
HIE-Enabled Data Sharing Between Hospital and Home Care Providers to Improve Patient Care Within...
40
HIE-Enabled Data Sharing Between Hospital and Home Care Providers to Improve Patient Care Within Bundled Payment Context: a Case Study Katie Mullaly MS, RN NYULMC Amy Weiss PT, DPT VNSNY
-
Upload
new-york-ehealth-collaborative -
Category
Healthcare
-
view
2.166 -
download
2
Transcript of HIE-Enabled Data Sharing Between Hospital and Home Care Providers to Improve Patient Care Within...

HIE-Enabled Data Sharing Between Hospital and Home Care Providers to Improve Patient Care
Within Bundled Payment Context: a Case Study
Katie Mullaly MS, RN NYULMCAmy Weiss PT, DPT VNSNY
Agenda
1. About Visiting Nurse Service of New York 2. About NYU Langone Medical Center3. Bundled Payment for Care Improvement Initiative4. Evolution of Data Exchange5. Results6. Challenges to Date7. Closing Thoughts
Presentation Title Goes Here 2

VNSN
Y: T
rans
form
ing
Hom
e He
alth
care
for T
oday
’s N
eeds
VNSN
Y: T
rans
form
ing
Hom
e He
alth
care
for T
oday
’s N
eeds
• VNSNY is the largest not-for-profit home healthcare organization in the United States
• About 65,000 patients under direct or managed care on any given day– Care for more than 35,000 patients daily in all five New York City boroughs
plus Nassau, Suffolk and Westchester Counties– Manage the care of more than 30,000 VNSNY CHOICE Medicare and
Medicaid Health Plan members
• 17,000 employees including almost 2,000 Registered Nurses and Licensed Practical Nurses
• 2,276,690 total paraprofessional (clinical) visits in 2013• Clinical staff speak 50+ languages• The operational scale to successfully implement quality care
innovations across the care continuum
About VNSNY

Working on Your Own, You Cannot Achieve the Innovation Demanded in Today’s Healthcare
Environment
About VNSNY:Partnership as a Solution

Working in Partnership, We Can Innovate and Succeed!
About VNSNY:Partnership as a Solution

About VNSNY:Our Partners
Large Academic Medical Center
Integrated Delivery Systems
Teaching Hospital
Specialty Hospitals
National Disease Specific
Foundations
Sub-acute Care Facilities
Local Community
Hospital
Account Care Organizations
Federal + State Institutions
National + RegionalInsurance Providers
Physicians
Rehabilitation Centers

Proof of Concept Build Coalition Create Unified Programming
Create Clear Criteria for Success
About VNSNY:Partner Process
Needs Assessment
COLLABORATE1Partnering
ALIGN2Create Value
SOLVE3Evaluate
MEASURE4

NYULMC: ABOUT US

• An integrated academic medical center.• Comprised of four hospitals• 1,069 licensed beds• 39,000 patient admissions• 670,000 outpatient visits
NYU LANGONE MEDICAL CENTER NYU FACULTY GROUP PRACTICE & NYUPN, CLINICALLY INTEGRATED NETWORK
• Physician owned and operated NYUPN Clinically-Integrated Network, LLC comprised of:
• 800 voluntary physicians • 1400 Faculty Group Practice (FGP) physicians • 130,000 lives in commercial ACO contracts
• NYU FGP annual volume of patient visits is 2M
9

