehabilitation. Each patient will have identifiable rehabilitative goals according to the
clinical pathway.
Services Provided Assessment and Screening:
standard physiotherapy assessment for post-operative care
focused assessment to determine breadth of deficits and intensity of rehabilitation required
assessment of function and ADL management with appropriate intervention as required
assess for barriers to discharge (review Pre-habilitation Assessment)
confirm equipment for discharge is in place/ready
Treatment:
Activity:
By post-operative day 1:
Patient is up in chair, is up to ambulate with assistance and mobility aid
ROM exercises and strengthening exercises have begun (For Knee Replacements, CPM is
at the discretion of Physiotherapy for exceptional cases only)2
Cryotherapy is used at the discretion of the physiotherapist3
By discharge day (Day 0, 1, 2 or 3 dependent on type of surgery):
Patient is safely mobilizing and transferring with aids as required (no specific walking
distance)
Patient is safe to ambulate on stairs if required at home
2 Mac JC, Fransen M, Jennings M, March L, Mittal R, Harris IA. Evidence-based review for patients undergoing elective hip and knee
replacement. ANZ J Surg. 2013 Mar 15. doi: 10.111/ans.12109. (Epub ahead of print); Waddell, JP, Frank C, Editors. Hip and knee
replacement surgery toolkit. Bone and Joint Canada; 2009 April 30 (coted 2013). Available from:
http://www.gov.pe.ca/photos/original/BJ_toolkit.pdf
3 Adie S, Kwan A, Naylor JM, Harris IA, Mittal R. (2012) Cryotherapy following total knee replacement (Review). The Cochrane
Collaboration. The Cochrane Library 2012, Issue

15
Exercise and General Education:
review post-operative exercises, progression of exercise program and related education
review home safety precautions
Hip Replacement – hip precaution education reviewed
Discharge Planning
An Orthopedic Physiotherapy Discharge Communication Report (Appendix B) is completed and
forwarded to service provider if patient is discharged to a provider other than the hospital where the
surgery was performed (e.g. CCAC, Private Clinic)
Ensure “key contacts” for post discharge are provided
Typical Duration Initiation: Therapy provided by rehabilitation professional is initiated post-operative Day 1.
Rehabilitation activities are supplemented by other members of the team (e.g. Nursing).
Duration: Target LOS is 2 – 3 days if patient is expected to move to inpatient rehabilitation unit and
1-3 days if patient is expected to return home
Frequency: Frequency of therapy post-operatively varies, but at a minimum, staffing levels should
be sufficient to support provision of therapy at least once per day
Discharge Criteria Criteria for discharge home:
Patient ambulates and transfers safely with mobility devices
Patient able to do stairs if needed
Home exercise/education program has been provided to patient and/or caregiver
Rehabilitation plan in place (Outpatient, CCAC)
If criteria for discharge not met, consider alternate levels of care e.g. Convalescent care,
Inpatient Rehabilitation Unit.
Performance
Indicators: Clinical
and Non-Clinical
Outcome Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures:
VAS or NRS *(recommended)
Satisfaction Survey *(recommended)
Clinical Objective Outcome Measures :
range of motion* (recommended)
strength * (recommended)
functional activity (TUG, Stairs) * (Stairs assessment is recommended if needed)
Non-Clinical Indicators (Quality)
Readmission Rates (within 30 days) Target: <3.1 % (provincial average - no target)**
Non-Clinical Indicators (Efficiency)
LOS acute care Target: 3 days (Local) Source: OQS
4.4 days (Provincial)

16
% Discharged Home - Target: 90% (provincial) Source: OQS
*Recommendation – no standard available in literature
**Based on the provincial average reported on Orthopedic Quality Scorecard – changes quarterly

