High-resolution spectral domain optical coherence ... · optical coherence tomography.Tubercular...
7
ORIGINAL RESEARCH High-resolution spectral domain optical coherence tomography and fundus autofluorescence correlation in tubercular serpiginouslike choroiditis Reema Bansal & Pandurang Kulkarni & Amod Gupta & Vishali Gupta & Mangat R. Dogra Received: 2 July 2011 /Accepted: 31 July 2011 /Published online: 17 August 2011 # The Author(s) 2011. This article is published with open access at SpringerLink.com Abstract Objective This study aims to describe changes in high- resolution spectral domain optical coherence tomography (SD-OCT) scans with simultaneous fundus autoflorescence (FAF) signals in tubercular serpiginouslike choroiditis (SLC). Methods Simultaneous SD-OCT and FAF imaging of eyes affected with SLC from acute stage until resolution of lesions was obtained using Spectralis HRA+OCT system (Heidelberg Engineering, Heidelberg, Germany). Patients Four eyes (three patients) with SLC were prospec- tively followed. Results Acute lesions of SLC (diffusely hyperautofluores- cent) corresponded to hyperreflective areas on SD-OCT involving the retinal pigment epithelium (RPE), photore- ceptor outer segment tips (POST), inner segment–outer segment (IS/OS) junction, external limiting membrane (ELM), and outer nuclear layer (ONL) with a minimal distortion of inner retinal layers. There was no backscatter- ing from inner choroid. During healing, lesions became discrete with a hypoautofluorescent border and predomi- nant hyperautofluorescence centrally. The hyperreflective fuzzy areas on SD-OCT scans disappeared, and irregular, knobbly elevations of outer retinal layers appeared. The RPE, POST, IS/OS junction, and ELM could not be distinguished. The ONL appeared normal. The choroid showed an increased reflectance. As the lesions healed further over the next 3–6 months, they became predomi- nantly hypoautofluorescent with loss of RPE, POST, IS/OS junction, and ELM in SD-OCT scan. Conclusion The SD-OCT provided an insight into the ultrastructural changes in the outer retina during the course of acute SLC lesions. The changes on OCT correlated with abnormal FAF findings. Keywords Fundus autofluorescence . Spectral domain optical coherence tomography . Tubercular serpiginouslike choroiditis Serpiginous choroiditis is a progressive, chronic, recurrent inflammatory disease primarily affecting the inner choroid and retinal pigment epithelial (RPE) cell layer [1]. Serpiginouslike choroiditis (SLC) of presumed tubercular etiology is a distinct clinical entity that begins usually as multifocal choroiditis lesions that coalesce and progress in a serpiginoid pattern [2, 3]. While the choriocapillaries have been shown to be the most affected layer in serpiginous choroiditis (SC), the primary site of inflammation in SLC is not yet known and is at best speculated, presumably the choriocapillaries [4]. The simultaneous recordings of topographic and tomo- graphic images by using a combination of scanning laser ophthalmoscopy and optical coherence tomography (OCT) have increased our understanding of the pathogenesis of various diseases of the retina and choroid [5]. The Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Summary statement Simultaneous spectral domain optical coherence tomography and fundus autofluorescence findings correlated well during the course of acute tubercular serpiginouslike choroiditis and provided an insight into the ultrastructural changes in the outer retina as the lesions healed. R. Bansal : P. Kulkarni : V. Gupta : M. R. Dogra Advanced Eye Centre, Post Graduate Institute of Medical Education and Research, Chandigarh, India A. Gupta (*) Department of Ophthalmology, Advanced Eye Centre, Post Graduate Institute of Medical Education and Research, Chandigarh 160012, India e-mail: [email protected] J Ophthal Inflamm Infect (2011) 1:157–163 DOI 10.1007/s12348-011-0037-7
Transcript of High-resolution spectral domain optical coherence ... · optical coherence tomography.Tubercular...

