
Henderson-Hasselbalch Equation Acid-base Balance 1.
43
Henderson-Hasselbalch Equation Acid-base Balance www.mecriticalcare.net 1
-
Upload
abner-mccoy -
Category
Documents
-
view
249 -
download
1
Transcript of Henderson-Hasselbalch Equation Acid-base Balance 1.
Henderson-Hasselbalch Equation
Acid-base Balance
www.mecriticalcare.net
1
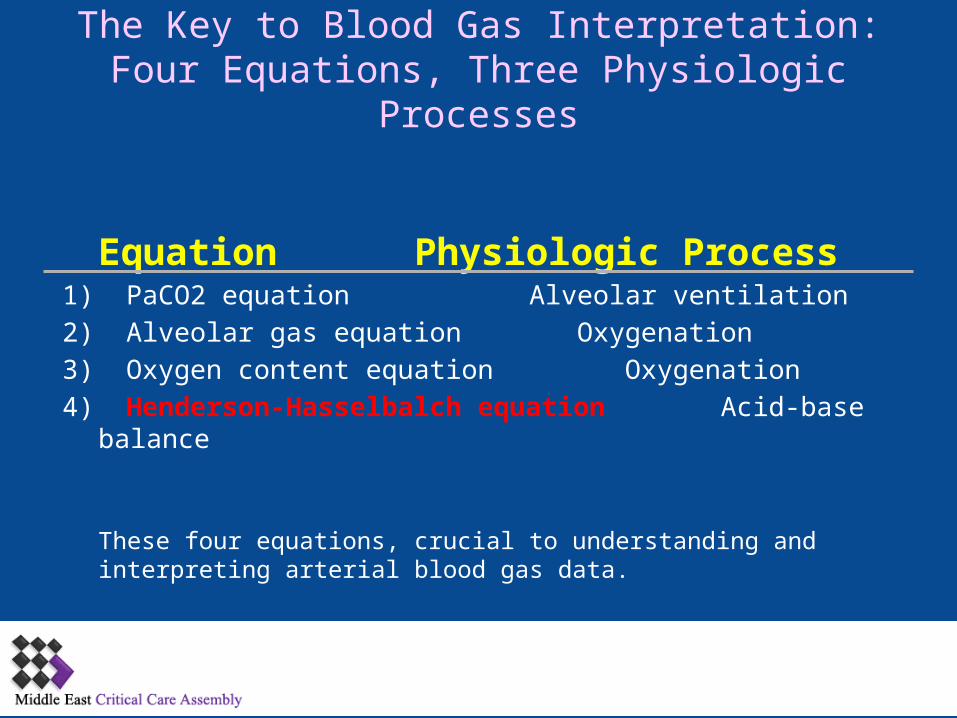
The Key to Blood Gas Interpretation:Four Equations, Three Physiologic Processes
Equation Physiologic Process1) PaCO2 equation Alveolar ventilation
2) Alveolar gas equation Oxygenation
3) Oxygen content equation Oxygenation
4) Henderson-Hasselbalch equation Acid-base balance
These four equations, crucial to understanding and interpreting arterial blood gas data.
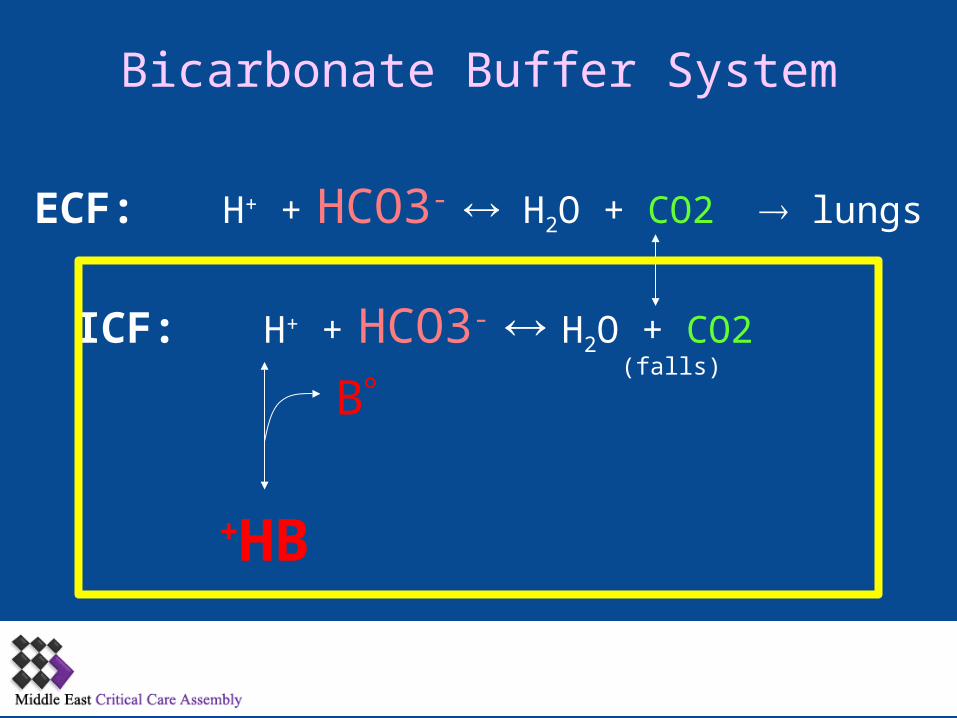
Bicarbonate Buffer System
ECF: H+ + HCO3- H2O + CO2 lungs
ICF: H+ + HCO3- H2O + CO2
HB+
B)falls)

Henderson-Hasselbalch Equation
For teaching purposes, the H-H equation can be shortened to its basic relationships:
pH = pK + log ----------------------[ HCO3-
]
0.03[ PaCO2]
pH ~ ---------------- HCO3
-
PaCO2
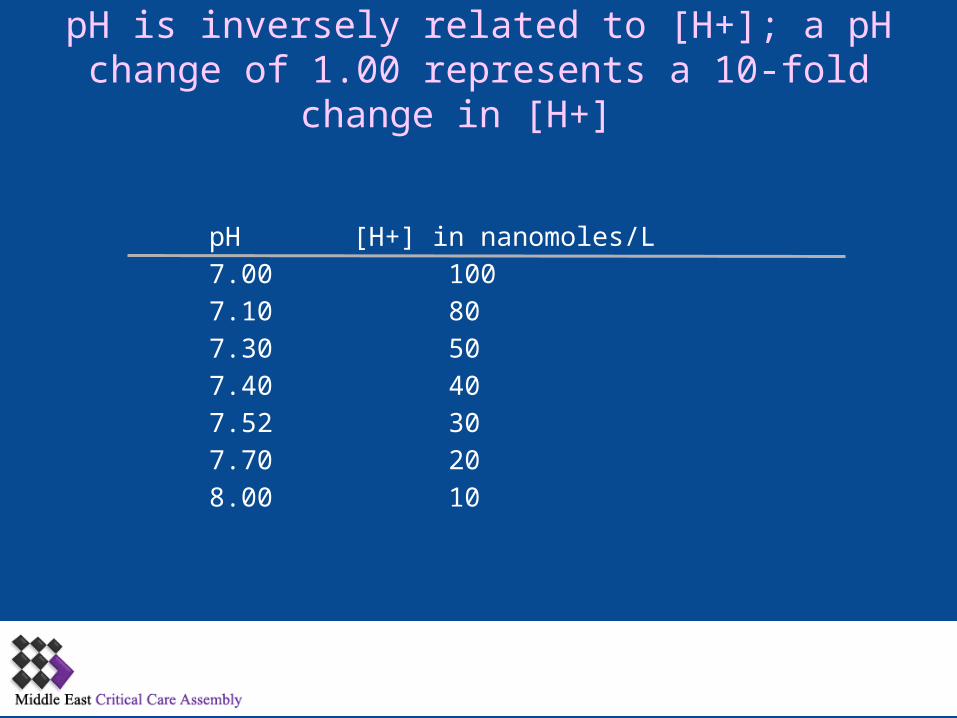