RECOGNIZED FOR CLINICAL EXCELLENCE AND QUALITY
10
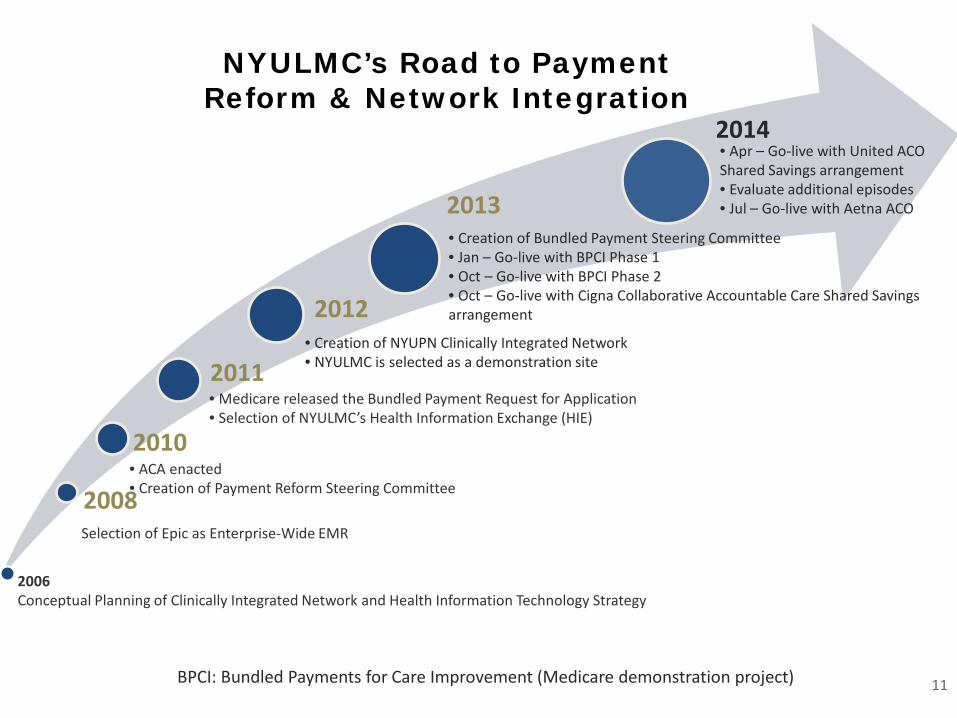
NYULMC’s Road to Payment Reform & Network Integration
2008
2010
2011
2012
2013
2006Conceptual Planning of Clinically Integrated Network and Health Information Technology Strategy
Selection of Epic as Enterprise-Wide EMR
• ACA enacted• Creation of Payment Reform Steering Committee
• Medicare released the Bundled Payment Request for Application• Selection of NYULMC’s Health Information Exchange (HIE)
• Creation of NYUPN Clinically Integrated Network• NYULMC is selected as a demonstration site
• Creation of Bundled Payment Steering Committee• Jan – Go-live with BPCI Phase 1• Oct – Go-live with BPCI Phase 2 • Oct – Go-live with Cigna Collaborative Accountable Care Shared Savings arrangement
BPCI: Bundled Payments for Care Improvement (Medicare demonstration project)
2014• Apr – Go-live with United ACO Shared Savings arrangement• Evaluate additional episodes• Jul – Go-live with Aetna ACO
11
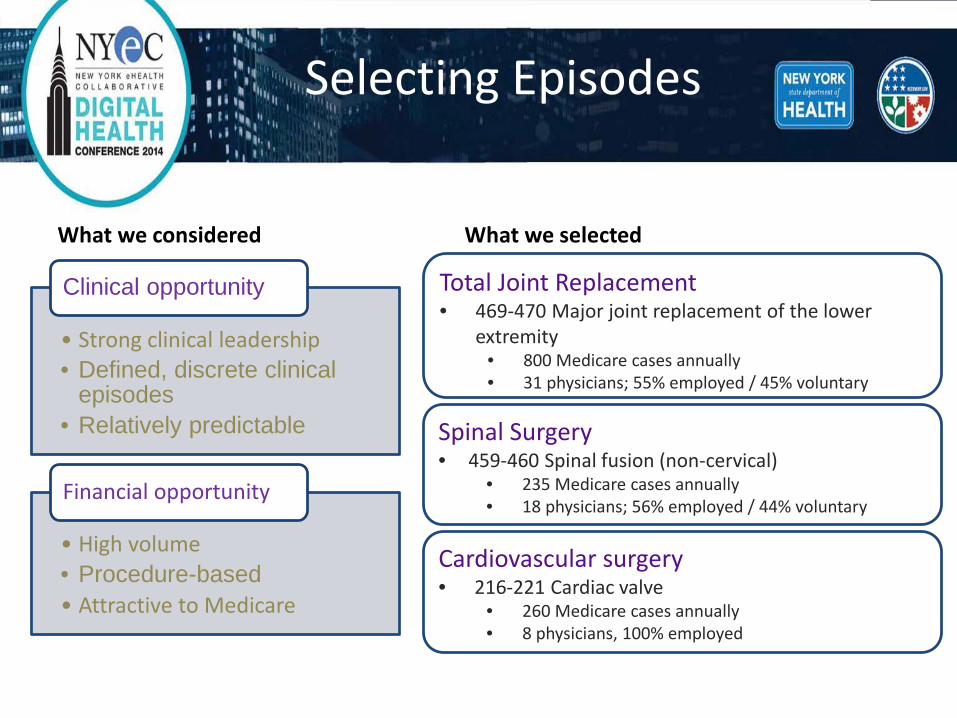
Selecting Episodes
What we considered
• Strong clinical leadership• Defined, discrete clinical
episodes• Relatively predictable
Clinical opportunity
• High volume• Procedure-based • Attractive to Medicare
Financial opportunity
Total Joint Replacement• 469-470 Major joint replacement of the lower
extremity• 800 Medicare cases annually• 31 physicians; 55% employed / 45% voluntary
Spinal Surgery• 459-460 Spinal fusion (non-cervical)
• 235 Medicare cases annually• 18 physicians; 56% employed / 44% voluntary
Cardiovascular surgery• 216-221 Cardiac valve
• 260 Medicare cases annually• 8 physicians, 100% employed
What we selected

