High-dose daunorubicin therapy for acute nonlymphocytic leukemia: Correlation of response and...
9
HIGH-DOSE DAUNORUBICIN THERAPY FOR ACUTE NONLYMPHOCYTIC LEUKEMIA: CORRELATION OF RESPONSE AND TOXICITY WITH PHARMACOKINETICS AND INTRACELLULAR DAUNORUBICIN REDUCTASE ACTIVITY WILLIAM GREENE, MD, DAVID HUFFMAN, MD, PETER H. WIERNIK, MD, STEPHEN SCHIMPFF, MD, ROBERT BEN JAMIN, MD, AND NICHOLAS BACHUR, PHD, MD Daunorubicin, administered in large doses intermittently to 23 patients with acute nonlymphocytic leukemia (ANLL), produced a complete hematologic remission rate of 33%. Five of 16 (31%) previously untreated patients achieved complete hematologic remission. Clinical response was closely correlated with in vitro determinations of peripheral leukemic myeloblast daunorubicin reductase activity. The measurement of the activity of daunorubicin reductase in peripheral myeloblasts from patients with ANLL prior to therapy may serve to identify those patients least likely to respond favorably to dauno- rubicin therapy in the dose and schedule used in this study. CUTE NONLYMPHOCYTIC LEUKEMIA (ANLL) A has remained, unlike acute lymphocytic leukemia (ALL), relatively resistant to chemo- therapy.14 Improvements in supportive care, e.g., platelet transfusions and new anti-Pseu- domonas antibiotics, have only partially modi- fied the toxicity of chemotherapeutic regi- mens.13J9,21 A more important approach in reducing the toxicity of the therapy of this disease would be improved specificity and increased efficacy of antileukemic drugs. In recent years several new agents or com- binations of agents have been introduced for the management of ANLL.9914 Daunorubicin (DNR), an antitumor antibiotic isolated from the mold Streptornyccs peucetius,22 has under- gone extensive clinical trial, especially in Eur0pe.4.5~12 Although toxic, it has been shown to be effective in ANLL producing remission rates near 50% in some studies.4925 Presented at the Eighth Annual Scientific Meeting, American Society of Clinical Oncology, Inc., Boston, Mass., May 3, 1972. From the Medicine and Biochemistry Sections of the Baltimore Cancer Research Center, National Cancer Institute, Baltimore, Md. Address for reprints: W. Greene, MD, Baltimore Cancer Research Center. 3100 Wvman Park Dr.. Balti- ore, MdT21211. secretarial assistance of Mrs. Nancy Cusack. The authors gratefully acknowledge the excellent Received for publication September 5, 1972. Published American experience with DNR as the sole antileukemic agent, however, has been limited.6 Previous studies have indicated that DNR, which interferes with nucleic acid metabolism, is metabolized extensively in vitro and in vivo by rat and man.l,2,1° A metabolic conversion common to all tissues is the reduction of DNR to daunorubicinol by the enzyme daunorubi- cin reductase.3 Both DNR and daunorubici- no1 are pharmacologically active and have long serum half lives. Since this conversion occurs in human blood cells,l6 we measured dauno- rubicin reductase activity in peripheral leu- kemic myeloblasts to determine its relation- ship, if any, to the clinical response to DNR therapy. We also studied the efficacy of a schedule of single, large doses of DNR admin- istered intermittently on the suggestion of the preceding data that persistent serum levels after one large dose might be equivalent to the usual schedule of daily smaller doses1 Evi- dence is presented that suggests that, by using biochemical criteria, one may be able to select those patients least likely to respond to dauno- rubicin. METHODS Patients: Twenty-three patients with a diag- nosis of ANLL were admitted to the Medical 1419
-
Upload
william-greene -
Category
Documents
-
view
212 -
download
0
Transcript of High-dose daunorubicin therapy for acute nonlymphocytic leukemia: Correlation of response and...

HIGH-DOSE DAUNORUBICIN THERAPY FOR ACUTE NONLYMPHOCYTIC LEUKEMIA:
CORRELATION OF RESPONSE AND TOXICITY WITH PHARMACOKINETICS AND
INTRACELLULAR DAUNORUBICIN REDUCTASE ACTIVITY
WILLIAM GREENE, MD, DAVID HUFFMAN, MD, PETER H. WIERNIK, MD, STEPHEN SCHIMPFF, MD, ROBERT BEN JAMIN, MD,
AND NICHOLAS BACHUR, P H D , MD
Daunorubicin, administered in large doses intermittently t o 23 patients with acute nonlymphocytic leukemia (ANLL), produced a complete hematologic remission rate of 33%. Five of 16 (31%) previously untreated patients achieved complete hematologic remission. Clinical response was closely correlated with in vitro determinations of peripheral leukemic myeloblast daunorubicin reductase activity. The measurement of the activity of daunorubicin reductase in peripheral myeloblasts from patients with ANLL prior to therapy may serve to identify those patients least likely to respond favorably to dauno- rubicin therapy in the dose and schedule used in this study.
