
Hépatite C chronique - afphb.be · 18/06/2018 3 Histologic Progression of liver disease Normal...
25
18/06/2018 1 Hépatite C chronique Professeur Christophe Moreno Directeur clinique Hépatologie, Hôpital Erasme Président BASL [email protected] Tel: 02/5553714 1 MALADIE CHRONIQUE DU FOIE 2 = Destruction et régénération progressive du parenchyme hépatique, menant à la fibrose hépatique (et éventuellement à la cirrhose et ses complications) Hépatite = inflammation du foie
Transcript of Hépatite C chronique - afphb.be · 18/06/2018 3 Histologic Progression of liver disease Normal...

18/06/2018
1
Hépatite C chronique
Professeur Christophe Moreno
Directeur clinique Hépatologie, Hôpital Erasme
Président BASL
[email protected]: 02/5553714
1
MALADIE CHRONIQUE DU FOIE
2
= Destruction et régénération progressive du parenchyme hépatique, menant à la fibrose hépatique (et éventuellement à la cirrhose et ses complications)
Hépatite = inflammation du foie
18/06/2018
2
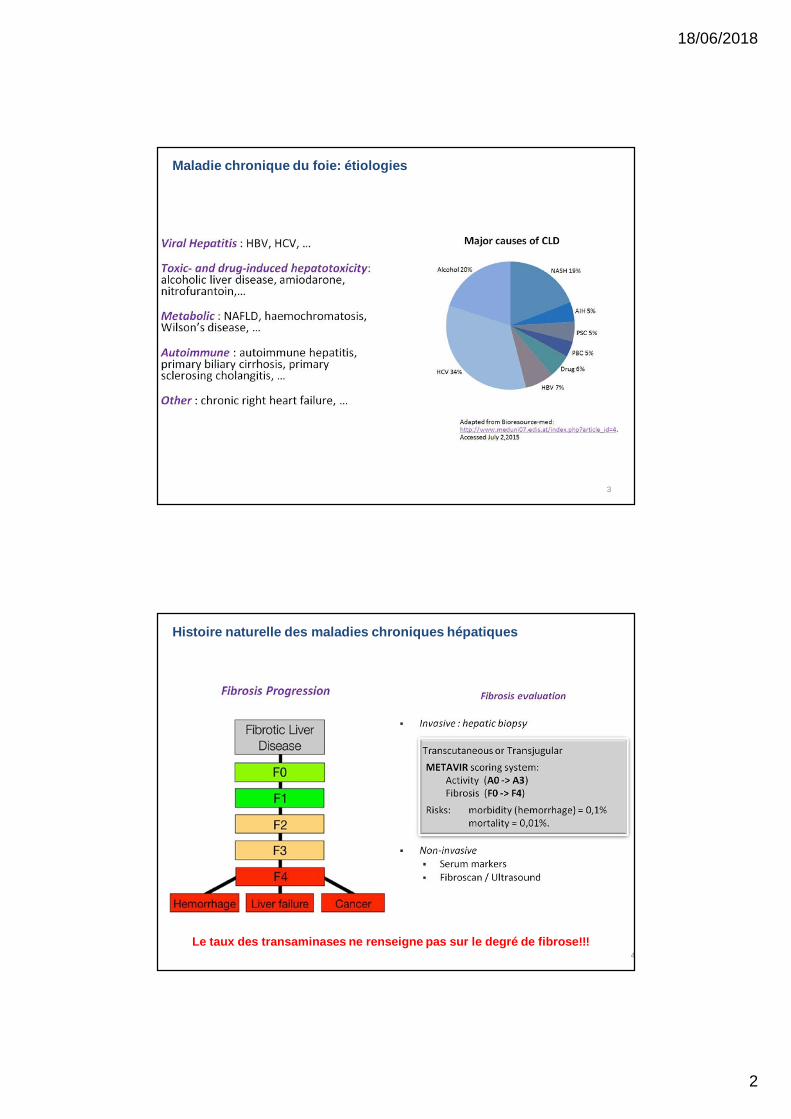
Maladie chronique du foie: étiologies
3
Histoire naturelle des maladies chroniques hépatiques
4Le taux des transaminases ne renseigne pas sur le degré de fibrose!!!