pH is inversely related to [H+]; a pH change of 1.00 represents a 10-fold change in [H+]
pH ]H+[ in nanomoles/L
7.00 100
7.10 80
7.30 50
7.40 40
7.52 30
7.70 20
8.00 10
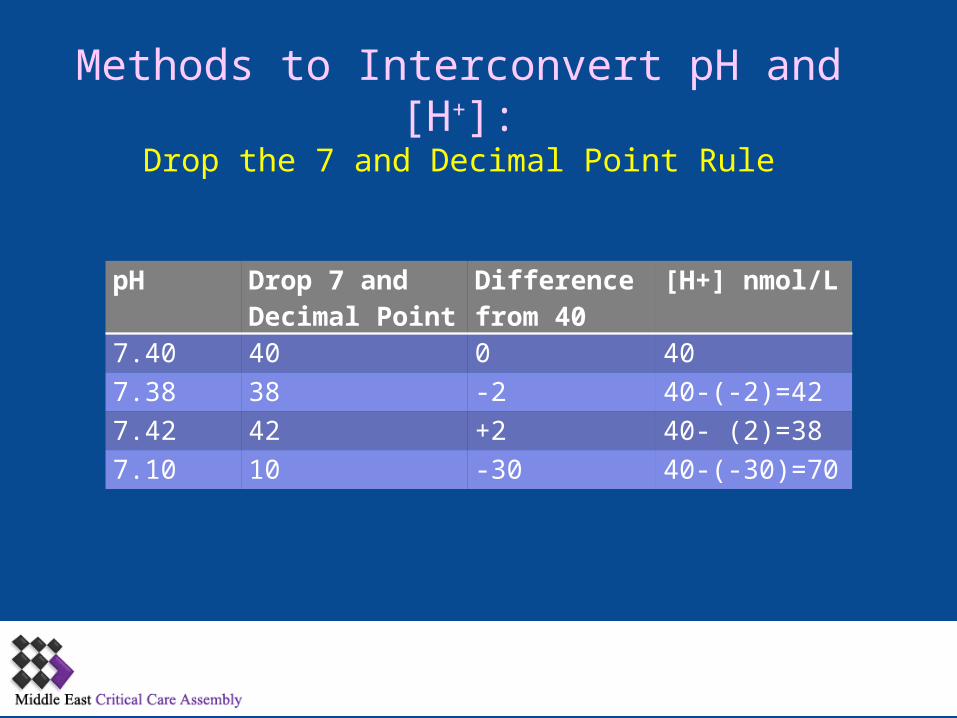
Methods to Interconvert pH and [H+]:Drop the 7 and Decimal Point Rule
pH Drop 7 and Decimal Point
Difference from 40
[H+] nmol/L
7.40 40 0 40
7.38 38 -2 40-)-2)=42
7.42 42 +2 40- )2)=38
7.10 10 -30 40-)-30)=70
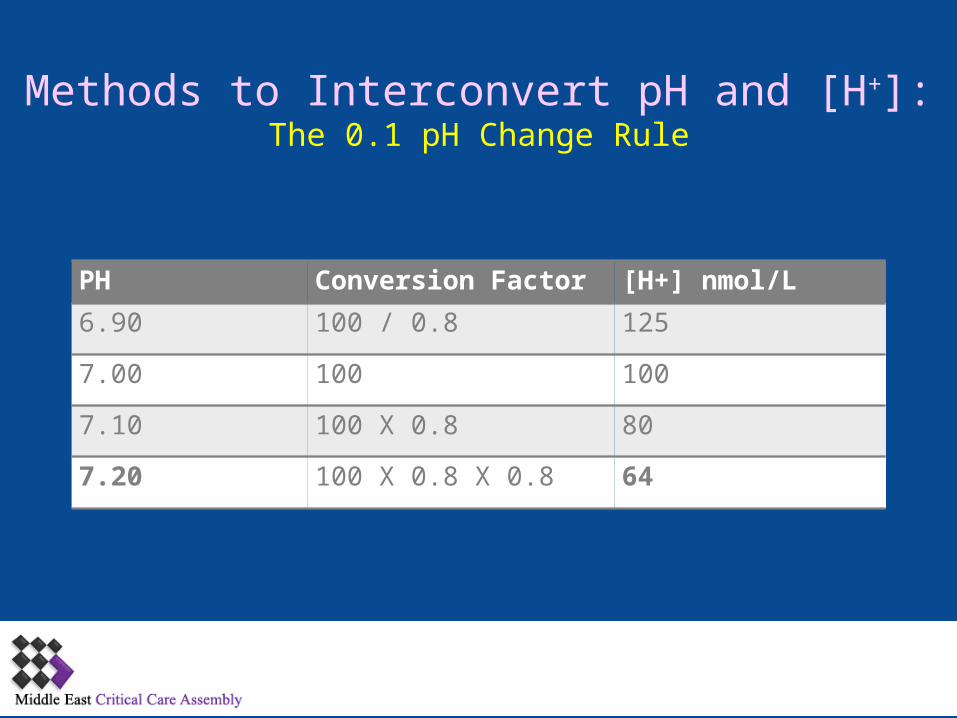
Methods to Interconvert pH and [H+]:The 0.1 pH Change Rule
PH Conversion Factor [H+] nmol/L
6.90 100 / 0.8 125
7.00 100 100
7.10 100 X 0.8 80
7.20 100 X 0.8 X 0.8 64
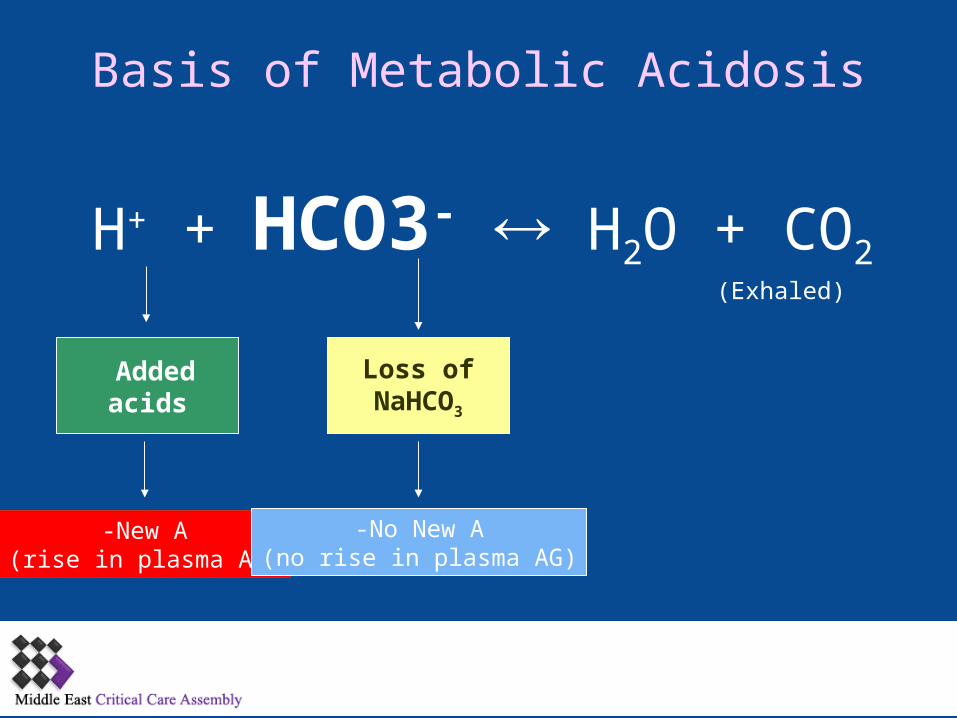
Basis of Metabolic Acidosis
H+ + HCO3- H2O + CO2
Added acids
Loss ofNaHCO3
New A-)rise in plasma AG)
)Exhaled)
No New A-)no rise in plasma AG)
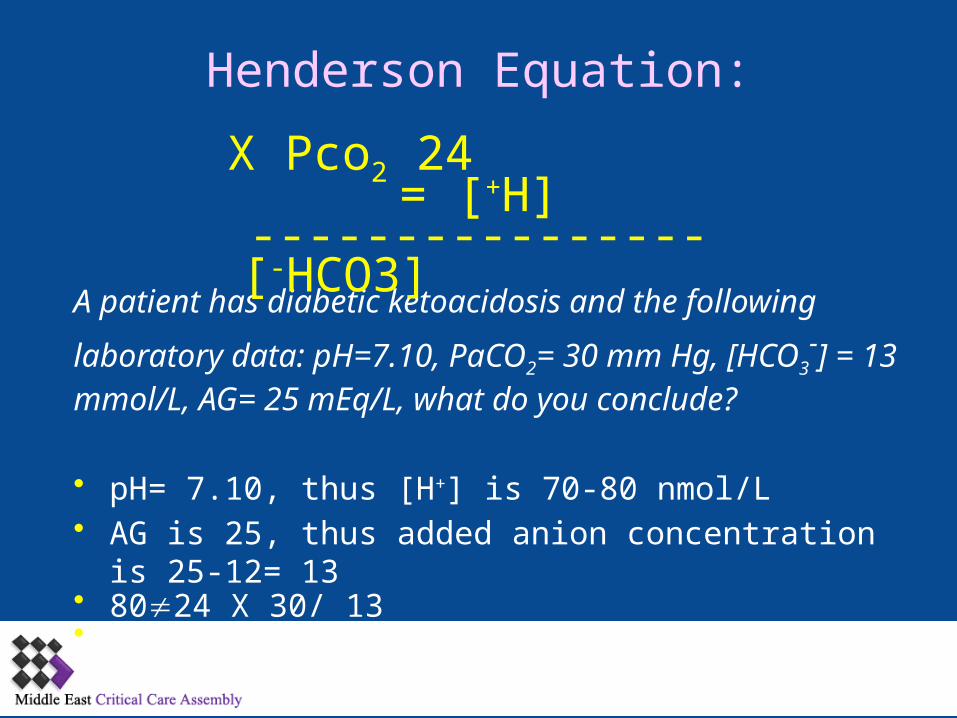
Henderson Equation:
A patient has diabetic ketoacidosis and the following
laboratory data: pH=7.10, PaCO2= 30 mm Hg, [HCO3-] =
13 mmol/L, AG= 25 mEq/L, what do you conclude?
• pH= 7.10, thus ]H+[ is 70-80 nmol/L• AG is 25, thus added anion concentration is 25-12= 13• 8024 X 30/ 13• 8056
24 X Pco2[H+---------------- = ]