17
Inpatient Rehabilitation Phase
Definition:
Episode of rehabilitative care provided by a rehabilitation team on a mixed or dedicated population Rehabilitation Unit in
acute care or rehabilitation hospitals. This level of rehabilitation is suitable for patients in need of an interprofessional
rehabilitation program who also cannot be safely discharged home.
Inpatient rehabilitation should not be the first choice for the typical patient with a primary, elective total hip or knee
replacement. It is expected that no more than 10% of hip/knee replacement patients will require inpatient rehabilitation4
(OQS)
Goal:
To optimize the patient’s capacity which will allow discharge to the most appropriate care setting by:
Assisting the patient to mobilize post operatively
reinforcing post-operative exercise regimen
preparing the patient for discharge by assessing knowledge and confirming that safety needs are addressed
ensuring that a longer term rehabilitation plan is in place post discharge
Criteria for Referral Unsafe for discharge to a home environment and has the potential to improve functional status
Patients will not be excluded from admission on the basis of a mild/moderate cognitive impairment.
Services Provided Assessment and Screening
Assessment and development of an individualized therapy plan (1:1 or group setting)
Assessment of functional outcome status (Functional Independence Measure - FIM) on
admission and at discharge to document progress and guide treatment selection
Treatment
Rehab services are provided 5 days per week at a minimum.
Frequency of therapy (Occupational and/or Physiotherapy) varies but at a minimum, staffing levels
should be sufficient to support provision of therapy at least twice per day. Rehabilitation activities are
supplemented by other members of the team (e.g. Nursing).
Therapeutic interventions include:
Exercises for ROM and strength, including home exercises
Functional training (e.g. gait, stairs, balance, transfers) including any applicable precautions
Activities of Daily Living (ADL)/Instrumental Activities of Daily Living (IADL) assessment
and training
4 Orthopedic Quality Scorecard. Released quarterly by Ministry of Health and Long Term Care
18
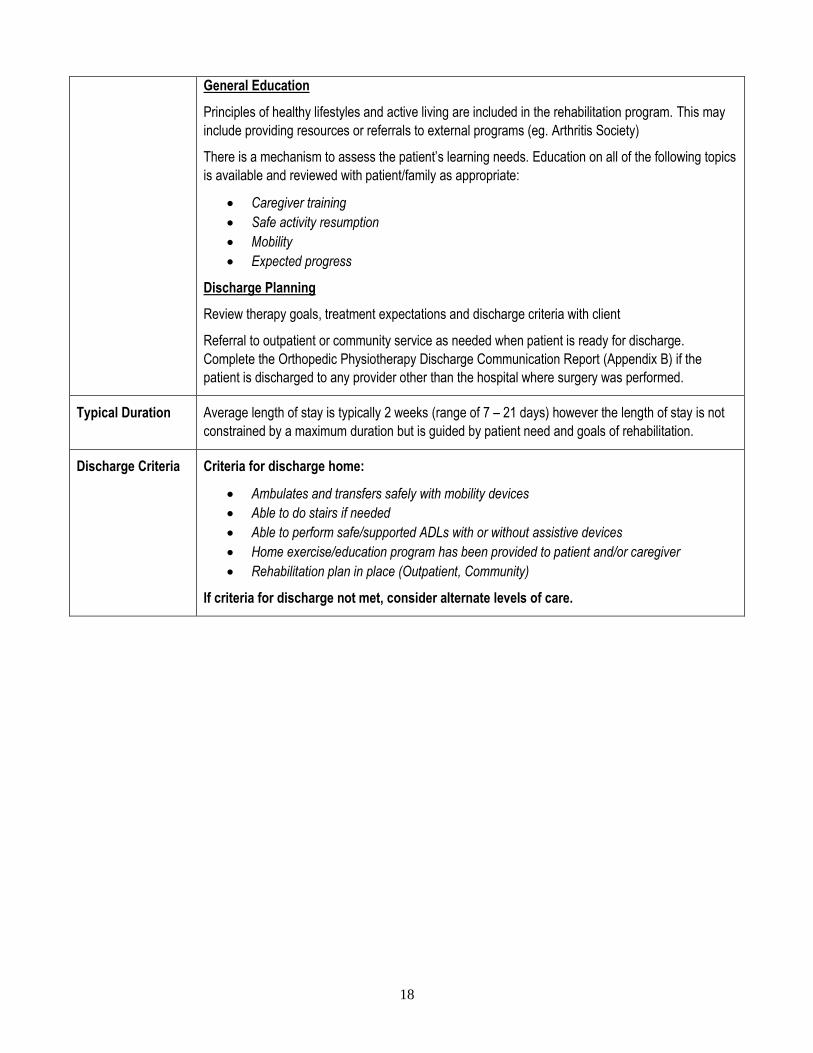
General Education
Principles of healthy lifestyles and active living are included in the rehabilitation program. This may
include providing resources or referrals to external programs (eg. Arthritis Society)
There is a mechanism to assess the patient’s learning needs. Education on all of the following topics
is available and reviewed with patient/family as appropriate:
Caregiver training
Safe activity resumption
Mobility
Expected progress
Discharge Planning
Review therapy goals, treatment expectations and discharge criteria with client
Referral to outpatient or community service as needed when patient is ready for discharge.
Complete the Orthopedic Physiotherapy Discharge Communication Report (Appendix B) if the
patient is discharged to any provider other than the hospital where surgery was performed.
Typical Duration Average length of stay is typically 2 weeks (range of 7 – 21 days) however the length of stay is not
constrained by a maximum duration but is guided by patient need and goals of rehabilitation.
Discharge Criteria Criteria for discharge home:
Ambulates and transfers safely with mobility devices
Able to do stairs if needed
Able to perform safe/supported ADLs with or without assistive devices
Home exercise/education program has been provided to patient and/or caregiver
Rehabilitation plan in place (Outpatient, Community)
If criteria for discharge not met, consider alternate levels of care.

