
HEV Related Neuro-chr Hep 2010-Fr
4
American Journal of Transplantation 2010; 10: 1321–1324 Wiley Periodicals Inc. C 2010 The Author s Journa l compilation C 2010 The American Society of Tra nsplantatio n and the American Society of Tra nsplant Surgeons doi: 10.1111/j.160 0-6143.2010.030 68.x Case Report Hepatitis E Virus-Induced Neurological Symptoms in a Kidney-Transplant Patient with Chronic Hepatitis N. Kamar a,b, * , J. Izopet c,d , P. Cintas e , C. Garrouste a,d , E. Uro-Coste f , O. Cointault a , L. Rostaing a,d a Department of Nephrology, Dialysis and Organ Transplantation, b INSERM U858, IFR-BMT, c Department of Virology, d INSERM U563, IFR-BMT, e Department of Neurology and f Department of Pathology, CHU Rangueil, Toulouse, France * Corresponding author: Nassim Kamar, [email protected] It has been shown that hepatitis E virus (HEV) may be responsible for chronic hepatitis in solid-organ trans- plant patients. It has also been suggested that HEV may be res ponsi ble for atypical neur ologi cal symp - toms during the acute phase. However, the relation- ship between the neurological symptoms and HEV in- fection was based on the detection of anti-HEV IgM in the sera. Herein, we report a case where neurolog- ical symptoms, that is peripheral nerve involvement with pro xima l muscular weakness that affecte d the four limbs joints with central nervous-system involve- ment and bilateral pyramidal syndrome, occurred in a kidne y-t ran splan t pati ent who was chr onica lly in- fected by HEV. For the first time, HEV RNA was de- tected in the ser um and cer ebrospinal flui d. In addition, clonal HEV sequences were analyzed in both compart- ments, that is serum and cerebrospinal fluid. The dis- covery of quasispecies compartmentalization and its tempor al association sugg ests that neur olog ical symp - toms could be linked to the emergence of neurotropic variants. Key words: Cerebr ospinal fluid, chronic hepatit is, hep- atitis E vir us,neurologicalsymptoms,org an-tr ansplant patients, quasispecies Received 19 November 2009, revised 07 January 2010 and accepted for publication 21 January 2010 Introduction Hepat iti s E vir us (HE V) is a well- kno wn cause of acu te hepatitis (1). Recently, it has been shown that it is also re- sponsible for chronic hepatitis that can evolve to cirrhosis (2). It has also been suggested that HEV may be responsi- ble for an extra-hepatic manifestations, that is neurological symptoms. Indeed, neurological manifestations, such as Guillain–Barr´ e syndrome, neuralgic amyotrophy or acute transverse myelitis, have been previously reported to be associated with acute HEV-infection (3–7). Herein, we re- port on a case where neurological symptoms occurred in a kidney-transplant patient who was chronically infected by HEV, and in whom, for the first time, HEV RNA was de- tected and characterized in the serum and cerebrospinal fluid (CSF). Case Report A 44-y ear -old kidne y-tr anspla nt patie nt prese nted at 50 months posttransplant with an acute autochthonous HEV inf ectio n that evolve d to ch ronici ty . At HEV infecti on di- agnosis, hepatitis C virus (HCV), hepatitis B virus (HBV) human-immunodeficiency virus (HIV) and hepatitis E virus (HEV) serologies, hepatitis A virus (HAV) IgM, as well as HCV RNA, HB V DNA and HI V RNA, which were all negati ve at transplantation, were still negative. There was no evi- dence of cytomegalovirus (CMV), Epstein Barr virus (EBV) and herpes simplex virus (HSV) infections. Antinuclear au- toantibodies (ANA), anti-liver-kidney microsomal (LKM) an- tibod ies, anti- smoot h-mu scle cell (SMC) antib odies and an- timit oc hondr ial antib odies were not detec ted. EB V DNA concentration in the blood was unchanged as compared to 4 months before the acute hepatitis episod, for example 4.3 log 10 copies/mL. Biliary-tract complications were ruled out by abdominal ultrasonography. Toxin- and drug-related causes of abnormal liver-function tests were ruled out by anamnesis. In contrast, HEV RNA was found to be posi- tive in the serum and the stools. Phylogenetic analysis of HEV RNA revealed that the strain belonged to genotype 3f (Genbank number FJ665423). By 6 months later, liver enzymes were still elevated HEV RNA was still detected in the serum and the stools, and anti-HEV IgG was posi- tive. By 33 months after the acute phase, he was admitted for progressive bilateral muscular weakness, difficulties in walking and palmar and plantar dysesthesia without evi- dence of systemic infection. The patient had no signs of meningeal infection, no fever and no biological markers of inflammati on (white blood cell counts were 5700/mm 3 with 82% polymorphonuclear cells, C-reactive protein was <2 mg/L). He was receiving tacrolimus (trough level of 1321
Transcript of HEV Related Neuro-chr Hep 2010-Fr
8/9/2019 HEV Related Neuro-chr Hep 2010-Fr
http://slidepdf.com/reader/full/hev-related-neuro-chr-hep-2010-fr 1/4
American Journal of Transplantation 2010; 10: 1321–1324Wiley Periodicals Inc.