CUTE NONLYMPHOCYTIC LEUKEMIA (ANLL) A has remained, unlike acute lymphocytic leukemia (ALL), relatively resistant to chemo- therapy.14 Improvements in supportive care, e.g., platelet transfusions and new anti-Pseu- domonas antibiotics, have only partially modi- fied the toxicity of chemotherapeutic regi- mens.13J9,21 A more important approach in reducing the toxicity of the therapy of this disease would be improved specificity and increased efficacy of antileukemic drugs.
In recent years several new agents or com- binations of agents have been introduced for the management of ANLL.9914 Daunorubicin (DNR), an antitumor antibiotic isolated from the mold Streptornyccs peucetius,22 has under- gone extensive clinical trial, especially in Eur0pe.4.5~12 Although toxic, it has been shown to be effective in ANLL producing remission rates near 50% in some studies.4925
Presented at the Eighth Annual Scientific Meeting, American Society of Clinical Oncology, Inc., Boston, Mass., May 3, 1972.
From the Medicine and Biochemistry Sections of the Baltimore Cancer Research Center, National Cancer Institute, Baltimore, Md.
Address for reprints: W. Greene, MD, Baltimore Cancer Research Center. 3100 Wvman Park Dr.. Balti- ore, MdT21211.
secretarial assistance of Mrs. Nancy Cusack. The authors gratefully acknowledge the excellent
Received for publication September 5 , 1972.
Published American experience with DNR as the sole antileukemic agent, however, has been limited.6
Previous studies have indicated that DNR, which interferes with nucleic acid metabolism, is metabolized extensively in vitro and in vivo by rat and man.l,2,1° A metabolic conversion common to all tissues is the reduction of DNR to daunorubicinol by the enzyme daunorubi- cin reductase.3 Both DNR and daunorubici- no1 are pharmacologically active and have long serum half lives. Since this conversion occurs in human blood cells,l6 we measured dauno- rubicin reductase activity in peripheral leu- kemic myeloblasts to determine its relation- ship, if any, to the clinical response to DNR therapy. We also studied the efficacy of a schedule of single, large doses of DNR admin- istered intermittently on the suggestion of the preceding data that persistent serum levels after one large dose might be equivalent to the usual schedule of daily smaller doses1 Evi- dence is presented that suggests that, by using biochemical criteria, one may be able to select those patients least likely to respond to dauno- rubicin.
METHODS
Patients: Twenty-three patients with a diag- nosis of ANLL were admitted to the Medical
1419

1420 CANCER December 1972 VOl. 30
Service of the Baltimore Cancer Research Center hom March 1, 1970 to June 30, 1971; 16 were previously untreated and 7 were in re- lapse following previous remissions achieved with other combinations or a different sched- ule of DNR (Table 1). Admission evaluation consisted of a complete history and physical examination, chest and abdominal x-rays, lumbar puncture, complete blood count (CBC), platelet count, and differential; blood urea nitrogen, creatinine, liver function tests, serum protein and albumin (done on an SMA-12 Autoanalyzer); electrolytes, urinalysis, and electrocardiogram. The referring diagno- sis was confirmed or that of relapse made by bone marrow examination.
Drug regimen: The DNR was administered as a rapid intravenous (I.V.) injection of 180 mg/m2 body surface area (BSA) delivered over 3 to 15 min. into a peripheral vein via a run- ning infusion of dextrose in water. In one pa- tient, local pain required a slower rate of ad- ministration over 1 hour. In general, patients were premedicated with chlorpromazine and acetaminophen and these were continued after the DNR dose at 4-hour intervals for 24 hours. CBC’s, differentials, platelet counts, and SMA-12 determinations were obtained routinely three times per week or more often, if clinically indicated.
A repeat bone marrow examination was performed approximately 9 to 10 days after the initial dose, If the bone marrow was hypo- cellular, with no decrease in percentage of “blasts,” the patient was retreated immedi- ately with DNR at a dose of 120 mg/m”; normo- or hypercellular, with no decrease in percentage of blasts, a second dose of DNR was given at that time at 180 mg/m2; or im- Proved from the pretreatment marrow or se- verely hypocellular, further therapy was de- ferred and repeat aspiration was performed 4 to 7 days later. Treatment was withheld as long as the bone marrow morphology contin- ued to improve. The routine after the second dose was exactly the same as that after the first. No patient was given more than three doses of DNR. If no response was evident after the third dose, the patient was consid- ered to be refractory and was begun on an- other drug. No patient received any “consoli- dation,” “cytoreductive,” or maintenance chemotherapy in this study.