ORIGINAL RESEARCH
High-resolution spectral domain optical coherencetomography and fundus autofluorescence correlationin tubercular serpiginouslike choroiditis
Reema Bansal & Pandurang Kulkarni & Amod Gupta &
Vishali Gupta & Mangat R. Dogra
Received: 2 July 2011 /Accepted: 31 July 2011 /Published online: 17 August 2011# The Author(s) 2011. This article is published with open access at SpringerLink.com
AbstractObjective This study aims to describe changes in high-resolution spectral domain optical coherence tomography(SD-OCT) scans with simultaneous fundus autoflorescence(FAF) signals in tubercular serpiginouslike choroiditis (SLC).Methods Simultaneous SD-OCT and FAF imaging of eyesaffected with SLC from acute stage until resolution oflesions was obtained using Spectralis HRA+OCT system(Heidelberg Engineering, Heidelberg, Germany).Patients Four eyes (three patients) with SLC were prospec-tively followed.Results Acute lesions of SLC (diffusely hyperautofluores-cent) corresponded to hyperreflective areas on SD-OCTinvolving the retinal pigment epithelium (RPE), photore-ceptor outer segment tips (POST), inner segment–outersegment (IS/OS) junction, external limiting membrane(ELM), and outer nuclear layer (ONL) with a minimaldistortion of inner retinal layers. There was no backscatter-ing from inner choroid. During healing, lesions becamediscrete with a hypoautofluorescent border and predomi-nant hyperautofluorescence centrally. The hyperreflective
fuzzy areas on SD-OCT scans disappeared, and irregular,knobbly elevations of outer retinal layers appeared. TheRPE, POST, IS/OS junction, and ELM could not bedistinguished. The ONL appeared normal. The choroidshowed an increased reflectance. As the lesions healedfurther over the next 3–6 months, they became predomi-nantly hypoautofluorescent with loss of RPE, POST, IS/OSjunction, and ELM in SD-OCT scan.Conclusion The SD-OCT provided an insight into theultrastructural changes in the outer retina during the courseof acute SLC lesions. The changes on OCT correlated withabnormal FAF findings.
Keywords Fundus autofluorescence . Spectral domainoptical coherence tomography . Tubercular serpiginouslikechoroiditis
Serpiginous choroiditis is a progressive, chronic, recurrentinflammatory disease primarily affecting the inner choroidand retinal pigment epithelial (RPE) cell layer [1].Serpiginouslike choroiditis (SLC) of presumed tubercularetiology is a distinct clinical entity that begins usually asmultifocal choroiditis lesions that coalesce and progress in aserpiginoid pattern [2, 3]. While the choriocapillaries havebeen shown to be the most affected layer in serpiginouschoroiditis (SC), the primary site of inflammation in SLC isnot yet known and is at best speculated, presumably thechoriocapillaries [4].
The simultaneous recordings of topographic and tomo-graphic images by using a combination of scanning laserophthalmoscopy and optical coherence tomography (OCT)have increased our understanding of the pathogenesis ofvarious diseases of the retina and choroid [5]. TheSpectralis HRA+OCT (Heidelberg Engineering, Heidelberg,
Summary statement Simultaneous spectral domain opticalcoherence tomography and fundus autofluorescence findingscorrelated well during the course of acute tubercular serpiginouslikechoroiditis and provided an insight into the ultrastructural changes inthe outer retina as the lesions healed.
R. Bansal : P. Kulkarni :V. Gupta :M. R. DograAdvanced Eye Centre,Post Graduate Institute of Medical Education and Research,Chandigarh, India
A. Gupta (*)Department of Ophthalmology, Advanced Eye Centre,Post Graduate Institute of Medical Education and Research,Chandigarh 160012, Indiae-mail: [email protected]
J Ophthal Inflamm Infect (2011) 1:157–163DOI 10.1007/s12348-011-0037-7

Germany) is a novel multimodal imaging device that enablesus to correlate confocal angiograms, fundus autofluorescence(FAF) images, and other imaging modes with the high-resolution spectral domain (SD)-OCT scans.
The role of OCT in patients with uveitis is complemen-tary to the conventional fundus photography and fundusfluorescein angiography (FA). More recently, FAF hasemerged as a very sensitive imaging modality to evaluateinflammatory disorders affecting the chorioretinal interface.The combined FAF and OCT signals have been effectivelyused in the evaluation of uveitic macular edema in terms ofvisual outcome [6]. The Spectralis HRA+OCT has beenused in imaging the choroid in intraocular inflammationusing the inverted scan technique.