C 2010 The Authors Journal compilation C 2010 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2010.03068.xCase Report
Hepatitis E Virus-Induced NeurologicalSymptoms in a Kidney-Transplant Patient
with Chronic Hepatitis
N. Kamara,b,*, J. Izopetc,d, P. Cintase,C. Garroustea,d, E. Uro-Costef, O. Cointaulta,L. Rostainga,d
aDepartment of Nephrology, Dialysis and OrganTransplantation, bINSERM U858, IFR-BMT, cDepartment of Virology, dINSERM U563, IFR-BMT, eDepartment of Neurology and fDepartment of Pathology, CHU Rangueil,Toulouse, France *Corresponding author: Nassim Kamar,
It has been shown that hepatitis E virus (HEV) may beresponsible for chronic hepatitis in solid-organ trans-plant patients. It has also been suggested that HEVmay be responsible for atypical neurological symp-toms during the acute phase. However, the relation-ship between the neurological symptoms and HEV in-fection was based on the detection of anti-HEV IgMin the sera. Herein, we report a case where neurolog-ical symptoms, that is peripheral nerve involvementwith proximal muscular weakness that affected thefour limbs joints with central nervous-system involve-ment and bilateral pyramidal syndrome, occurred ina kidney-transplant patient who was chronically in-
fected by HEV. For the first time, HEV RNA was de-tected in the serum and cerebrospinal fluid. In addition,clonal HEV sequences were analyzed in both compart-ments, that is serum and cerebrospinal fluid. The dis-covery of quasispecies compartmentalization and itstemporal association suggests that neurological symp-toms could be linked to the emergence of neurotropicvariants.
Key words: Cerebrospinal fluid, chronic hepatitis, hep-atitis E virus, neurological symptoms, organ-transplantpatients, quasispecies
Received 19 November 2009, revised 07 January 2010and accepted for publication 21 January 2010
Introduction
Hepatitis E virus (HEV) is a well-known cause of acute
hepatitis (1). Recently, it has been shown that it is also re-
sponsible for chronic hepatitis that can evolve to cirrhosis
(2). It has also been suggested that HEV may be responsi-
ble for an extra-hepatic manifestations, that is neurological
symptoms. Indeed, neurological manifestations, such as
Guillain–Barre syndrome, neuralgic amyotrophy or acute
transverse myelitis, have been previously reported to be
associated with acute HEV-infection (3–7). Herein, we re-
port on a case where neurological symptoms occurred in a
kidney-transplant patient who was chronically infected by
HEV, and in whom, for the first time, HEV RNA was de-
tected and characterized in the serum and cerebrospinal
fluid (CSF).
Case Report
A 44-year-old kidney-transplant patient presented at 50
months posttransplant with an acute autochthonous HEV
infection that evolved to chronicity. At HEV infection di-
agnosis, hepatitis C virus (HCV), hepatitis B virus (HBV)
human-immunodeficiency virus (HIV) and hepatitis E virus
(HEV) serologies, hepatitis A virus (HAV) IgM, as well as
HCV RNA, HBV DNA and HIV RNA, which were all negative
at transplantation, were still negative. There was no evi-
dence of cytomegalovirus (CMV), Epstein Barr virus (EBV)
and herpes simplex virus (HSV) infections. Antinuclear au-toantibodies (ANA), anti-liver-kidney microsomal (LKM) an-
tibodies, anti-smooth-muscle cell (SMC) antibodies and an-
timitochondrial antibodies were not detected. EBV DNA
concentration in the blood was unchanged as compared to
4 months before the acute hepatitis episod, for example
4.3 log10 copies/mL. Biliary-tract complications were ruled
out by abdominal ultrasonography. Toxin- and drug-related
causes of abnormal liver-function tests were ruled out by
anamnesis. In contrast, HEV RNA was found to be posi-
tive in the serum and the stools. Phylogenetic analysis of
HEV RNA revealed that the strain belonged to genotype
3f (Genbank number FJ665423). By 6 months later, liver
enzymes were still elevated HEV RNA was still detected
in the serum and the stools, and anti-HEV IgG was posi-
tive. By 33 months after the acute phase, he was admitted
for progressive bilateral muscular weakness, difficulties in
walking and palmar and plantar dysesthesia without evi-
dence of systemic infection. The patient had no signs of
meningeal infection, no fever and no biological markers
of inflammation (white blood cell counts were 5700/mm3
with 82% polymorphonuclear cells, C-reactive protein was
<2 mg/L). He was receiving tacrolimus (trough level of
1321
8/9/2019 HEV Related Neuro-chr Hep 2010-Fr
http://slidepdf.com/reader/full/hev-related-neuro-chr-hep-2010-fr 2/4
Kamar et al.