19
Performance
Indicators: Clinical
and Non-Clinical
Outcome
Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures:
VAS or NRS *(recommended)
WOMAC
Satisfaction Survey
Clinical Objective Outcome Measures:
range of motion *(recommended)
strength *(recommended)
balance (BERG or TINETTI)
functional activity (Gait Speed)
functional activity (TUG, Stairs) *(recommended)
functional activity (FIM) (mandatory)
cognition (MOCA, MMSE)
Non-Clinical Indicators (Access)
% admitted from acute care Target: 10% or less**
Wait time for admission from acute care Target: 1 – 2 days ***
(Administrative) Performance Indicators (Efficiency)
Average Length of Stay Target: 14 days***
*Recommendation – no standard available in literature
**Orthopedic Quality Scorecard
***Local Target set by consensus Ortho-Rehab Working Group

20
Outpatient Rehabilitation – Hospital or Private/Public Physiotherapy Clinics
Definition:
Episode of care suitable for individuals who are in need of an outpatient rehabilitation service in a single specialty
area/profession. Services include assessment and treatment. Treatment may be provided in group or individual format.
Goal:
To optimize patient’s functional capacity in order to maximize normal function.
Criteria for Referral Patients reside in the community and have been discharged either from an acute surgery unit, an
inpatient rehabilitation unit, another outpatient rehabilitation program or from a community in-home
rehabilitation program
Referral from a physician for hospital outpatient clinic (majority of hospital outpatient clinics accept
referrals from physicians with privileges in that hospital only)
Able to get to the clinic
Able to actively participate either independently or with support (eg. family member)
Services Provided
Assessments and treatment are focused on patient safety at home as well as physical and functional
abilities necessary for daily activities
Treatment is provided by a combination of physiotherapist and rehabilitation assistant for group
sessions; group size is dependent on space & staffing but typically group size ranges between 5 and
15 clients. Knee post discharge rehabilitation is most efficiently provided in a group setting.
Assessment and Screening
initial focused assessment is 1:1 with a physiotherapist to determine breadth of deficits and
intensity of rehabilitation required
assessment of function and ADL management with appropriate intervention as required
assessment for and development of individualized therapy plans (eg. 1:1 or group settings)
Treatment
exercises for ROM and strength, including home exercises
functional training (eg. gait, stairs, balance, transfers) including home exercises
hands on therapy as required
pain management
General Education
Principles of healthy lifestyles and active living are incorporated in the rehabilitation program. This
may include providing resources or referrals to external programs
There is a mechanism in place to assess the patient’s learning needs. Education on all of the
following topics is available:
Caregiver training
Safe activity resumption
Mobility and precautions if applicable
Expected progress
Sources of help