1
Overview of Bundle Payment For Care Improvement Initiative

Medicare Bundled Payments for Care Improvement
• Payment for episode of care defined by hospital admission in select DRGs for Medicare FFS patients
• Four models1. Retrospective acute care hospital stay only 2. Retrospective acute care hospital + post acute care (30 or 90 days)3. Retrospective post-acute care only4. Prospective acute care only
• All providers paid traditional FFS rates
• Total Medicare cost for episode compared to historical baseline
• Savings go to provider organization after discount; provider repays if exceeds historical baseline
• Quality measures
CMS Demonstration for Episode Based Payment Models
14

What is Included in the Model 2 Target Price?
Home Health Agencies
Outpatient Therapy Services
Skilled Nursing Facilities & LTACH
Inpatient Rehab
Hospital
Surgeon
Physician Visits (surgeon and other)
Any services during the 90-Day Post-Acute Period
such as…
Consulting Physicians
Readmissions (to NYU or others)
DMEPart B Drugs Outpatient Services
Lab Services
Anesthesiologist
Any services during the Acute Staysuch as…
Any services that roll into the Index Admission through the current IPPS 72-hour rule such as…
ED Visits
Days 91-120
CMS will be monitoring the period immediately following to ensure that services are not being shifted outside the bundle.
NYUHC will be financially responsible if such behavior is observed and may be removed from the program.
15

Post Acute Goal – Improved Outcomes and Patient Experience NYULMC Post-Acute Partners
Home Health Facilities1. Visiting Nurse Service of New York Home Care CHHA2. Village Center for Care CHHA3. Revival Home Health Care4. Jewish Home Lifecare Long Term Home Health Care
Skilled Nursing Facilities1. Village Center for Care, Manhattan2. Gouverneur Healthcare Services, SNF, Manhattan3. Jewish Home Lifecare, Manhattan, Bronx, Westchester4. Mary Manning Walsh, Manhattan5. Terence Cardinal Cooke, Manhattan6. Haym Salomon Home for the Aged, Brooklyn7. Cobble Hill Health Center, Brooklyn8. Clove Lakes Rehabilitation Center, Staten Island9. Trump Pavilion for Nurse Rehab at Jamaica Hospital, Queens
NYULMC clinicians and staff selected facilities based on a set of rigorous quality and care coordination criteria, taking into account existing clinical relationships, patient geography, and physician discharging preferences.
16
Episodes of Care InitiativeWays to Improve Quality and Efficiency
• Reduce readmissions • Reduce LOS• Reduce implant, supply, or drug costs• Reduce OR time • Alter discharge patterns to more cost-efficient settings• Decrease excess utilization (e.g., consults, ancillary tests)
Quality improvements and efficiencies will benefit all patients, regardless of payor.
17

Staffing
Care Coordination Staffing – Dedicated to Bundled Payment• Clinical Care Coordinators (CCC) are the “General Manager” of the 90-day episode
• Help answer questions and facilitate communication with providers• Receive regular updates on patient progress• Help ensure follow-up visits with surgeon and PCPs
• 5 RN FTE Clinical Care Coordinators manage 1,200 patients • Preoperatively 1 CCC : 20-25 patients • Inpatient 1 CCC : 4-6 patients • 90-days post-discharge 1 CCC : 50-60 patients • Annual staffing ratio 1 CCC : 240 patients
Program Staffing – Support all Population Management Initiatives• The Network Integration and Payment Reform team consists of:
• MD Executive Sponsor • RN Senior Director of Clinical Operations• RN Director of Clinical Care Coordination • RN Manager of Clinical Care Coordination• Director of Program Implementation• Manager of Payment Reform• Data Analyst(s)• Project Manager(s)• Project Assistant(s)
18

