Hepatic Disease Normal Anatomy andPhysiology. Hepatic: Normal Anatomy 1. Biliary system 2. Portal...
25
Hepatic Disease Hepatic Disease Normal Anatomy Normal Anatomy and and Physiology Physiology
-
Upload
milton-mcbride -
Category
Documents
-
view
240 -
download
2
Transcript of Hepatic Disease Normal Anatomy andPhysiology. Hepatic: Normal Anatomy 1. Biliary system 2. Portal...
Hepatic DiseaseHepatic Disease
Normal AnatomyNormal Anatomy
and and
PhysiologyPhysiology
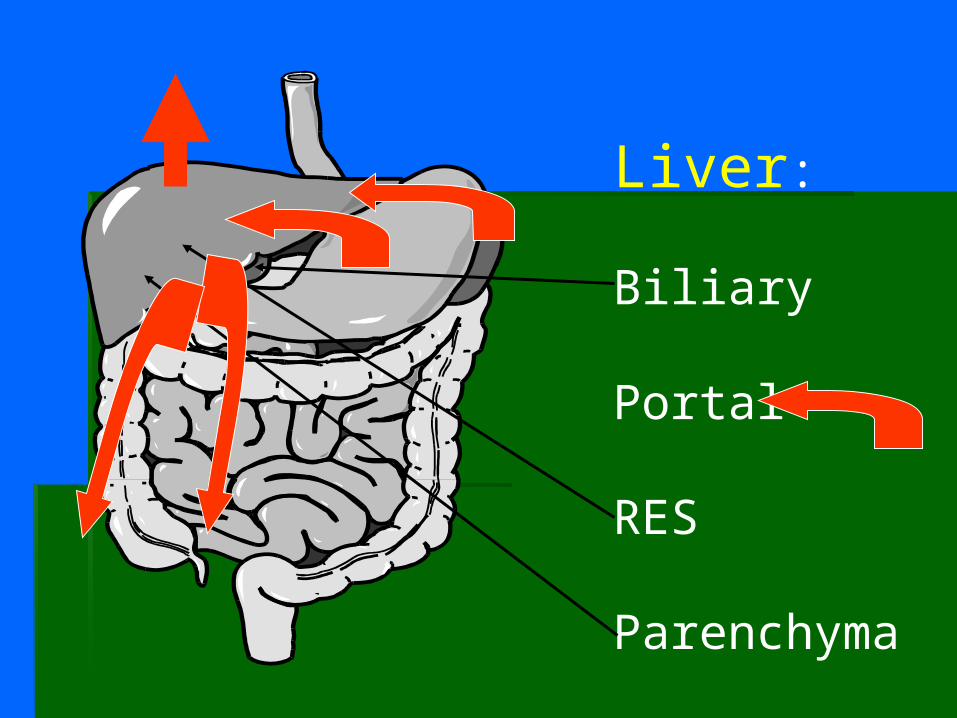
Hepatic: Normal Anatomy
1. Biliary system1. Biliary system
2. Portal system 2. Portal system
3. Reticulo-endothelial system3. Reticulo-endothelial system
4. Hepatic parenchyma:4. Hepatic parenchyma:
synthetic synthetic
metabolicmetabolic
Liver:
Biliary
Portal
RES
Parenchyma
Hepatic: Normal physiologyHepatic: Normal physiology
1. Secretion of bile for fat absorption2. Short term sugar storage (glycogen)3. Aged RBC breakdown and
excretion of bilirubin4. Synthesis of coagulation factors5. Synthesis of albumin6. Drug metabolism
HepatitisHepatitis: Inflammation of the liver