21
Discharge Planning
Review therapy goals, treatment expectations and discharge criteria with client
Communication to Orthopedic Surgeon only as needed.
Typical Duration KNEE REPLACEMENT
Initiation: Treatment begins in a timely manner for all patients based on individual needs.
Specifically, treatment for patients referred from acute care should begin within 2 weeks*** of acute
care discharge.
Duration: The typical duration is 5-6 weeks
Frequency: Up to twice per week for a full knee replacement and once per week for a partial knee
replacement.
HIP REPLACEMENT
Initiation: Treatment begins in a timely manner for all patients based on individual needs.
Specifically, treatment for patients referred from acute care should begin at the 3 week mark for
assessment and review/progression of home exercise program.
Duration: The typical duration is 4-6 weeks after initial assessment.
Frequency: Frequency of treatment depends on achievement of goals, typically no more than once
per week.
***Local Target set by consensus Ortho-Rehab Working Group
Discharge Criteria
Functional active ROM (consider pre-op status and lifestyle)
Extension 0 degrees (hip); 0-5 degrees (knee)
Flexion minimum 90 degrees (hip); 110 degrees (knee)
Functional Strength (consider pre-op status and lifestyle)
Hip: Grade 4/5 hip flexion and extension
Grade 3/5 hip abduction
Knee: Grade 4/5 or functional control of the knee
Independent ambulation (indoors and outdoors, with/without ambulation aid as required –
consider pre-op status)
Safe transfers as required (home, vehicle)
Safe use of stairs if required
Swelling resolved or self-managed; wound healed or self-managed; pain self-managed
with/without medications
Long-term equipment needs identified; vendors, funding and safe use understood
Patients are discharged when they have achieved their discharge goals or they have reached a
plateau (showing no improvement for 2 weeks) rather than based on a maximum number of visits.
If client’s personal goals exceed the program goals above, a home exercise program or referral to a
private clinic may be arranged.