We describe the changes in high-resolution SD-OCTscans that were simultaneously obtained with FAF signalson Spectralis HRA+OCT in four eyes of three patients withSLC who were followed from the stage of acute lesion tothe healed stage over a period of 3–6 months.
Methods
We prospectively followed four eyes of three patients withactive SLC. The diagnosis of SLC was made in thepresence of multifocal choroiditis lesions with centralhealing and active edges that were hyperautofluorescent inareas of active edges and hypoautofluorescent in healedareas and showed early hypofluorescence and late hyper-fluorescence of active lesions on FA. The etiology waspresumed to be tubercular if there was (a) corroborativeevidence (such as a positive tuberculin skin test orQuantiFERON-TB Gold test), (b) exclusion of all otherknown causes of infectious uveitis except tuberculosis andnoninfectious uveitic syndromes, and (c) a favorabletherapeutic response to antitubercular therapy. All patientsunderwent chest radiography that was normal. Besides acomplete clinical evaluation that included best-correctedvisual acuity (BCVA), intraocular pressure (IOP), slit lampbiomicroscopic examination, and conventional imagingmethods (digital photography and FA, when required, onVisupac 450 Plus, Carl Zeiss, Jena, Germany), thesepatients additionally underwent Spectralis HRA+OCT(Heidelberg Engineering, Heidelberg, Germany) imagingwith simultaneously obtained FAF and OCT images at allfollow-ups. The Spectralis system uses Heidelberg EyeExplorer Software Version 1.5.0 with Image CaptureModule Version 1.1.0. An infrared fundus image wasacquired parallel to OCT scan to ensure correct placementof image before acquiring FAF images simultaneous withOCT scans. The pupils were dilated before acquiring allscans. The Spectralis scans along with the FAF images wereobtained before doing FA, using the 30° field-of-view
mode. All images were recorded using the automatic real-time mode. The image acquisition was done by selectingthe dense volume scan type over a scan angle of 20° or 30°and by adjusting the width/height of the OCT scan(depending upon the extent of the lesions in the fundus).We routinely perform dense volume scan with simultaneousFAF and SD-OCT mode. We use infrared mode to focus thefundus image, and once focused, we switch to combinedFAF and SD-OCT mode and capture the images simulta-neously. An integrated eye tracking allowed for liveaveraging of FAF images and the SD-OCT scans. Thebaseline FAF-OCT images were defined as the referenceimages to enable acquisition of images at the same siteduring follow-up visits. Patients were seen every 2 weeksuntil the lesions healed. In addition to oral corticosteroids,all patients received four-drug antitubercular therapy in-cluding isoniazid (5 mg/kg/day), rifampicin (450 mg/day ifbody weight was ≤50 kg and 600 mg/day if body weightwas >50 kg), ethambutol (15 mg/kg/day), and pyrazinamide(25 to 30 mg/kg/day) initially for 3 to 4 months. Thereafter,rifampicin and isoniazid are used for another 9–14 months.Pyridoxine supplementation was given to all patientsreceiving antitubercular therapy until cessation of therapy.The corticosteroids were tapered depending upon theclinical response. All patients were receiving antituberculartherapy until their last visit and did not show any recurrenceof inflammation.
Demographic details and treatment response to oralcorticosteroids and antitubercular therapy were also noted.The OCT scans were analyzed and correlated with FAF/FAimages in acute as well as healing stages.
Results
During the course of the disease in patients with SLC, weobserved a progressively changing pattern on SD-OCTscans that was consistent with the abnormal FAF signalsdetected simultaneously.
1. In an acute lesion of SLC, there was an ill-defined areaof increased autofluorescence around the lesion. TheSD-OCT passing through the area showed a localized,fuzzy area of hyperreflectivity in the outer retinal layersinvolving the RPE, photoreceptor outer segment tips(POST), photoreceptor inner segment–outer segment(IS/OS) junction, external limiting membrane (ELM),and the outer nuclear layer (ONL). The lesion waslocalized external to the outer plexiform layer with amild distortion of the inner retinal layers. There was noincreased backscattering from the inner choroid.