Causes: alcoholic and viral (A,B,C,D,E)
(others: mononucleosis, syphillis, TB, methotrexate, ketoconazole)
Acetaminophen overdose
HepatitisHepatitis: Acute symptoms
Abdominal pain, nausea, vomiting, fever, malaise
Jaundice
Hepatomegaly and splenomegaly
In recovery phase: persistent hepatomegaly and abnormal LFTs
HepatitisHepatitis: Chronic symptoms
May be asymptomatic for 10 to 30 years
Nonspecific signs: fatigue, weight loss, itchiness, right upper quadrant pain
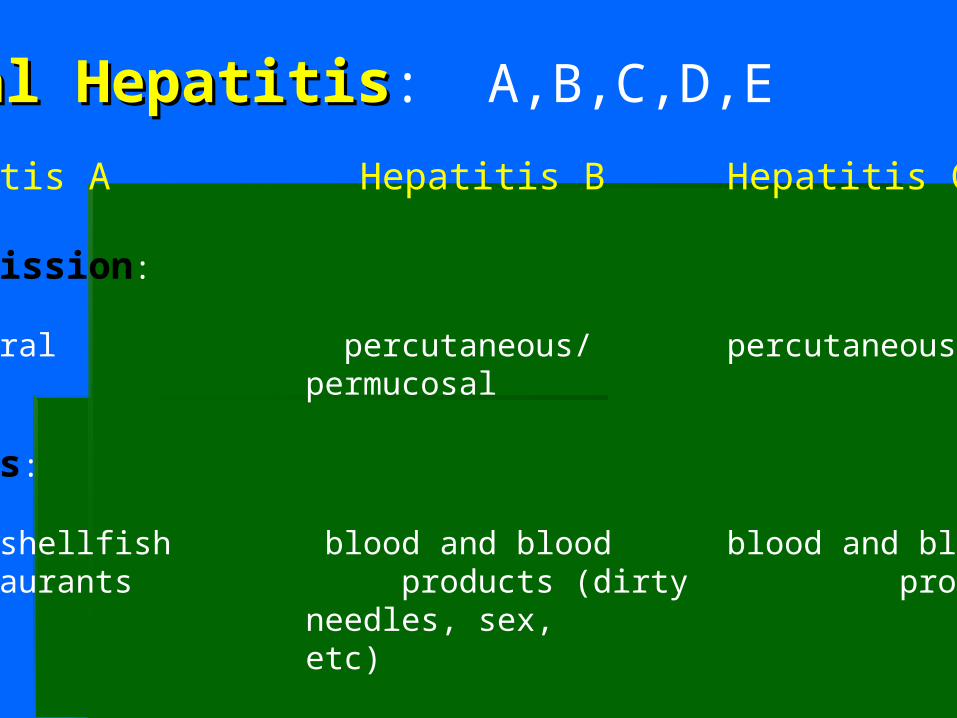
Viral HepatitisViral Hepatitis: A,B,C,D,E
Hepatitis A Hepatitis B Hepatitis C
Transmission:
Fecal-oral percutaneous/ percutaneous permucosal
Sources:
Water, shellfish blood and blood blood and blood restaurants products (dirty products
needles, sex, etc)
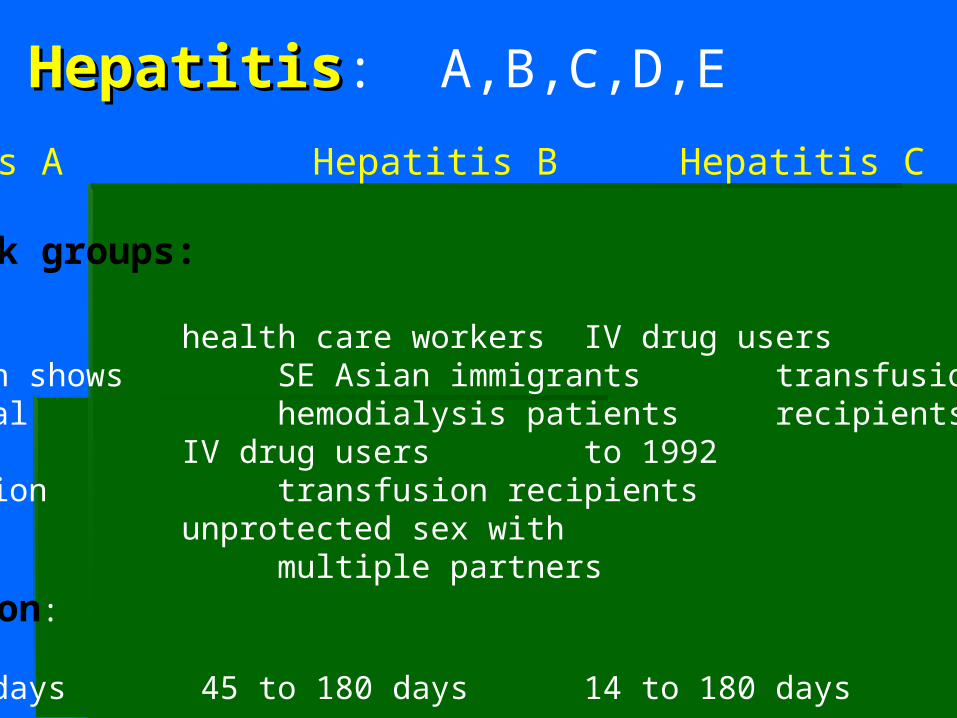
Viral HepatitisViral Hepatitis: A,B,C,D,E
Hepatitis A Hepatitis B Hepatitis C
High risk groups:
40% of US health care workers IV drug userspopulation shows SE Asian immigrants transfusion serological hemodialysis patients recipients priorevidence IV drug users to 1992of infection transfusion recipients