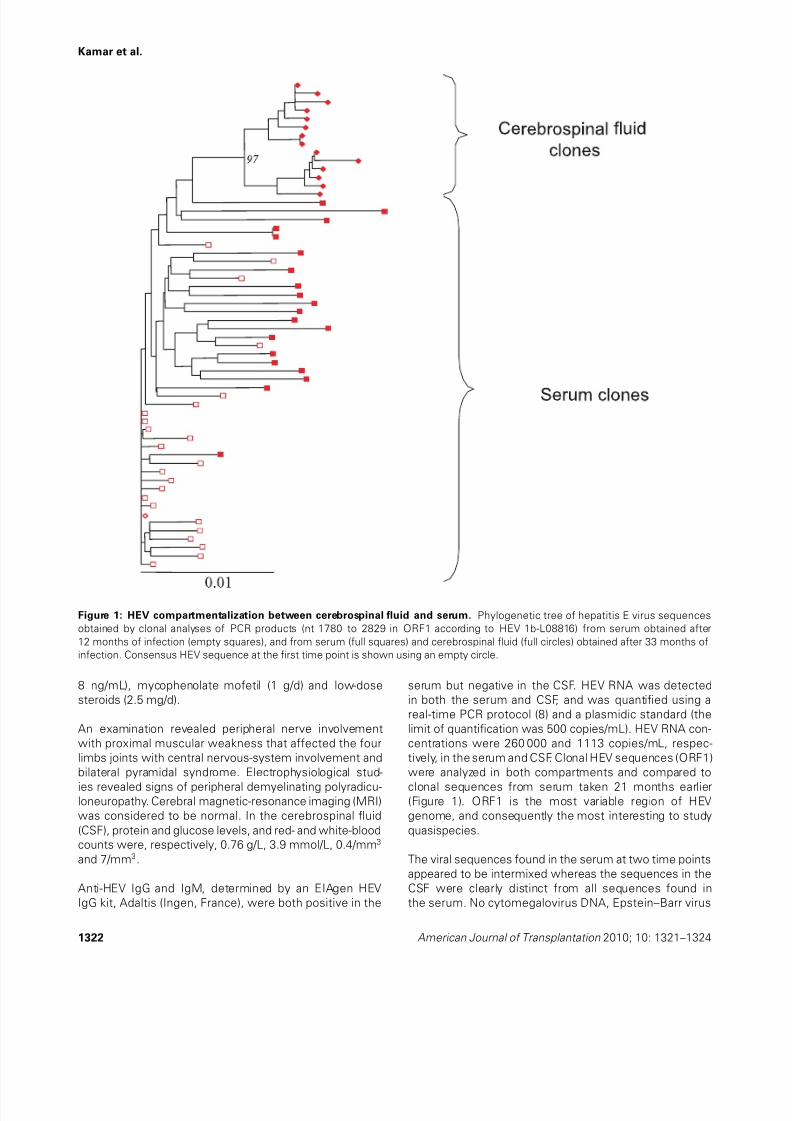
Figure 1: HEV compartmentalization between cerebrospinal fluid and serum. Phylogenetic tree of hepatitis E virus sequences
obtained by clonal analyses of PCR products (nt 1780 to 2829 in ORF1 according to HEV 1b-L08816) from serum obtained after
12 months of infection (empty squares), and from serum (full squares) and cerebrospinal fluid (full circles) obtained after 33 months of
infection. Consensus HEV sequence at the first time point is shown using an empty circle.