2. As the lesions started to heal, they became well definedand acquired a thin border of hypoautofluorescence
158 J Ophthal Inflamm Infect (2011) 1:157–163

while remaining predominant hyperautofluorescentcentrally. The SD-OCT scan through the hyperauto-fluorescent area showed disappearance of the hyper-reflective fuzzy areas that were replaced by irregular,hyperreflective knobbly elevations of the outer retinallayers. The RPE, the POST, IS/OS junction, and theELM could not be distinguished. The ONL appearednormal. At this stage, there was an increased reflec-tance from the choroidal layers due to attenuatingRPE–photoreceptor complex.
3. As the lesions healed further over the next 3–6 months,they appeared stippled with predominantly hypoauto-fluorescence. The SD-OCT scan showed loss of RPE,POST, IS/OS junction, and ELM. The increasedreflectance from the choroid persisted.
The clinical details and the findings on FAF and SD-OCT during the healing of lesions are listed in Table 1.These changes are illustrated in Figs. 1 and 2.
Case example
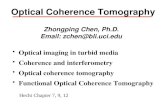
Patient 2: A 19-year-old male presented with decreased visionin both eyes since 3months. On examination, the BCVAwas 6/9 and 6/6 in the right and left eyes, respectively. The IOP were14 and 12 mmHg in the right and left eyes, respectively. Botheyes showed unremarkable anterior segment and multifocallesions of active as well as inactive choroiditis in the posteriorpole (Fig. 1a–f). Simultaneous FAF and SD-OCT imaging ofthe right eye revealed findings as explained in the “Results”Section (1.) (Fig. 2a). The QuantiFERON-TB Gold test waspositive. Other laboratory tests were normal. He receivedfour-drug antitubercular therapy with oral corticosteroids.About 2 weeks later, the lesions started to heal and appearedas described in “Results” Section (2.) (Fig. 2b). Threemonths later, the lesions healed further and appeared asexplained in “Results” Section (3.) (Fig. 2c). Likewise, lefteye imaging also showed a similar pattern of FAF and SD-OCT changes during acute, healing, and healed stages of thelesions (Fig. 2d–f).
Discussion
Tubercular SLC can be clinically differentiated from SC bythe frequent presence of vitritis and multifocal choroiditislesions in posterior pole and periphery, often sparing thejuxtapapillary region [3]. The lesions in SC are, however,usually around the optic disk and spread contiguously to themacula. People with SLC are from areas endemic fortuberculosis, have positive uveitis work-up for tuberculosis,and respond favorably to antitubercular therapy with oralcorticosteroids.T
able
1Clin
ical
details
ofpatientswith
activ
etubercular
serpiginou
slikechoroiditis
alon
gwith
find
ings
oncombinedfund
usautofluo
rescence
andSpectralis
domainop
tical
coherence
tomog
raph
yim
agingas
thelesion
sevolvedfrom
anacutestageup
tohealed
stage
Patient
Sex
Age
Eye
Initial
visual
acuity
AS
inflam
mation
Vitreous
cells
Typeof
SLClesions
TST
QuantiFERON-
TBGoldtest
FAFof
acute
lesion
SD-O
CTof
acutelesion
1M
20Right
CF1ft
Nil
++
Placoid
Positive
ND
Diffuse,feeble
hyperautofluorescent
Fuzzy,hyperreflectiveareas
involvingRPE,POST,
photoreceptorIS–O
Sjunctio
n,ELM
andONL
2M
19Right
6/9
Nil
+Multifocal
Negative
Positive
Left
6/6
Nil
+Multifocal
3M
35Left
6/9
Nil
Nil
Multifocal
Positive
ND
Patient
FAFof
healinglesion
SD-O
CTof
healinglesion
FAFof
healed
lesion
SD-O
CTof
healed
lesion
Follow-up(m
onths)
Final
visual
acuity
1Central
hyperautofluorescent
with
hypoautofluorescent
border
Irregular,knobblyelevations
ofouterretin
allayers
that
areindistinct.The
ONL
appearsnorm
al.