22
Performance
Indicators Clinical
and Non-Clinical
Outcome
Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures (pre and post):
WOMAC
LEFS * (recommended)
VAS or NRS *(recommended)
M-HAQ
Satisfaction Survey
Clinical Objective Outcome Measures (pre and post):
range of motion *(recommended)
strength *(recommended)
functional activity (TUG, GAIT)
functional activity (Stairs) *(recommended)
balance (TINETTI or BERG)
Non-Clinical Indicators (Access)
Wait time to access publicly funded outpatient rehabilitation program Target: 2 weeks (knees)***
3 weeks (hips)***
Non-Clinical Indicators (Efficiency)
Number of Visits per patient Target: 10-12 visits (full knee replacement)***
6 - 8 visits (partial knee replacement)***
6 – 8 visits (hip replacement)***
*Recommendation – no standard available in literature
***Local Target set by consensus Ortho-Rehab Working Group
23
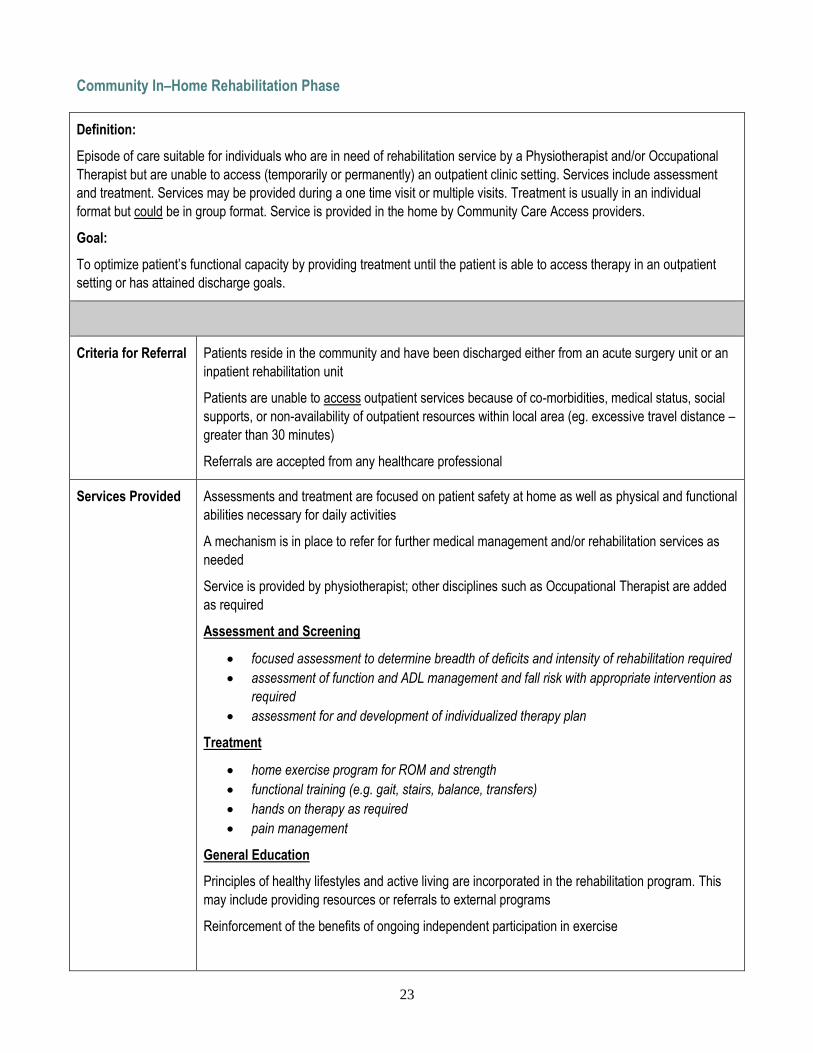
Community In–Home Rehabilitation Phase
Definition:
Episode of care suitable for individuals who are in need of rehabilitation service by a Physiotherapist and/or Occupational
Therapist but are unable to access (temporarily or permanently) an outpatient clinic setting. Services include assessment
and treatment. Services may be provided during a one time visit or multiple visits. Treatment is usually in an individual
format but could be in group format. Service is provided in the home by Community Care Access providers.
Goal:
To optimize patient’s functional capacity by providing treatment until the patient is able to access therapy in an outpatient
setting or has attained discharge goals.
Criteria for Referral Patients reside in the community and have been discharged either from an acute surgery unit or an
inpatient rehabilitation unit
Patients are unable to access outpatient services because of co-morbidities, medical status, social
supports, or non-availability of outpatient resources within local area (eg. excessive travel distance –
greater than 30 minutes)
Referrals are accepted from any healthcare professional
Services Provided Assessments and treatment are focused on patient safety at home as well as physical and functional
abilities necessary for daily activities
A mechanism is in place to refer for further medical management and/or rehabilitation services as
needed
Service is provided by physiotherapist; other disciplines such as Occupational Therapist are added
as required
Assessment and Screening
focused assessment to determine breadth of deficits and intensity of rehabilitation required
assessment of function and ADL management and fall risk with appropriate intervention as
required
assessment for and development of individualized therapy plan
Treatment
home exercise program for ROM and strength
functional training (e.g. gait, stairs, balance, transfers)
hands on therapy as required
pain management
General Education
Principles of healthy lifestyles and active living are incorporated in the rehabilitation program. This
may include providing resources or referrals to external programs
Reinforcement of the benefits of ongoing independent participation in exercise