18/06/2018
3
Histologic Progression of liver disease
Normal Mild Chronic Hepatitis
Moderate Chronic Hepatitis Cirrhosis
MALADIE CHRONIQUE DU FOIE: SYMPTÔMES ET SIGNES CLINIQUES
6
- Common symptoms and signs: fatique, asthenia, arthromyalgia, anorexia, nausea, jaundice (acute phase, very rare), pruritus
- Clinical signs often linked to liver decompensation
- Possible extrahepatic manifestations: cryoglobulinemia (vasculitis…)

18/06/2018
4
CIRRHOSE: SYMPTÔMES ET SIGNES CLINIQUES
7
MALADIE CHRONIQUE DU FOIE: PRINCIPES DE TRAITEMENT
8

18/06/2018
5
9
Virus de l’hépatite C
VHC: une découverte récente…
10

18/06/2018
6
Virus de l’hépatite C
11
Virus de l’hépatite C: 6 (7) génotypes
Genotype 1: most common (60-75%) in Europe (1b), US (1a), and latin America
Genotype 2: Mediterranean sea
Genotype 3: most common in India, Far East, and Australia
common in IVDU
Genotype 4: most common in Africa and the middle East (Egypt)
Emerging in Europe among migrations, IVDU…
Genotype 5: most common in South Africa (presence in South-West Flanders)
Genotype 6: most common in Vietnam and Hong-Kong Genotype 7: described in Congo (RDC), case described in Belgium 12

18/06/2018
7
Virus de l’hépatite C: 6 (7) génotypes
13
MODES DE TRANSMISSION DU VHC
14

18/06/2018
8
MODES DE TRANSMISSION DU VHC
15
HCV INFECTION: HIGH-RISK POPULATIONS IN WHICH SCREENING IS INDICATED
Injection drug use Nasal inhalation of cocaine Chronic renal failure on
dialysis Incarceration Multiple sexual partners,
MSM, HIV positive
Transplantation or transfusion of blood products before 1992
Occupational exposure to blood products
Body piercing and possibly tattoo
Children born to HCV-positive women
Centers for Disease Control and Prevention. April 10, 2007. Verucchi G, et al. Infection. 2004;32:33-46.

18/06/2018
9
QUELS CONSEILS DONNER?
17
Hépatite C : Histoire naturelle de la maladie
9 patients sur 10 sont asymptomatiques pendant la phase
aiguë de l’infectionInfection aiguë
20 % guérison spontanée 80 % infection persistante
Pas de guérison spontanée après
passage à la chronicitéHépatite C Chronique
Stable – Non évolutive Variable – Evolutive
FibroseCirrhose
20-30 % (± après 20-30 ans)Les facteurs influençant la progression vers la cirrhose sont : l’âge au moment
de la contamination > 50 ans, la consommation d’alcool, de tabac1 et de
marijuana2Décompensation hépatique Hépatocarcinome
5% par an 3% par an
L'infection devient persistante si le virus est toujours présent 6 mois
après l'infection aiguë
Sévère – Agressive

18/06/2018
10
Serologic Pattern of Acute HCV Infection with Recovery
•Symptoms +/-
•Time after Exposure
•Tite
r
•anti-HCV
•ALT
•Normal
•0 •1 •2 •3 •4 •5 •6 •1 •2 •3 •4•Years•Months
•HCV RNA
Serologic Pattern of Acute HCV Infection with Progression to Chronic Infection
•Symptoms +/-
•Time after Exposure
•Tite
r
•Normal
•0 •1 •2 •3 •4 •5 •6 •1 •2 •3 •4•Years•Months
•HCV RNA
•anti-HCV

18/06/2018
11
Facteurs favorisant et accélérant la progression de la fibrose
21
Consommation d’alcool Obésité Diabète Marijuana HIV Carence en vitamine D (?) Facteurs génétiques Age au moment de la contamination Maladies hépatiques concomitantes (hépatite B
chronique…)
HCV Therapy
chronic hepatitis
CIRRHOSIS20%
Liver dec Death HCC3-5% 2-5% 2-4%
Annual incidences
20-30 yrs

18/06/2018
12
Hépatite C: épidémiologie
23
WORLDWIDE PREVALENCE RATES
24

18/06/2018
13
25
EPIDEMIOLOGY IN BELGIUM
Estimated 70.000 people in Belgium suffer from chronic HCV infection Around 300 die each year due to severe complications caused by HCV HCV is the leading cause of liver cancer
Chronic HCV infection = « silent killer » 50% those with HCV are unaware they are infected
Important lack of knowledge 60% of the population do not know how HCV is transmitted Nearly three-quarters of people underestimate the seriousness of HCV
Without action, the impact will increase by 2030 Deaths from HCV will nearly double Liver cancer and decompensated cirrhosis will significantly increase! 26

18/06/2018
14
Hépatite C: screening, diagnostic et mise au point
27
WHO TO SCREEN FOR HCV IN PRIORITY?
28