Enzyme studies: Leukemic myeloblasts and erythrocytes were separated from heparinized venous blood obtained from the patients prior
to therapy with DNR. After these cellular fractions were isolated by differential centrifu- gation and hypotonic lysis,lO they were homog- enized in two volumes of 0.05 M Tris-C1 (PH 7.44). The level of daunorubicin reductase contained in the homogenates was estimated by a previously described m e t h ~ d , ~ capable of detecting low levels of enzyme activity with high accuracy and precision. One enzyme unit is defined as the activity that produces one nanamole of daunorubicinol per milligram of protein in 30 min. Some instability of dauno- rubicin reductase has been noted previously, both in hematologic and nonhematologic tis- sue preparations. Therefore, in order to stand- ardize the day-to-day estimation of the enzyme, the ratio of myeloblast reductase activity to erythrocyte reductase activity was deter- mined for each patient. With the exception of one patient who had no circulating leukemic cells, the 13 patients studied enzymatically had >80% myeloblasts in the analyzed ho- mogenate. These ratios were derived at a time just prior to DNR therapy and were done on a double blind basis, the results being unavail- able to the physician caring for the patient until the patient either obtained a response or was taken off study.
Results of therapy: The results of therapy were assessed by the criteria and terms set forth by the Acute Leukemia Group B.8 A complete remission consisted of a return to normal of peripheral blood, bone marrow, and physical examination in an asymptomatic patient.
Ancillary therapy: All patients were treated on the same ward by the same nursing staff and primarily by one physician (WHG). Packed red blood cells and platelet transfu- sions were used frequently. Repeated WBC transfusions from blood relatives prepared with the IBM cell separator were adminis- tered in three patients. Extensive surveillance culturesz0 were routine; other cultures were obtained as indicated. Systemic antibiotic therapy with carbenicillin and gentamicin for presumed infection was empiric until results of cultures were known.21 Six patients spent all or part of their hospitalization in a lami- nar air flow (LAF) unit, taking oral, “prophy- latic,” nonabsorbable antibiotics for gastroin- testinal microbial flora suppression. The other 17 patients were given either ward care alone or ward care plus oral antibiotics.20
Statistical calculations: P values were deter- mined utilizing the student’s ‘ I t ” test. Pear-

No. 6 DAUNORUBICIN IN ACUTE NONLYMPHOCYTIC LEUKEMIA - Greene et al. 1421
TABLE 1. A. Previously Untreated Patients
Previous Complications a t DNR doses Patient Age/sex Diagnosis: therapy$ time of therapy (mg/m2 BSA)
R. L.* J. R.t B. S. N.J.
J.H. E.S.
M.R.
W.S.
E.G.* A.K.
M.G.t J.A.* G.M. A.E.? E.K.t T.W.
26/M 45/M 51/F 73/F
60/M 64/F
62/F
65/M
72/M 63/F
26/M 64/M 66/M 55/M 55/F 54/M
AML AMML AMML AML
AML AML
AML
AML
AML AMML
AML AMOL AML AML AML AML
O.E.* 54/F AML W.D.* 27/M AML
S.H. 29/F APL
J.D.7 20/M AML
R.H. 34/F AML
D.H.t 20/M AML
B.B. 27/M AML
None None 6-MP x10 days None
None None
H ydroxyurea None
Prednisone x 1 week
None
None None
None H ydroxyurea H yd rox y urea
None None
None Congestive heart failure: diabetes mellitus: urinary tract infection Rectal abscess Acute myocardial infarction and conges- tive heart failure; dia- betes mellitus Diabetes mellitus: psychotic depression
Acute myocardial infarction
None History of angina pectoris
None None
Rectal abscess None None
H ydroxyurea None
180, 120 180, 180,120 180, 120, 120 180,120
180, 120 180
180,120
180,120
180 180,120,180
180,120 180
180, 180, 180, 180, 180 180, 120,180
Results11
CR NR CR
Died in induction
Died in induction Died in induction
Complete hematologic remission; died of progressive pneumonia Died in induction
Died in induction Died in induction
CR PR NR
Died in induction NR
180,180,180 NR
B. Previously Treated Patients POMP -+ CR Acute pyelonephritis 180,180,120 CR POMP -1 CR None 180,180 CR x2 DNR -+ CR None 180, 180 PR X 2, Ara-C and TG-+ C R X 1 DNR -+ CR, None 180,180 Died in induction Ara-C and TG-l CR, re- f ractory subsequently to POMP, and Ara-C and TG DNR -+ CR None 180,120 Switched to POMP
Ara-C, TG, None 180 Died in induction Vcr, and pred nisone Multiple agents None 180,180,180 NR
after 2 doses
* Received oral “prophylactic” antibiotics for microbial flora suppression while on the ward. f Spent all or part of their time on study in a laminar air flow room receiving oral “prophylactic” antibiotics
for microbial flora suppression. AML = Acute myelogenous leukemia. AMML = Acute myelomonocytic leukemia. AMOL = Acute monocytic leukemia. APL = Acute progranulocytic leukemia.