24
There is a mechanism in place to assess the patient’s learning needs. Education on all of the
following topics is available:
Caregiver training
Safe activity resumption
Mobility and precautions if applicable
Expected progress
Discharge Planning
Communication to attending physician is established if required because of complications or lack of
progress
Referral to outpatient physiotherapy as needed when patient is ready for discharge from community
program; copy of original medical referral plus a new Orthopedic Physiotherapy Discharge
Communication Report (Appendix A) must be completed and sent to provider
Typical Duration Initiation:
Patient care as defined by delivery of direct services by PT and/or OT (NOT including CCAC Care
Coordinator assessment or equipment delivery) should be started within 1 week of discharge. High
risk patients should be identified as per normal hospital process for earlier initiation of service.
Duration:
Knee Replacement: the typical maximum duration of therapy is 8 – 12 weeks if patient is unable to
access outpatient clinic.
Hip Replacement: the typical maximum duration of therapy is 12 weeks if patient is unable to access
outpatient clinic
Frequency:
Typical number of visits is once per week for both hip and knee patients
Discharge Criteria Patients are discharged when they are able to access appropriate community resources (eg.
outpatient services) or have achieved their discharge outcome (functional goals) or they have
reached a plateau (showing no improvement in 2 weeks) in any of the following conditions (strength,
range of motion, pain or swelling) rather than based on a maximum number of visits
If the patient’s in-home community rehabilitation is temporary, the discharge criteria is:
Patient is able to get in and out of home and vehicle safely to attend outpatient clinic
If the patient’s entire post-acute rehabilitation is provided in the community in a home
environment, the discharge criteria are:
1. Functional active ROM (consider pre-op status and lifestyle)
Extension 0 degrees (hip); 0-5 degrees (knee)
Flexion minimum 90 degrees (hip); 90-110 degrees (knee)
2. Functional Strength (consider pre-op status and lifestyle)
Grade 4/5 hip flexion and extension
Grade 3/5 hip abduction OR
Grade 4/5 or functional control of the knee

25
3. Independent ambulation (indoors and outdoors, with/without ambulation aid as required –
consider pre-op status)
4. Safe transfers as required (home, vehicle)
5. Safe use of stairs if required
6. Swelling resolved or self-managed; wound healed or self-managed; pain self-managed
with/without medications
7. Long-term equipment needs identified; vendors, funding and safe use understood
If patient’s personal goals exceed the program goals above, a home exercise program or referral to
a private in-home or outpatient clinic may be arranged.
Performance
Indicators: Clinical
and Non-Clinical
Outcome
Indicators
Clinical Outcome Indicators (Quality)
Patient Self Report Outcome Measures (pre and post):
WOMAC
LEFS * (recommended)
VAS or NRS *(recommended)
M-HAQ
Satisfaction Survey
Clinical Objective Outcome Measures (pre and post):
range of motion *(recommended)
strength *(recommended)
functional activity (GAIT)
functional activity (TUG, Stairs) *(recommended)
balance (BERG or TINETTI)
cognition (MOCA, MMSE)
Non-Clinical Indicators (Access and Efficiency)
Wait time to access Community in-home physiotherapy: Target: 1 week or less***
Length of Time receiving CCAC Therapy: (days/weeks): Target: 12 weeks or less***
Readmission Rates (within 30 days) Target: <3.1 % (provincial average - no target)**
*Recommendation – no standard available in literature
***Local Target set by consensus Ortho-Rehab Working Group

26
Appendix A: Clinical Outcome Measures
Outcome Tool Acronym Description of Tool
Rehabilitation Phase appropriate for Use of Tool
√ = Appropriate for use
R = Recommended for use
TJAC Cons
Mgmt
Pre-
hab
Inpt
Acute
Inpt
Rehab
Outpt Comm
BERG BALANCE
SCALE
BBS Measures Balance and functional mobility
(Objective performance measure)
√ √ √
FUNCTIONAL
INDEPENDENCE
MEASURE
FIM Provides a uniform system of measurement for disability
based on the International Classification of Impairment,
Disabilities and Handicaps ; measures the level of a
patient’s disability and indicates how much assistance is
required for the individual to carry out activities of daily
living. Contains 18 items composed of 13 motor tasks and 5
cognitive tasks. Scores range from 18 (lowest) to 126
(highest). Scores generally rated at admission & discharge5
√
(manda
ted by
MoH)
GAIT SPEED
TESTING
GAIT Measures walking speed as an indicator of functional ability;
in conjunction with other measures can be predictive;
examples include 4 Meter Walk Test
(Objective performance measure)
√ √ √ √
Lower Extremity
Functional Scale
LEFS The LEFS is a self-report questionnaire. Patients answer the
question "Today, do you or would you have any difficulty at
all with:" in regards to twenty different activities. Patients
select an answer from the following scale for each activity
listed:
√ √/R √/R √/R √/R
5 Rehab Measures: Functional Independence Measure. http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=889