TJR Pathway Development Governance Structure
Implementation
MCIT Reporting
Epic Workflow
Bundled Payment Initiative Steering
Committee
Pre-hospital Team Inpatient Team Post Acute Team
Total Joint Care Pathway Committee
19
Standardization
• Systematization and standardizing are the foundations of good operational routines that can be measured and facilitate improvements, outcomes, and ever-greater efficiency.
Advantages of Standardization1. Increased efficiency 2. Improved ability to monitor and study
individual factors3. Improved communication4. It allows for identification of outliers or
modifiable factors
20
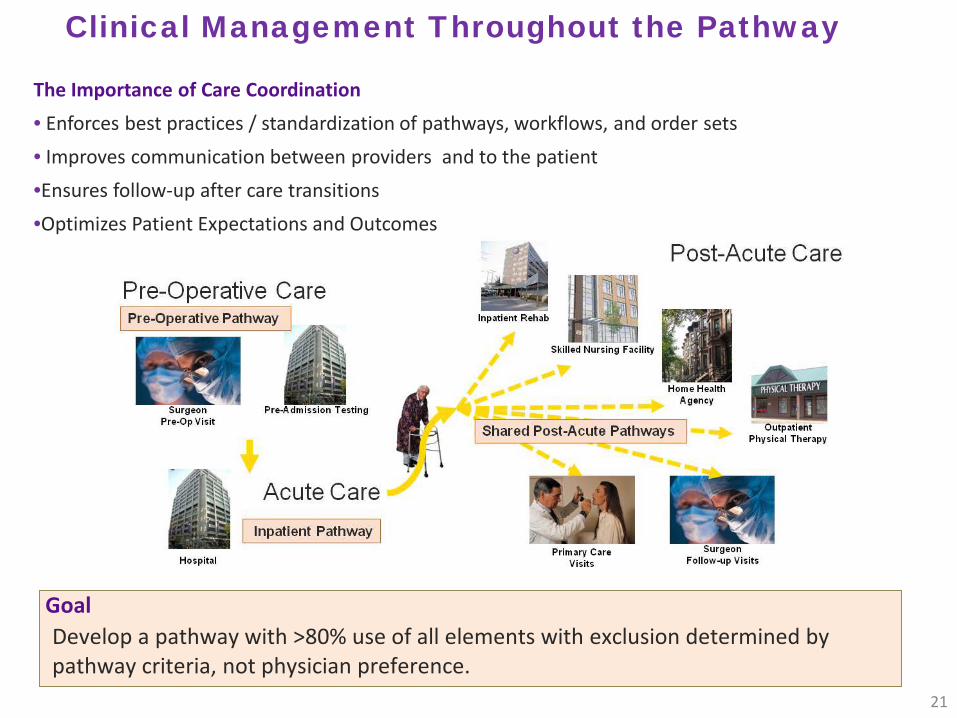
Clinical Management Throughout the Pathway
The Importance of Care Coordination • Enforces best practices / standardization of pathways, workflows, and order sets• Improves communication between providers and to the patient•Ensures follow-up after care transitions•Optimizes Patient Expectations and Outcomes
GoalDevelop a pathway with >80% use of all elements with exclusion determined by pathway criteria, not physician preference.
21
Inpatient WorkflowGoal – Standard Pathway with > 80% agreement