8 ng/mL), mycophenolate mofetil (1 g/d) and low-dose
steroids (2.5 mg/d).
An examination revealed peripheral nerve involvement
with proximal muscular weakness that affected the four
limbs joints with central nervous-system involvement and
bilateral pyramidal syndrome. Electrophysiological stud-
ies revealed signs of peripheral demyelinating polyradicu-loneuropathy. Cerebral magnetic-resonance imaging (MRI)
was considered to be normal. In the cerebrospinal fluid
(CSF), protein and glucose levels, and red- and white-blood
counts were, respectively, 0.76 g/L, 3.9 mmol/L, 0.4/mm3
and 7/mm3.
Anti-HEV IgG and IgM, determined by an EIAgen HEV
IgG kit, Adaltis (Ingen, France), were both positive in the
serum but negative in the CSF. HEV RNA was detected
in both the serum and CSF, and was quantified using a
real-time PCR protocol (8) and a plasmidic standard (the
limit of quantification was 500 copies/mL). HEV RNA con-
centrations were 260 000 and 1113 copies/mL, respec-
tively, in the serum and CSF. Clonal HEV sequences (ORF1)
were analyzed in both compartments and compared to
clonal sequences from serum taken 21 months earlier(Figure 1). ORF1 is the most variable region of HEV
genome, and consequently the most interesting to study
quasispecies.
The viral sequences found in the serum at two time points
appeared to be intermixed whereas the sequences in the
CSF were clearly distinct from all sequences found in
the serum. No cytomegalovirus DNA, Epstein–Barr virus
1322 American Journal of Transplantation 2010; 10: 1321–1324

8/9/2019 HEV Related Neuro-chr Hep 2010-Fr
http://slidepdf.com/reader/full/hev-related-neuro-chr-hep-2010-fr 3/4
HEV-Induced Neurological Symptoms
DNA, Herpes simplex 1 and 2 DNA, Varicella Zoster virus
DNA, JC virus DNA, cryptococcal antigen, Toxoplasma
gondii DNA or Candida was detected in the CSF. Stan-
dard cultures of CSF remained negative. Serum HCV, HBV
and HIV serologies, as well as HCV RNA, HBV DNA,
HIV RNA and CMV DNA were still negative. EBV DNA
concentration in the blood was unchanged at 4.4 log10
copies/mL. Alanine aminotransferase level was 105 IU/L.
A liver biopsy showed the presence of cirrhosis with aMetavir score of A2F4. Serum CD4-positive cell count was
167/mm3. Antigangliosides 1A (titer 125) and anticytoplas-
mic nuclear (titer 100) antibodies were found to be pos-
itive in the serum. The CSF to serum–albumin ratio was
12.26. The CSF (IgG:albumin) to serum (IgG:albumin) ratio
was 0.54.
Three months later, because of severe ataxia, and loss of
bladder and bowel sensations, he underwent a neuromus-
cular biopsy. This showed nonspecific signs of neurogenic
muscular atrophy without signs of vasculitis on both mus-
cular and nerve specimens. Consequently, tacrolimus dose
was significantly reduced to target a trough level of 2.5
ng/mL and intravenous immunoglobulins were adminis-
trated (0.4 g/kg/d for 5 days, total dose 2 g/kg). However, no
significant improvement was observed. One month later,
he presented with decompensated cirrhosis and deceased
from hemorrhagic shock.
Discussion
HEV infection is an emerging disease in industrialized coun-
tries. Initially, it was thought to only be responsible for
acute hepatitis. However, HEV has been recently shown
to lead to chronic hepatitis in solid-organ transplants (SOT)
(2,9), and in HIV (10) and hematological patients (11).Scarce case reports suggest that HEV may be responsi-
ble for atypical neurological symptoms.
To date, three cases of Guillain–Barre syndrome associated
with an acute HEV episode have been reported (3,5,4).
Mandal and Chopra reported a case of acute transverse
myelitis following HEV infection (7). More recently, Fong
and Illahi reported a case of neuralgic amyotrophy, also
called Parsonage–Turner syndrome, associated with HEV
(6). In all these cases, the relationship between the neu-
rological symptoms and HEV infection was based on the
detection of anti-HEV IgM in the sera. However, HEV RNA
was not looked for in either the sera or CSF.
Herein, we report for the first time that HEV RNA can be
detected in the CSF of a patient with chronic HEV infection,
and can be responsible for atypical neurological symptoms.