[ HCO3-]
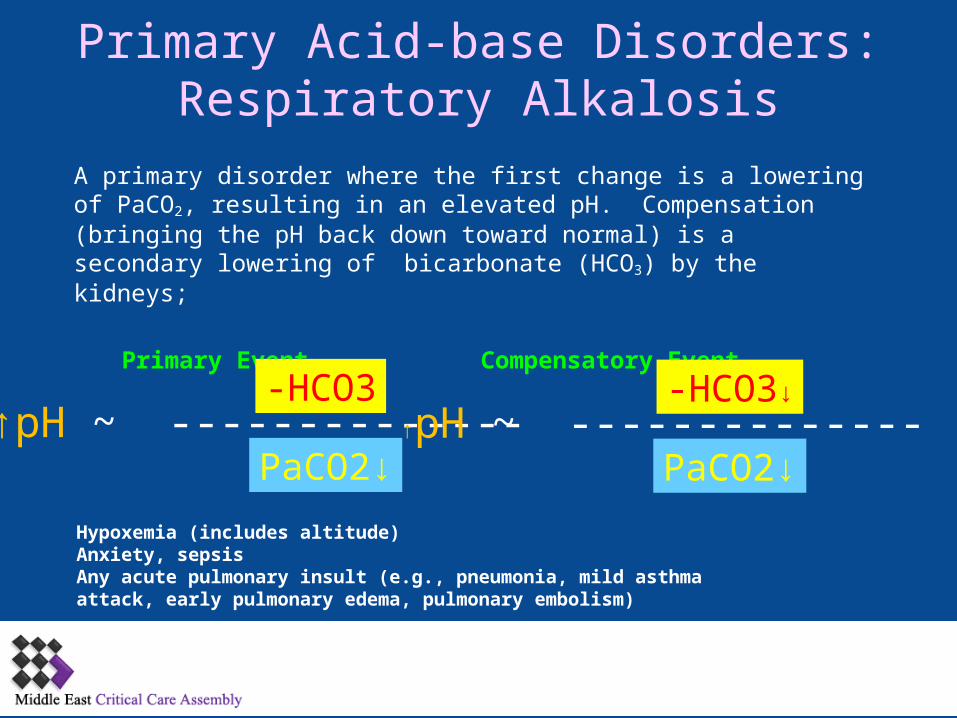
Primary Acid-base Disorders:Respiratory Alkalosis
A primary disorder where the first change is a lowering of PaCO2, resulting in an elevated pH. Compensation )bringing the pH back down toward normal) is a secondary lowering of bicarbonate )HCO3) by the kidneys;
Primary Event Compensatory Event
↑pH ~ --------------HCO3-
↓PaCO2↑pH ~ --------------
↓HCO3-
↓PaCO2
Hypoxemia (includes altitude)Anxiety, sepsisAny acute pulmonary insult (e.g., pneumonia, mild asthma attack, early pulmonary edema, pulmonary embolism)
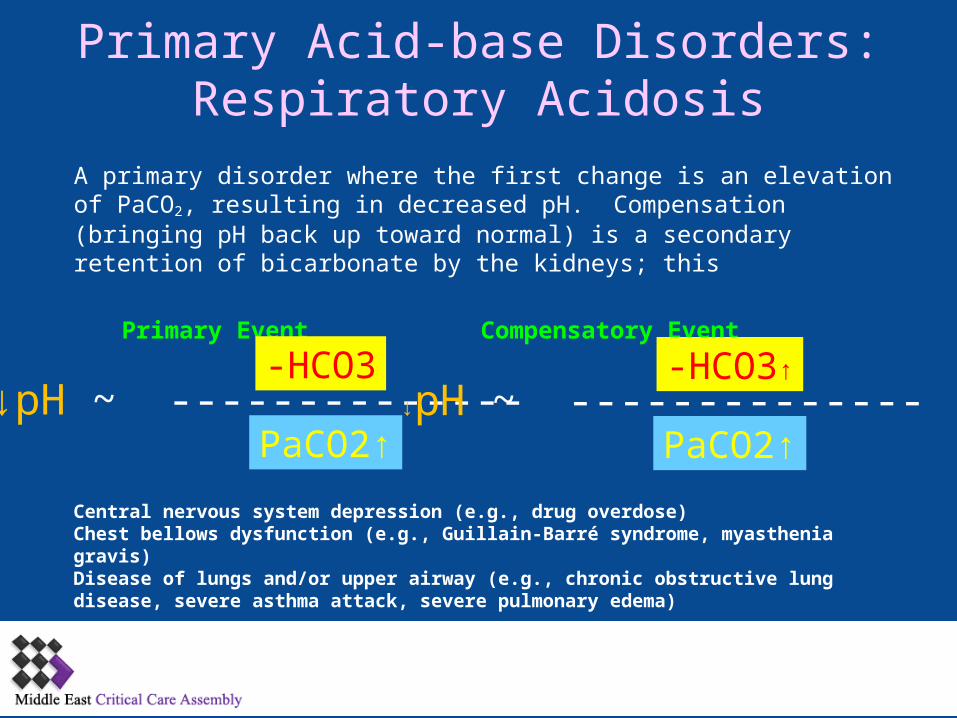
Primary Acid-base Disorders:Respiratory Acidosis
A primary disorder where the first change is an elevation of PaCO2, resulting in decreased pH. Compensation )bringing pH back up toward normal) is a secondary retention of bicarbonate by the kidneys; this
Primary Event Compensatory Event
↓pH ~ --------------HCO3-
↑PaCO2↓pH ~ --------------
↑HCO3-
↑PaCO2
Central nervous system depression (e.g., drug overdose)Chest bellows dysfunction (e.g., Guillain-Barré syndrome, myasthenia gravis) Disease of lungs and/or upper airway (e.g., chronic obstructive lung disease, severe asthma attack, severe pulmonary edema)