Confidential. Do not Distribute. 23
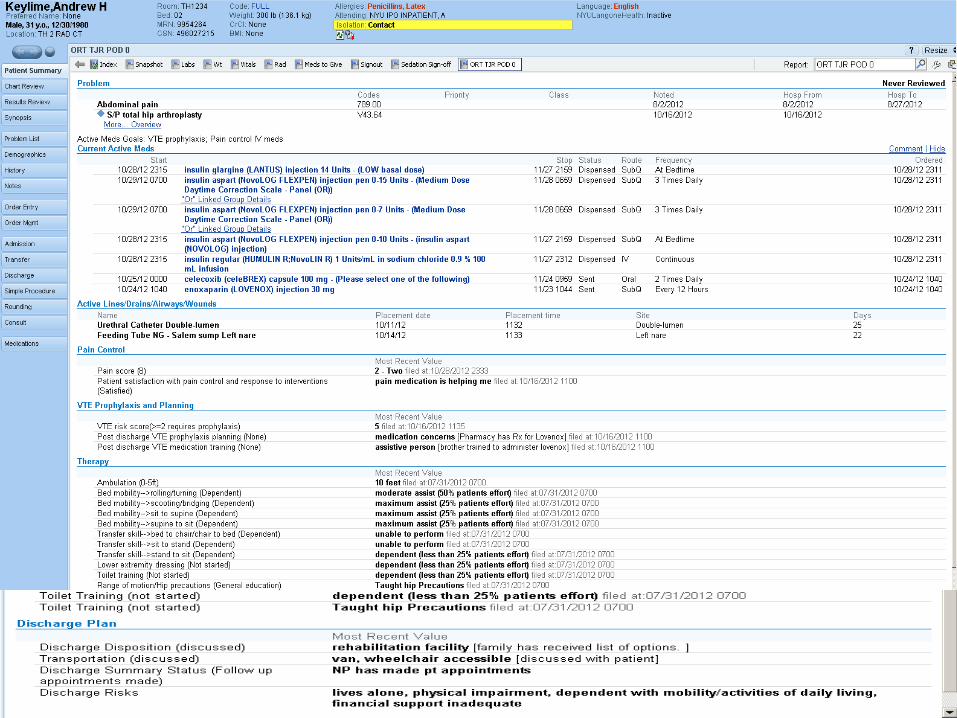
EMR care coordination tools and patient registries• Care coordination tools were built into the EMR so that Clinical Care Coordinators could see their
daily patient lists, view the 90-day longitudinal plan of care as well as document all notes, including information from patients, post-acute providers, and readmissions back to NYULMC and to other hospitals

Home Care Post-Acute Pathway
• Two Home Care Pathways– Standard Pathway– Enhanced Support Pathway
• VNSNY/TJR Enhanced Support Pathway Pilot Criteria – Single Joint replacement– Caregiver able to participate in therapy prior to DC– Stairs before discharge / No more that 1 flight in home– If private home bed/bath cant be longer than a flight of stairs– Eligible for SNF / Complex Needs
• Established risk profile to assist in determining appropriate disposition.
• Focus on bi-directional electronic exchange of information.24
1
EvolutionTransition of Care Communication Tool

Redesigning CareStrategy to Improve Care Transitions
The goal: To improve the communication, quality, safety and patient experience across the care continuum.
Transitional Care Communication ToolNYULMC in collaboration with partners developed a new electronic communication tool leveraging our (HIE) provide a seamless transfer of clinical data between providers caring for the patient at the time of discharge and throughout the post-acute period.
Critical to our success was an effective care transition intervention that reduces fragmentation of care delivery across an episode of care.
26