6-MP = 6-mercaptopurine. POMP = Prednisone, vincristine, methotrexate, and 6-mercaptopurine. Ara-C = Cytosine arabinoside. TG = Thioguanine.
11 CR = Complete remission. PR = Partial remission. NR = No response.
* DNR = Daunorubicin.

1422 CANCER December 1972 Vol. 30
son’s correlation coefficient was used for the regression analysis.
RESULTS Remissions (Table 1)
Patients with previous remissions: There were seven patients who had achieved a com- plete remission previously with other drugs or DNR, four male and three female, with a mean age of 30 years (range 20-54). Of these, two sustained a complete remission and one a partial remission; two died during induction therapy; one had no response and was switched to another drug, and one was consid- ered not evaluable because she was given an- other antileukemic agent before receiving a full course of daunorubicin. Among the evalu- able patients, the complete remission rate is 2/6 (3379. The three patients (O.E., W.D., S.H.) who obtained remission received three, two, and two doses of daunorubicin achieving remission after 42, 49, and 29 days, respec- tively. O.E.’s remission was her second, and lasted 8 months, preceded by a 4-month remis- sion induced with POMP. W.D. bad pre- viously achieved remission twice after POMP induction, The remission obtained in this study lasted 6 weeks as had the previous two. S.H. had acute progranulocytic leukemia which had twice responded to a different schedule of daunorubicip and once to cytosine arabinoside and thioguanine with remissions lasting 10, 2, and 2 months, respectively. She was reinduced with the protocol described in this report and died, in partial remission of 2 weeks, from refractory congestive heart failure and cardiogenic shock, possibly secondary to Candida sepsis.
Previously untreated patients: There were 16 newly diagnosed patients, ten male and six female, with a mean age of 56 (range 26-73). One (J.R.) had received 10 days of 6-MP with- out change in bone marrow picture; another (M.R.) was given approximately one week of prednisone for hypercalcemia, without change in bone marrow status; and three (J.W., J.H., J .A.) received two daily doses of hydroxyurea for control of leukocytosis 2 to 11 days prior to daunorubicin. Of the 16 patients, four (25%) achieved complete hematologic remis- sion-one was marred by the appearance 5 days later of meningeal leukemia, but the others had complete symptomatic as well as hematologic remission; one developed a nor- mal bone marrow and hematogram but died
of progressive pneumonia; four (25%) were refractory and were given other drugs, and seven (44%) died during induction therapy, either prior to or just after the second dose of DNR. The remitters in this group (J.A., M.G., R.L., B.S.) received 1, 2, 2, and 3 doses, respectively, requiring 28, 30, 30, and 64 days, respectively, before achieving remission.
One patient (R.L.) obtained three remis- sions on this regimen, lasting 5, 4, and 3 weeks, respectively, and died during an at- tempted fourth reinduction with cytosine ara- binoside and thioguanine. Patient B.S., having gained partial remission status at 41 days after DNR and complete remission status at 64 days, remained in remission for 7 months, was reinduced with a different regimen at 10 months, and remains alive and well at this time, 17 months after her first admission to this Center. M.G.’s remission lasted 2 months, as did the hematologic and bone marrow re- mission of J.A., whose meningeal leukemia was controlled by intrathecal methotrexate.
Among the previously untreated patients, the responders survived a mean of 9.5 months (range 4-17+ months). The nonresponders av- eraged a survival of 9 weeks (range 5-14 weeks) and the patients dying during induc- tion survived a mean of 3.5 weeks (range 1.5-8 weeks). The preponderance of elderly patients in this group is apparent and adversely af- fected overall s~rvival.2~
Of the 23 patients in this study, six were al- located to the LAF unit, two patients with previous remissions and four previously un- treated patients. Only one of these six went on to achieve a remission.