In addition, for the first time, clonal HEV sequences were
analyzed in both compartments, that is serum and CSF.
The discovery of quasispecies compartmentalization and
its temporal association suggests that neurological symp-
toms could be linked to the emergence of neurotropic vari-
ants. However, we can exclude that small amount of HEV
RNA entered the CSF due to a problem in the brain–blood
barrier and that the evolution of HEVquasispecies occurred
later on.
Infections may lead to neurological manifestations through
an autoimmune-mediated process. Autoimmune dysfunc-
tion can occur in chronic active hepatitis, such as hepatitis
C virus or hepatitis B virus infection. Interestingly, antigan-gliosides 1A and anticytoplasmic nuclear antibodies were
found to be positive in the serum of our patient, suggest-
ing that chronic HEV infection may also induce an autoim-
mune dysfunction. In the case of Guillain–Barre syndrome
associated with HEV infection, as reported by Lolly et al.
(5), serum antiganglioside antibodies can also be positive.
However, the mechanism by which antiganglioside anti-
bodies may induce neurological symptoms in the setting
of HEV infection remains unknown. Thus, further studies
are required to document the relationship between HEV-
induced neurological symptoms and the detection of anti-
ganglioside antibodies.
Unfortunately, in the present case, the use of intravenous
immunoglobulin associated with immunosuppressant-
dose reduction did not result in improved neurological
symptoms. However, in liver-transplant patients chroni-
cally infected by HEV, we have recently shown that 3
months of pegylated-interferon therapy may effectively
clear this virus (12). Thus, the use of interferon-a in the set-
ting of HEV-induced neurological symptoms needs to be
evaluated.
Conclusion
In patients with elevated liver enzymes or with a knownHEV infection, and who present with neurological symp-toms, HEV RNA should be looked for in the serum andCSF.
References
1. Dalton HR, Bendall R, Ijaz S, Banks M. Hepatitis E: An emerging
infection in developed countries. Lancet Infect Dis 2008; 8: 698–
709.
2. Kamar N, Selves J, Mansuy JM et al. Hepatitis E virus and chronic
hepatitis in organ-transplant recipients. N Engl J Med 2008; 358:
811–817.
3. Kamani P, Baijal R, Amarapurkar D et al. Guillain-Barre syndrome
associatedwith acute hepatitis E. Indian J Gastroenterol 2005; 24:216.
4. Sood A, Midha V, Sood N. Guillain-Barre syndrome with acute
hepatitis E. Am J Gastroenterol 2000; 95: 3667–3668.
5. Loly JP, Rikir E, Seivert M et al. Guillain-Barre syndrome following
hepatitis E. World J Gastroenterol 2009; 15: 1645–1647.
6. Fong F, Illahi M. Neuralgic amyotrophy associated with hepatitis E
virus. Clin Neurol Neurosurg 2009; 111: 193–195.
7. Mandal K, Chopra N. Acute transverse myelitis following hepatitis
E virus infection. Indian Pediatr 2006; 43: 365–366.
American Journal of Transplantation 2010; 10: 1321–1324 1323

8/9/2019 HEV Related Neuro-chr Hep 2010-Fr
http://slidepdf.com/reader/full/hev-related-neuro-chr-hep-2010-fr 4/4
Kamar et al.
8. Mansuy JM, Peron JM, Abravanel F et al. Hepatitis E in
the south west of France in individuals who have never
visited an endemic area. J Med Virol 2004; 74: 419–
424.
9. Gerolami R, Moal V, Picard C, Colson P. Hepatitis E virus as an
emerging cause of chronic liver disease in organ transplant recipi-
ents. J Hepatol 2009; 50: 622–624.
10. DaltonHR, Bendall R, Keane F, Tedder R, Ijaz S. Persistentcarriage
of hepatitis E virus in patients with HIV infection. N Engl J Med
2009; 361: 1025–1027.
11. Ollier L, Tieulie N, Sanderson F et al. Chronic hepatitis after hep-
atitis E virus infection in a patient with non-Hodgkin lymphoma
taking rituximab. Ann Intern Med 2009; 150: 430–431.
12. Kamar N, Rostaing L, Abravanel F et al. Pegylated alpha-interferon
for treating chronic hepatitis E virus infection after liver transplan-
tation. Clin Infect Dis 2010; 50: e30–e33.
1324 American Journal of Transplantation 2010; 10: 1321–1324


