•NYULMC’s Health Information Exchange
•Allows care team to review clinical results/notes of other facilities and physicians
•“EMR Light” allows for enhanced communication with post-acute care providers through the use of an electronic transitional care communication tool. The tool consists of:
• Transfer Document: Completed by a NYULMC Clinical Care Coordinator upon hospital discharge and made available to the post-acute provider through EMR Light. Includes information such as demographics, type of surgery, care pathway, most recent clinical status, and Clinical Care Coordinator contact information.
• Follow-up Form: Sent from the post-acute provider to NYULMC as a patient progress report. Includes information such as post-acute length of stay, changes in clinical condition, physician / nurse practitioner evaluations, and medication changes.
• Continuity of Care Document: The post-acute provider can also access the patient’s Continuity of Care Document that is generated by NYULMC’s electronic health record. The document is an electronic patient summary containing a set of standardized clinical elements that are most relevant during care transitions. These elements include allergies, medications, problem list, procedures, and results.
Transitional Care Communication Tool Strategy
27
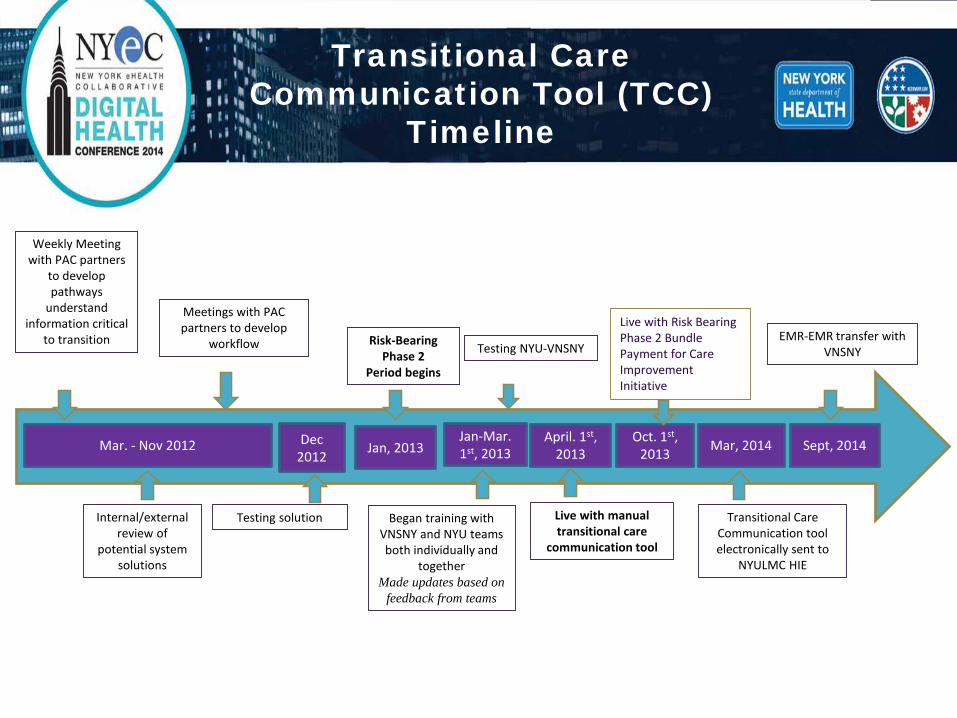
Jan-Mar. 1st, 2013
Weekly Meeting with PAC partners
to develop pathways
understand information critical
to transitionTesting NYU-VNSNY
Mar. - Nov 2012 April. 1st, 2013 Sept, 2014
EMR-EMR transfer with VNSNY
Risk-Bearing Phase 2
Period begins
Oct. 1st, 2013
Live with manual transitional care
communication tool
Mar, 2014
Transitional Care Communication tool electronically sent to
NYULMC HIE
Internal/external review of
potential system solutions
Meetings with PAC partners to develop
workflow
Testing solution
Dec 2012 Jan, 2013
Began training with VNSNY and NYU teams both individually and
together Made updates based on
feedback from teams
Live with Risk Bearing Phase 2 Bundle Payment for Care Improvement Initiative
Transitional Care Communication Tool (TCC)
Timeline