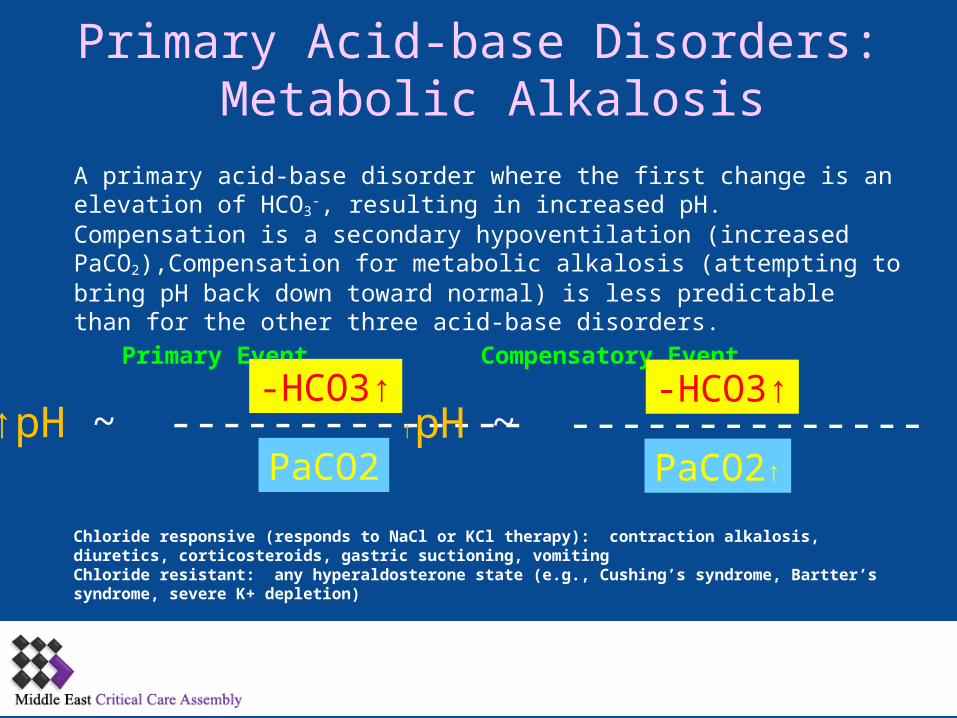
Primary Acid-base Disorders: Metabolic Alkalosis
A primary acid-base disorder where the first change is an elevation of HCO3-,
resulting in increased pH. Compensation is a secondary hypoventilation )increased PaCO2),Compensation for metabolic alkalosis )attempting to bring pH back down toward normal) is less predictable than for the other three acid-base disorders.
Primary Event Compensatory Event
↑pH ~ --------------↑HCO3-
PaCO2↑pH ~ --------------
↑HCO3-
↑PaCO2
Chloride responsive (responds to NaCl or KCl therapy): contraction alkalosis, diuretics, corticosteroids, gastric suctioning, vomiting Chloride resistant: any hyperaldosterone state (e.g., Cushing’s syndrome, Bartter’s syndrome, severe K+ depletion)

Primary Acid-base Disorders: Metabolic Acidosis
A primary acid-base disorder where the first change is a lowering of HCO3-, resulting in decreased pH. Compensation )bringing pH back up toward normal) is a secondary hyperventilation; this lowering of PaCO2 is not respiratory alkalosis since it is not a primary process.