Predominantly
hypoautofluorescent
Lossof
RPE,POST,
IS–
OSjunctio
n,andELM
5CF1m
23
6/9
6/6
36
6/6
ASanterior
segm
ent,SL
Cserpiginou
slikechoroiditis,TST
tuberculin
skin
test,M
male,
CFcoun
tingfing
ers,
ND
notdo
ne,AFautofluo
rescence,SD
-OCTspectral
domainop
tical
coherence
tomog
raph
y,RPEretin
alpigm
entepith
elium,P
OST
photoreceptorou
tersegm
enttip
s,IS–O
Sjunctio
ninnersegm
ent–ou
tersegm
entjunctio
n,ELM
externallim
iting
mem
brane,ONLou
ternu
clear
layer
J Ophthal Inflamm Infect (2011) 1:157–163 159

The main histological findings described in SC areatrophy of the choriocapillaries, the RPE, and the photo-receptors [4, 7]. While the choriocapillaries was reported tobe the most affected layer that appeared acellular, the largechoroidal vessels were unremarkable. Moderate, diffuselymphocytic infiltration of the choroid has been reported,with predominant RPE atrophy. Occasionally, RPE hyper-trophy has been seen correlating with areas of pigmentclumping clinically [4, 7]. On the other hand, clinicopath-ological correlation in tubercular SLC is still not known.Clinically, SLC appears to involve primarily the innerchoroid and the RPE. However, isolation of Mycobacteriumtuberculosis from the RPE in an eye with tubercularpanuveitis has strongly suggested preferential localizationof the mycobacteria in the RPE, even in eyes withpanuveitis or related intraocular inflammation, includingmultifocal choroiditis or serpiginouslike choroiditis [8].
High-speed, high-resolution OCT, by providing unprec-edented details, has enhanced our understanding of theultrastructure of the retina [9]. Distinct scattering bandscorrespond to photoreceptor IS/OS junction, photoreceptorouter segment tips, and the RPE and represent the thickscattering bands of outer retina [9]. The SD-OCT changes inhealed scars of SLC have shown disruption of the outerretina at the site of scars with loss of junction between theinner and outer segments of photoreceptors and thinning ofRPE/Bruch membrane complex and a correspondent in-crease in light reflectivity from the choroid [3]. Areas of
thickening of RPE/Bruch membrane complex have alsobeen shown in the regions of scars. However, there is noreport of SD-OCT changes in any active and healing stagesof SLC lesions.
All eyes with active lesions of SLC in our patientsillustrate the progressive changes in the outer retinal layerson OCT scans that correlated with the FAF changes. TheFAF images obtained simultaneously demonstrated thetransition from initial hyperautofluorescent of acute lesionsto predominant hypoautofluorescent in the healed stage.Absence of any demonstrable changes in the inner choroidduring the active stage of the lesion on OCT scans maysuggest a primary involvement of the RPE and not thechoroid in tubercular SLC lesions. The FAF signals providea strong clue to the status of RPE cells in various degenerative,inflammatory, and neoplastic disease processes. The FAF isincreased (hyperautofluorescence) in the presence of in-creased metabolic activity of the RPE and decreased(hypoautofluorescence) when there is loss of the RPE.