Components of TCC Forms- CHHA/SNF
Transfer Document (Discharge)
•Demographics•Type of surgery, date, •Care Pathway•Readmission Risk•Clinical Status •Functional Status •Patient Preferences/Comments •Social History •Knowledge Deficit•Follow-up Appointments •Hospital Contact Information•VS/Smoking Status•Education •+CCD
Follow-up Form (weekly)Clinical Status• Pain• VTE pro• Surgical Wound• Pressure Ulcer• UTI• Fever• Diet• Any new medications added • Change in clinical condition • Evaluated by MD/NPFunctional Status• Number of PT/OT visits week• Ambulation• Stairs• Transfers • FallsDischarge Status• Anticipated Discharge Date• Barriers to Discharge• Patient on target for Discharge
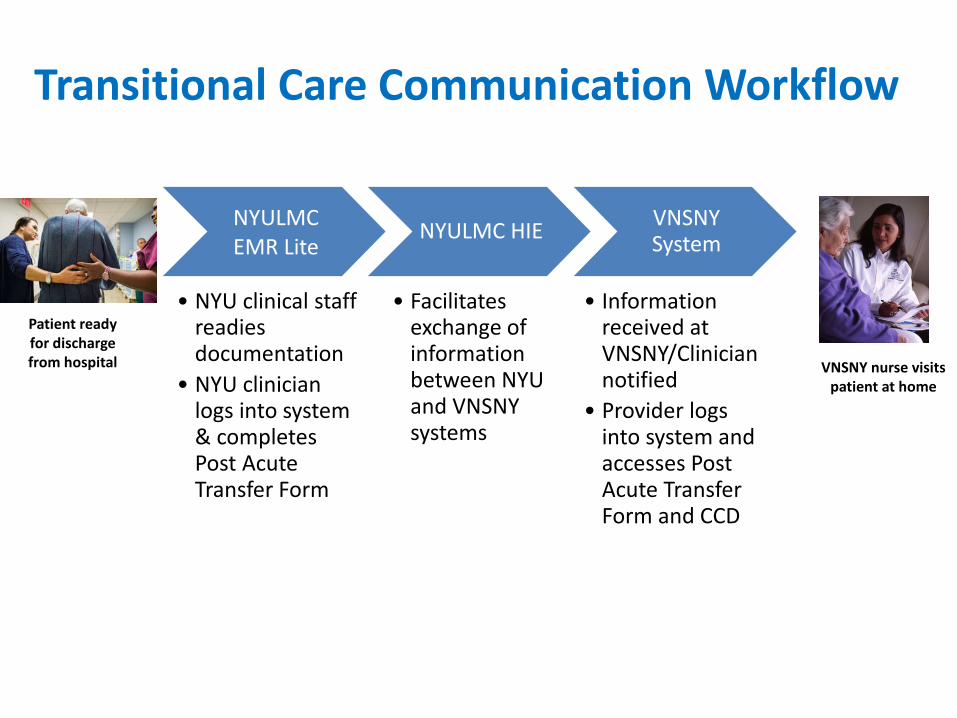
NYULMC EMR Lite
• NYU clinical staff readies documentation
• NYU clinician logs into system & completes Post Acute Transfer Form
NYULMC HIE
• Facilitates exchange of information between NYU and VNSNY systems
VNSNY System
• Information received at VNSNY/Clinician notified
• Provider logs into system and accesses Post Acute Transfer Form and CCD
Transitional Care Communication Workflow
Patient readyfor discharge from hospital VNSNY nurse visits
patient at home

Transitional Care Communication Tool
Progression
• To date we have sent exchanged over 4,000 forms – Approximately 2000 forms with VNSNY
April 1 2013 Manual
March 2014VNSNY EMR to NYULMC HIE
September 2014EMR-EMR
31

Implementing TCC ToolSteps to Success
• Foundational work on pathways assisted in identifying areas of focus
• Weekly NYULMC-VNSNY Joint IT Operations meetings • NYULMC-VNSNY Training • Continuous updates to improve the functionality of the
tool
32

NYULMC-VNSNY HIE:Real World Application
• 80 year old female, s/p cardiac valve repair• Discharged home after 5 day hospital stay• Transfer form sent from NYULMC to VNSNY upon transition• Weekly follow-up form sent from VNSNY to NYULMC• NYULMC RN Clinical Care Coordinator observed improved BP
control, prompting discussion of medication titration• Patient weaned off of BP meds with ongoing assessment of
VNSNY RN• Overall medication adherence improved, BP meds and diuretics
adjusted appropriately for optimal fluid management• Patient remained in community, with no readmission during
bundled episode

Staff Feedback
• “It’s my eyes and ears telling me how the patient is doing at home”
• “It makes our communication more meaningful-instead of reporting vitals and other measurements, we spend our time talking about what we are going to do about the biometric trends we have both been monitoring.”
• “The data exchange helps to make the VNSNY home care RN and the NYULMC Clinical Care Coordinator a unified team, both working with the patient to address the key issues and address the patient’s goals.”
1
Results

Changing care delivery while improving quality
n=LOS:
5075.62
6804.27
6733.84
1206.46
2114.58
1674.67
18711.81
2539.82
1789.27
8193.49
1784.83
2538.70
Discharge Disposition Patterns
Based on NYULMC internal data and Medicare claims dataFY 2014: Sept.1, 2013 - Aug. 31, 2014 36

Changing care delivery while improving quality
Data based on Medicare claims data for bundled payment admissions
90-day all-cause readmission rates
37

Challenges & Next Steps
• Challenges:– HIE Access and Patient Consent– Mapping discrete data – Patient Matching
• Next Steps – Continual Improvement of Provider Communication
• Order sets• Texting
38

Closing Thoughts
• Our patients are experiencing improved care through enhanced coordination and communication between providers
• Well-coordinated care is better for our patients and results in reduced costs
• Providing information and education to providers across the spectrum, combined with the financial mechanisms to align incentives, is a powerful combination
• Strategic design and implementation of IT infrastructure is a foundation for success
39

Questions?
40


