unprotected sex with multiple partners
Incubation:
15 to 50 days 45 to 180 days 14 to 180 days
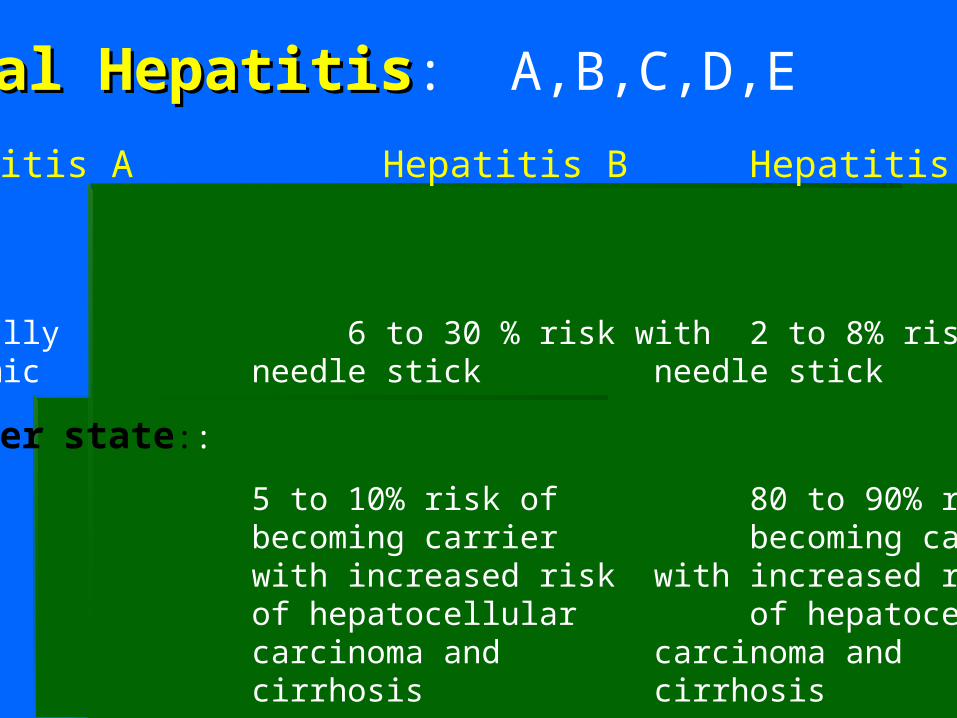
Viral HepatitisViral Hepatitis: A,B,C,D,E
Hepatitis A Hepatitis B Hepatitis C
Risk:
Typically 6 to 30 % risk with 2 to 8% risk withepidemic needle stick needle stick
Carrier state::
None 5 to 10% risk of 80 to 90% risk becoming carrier becoming carrier with increased risk with increased risk of hepatocellular of hepatocellular carcinoma and carcinoma and cirrhosis cirrhosis
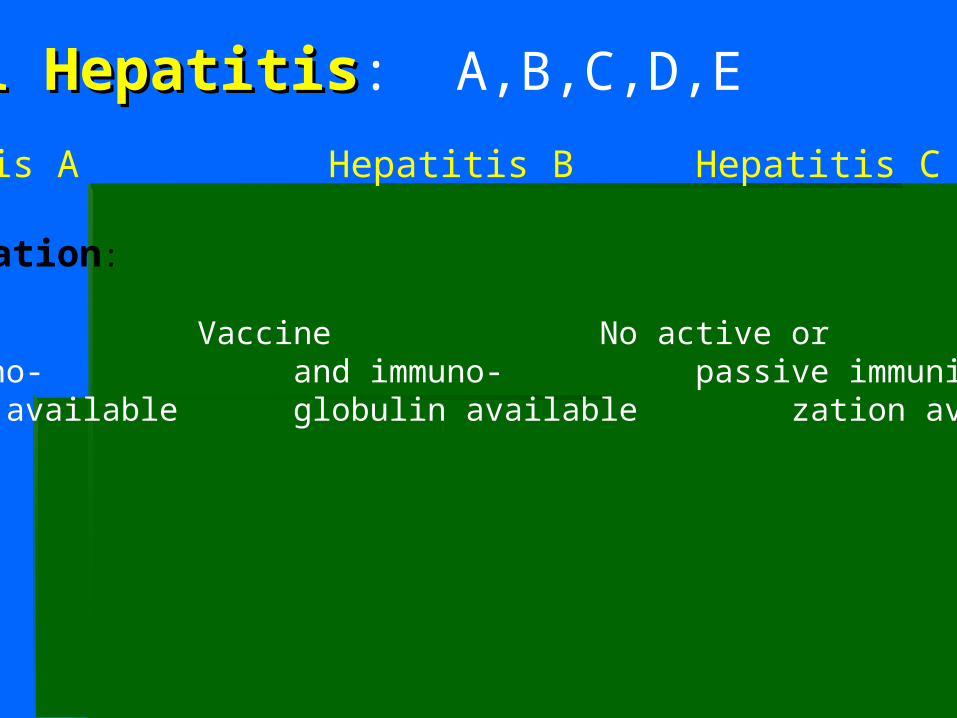
Viral HepatitisViral Hepatitis: A,B,C,D,E
Hepatitis A Hepatitis B Hepatitis C
Immunization:
Vaccine Vaccine No active orand immuno- and immuno- passive immuni-globulin available globulin available zation available
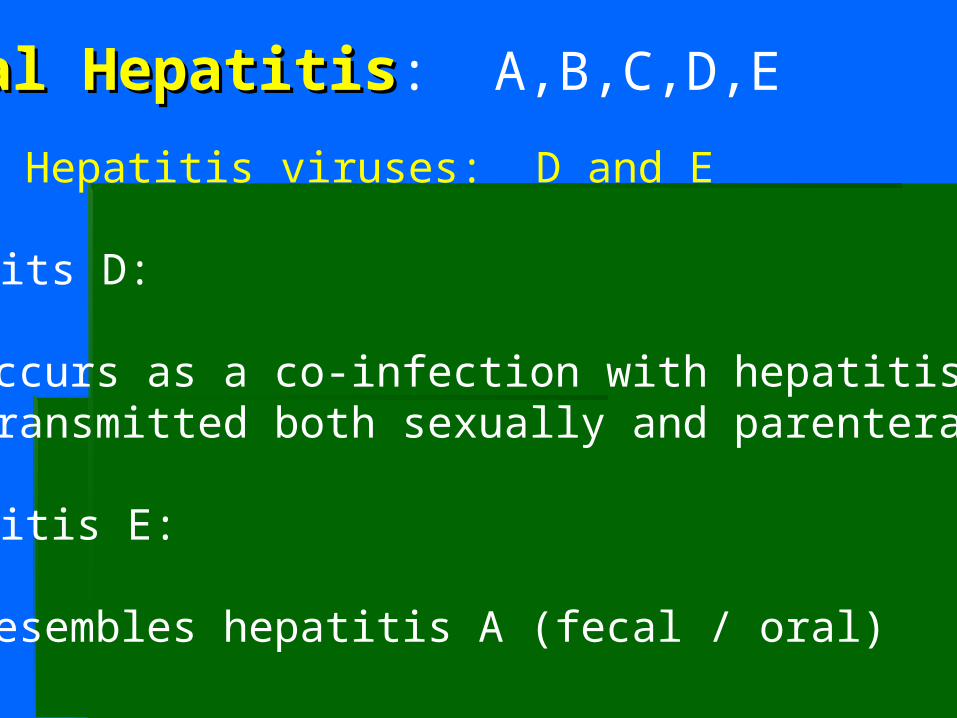
Viral HepatitisViral Hepatitis: A,B,C,D,E
Other Hepatitis viruses: D and E
Hepatits D:
occurs as a co-infection with hepatitis Btransmitted both sexually and parenterally
Hepatitis E:
resembles hepatitis A (fecal / oral)
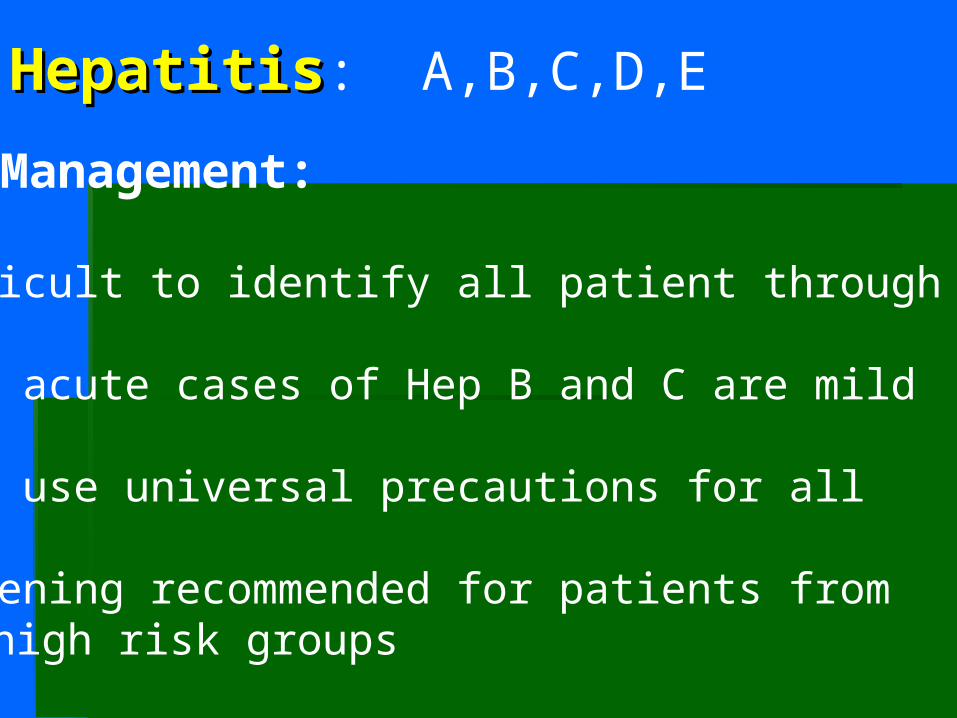
Viral HepatitisViral Hepatitis: A,B,C,D,E