27
Outcome Tool Acronym Description of Tool
Rehabilitation Phase appropriate for Use of Tool
√ = Appropriate for use
R = Recommended for use
TJAC Cons
Mgmt
Pre-
hab
Inpt
Acute
Inpt
Rehab
Outpt Comm
0. Extreme Difficulty or Unable to Perform Activity
Quite a Bit of Difficulty
Moderate Difficulty
A Little Bit of Difficulty
No Difficulty
The patient's score is tallied at the bottom of the page. The
maximum possible score is 80 points, indicating very high
function. The minimum possible score is 0 points, indicating
very low function.6
(self-report outcome measure)
Modified Health
Assessment
Questionnaire
M-HAQ The Health Assessment Questionnaire (HAQ) is one of the
most widely used self-assessment instruments for
measuring functional disability in patients. The HAQ is a
generic questionnaire in the sense that it does not
differentiate between disability caused by arthritis and that
caused by other disease conditions.7
(self-report outcome measure)
√ √ √
MINI MENTAL
STATE
EXAMINATION
MMSE The Mini-Mental State Examination (MMSE) is a 10-minute
bedside measure of impaired thinking. The summed score
of the individual items indicates the current severity of
√ √ √ √
6 www.physio-pedia.com/Lower_Extremity_Functional_Scale 7 Krishnan, E., Sokka, T., Häkkinen, A., Hubert, H. and Hannonen, P. (2004), Normative values for the Health Assessment Questionnaire Disability Index: Benchmarking disability in the general
population. Arthritis & Rheumatism, 50: 953–960. doi: 10.1002/art.20048

28
Outcome Tool Acronym Description of Tool
Rehabilitation Phase appropriate for Use of Tool
√ = Appropriate for use
R = Recommended for use
TJAC Cons
Mgmt
Pre-
hab
Inpt
Acute
Inpt
Rehab
Outpt Comm
cognitive impairment.
Deterioration in cognition is indicated by decreasing scores
of repeated tests8
MONTREAL
COGNITIVE
ASSESSMENT
MOCA The MoCA is a brief cognitive screening tool with high
sensitivity and specificity for detecting MCI as currently
conceptualized in patients performing in the normal range
on the MMSE.9
√ √ √ √
NUMERICAL
RATING SCALE
OR
NRS The Numeric Rating Scale (NRS-11) is an 11–point scale for
patient self-reporting of pain. It is for adults and children 10
years old or older
(self-report outcome measure)
√/R √/R √/R √/R √/R √/R √/R
VISUAL ANALOG
TOOL FOR PAIN
VAS The visual analog scale (VAS) is a tool used to measure
pain10 (self-report outcome measure)
√/R √/R √/R √/R √/R √/R √/R
PATIENT
SATISFACTION
SURVEY
Specific questionnaire according to organization √ √ √ √ √ √ √
8 Principles and Practice of Geriatric Psychiatry. Editors: Professor John R. M. Copeland, Dr Mohammed T. Abou-Saleh and Professor Dan G. Blazer. Copyright & 2002 John Wiley & Sons Ltd
Print ISBN 0-471-98197-4 Online ISBN 0-470-84641-0
9 Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., Cummings, J. L. and Chertkow, H. (2005), The Montreal Cognitive Assessment, MoCA: A Brief
Screening Tool For Mild Cognitive Impairment. Journal of the American Geriatrics Society, 53: 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
10 Myles, Paul S. MBBS, MPH, MD, FFARCSI, FANZCA; Troedel, Sally MBBS; Boquest, Michael MBBS; Reeves, Mark MBBS. The Pain Visual Analog Scale: Is It Linear or Nonlinear?
Anesthesia & Analgesia:
December 1999 - Volume 89 - Issue 6 - p 1517 doi: 10.1213/00000539-199912000-00038