Enzyme studies: Thirteen patients had en- zyme analyses. As can be seen from Table 2, those patients responding to DNR in this schedule had the highest myeloblast- :erythrocyte daunorubicin reductase ratios. The mean ratio for the four patients who achieved hematologic remission was 44.5 f 3.0 (mean f S.D.) which was significantly greater (p <0.05) than the level (20.2 ? 9.9) for those patients failing to achieve remission.15 Inter- estingly, there was no difference (p >0.05) be- tween the level for the nonresponding group (20.2 f 9.9) and that obtained for the patients dying during induction therapy (20 4 5.3). One patient (R.H.) had a ratio of 54.5 but was not evaluable for this study because dauno- rubicin was discontinued after only 2 doses. She had, however, previously responded to daunorubicin in a different schedule, and her

No. 6 DAUNORUBICIN IN ACUTE NONLYMPHOCYTIC LEUKEMIA - Greene et al. 1423 TABLE 2. Daunorubicin Reductase Activity
L I I I I I I
Myeloblast Erythrocyte ( M ) D N R (E) D N R
R
reductase reductase activity activity M:E reductase Hematologic
Patient (units)* (units)* activity ratio Mean ratio* P value response
R.L. M.R.
J.A. S.H. N.J. J.H. E.S. A.K. G.M. J.R. J.W. R.H. B.S.
58 54.8
31.7 67.5 19.5 28.7 67.5 47.5 57.7 12.8 59.7 74.5 4.5+
1.3 1.37
0.7 1.4 0.84 2.2 3.6 1.9 2.5 1.4 2.09 1.37 1.43
44.6
I 44.5 f 3.0 40.01
45.31 48.2 23.21
13'0 1 I1 18.8
20 f 5.3
25. o] 23.11 "'1 111 20.2 f 9.9 28.4 54.4 3.15'
Complete Complete hematologic remission- died of progressive pneumonia Complete
I vs. I1 Complete < O , 01 Died in induction
Died in induction Died in induction
<0.05 Died in induction I vs. I11
No response No response No response Not evaluable Complete
* One enzyme unit defined as one nanamole daunorubicinol per mg protein per 30 min. + Patient was aleukemic and had no circulating myeloblasts. t Entries represent mean & standard deviation.
bone marrow was pancytopenic without circu- lating blasts when the daunorubicin was stopped. The ratios bore no apparent relation- ship to either sex or previous therapy nor did the absolute level of myeloblast daunorubicin reductase correlate with these factors. In view of the large number of therapeutic failures in patients over the age of 60, a least-squares re- gression analysis was performed comparing the age of each patient with his daunorubicin reductase ratio (Fig. 1). This demonstrated a significant inverse correlation (r = -0.534, p < 0.01). The meaning of this relationship is unclear since no such correlation was noted among normal controls, but it may, in part, explain the poorer response rate among older patients, although the latter appears to be true regardless of regimen used.25
Toxicity Hematologic: Myelosuppression was univer-
sal and severe. Even among those patients who ultimately were not improved by the drug, cir- culating leukocytes and blast cells were invari- ably depressed with each dosage, as were plate- lets and erythrocytes. Means and medians were calculated for the day post-therapy that the WBC nadir occurred, as well as for the ac- tual WBC nadir after the first and second
dose (Table 3). These calculations exclude the five patients who received hydroxyurea or 6- MP prior to the daunorubicin therapy. The maximum WBC depression for previously un- treated (PU) and previously treated (PT) pa- tients after the first dose occurred at approxi- mately 9 days and 7 to 9 days after the second dose, which was, on the average, given to PU patients on day 16 and to P T patients on day 10. The apparent delay in therapy for the PU patients is related to the fact that many P T patients, while having pancytopenia, did not
!Ot 40 * * .
30t 3 20 ( I 5 10
& a
2 .