Dental Management:
Difficult to identify all patient through history
Many acute cases of Hep B and C are mild
MUST use universal precautions for all
Screening recommended for patients fromhigh risk groups
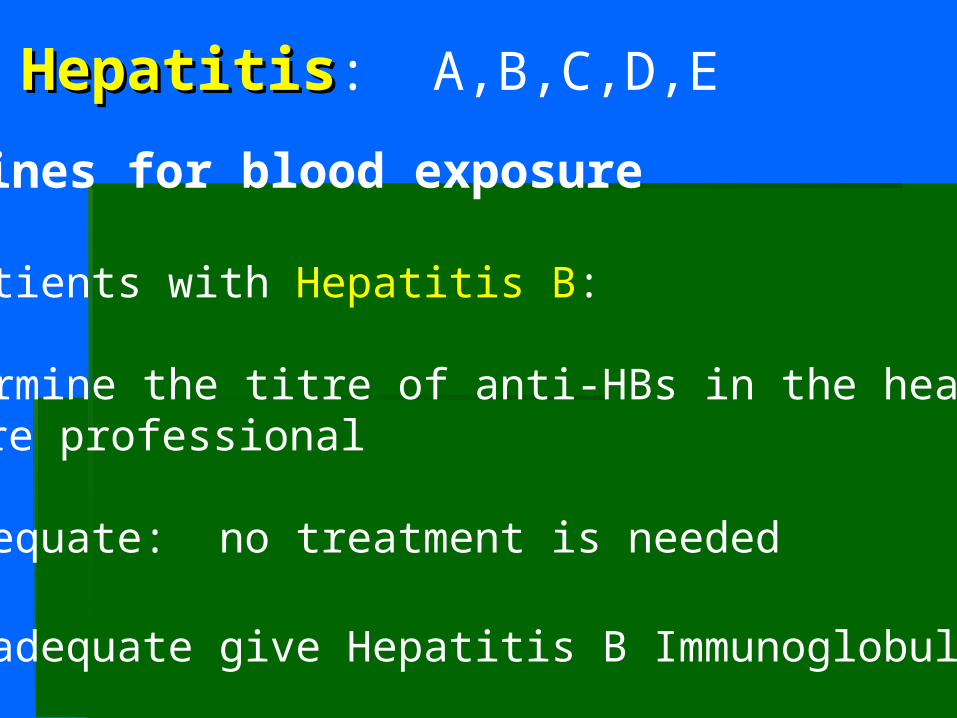
Viral HepatitisViral Hepatitis: A,B,C,D,E
Guidelines for blood exposure
From patients with Hepatitis B:
1. Determine the titre of anti-HBs in the health care professional
2. If adequate: no treatment is needed
3. If inadequate give Hepatitis B Immunoglobulin
Viral HepatitisViral Hepatitis: A,B,C,D,E
Guidelines for blood exposure
From patients with Hepatitis C
1. Exposed professional gets baseline and
follow up testing for anti-HCV and liver
enzymes
Viral HepatitisViral Hepatitis: A,B,C,D,E
Guidelines for blood exposure
From patients with Unknown
1. Ask for serological testing of the patient
(this can be ordered by the Medical
Officer)
Alcoholic Liver Disease:Alcoholic Liver Disease:
1. Definition of an alcoholic …
estimate: 170 to 200 out of 2000 patients
2. Problem drinking:
male > 12 oz. / week
female > 9 oz. / week