Primary Event Compensatory Event
↓pH ~ --------------↓HCO3-
PaCO2↓pH ~ --------------
↓HCO3-
↓PaCO2

Anion Gap
Note: CO2 in this equation is the “total CO2” measured in the chemistry lab as part of routine serum electrolytes, and consists mostly of bicarbonate. Normal AG is typically 12 ± 4 mEq/L. If AG is calculated using K+, the normal AG is 16 ± 4 mEq/L..
Serum Cations (+) Serum Anions (-)
Na+ Cl-
K+ HCO3-
Mg++ HPO4--
Ca++ SO4--
Proteins-
Na+ + K+ + Mg++ + Ca++ + Protein+ = Cl- + HCO3- + HPO4
-- + SO4-- + Proteins-
Na+ + K+ + UC+= Cl- + HCO3- + UA--
AG = Na+ - )Cl- + CO2)
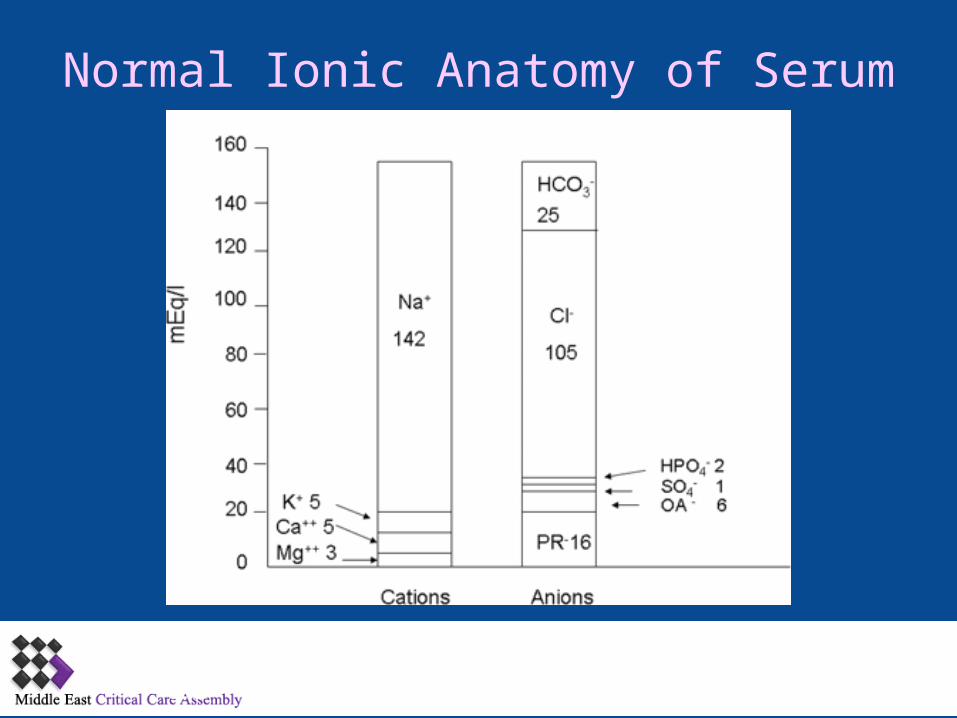
Normal Ionic Anatomy of Serum
15
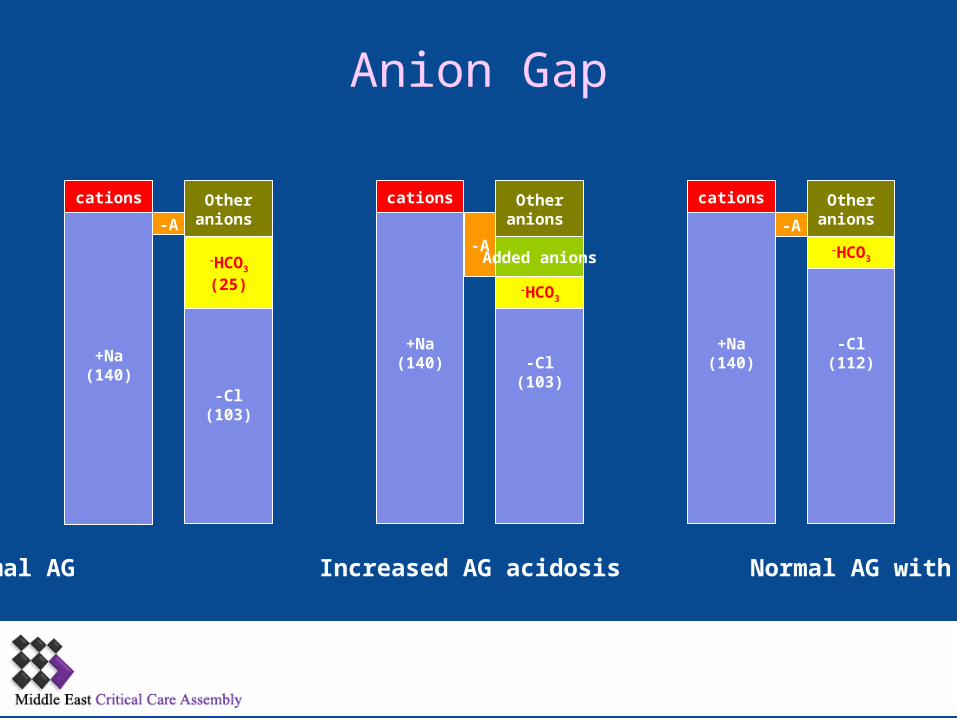
Na+)140(
Cl-)103(
Na+)140( Cl-
)103(
Na+)140(
Cl-)112(
A-
cations
HCO3-
)25(
Other anions
A-
Other anions
Other anions
cationscations
A-
HCO3-
Added anions HCO3-
Normal AG Increased AG acidosis Normal AG with acidosis
Anion Gap
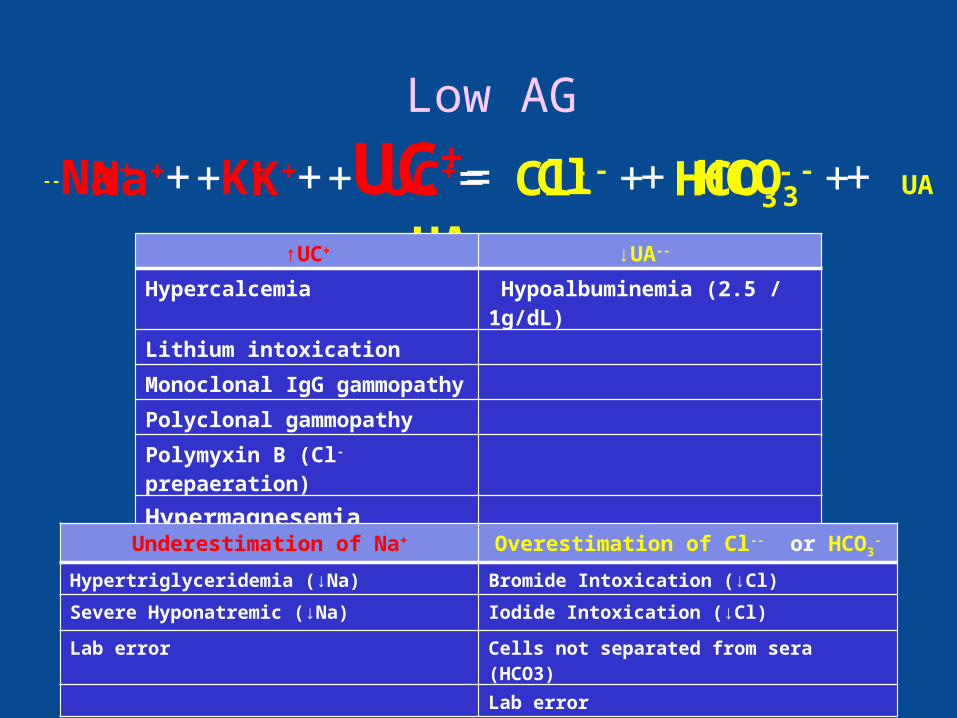
Low AG
Na+ + K+ + UC+= Cl- + HCO3- + UA-- Na+ + K+ + UC+= Cl- + HCO3
- + UA--
↑UC+ ↓UA--
Hypercalcemia Hypoalbuminemia (2.5 / 1g/dL)
Lithium intoxication
Monoclonal IgG gammopathy
Polyclonal gammopathy
Polymyxin B (Cl- prepaeration)
Hypermagnesemia
Underestimation of Na+ Overestimation of Cl-- or HCO3-
Hypertriglyceridemia (↓Na) Bromide Intoxication (↓Cl)
Severe Hyponatremic (↓Na) Iodide Intoxication (↓Cl)
Lab error Cells not separated from sera (HCO3)
Lab error

High AG