d

1424 CANCER December 1972 VOl. 30
TABLE 3. Maximum WBC Depression
Mean Median
All patients (18) First dose
Day of nadir
Day of second dose
Day of nadir
WBC/rnrn3 X lo3 a t nadir
Second dose
WBC/rnrn3 X lo3 a t nadir
Previously untreated patients (1 1) First dose
Day of nadir
Day of second dose
Day of nadir
WBC/mm3 X lo3 at nadir
Second dose
WBC/mm3 X lo3 a t nadir
Previously treated patients (7) First dose
Day of nadir
Day of second dose
Day of nadir
WBC/mrn3 X lo3 a t nadir
Second dose
WBC/mm3 X 103 a t nadir
9 0.630
13
9 0.423
9 0.573
16
7 0.486
10 0.729
11
10 0.350
8 0.700
12
9 0.300
8 0.600
15
7 0.400
9 0.700
11
9 0,300
suffer parallel marrow toxicity. Thus, DNR therapy was rarely delayed by severe marrow hypoplasia in P T patients. This explanation is confirmed by the fact that of the six P T pa- tients receiving 2 doses, only one required at- tenuation of the second dose from 180 mg/m2 to 120; whereas 9 of the 13 PU patients re- quired this reduction. The actual WBC and
t
DAYS AFTER FIRST DOSE DAYS AFTER SECOND DOSE
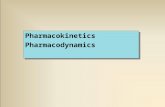
FIGURE 2.
granulocyte nadirs (lOOO/mm3 or less, and 500/mm3 or less, respectively) were similar for both groups.
The serial mean circulating leukocyte counts after therapy for PU and P T patients calculated separately or collectively in terms of days after the first and second dose are com- pared in Fig. 2. The combined curve suggests that patients remained continually leukopenic until after the second dose and that recovery began 8 to 11 days following that dose. When the PU patients are compared with the P T patients, certain differences in granulocyte ki- netics emerge. Although not statistically sig- nificant, the delay in WBC recovery of the P T patients as compared to the PU patients is striking. All PU patients who attained a post- therapy WBC of 3000/mm3 or greater did so within 3 weeks of the last dose, while the six surviving P T patients required 14, 17, 29, 32, 44, and 46 days to similarly recover. Maxi- mum depression and recovery of the platelet count paralleled the WBC, including the trend toward prolonged depression among previously treated patients.
Oropharyngeal-Gastroin testinal Nausea and vomiting: Of the 50 doses of
DNR administered to 23 patients, 15 doses (30%) in eight patients were accompanied by nausea and/or vomiting ranging from anor- exia to severe emesis. In general, these symp- toms abated within 24 hours. I n three patients, however, moderate nausea and vomit- ing persisted for 3 to 7 days. Those patients who had GI symptoms on the first dose also tended to have them on subsequent doses.
Pharyngitis: Eleven of the patients devel- oped moderate-to-severe pharyngitis22 charac- terized by erythema and, occasionally, superfi- cial mucosal erosion. Onset varied from day 4 to day 29 following the first DNR dose. In four patients, the pharyngitis progressed to bacteremia. Full relief of symptoms fre- quently was dependent upon discontinuation of daunorubicin after complete remission or induction failure.
Fever: Following 23 injections (46%) in 15 patients, a rise in body temperature to >100F or a rise of 1F above a previously stable tem- perature occurred within 2 to 12 hours (usually preceded by a shaking chill), and re- turned to baseline within 24 hours. The peak temperature was, in most instances, less than or equal to 102F; however, elevations u p to 105" were seen. Repeated blood cultures taken

No. 6 DAUNORUBICIN IN ACUTE NONLYMPHOCYTIC LEUKEMIA * Greene et al. 1425 during these episodes were negative for bac- terial or fungal growth.
Cutaneous Local reactions: Four patients developed a
chemical cellulitis, two of them severe, follow- ing administration of DNR into small venous radicles, without apparent extravasation. Most of these patients noted local pain during drug administration, which resolved when the rate of administration was slowed.
Alopecia: Alopecia occurred to some degree in all patients, usually requiring temporary provision of wigs. Regrowth of hair, begin- ning weeks after discontinuation of DNR, was the rule.
Cardiac: See Deaths. No renal or hepatic toxicity could be definitely ascribed to DNR.
Deaths (Table 4): Ten patients died during induction therapy, six from infection, one from hemorrhage, and two from hemorrhage and infection. One patient’s death was of un- certain cause. A 20-year-old man (J.D.) died while pancytopenic in refractory congestive heart failure and shock of abrupt onset several weeks after his last DNR dose. Despite a clini- cal picture of sepsis, numerous pre- and post- mortem cultures revealed no growth of orga- nisms. In addition, no site of infection could be demonstrated at autopsy. The heart, how- ever, was dilated with microscopic evidence of interstitial edema and mild myocardial de- generation. He received 1000 mg (20 mg/kg) over his 3-year course (520 mg in the month prior to death), and may well represent an example of DNR cardiac toxicity.
The preponderance of elderly patients in the previously untreated group is reflected in the mortality ~tatistics.2~ Of the nine patients more than 60 years of age, seven died during induction therapy; of those seven patients younger than 60, only one failed to complete the course of therapy (p < 0.05).