We observed that the structural changes on OCT scansoccurring during the course of SLC followed a stepwiseorderly sequence, similar to those as seen on the FAFimages. Increased autofluorescence in the acute lesions seenas diffuse, subtle, feeble hyperautofluorescent probablyreflects retinal edema which was structurally evident ashyperreflectivity spreading into the outer retinal layers inthe OCT scans of our patients. This possibly suggestscellular infiltration or extracellular fluid accumulation in
Fig. 1 a–f Right eye fundus picture of patient #2 with inactive and active (arrows) lesions of serpiginouslike choroiditis (a) that appearedhypofluorescent in early (b) and hyperfluorescent in late-phase fluorescein angiogram (c). The left eye showed similar lesions (d–f)
160 J Ophthal Inflamm Infect (2011) 1:157–163

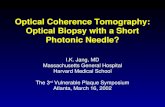
Fig. 2 Combined fundus autofluorescence (FAF) and spectral domainoptical coherence tomography (SD-OCT) images through the activelesion(s). The green frame (left panel) indicates the borders of thescanned area. The position marker corresponds to the retinal locationthrough which the displayed OCT scan is obtained. In the right eye (a–c), in acute stage (a), there is an ill-defined area of increasedautofluorescence (left panel) with fuzzy area of hyperreflectivity inouter retinal layers (white arrows) involving the retinal pigmentepithelium (RPE), photoreceptor outer segment tips (POST), photore-ceptor inner segment–outer segment (IS–OS) junction, external limitingmembrane (ELM), and outer nuclear layer (ONL) (right panel). Theinner retinal layers showed mild distortion. There was absence of anybackscattering from the inner choroid (red arrows). About 2 weeks later
(b), as the lesions started healing, they became well defined with a thinhypoautofluorescent border and predominantly hyperautofluorescencecentrally in the right eye (left panel). The SD-OCT showed irregularknobby elevations (white arrows) of the outer retinal layers (rightpanel). The RPE, POST, IS–OS junction, and ELM could not bedistinguished. There was an increased reflectance from the choroidallayers (red arrows) due to disappearing RPE–photoreceptor complex.Three months later (c), as the lesions healed further, they appearedstippled with predominantly hypoautofluorescence (left panel). The SD-OCT scan showed loss of RPE, POST, IS–OS junction, and ELM (whitearrows) (right panel). The increased backscattering of the choroidpersisted (red arrows). d–f Similar changes were seen in the left eye inacute (d), healing (e), and healed (f) stages of active lesions of SLC
J Ophthal Inflamm Infect (2011) 1:157–163 161

these layers due to inflammation. As the lesions startedhealing, hyperautofluorescence decreased and hypoauto-fluorescence increased due to loss of RPE. The outer retinallayers on OCT scans of our patients showed attenuation andprogressive loss in the affected areas as the lesions healed.The FAF becomes increasingly hypoautofluorescent whichindicates severe damage to RPE and photoreceptors. Thiswas seen as an irreversible, collective loss of the outerretinal layers involving the RPE, photoreceptor outer andinner segments, and the ELM in OCT scans.
Acute inflammatory lesions involving the RPE oftencause a thickening at the level of RPE. It is believed that thelesions in SC arise deep in the retina, and the overlyingretina appears edematous. The edema subsides as thelesions heal, and the RPE–choriocapillaries undergo atro-phy. There is loss of photoreceptor–RPE complex withvariable degrees of RPE hyperplasia. Yeh et al. havehypothesized that RPE may be the site of primary insultand hence, more severely damaged in presumedtuberculosis-associated serpiginouslike choroidopathy [10].Increased autofluorescence in acute phase may be due to anumber of factors. The size, number, or content of thefluorophores in the RPE cells may be altered by inflamma-tion which increases the fluorophores content by inducingcertain prooxidative pathways. Increased autofluorescencein other inflammatory conditions also such as White DotSyndromes has been correlated with areas of RPE elevationon OCT image during active disease [10]. Once healed, thehypoautofluorescent areas showed resolution of RPEabnormalities on OCT scan.
The FAF abnormalities (hyperautofluorescent in activestage progressively becoming hypoautofluorescent inhealed stage) have been well recognized (unpublisheddata). We observed that in the very initial stages of diseaseoccurrence, when there was feeble hyperautofluorescencein the areas of new lesions, the OCT showed hyper-reflectivity in the outer retinal layers that was fuzzy andill defined. The choroid did not show any reflectance. Thisis an important OCT finding during the acute stage of SLCthat may reflect the site of primary insult in SLC. However,SD-OCT technology is not yet able to image the choroidsimilarly to the retina, and hence, the absence of choroidchanges on SD-OCT is not enough to definitely exclude itsprimary involvement in SLC.
Hyperreflectivity in the outer retinal layers in an active SClesion is believed to be suggestive of acute inflammationinvolving deeper retinal and choroidal structures. From theOCT findings of our patients, we speculate that in an acutelesion of SLC, there is an increased metabolic activity causedby primary inflammation of the RPE cells. Release ofinflammatory mediators into the retinal layers adjacent to theRPE causes a fuzzy, hyperreflective appearance on SD-OCT.