18/06/2018
15
HOW TO SCREEN FOR HCV?
29
Evaluation de la fibrose: Gold standard = biopsie hépatique
30

18/06/2018
16
EVALUATION DE LA FIBROSE: APPROCHE MODERNE = TESTS NON INVASIFS
31
Elastographie par Fibroscan®
EVALUATION DE LA FIBROSE: APPROCHE MODERNE = TESTS NON INVASIFS
32
Elastographie par Fibroscan®

18/06/2018
17
EVALUATION DE LA FIBROSE: APPROCHE MODERNE = TESTS NON INVASIFS
33
ELASTOGRAFY for fibrosis assesment F2-F3-F4cut-offs of ELASTOGRAFY for fibrosis assesment F2-F3-F4chronic hepatitis C
(agreed at RIZIV-INAMI 01.12.2016)1. Fibroscan1
Valid if 10 correct measurements, success rate > 60%, IQR < 30%
F2 ≥ 7.1 kPAF3 ≥ 9.5 kPAF4 ≥ 12.5 kPA
2. Shear wave elastografie2
F2 ≥ 7.1 kPAF3 ≥ 8.7 kPAF4 ≥ 10.4 kPA
3. Acoustic radiation forse impulse (ARFI, Siemens technique)3,4
F2 ≥ 1.22 m/sF3 ≥ 1,55 m/sF4 ≥ 1,80 m/s
1Castera et al. Gasteroenterology 20052Ferraioli et al Hepatology 2012
3Friedrich-Rust et al J Viral Hepat 20124Ferraioli et al J Ultrasound Med 2014

18/06/2018
18
cut-offs of BIOLOGICAL FIBROSIS-SCORES for assesment F2-F3-F4 in chronic hepatitis C
(agreed at RIZIV-INAMI 01.12.2016)
1. Fibrotest (Biopredictive):
Elements : α2 macroglobulin, haptoglobin, apolipoprotein A1, total bilirubin, GGTF2 : ≥ 0.49F3: 0.59-0.72F3-F4: 0.73-0.74F4: ≥0.75
2. Apri (ast-platelet ratio)In a pure HCV cohortF2: APRI not to use for detection of F2F3: ≥ 1F4: ≥ 1.6Reference: Holmberg, Clin Infect Dis 2013
3. Fib-4 (age, AST,ALT, platelets)F2 ≥ 1.45F3: ≥ 2.1F3-F4: ≥ 3.25F4: ≥ 3.85References: Vallet-Pichard, Hepatology 2007, Holmberg, Clin Infect Dis 2013, Martinez APT 2011
Useful website: www.hepatitisc.uw.edu/page/clinical-calculators
ADDITIONAL EVALUATION FOR TREATMENT
36
18/06/2018
19
Traitement antiviral C: passé, présent et futur
37
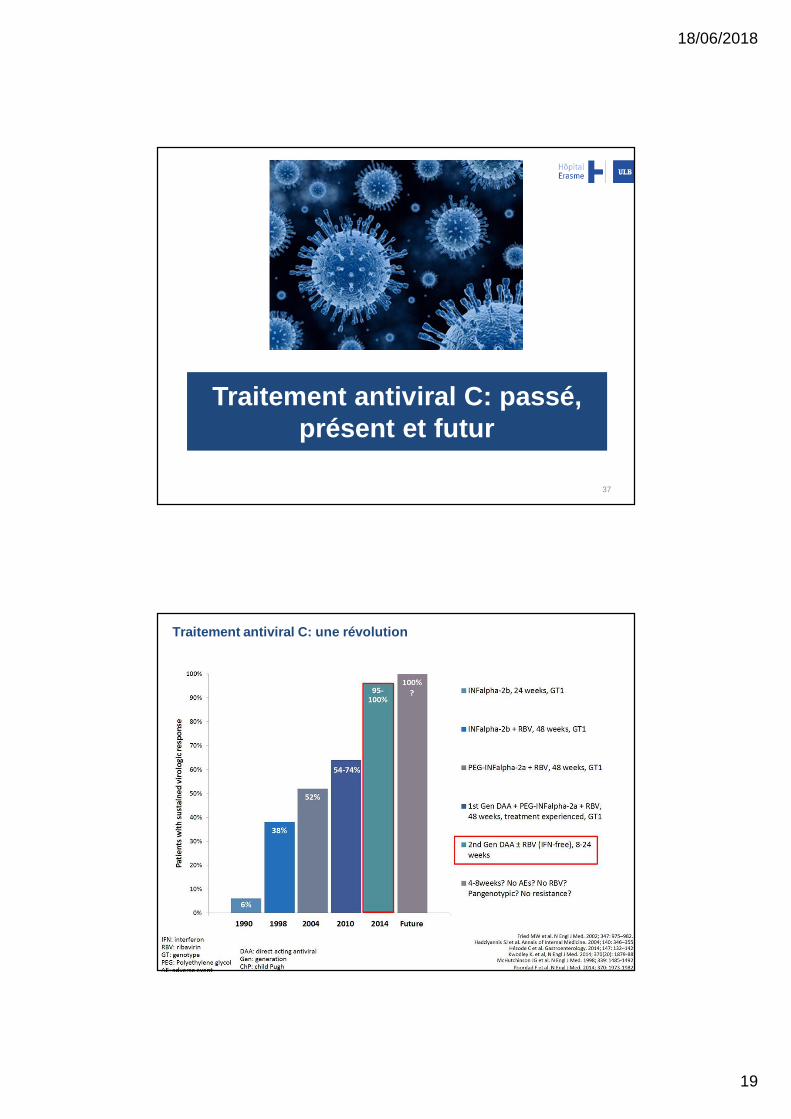
Traitement antiviral C: une révolution
38