DISCUSSION
Progress in the treatment of acute leukemia has been greatest in acute lymphoblastic leu- kemia. Remission rates in excess of 90% are commonplace in that disorder using agents which are not appreciably mye10toxic.l~ In contrast, improvement in the therapy of acute nonlymphocytic leukemia has been slow, and remission rates near 50% are attained only at the expense of profound and, usually, pro- longed bone marrow toxicity with its resultant
TABLE 4. Causes of Death ~~ ~
A. Infection-6 B. Hemorrhage-1 (subarachnoid) C. Hemorrhage and infection-2
Bacteremia and aspiration during severe epistaxis -1 Subarachnoid hemorrhage and bacteremia -1
D. Unknown-1 (possible daunorubicin cardiac toxicity )
anemia, granulocytopenia, and thrombocyto- p e n i a . l 3 ~ ~ ~ Although advances in supportive care, such as new anti-Pseudomonas anti- biotics and platelet transfusions,13,21 have modified the consequences of this toxicity to some extent, the frequency of deaths during therapy attests to the overall inadequacy of these advances.llJ5
The most rewarding approach to this prob- lem thus far has been the use of controlled, clinical trials of hopefully less toxic and more effective schedules of old and/or new antileu- kemic agents after animal studies have sug- gested antileukemic activity and preliminary clinical studies have established a reasonably tolerated dose. Indeed, the present study is a clinical trial of a new schedule of a previously investigated agent. The schedule used in this trial results from earlier pharmacokinetic studies1 that suggested that one dose of DNR at a level of 140 mg/m2 or more would give serum drug concentration curves similar to those obtained in a previous study by Serpick and Wiernik using 3 daily doses of 60 mg/m2.25 The latter was a controlled trial which resulted in a 50% remission rate for DNR as compared to 26% for POMP. Other studies also have suggested remission rates of 50% or more with daily I. V. administra- tion,6,12 although response criteria and pa- tient populations have not always been speci- fied or uniform.
In any event, it seems clear that the remis- sion rate in the present trial was diappoint- ingly low. Two factors appear to be pertinent in this regard: 1. The PU group was heavily weighted with patients greater than 60 years of age, with multiple “degenerative” complica- tions of that age group. Previous studies have demonstrated the increased mortality and morbidity of leukemia in elderly patients,24 and this was reflected in our present trial, in which there was a statistically significant de- crease in response and survival in patients older than 60 years. 2. More recent biochemi-

1426 CANCER December 1972 Vol. 30
cal and pharmacokinetic data reveal that the major component of the prolonged plasma half-life previously observed €or DNR and its metabolites is daunor~bicinol l~ and that dau- norubicinol penetrates cells less readily than daunorubicin.18 This suggests that previous schedules of sequential daily doses may allow high concentrations of daunorubicinol in leu- kemic cells by providing higher plasma levels of daunorubicin to serve as substrate for intra- cellular daunorubicin reductase.
In addition to trying new agents or new schedules of old ones, one might improve the efficacy of therapy in ANLL if predictive bio- chemical tests for active compounds were available, Such tests allow therapy to be fitted to the patient, as well as his disease. An in vitro test partially reliable in identifying ALL patients likely to be refractory to L-asparagi- nase therapy exists,8 but no such test has been devised for drugs useful in ANLL. T h e pres- ent study suggests a correlation between intra- cellular levels of daunorubicin reductase activ- ity and clinical response to DNR. When this correlation was examined by standard statisti- cal techniques, i t was confirmed. The number of patients in each group, however, i s so small that it is indeed possible that there i s no cor- relation and that these results are fortuitous. Since daunorubicin reductase ratios in leu- kemic patients correlate well with the age of the patient, it is also possible that the correla- tion we have described between reductase ra- tios and response to therapy is simply a confir-
mation of the well-known fact that older leu- kemic patients have a poorer prognosis than younger ones, regardless of the therapy used. Nevertheless, it should be noted that two of the four patients with hematologic and bone marrow remissions associated with high reduc- tase ratios were older than G O . Cognizant of these limitations, it would appear that meas- urement of daunorubicin reductase activity prior to therapy might be helpful in identify- ing patients least likely to respond to dauno- rubicin in the schedule and dose employed in this study. By withholding daunorubicin ther- apy from such patients, the number of respon- ses among patients treated with daunorubicin might be significantly increased, and the num- ber of deaths during therapy might be re- duced. Studies are in progress in this labora- tory to test this proposal.