Na+ + K+ + UC+= Cl- + HCO3- + UA--
19
Na+ + K+ + UC+= Cl- + HCO3- + UA--
↓UC+ ↑UA--
L-Lactic acid (Type A and B)
D-Lactic acid
Ketoacidosis (-hydroxybutyric acid))
Hyperlbuminemia
Severe hyperphosphatemia
Hypocalcemia Increased anionic paraproteins (IgA-)
Hypomagnesemia Drug poisonings (e.g., aspirin, ethylene glycol, methanol)
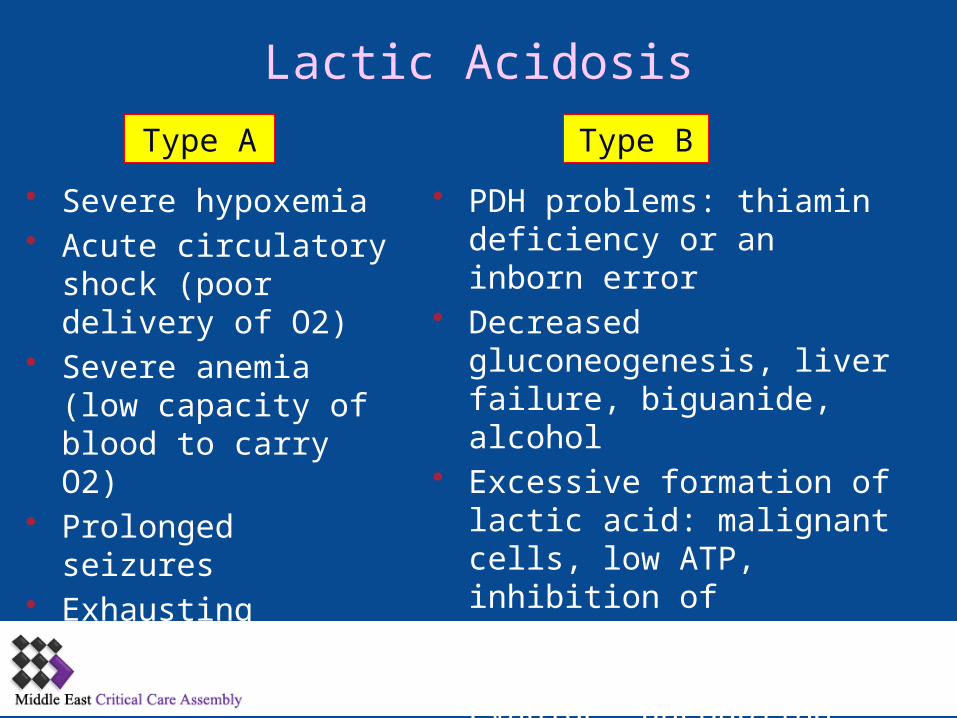
Lactic Acidosis
• Severe hypoxemia • Acute circulatory shock
)poor delivery of O2)• Severe anemia )low
capacity of blood to carry O2)
• Prolonged seizures• Exhausting exercise
• PDH problems: thiamin deficiency or an inborn error
• Decreased gluconeogenesis, liver failure, biguanide, alcohol
• Excessive formation of lactic acid: malignant cells, low ATP, inhibition of mitochondrial generation of ATP: cyanide, uncoupling oxidation and phosphorylation, alcohol intoxication
Type A Type B
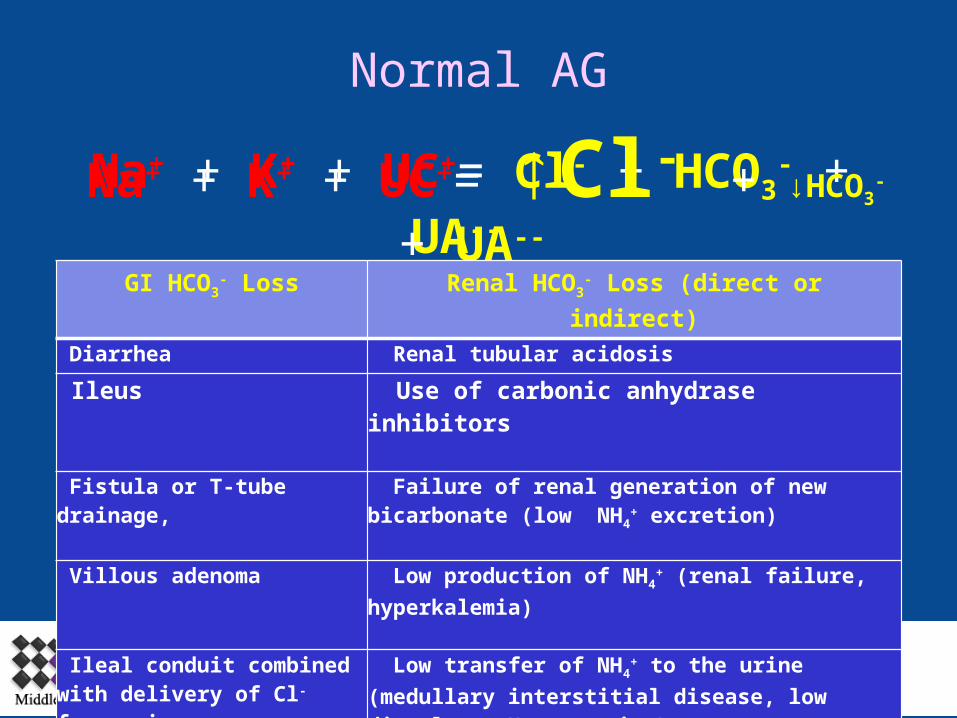
Normal AG
Na+ + K+ + UC+= Cl- + HCO3- + UA--
21
Na+ + K+ + UC+= ↑Cl- + ↓HCO3- + UA--
GI HCO3- Loss Renal HCO3
- Loss (direct or indirect)
Diarrhea Renal tubular acidosis
Ileus Use of carbonic anhydrase inhibitors
Fistula or T-tube drainage, Failure of renal generation of new bicarbonate (low NH4
+ excretion)
Villous adenoma Low production of NH4+ (renal failure,
hyperkalemia)
Ileal conduit combined with delivery of Cl- from urine
Low transfer of NH4+ to the urine (medullary
interstitial disease, low distal net H+ secretion)

Is it Mixed Disorder?