Following an acute inflammatory episode, the RPE cellsundergo hyperplasia and hypertrophy which is evident ashyperautofluorescence on FAF due to increased collection oflipofuscin. This corresponds to the localized, knobbly eleva-tions of the outer retinal layers which represents clumping ofthe inflamed RPE cells. Once these damaged RPE cellsundergo atrophy, there is an irreversible loss of photoreceptorsgiving rise to the loss of the outer retinal layers on OCT. Thesimultaneous increased hypoautofluorescence depicts theatrophied RPE cells. The late pigmentation of the retinal scarassociated with RPE hypertrophy or hyperplasia also leads to adecreased FAF signal (especially when photoreceptors aredisrupted), as can also be seen in Figs. 1 and 2. The baring ofchoroidal vessels in healed lesions of SC in contrast to theirmasking by hyperpigmentary changes of the RPE in SLCmay also be due to entirely different entities affecting theinner choroid and the RPE cells, respectively.
The limitations of our study include a small number ofcases and lack of clinicopathologic correlation. The outerretinal bands on SD-OCT, particularly IS/OS junction andPOST, have not been so far correlated to the histologicalstructures, and such correlation is still mostly presumed.However, the sequential ultrastructural changes in the outerretinal morphology on SD-OCT scans as seen in ourpatients provide important information that may add anew dimension in understanding the primary site ofpathology in inflammatory conditions affecting the choroidand the RPE–photoreceptor complex.
Conflict of interest None of the authors have any proprietaryinterest.
Open Access This article is distributed under the terms of theCreative Commons Attribution License which permits any use,distribution and reproduction in any medium, provided the originalauthor(s) and source are credited.
References
1. Schatz H, Maumenee AE, Patz A (1974) Geographic helicoidperipapillary choroidopathy: clinical presentation and fluoresceinangiographic findings. Trans Am Acad Ophthalmol Otolaryngol78:747–761
2. Gupta V, Gupta A, Arora S et al (2003) Presumed tubercularserpiginouslike choroiditis: clinical presentations and manage-ment. Ophthalmology 110:1744–1749
3. Vasconcelos-Santos DV, Rao PK, Davie JB et al (2010)Clinical features of tuberculous serpiginouslike choroiditis incontrast to classic serpiginous choroiditis. Arch Ophthalmol128:853–858
4. Wu JS, Lewis H, Fine SL et al (1989) Clinicopathologic findingsin a patient with serpiginous choroiditis and treated choroidalneovascularization. Retina 9:292–301
162 J Ophthal Inflamm Infect (2011) 1:157–163

5. Helb HM, Issa PC, Fleckenstein M et al (2010) Clinicalevaluation of simultaneous confocal scanning laser ophthalmos-copy imaging combined with high-resolution, spectral-domainoptical coherence tomography. Acta Ophthalmol 88:842–849
6. Roesel M, Henschel A, Heinz C et al (2009) Fundus autofluor-escence and spectral domain optical coherence tomography in uveiticmacular edema. Greafes Arch Clin Exp Ophthalmol 247:1685–1689
7. Gass JDM (1987) Stereoscopic atlas of macular diseases:diagnosis and treatment, vol 1, 3rd edn. Mosby, St. Louis, pp 136–144
8. Rao NA, Saraswathy S, Smith RE (2006) Tuberculous uveitis:distribution of Mycobacterium tuberculosis in the retinal pigmentepithelium. Arch Ophthalmol 124:1777–1779
9. Srinivasan VJ, Monson BK, Wojtkowski M et al (2008)Characterization of outer retinal morphology with high-speed,ultrahigh-resolution optical coherence tomography. Invest Oph-thalmol Vis Sci 49:1571–1579
10. Yeh S, Forooghian F, Wong WT et al (2010) Fundus autofluor-escence imaging of the White Dot Syndromes. Arch Ophthalmol128:46–56
J Ophthal Inflamm Infect (2011) 1:157–163 163