3. During history taking: double it
Alcoholic Liver Disease:Alcoholic Liver Disease:
1. 10 to 15% of alcoholics develop cirrhosis
2. Early change: fatty liver
3. Second stage: alcoholic hepatitis
4. Final stage: cirrhosis with parenchymal damage
and scarring leading to portal hypertension
End-stage Liver Disease:End-stage Liver Disease:(regardless of cause)
1. Loss of Synthetic function:Vit K dependant coagulation factors (II, VII, IX, X)hypoalbuminemia (edema)
2. Portal hypertensionesophageal, umbilical, hemorroidal varicesascites (abdominal fluid build-up)splenomegaly (thrombocytopenia)
3. Loss of de-toxification function: ammonia poisoning: encephalopathy and dementia
End-stage Liver Disease:End-stage Liver Disease:(regardless of cause)
4. Bone marrow toxicity: anemia, leukopenia and thrombocytopenia (decrease HgB, WBC and platelets on CBC)
5. Endocrine disturbances: testicular atrophy andgynecomastia
6. Esophagitis / gastritis
7. Elevated Liver enzymes: AST / ALT
End-stage Liver Disease:End-stage Liver Disease:(regardless of cause)
8. Elevated bilirubin: causing Jaundice
9. Elevated INR: causing bleeding
10. Decreased albumin: causing edema and ascites
11. Altered drug metabolism: unpredictable
Drug effect can be Up or Down
End-stage Liver Disease:End-stage Liver Disease:(regardless of cause)
11. Altered drug metabolism (cont’d): unpredictable
Decreased drug effect due to induction of hepaticmicrosomal enzymes and accelerated metabolismof the drug
Increased drug effect due to loss of hepatic function and slowed metabolism of the drug
Increased drug effect due to decreased plasmaprotein (albumin) binding and therefore increasedunbound (active) drug
Liver Disease: Liver Disease: treatmenttreatment
1. In acute hepatitis: supportive, steroids
2. In chronic hepatitis: interferon
3. In failure or end stage disease: transplant
Liver Disease: Liver Disease: managementmanagement
1. Beware of second addictions (narcotics, etc)
2. Unpredictable drug metabolism
3. Caution or avoid hepatically metabolized drugs:NSAIDs, narcotics, acetaminophen, benzodiazepines, metronidazole, localanaesthetics
4. Bleeding tendencies (CBC, PTT, INR):may require vit K, FFP or platelets
Questions????