22
Tips to Diagnosing Mixed Acid-base Disorders
•Examine serum electrolytes: Na+, K+, Cl-, and CO2. •Normal pH in acid-base abnormality indicate mixed disease!•Calculate the expected compensatory values for the disorder and compare with actual •∆ ∆ in metabolic acidosis
24

Acute Respiratory Acidosis
~ ----------------------------- ↑1 mEq/LHCO3-
↑10 PaCO2 ↓0.07 pH
Chronic Respiratory Acidosis
~ ----------------------------- ↑3-4 mEq/LHCO3-
↑10 PaCO2 ↓0.03 pH

Acute Respiratory Alkalosis
~ ----------------------------- ↓2 mEq/LHCO3-
↓10 PaCO2 ↑0.08 pH
Chronic Respiratory Alkalosis
~ ----------------------------- ↓5 mEq/LHCO3-
↓10 PaCO2 ↑0.03 pH
Metabolic Acidosis
~ ----------------------------------- ↓HCO3-
∆PaCO2= [1.5 x serum CO2] + (8 ± 2)↓ pH
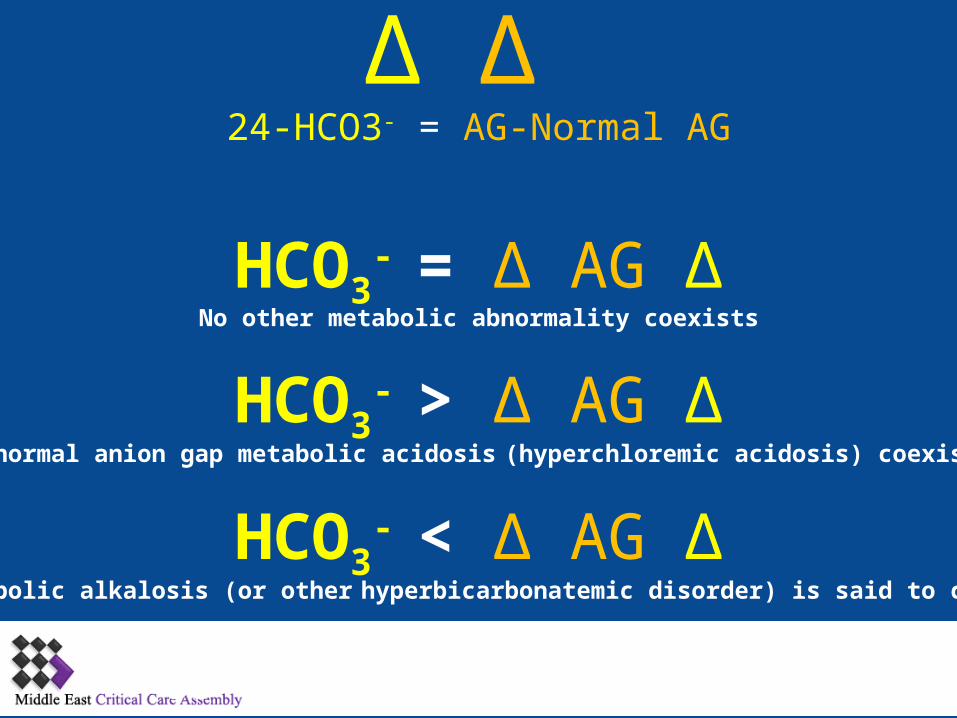
∆ ∆ 24-HCO3- = AG-Normal AG
33
∆HCO3- = ∆ AG
∆HCO3- > ∆ AG
∆HCO3- < ∆ AG
A normal anion gap metabolic acidosis (hyperchloremic acidosis) coexists
No other metabolic abnormality coexists
A metabolic alkalosis (or other hyperbicarbonatemic disorder) is said to coexist
Acid-base Disorders:
A patient’s arterial blood gas shows pH of 7.14, PaCO2 of 70 mm Hg, and HCO3
- of 23 mEq/L. How would you describe the likely acid-base disorder)s)?
1. Acute elevation of PaCO2 leads to reduced pH: acute respiratory acidosis.
2. For every 10-mm Hg rise in PaCO2 pH falls about 0.07 units. 3. Expected fall in pH: 0.21 thus pH should be = 7.194. Actual pH: 7.14 suggesting combined metabolic acidosis5. HCO3
- should be elevated 1 mEq/L for each 10 mm Hg= 3 mEq/L 6. Expected HCO3
- should be 27, actual is 23 suggesting combined metabolic acidosis
7. Decreased perfusion leading to mild lactic acidosis would explain the metabolic component.
Acid-base Disorders
A 45-year-old man comes to the hospital complaining of dyspnea for three days. Arterial blood gas reveals pH 7.35, PaCO2 60 mm Hg, PaO2 57 mm Hg, HCO3
- 31 mEq/L. How would you characterize his acid-base status?
1. Since the patient has been dyspneic for several days it is fair to assume a chronic acid-base disorder
2. For every 10-mm Hg rise in PaCO2 pH falls about 0.03 units. 3. Expected fall in pH: 0.06 thus pH should be = 7.344. Actual pH: 7.35 close to expected5. HCO3
- should be elevated 3-4 mEq/L for each 10 mm Hg= 3 mEq/L
6. Expected HCO3- should be 31
7. Actual is 31 as expected8. Chronic respiratory acidosis with adequate compensation
Acid-base Disorders
• 60 year old man with history of ethanol abuse was admitted to the hospital with severe acute pancreatitis.
• Developed progressive hypotension and respiratory failure and required intubattion and mechanical ventilation.
• He was sedated with lorazepam using bolus and infusion dosing and paralyzed using cis-atracurium.
• As a result of marked agitation, possibly associated with ethanol withdrawal, escalating doses of sedation were required.