18/06/2018
20
Antiviraux à action directe
39
TRAITEMENT ACTUEL: PRINCIPES
Combinaisons de 2-3 antiviraux à action directe
+/- Ribavirine
Sans interféron
8 à 24 semaines (12 le plus souvent)
Excellente tolérance
Efficacité élevée (>90%)40

18/06/2018
21
Guérison?
= Guérison virologique
SVR12 = absence d’ARN viral C détectable dans le sang 12 semaines après la fin du traitement
! Anticorps restent positifs (non protecteurs)!

18/06/2018
22
WHICH DRUGS?
Sovaldi (sofosbuvir): GT1, 2, 3, 4, 5, 6 (12 or 24 wk)
Daklinza (daclatasvir): GT1, 2, 3, 4, 5, 6 (12 or 24 wk) with Sovaldi
Harvoni (sofosbuvir/ledipasvir): GT1, 2, 3, 4, 5, 6 (12 or 24 wk)
Epclusa (sofosbuvir/velpatasvir): GT1, 2, 3, 4, 5, 6, 7 (12 or 24 wk)
Zepatier (elbasvir/grazoprevir): GT1 and 4 (12 or 16 wk)
Maviret (Glecaprevir/pibrentasvir): GT 1, 2, 3, 4, 5, 6 (8, 12 or 16 wk)
Vosevi (sofosbuvir/velpatasvir/voxilaprevir): NS5a failure (12 wk)43
Prix?

18/06/2018
23
Précautions: interactions médicamenteuses
45
NEW REIMBURSEMENT CRITERIA: JANUARY 1ST 2017
Chronic hepatitis C with ≥ F2 fibrosis stage Confirmed by either a liver biopsy or a combination of
elastography and biological fibrosis score
Chronic hepatitis C regardless of fibrosis stage if: HIV-HCV coinfection HBV-HCV coinfection Listed for or post-solid organ transplantation Listed for or post hematopoietic stem cell/bone marrow transplantation Severe extrahepatic manifestation: diffuse large cell lymphoma B,
immunomediated vasculitis, renal disease related to mixed cryoglobulinemia Patient on dialysis Hemophilia or other coagulation disorder Hemoglobinopathy pregnancy
46

18/06/2018
24
NEW REIMBURSEMENT CRITERIA: JANUARY 1ST 2017
Presciption by a Specialist in Gastroenterology or InternalMedicine Attached to an academic centre if 580, 588 or 987 Attached to academic or non academic hospital if 650, 651 or 659 Training in Hepatology (15 CME/year) Agrees to record follow-up data of treated patients (presentation
today at 16:40)
Trough e-health plateform
According to international recommandations
47
Quel suivi après guérison?
Guérison virologique ≠ guérison maladie hépatique
Persistance risque hépatocarcinome chez les patients avec fibrose avancée ou cirrhose
Poursuite du suivi et dépistage (échographie hépatique et biologie avec AFP) / 6 mois

18/06/2018
25
CONCLUSIONS
Hépatite C chronique = maladie facilement curable
Nouveaux antiviraux à action directe: très efficace, excellente tolérance, traitement court
Importance de la compliance et interactions médicamenteuses
Enjeux du futur: Augmentation drastique dépistage et accès au traitement diminution mortalité/morbidité et éradication HCV
Hépatite C chronique: asymptomatique, nécessité d’évaluation de la fibrose (tests non invasifs) chez tout patient HCV


