29
Outcome Tool Acronym Description of Tool
Rehabilitation Phase appropriate for Use of Tool
√ = Appropriate for use
R = Recommended for use
TJAC Cons
Mgmt
Pre-
hab
Inpt
Acute
Inpt
Rehab
Outpt Comm
TINETTI BALANCE
ASSESSMENT
TOOL 11
TINETTI A falls risk index for elderly patients based on number of
chronic disabilities; one section measures balance sitting
and standing and is scored out of 16; a second section
measures GAIT at usual speed and at a rapid pace and is
scored out of 12. Risk of Fall: ≤18 = high risk, 19-23 =
moderate risk, ≥24 low risk
(Objective performance measure)
√ √ √ √
TIMED UP AND GO TUG The TUG measures limited aspects of balance and
therefore, risk of falls; has been used to measure
responsiveness to change in patients who receive physical
therapy
Measurement of the time in seconds for a person to rise
from sitting from a standard arm chair, walk 3 meters , turn,
walk back to the chair, and sit down. The person uses
regular and customary walk aid.12
(Objective performance measure)
√ √ √ √ √ √
Western Ontario
and McMaster
Universities
Osteoarthritis
Index -Physical
function subscale
WOMAC Measures the individual’s perspective of his/her own level of
mobility (licensing fee)
(Self-report outcome measure)
√ √ √ √ √ √
11 Tinetti ME, Williams TF, Mayewski R, Fall Risk Index for elderly patients based on number of chronic disabilities. Am J Med 1986:80:429-434 12 Deborah M Kennedy, Paul W Stratford, Jean Wessel, Jeffrey D Gollish and Dianne Penney . Assessing stability and change of four performance measures: a longitudinal study evaluating
outcome following total hip and knee arthroplasty. BMC Musculoskeletal Disorders 2005, 6:3 doi:10.1186/1471-2474-6-3

30
Appendix B: Champlain LHIN Orthopedic Physiotherapy Discharge
Communication Report
(Insert Hospital or
CCAC logo)
ORTHOPEDIC PHYSIOTHERAPY
DISCHARGE COMMUNICATION
REPORT
Client name:
Address:
Date of birth:
Health Card #:
Instructions for use: For use when a patient is discharged from one physiotherapy provider to another
physiotherapy provider (e.g. hospital to CCAC, CCAC to outpatient clinic).
Surgical Procedure:
______________________
Date of Procedure: ___________________ Surgeon Name: ______________________________
Orthopedic Clinic Follow-Up Date: ________________________________
CURRENT STATUS
Weight Bearing Status:
Contra-Indications:
° (___ wks)
st gravity (___ wks)
Transfers and Mobility:
Transfer status (with or without aids):
Ambulation Aids:
Distance: _____________ meters
Comments / Other Functional Information:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
______________________________
Outpatient physiotherapy referral completed: NO YES Location: ________________________________
Signature: __________________________________________ Date: _______________________________
Name (print): _______________________________________ Phone #: _____________________________
Discipline: PT OT RN MD SW Pager # ______________________________
Origin of Report: Champlain Orthopedic Rehabilitation Working Group (May 26, 2014)

31

32
















![Knee Osteoarthritis: A Review of Pathogenesis and State-Of ......with knee and hip joint replacements as the majority of that cost [9,12]. Furthermore, after low-back Furthermore,](https://static.fdocuments.net/doc/165x107/6086506fb492ce60b97ff111/knee-osteoarthritis-a-review-of-pathogenesis-and-state-of-with-knee-and.jpg)