One further aspect of this study requires comment. The hematologic toxicity of this schedule was profound and universal. Never- theless, previously treated patients, even those treated months before, with an intervening remission, had prolonged bone marrow de- pression well beyond that seen in previously untreated patients. The explanation for this finding is not immediately apparent but simi- lar data have recently been obtained for 1 - (2-bischloroethyl)-3 -cyclohexyl- 1 - nitrosurea (CCNU).23"
* M. D. Walker: Personal communication, January 1972.
REFERENCES
1. Alberts, D. S., Bachur, N. R., and Holtzman, J. L.: The pharmacokinetics of daunomycin in man. Clin. Pharmacol. Therap. 12:196-204, 1971.
2. Bachur, N. R., and Cradock, J. C.: Daunomycin metabolism in rat tissue slices. J . Pharmacol. Ex!). Therap. 175:331-337, 1970.
3. Bachur, N. R., and Huffman, D. H.: Daunorubi- cin metabolism: estimation of daunorubicin reductase. Br. J . Pharrnacol. 43:828-833, 1971.
4. Bernard, J., and Boiron, M.: Current status: Treatment of acute leukemia. Semin. Hemntol. 7:427-440, 1970.
5. Boiron, M., et al.: Daunorubicin in the treatment of acute myelocytic leukaemia. Lancet 1:330-333, 1969.
6. Bornstein, R. S., Theologides, A,, and Kennedy, B. J.: Daunorubicin in acute myelogenous leukemia in adults. J A M A 207: 1301-1306, 1969.
7. Capizzi, R. L., et al.: L-asparaginase: Clinical, bio- chemical, pharmacological and immunological studies. Ann. Intern. M e d . 74:893-901, 1971.
8. Ellison, K. R., et al.: Arabinosyl cytosine: A use- ful agent in the treatment of acute leukemia in adults. Blood 32:507, 1968.
9. Fairley, G. H.: The treatment of acute myelohlas- tic leukemia. Br. J. Haernatol. 20:567-570, 1971.
10. Fallon H. J., Frei, E., Davidson, J. D., Trier, J S., and Burk, D.: Leukocyte preparations from human blood: Evaluation of their morphologic and metabolic state. J . Lah. Clin. M e d . 59:779-791, 1962.
11. Gee, T. S., You, K-P, and Clarkson, B. D.: Treat- ment of adult acute leukemia with arabinosylcytosine and thiognanine. Cancer 23: 1019-1032, 1969.
12. Goudenand, M., Sautiere-Habay, D., Bauters, F., and Lerche-Habart, B.: Treatment with rubidomycin of 35 cases of acute myeloblastic leukemia. Lilk M e d . 14:257-263, 1969.
13. Han, T., Stutzman, L., Cohen, E., and Kim, U.: Effect of platelet transfusion on hemorrhage in pa- tients with acute leukemia: An autopsy study. Cancer 19:1937-1942, 1966.
14. Henderson E. S.: Treatment of acute leukemia. Semin. Hematol. 6:271-319, 1969.
15. Huffman, D. H., and Bachur, N. R.: Daunorubi- cin metabolism in acute myelocytic leukemia. Blood 39:637:643, 1972.
16. Huffman, D. H., Bachur, N. R., and Gee, M.:

tainic.iii for felii-ilc paticiits with taiiccr aiitl giariulocy- topeiiia. S. Etig l . , I . '\Jet/. 284: IOGI-lO(i5, 1971.
;ind l ia iuofsky, 1). :\.: 1)auiioiiiycin. an a i i t i t u n i o ~ an t i - botic, in the tic;itiiie~it o f iicoplastic disease. Curice) 2f1:533-353, 1967.
23. I\~alker, h l . I ) . , Roseiil)lum, hf. L., Sniitli, K. A , , a i i t l Re)noltls, A . I:.: The treatmeiit of b ra in tu i i i or w i t h 1 -(2-Cliloroetli~l)-3-C) cloliex) 1-1 -Nitrosiirea (CCStl) . Cnnrc? /<es. I2:51, l 9 i l .
21. \\'iernik, 1'. H., ai id Serpick, .A. A , : Factois cffect- iiig icmi\sion ant1 stirvital iii adul t acute Iioiilyriipho- cytic Iciihctiiia (ASLL) . Nediciiie 40:505-513, 1970.
-. 9 5 . - , ant1 ---: ;\ iantlomizetl cliirical tiial of dairnorubicin atid a coniIiinatiori of prediiisoiie, vincristiiie, 6-mci-captopurine, atid methotrexate in adul t acute iionlympliocytic leukemia. Cnpicer Re.,.
22. *rLill. c:., T M ~ X , H., YOII , K - P , R i t l y p i l y . hr. I,.,
32:2023-2026, 1972.