Acid-base Disorders: Test Your Understanding
• Other medication included norepinephrine infusion, intravenous pantoprazole and piperacillin/tazobactam.
• On the 6th hospital day, WBC 21,000, Hg 106, Na 135, K 5, Cl 99, total CO2 15, BUN 12.5, creatinine 70 and glucose 18
• Plasma lactic acid was 4.7 mmol/L, serum osmolality 327 mOsm/kg H2O
• pH 7.26, PCO2 35 and PO2 126, ]H+[= 55
Acid-base Disorders: Test Your Understanding
a) Sepsis
b) Propylene glycol intoxication
c) Isopropyl alcohol intoxication
d) Ethylene glycol intoxication
e) Hypoventilation
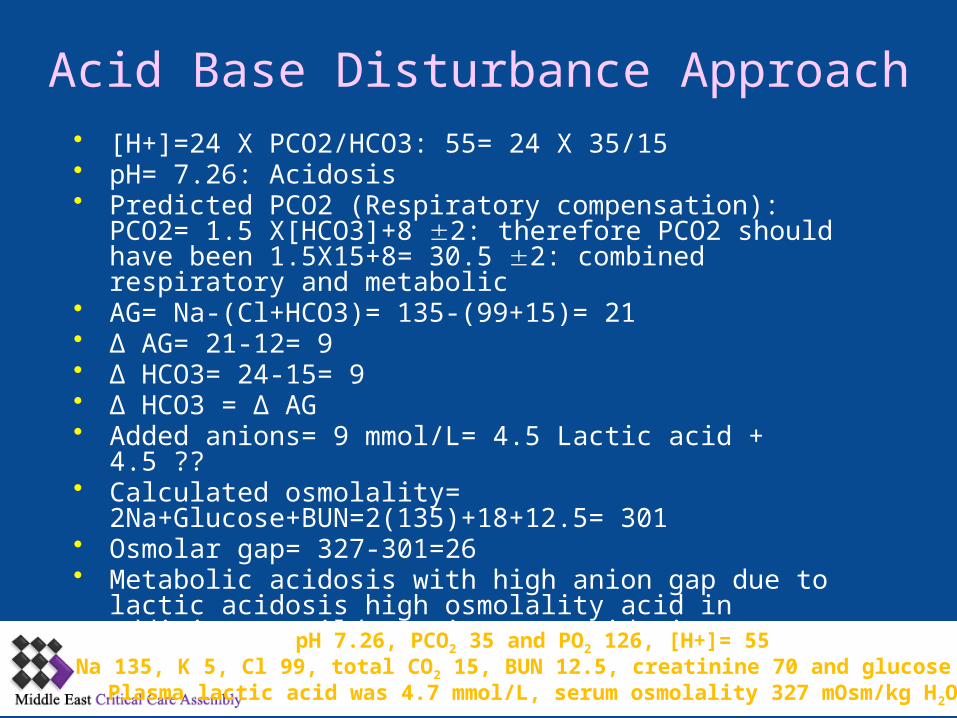
Acid Base Disturbance Approach• ]H+[=24 X PCO2/HCO3: 55= 24 X 35/15• pH= 7.26: Acidosis• Predicted PCO2 )Respiratory compensation): PCO2= 1.5
X]HCO3[+8 2: therefore PCO2 should have been 1.5X15+8= 30.5 2: combined respiratory and metabolic
• AG= Na-)Cl+HCO3)= 135-)99+15)= 21• ∆ AG= 21-12= 9• ∆ HCO3= 24-15= 9• ∆ HCO3 = ∆ AG• Added anions= 9 mmol/L= 4.5 Lactic acid + 4.5 ??• Calculated osmolality= 2Na+Glucose+BUN=2)135)+18+12.5=
301• Osmolar gap= 327-301=26• Metabolic acidosis with high anion gap due to lactic acidosis
high osmolality acid in addition to mild respiratory acidosis
pH 7.26, PCO2 35 and PO2 126, [H+]= 55Na 135, K 5, Cl 99, total CO2 15, BUN 12.5, creatinine 70 and glucose 18Plasma lactic acid was 4.7 mmol/L, serum osmolality 327 mOsm/kg H2O
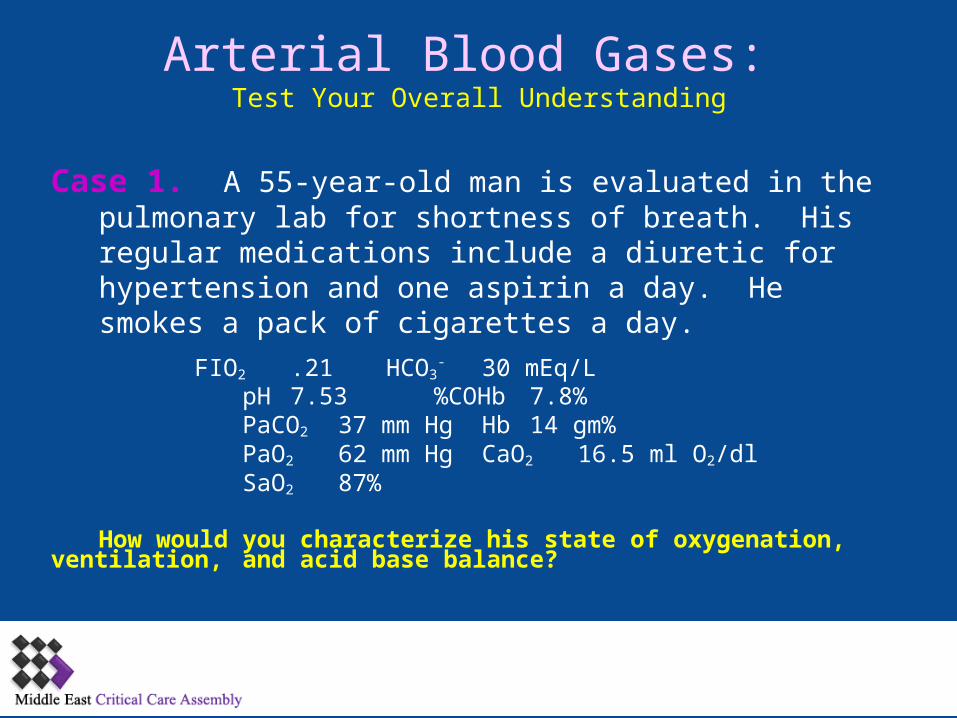
Arterial Blood Gases: Test Your Overall Understanding
Case 1. A 55-year-old man is evaluated in the pulmonary lab for shortness of breath. His regular medications include a diuretic for hypertension and one aspirin a day. He smokes a pack of cigarettes a day.
FIO2 .21 HCO3- 30 mEq/L
pH 7.53 %COHb 7.8%PaCO2 37 mm Hg Hb 14 gm%PaO2 62 mm Hg CaO2 16.5 ml O2/dlSaO2 87%
How would you characterize his state of oxygenation, ventilation, and acid base balance?
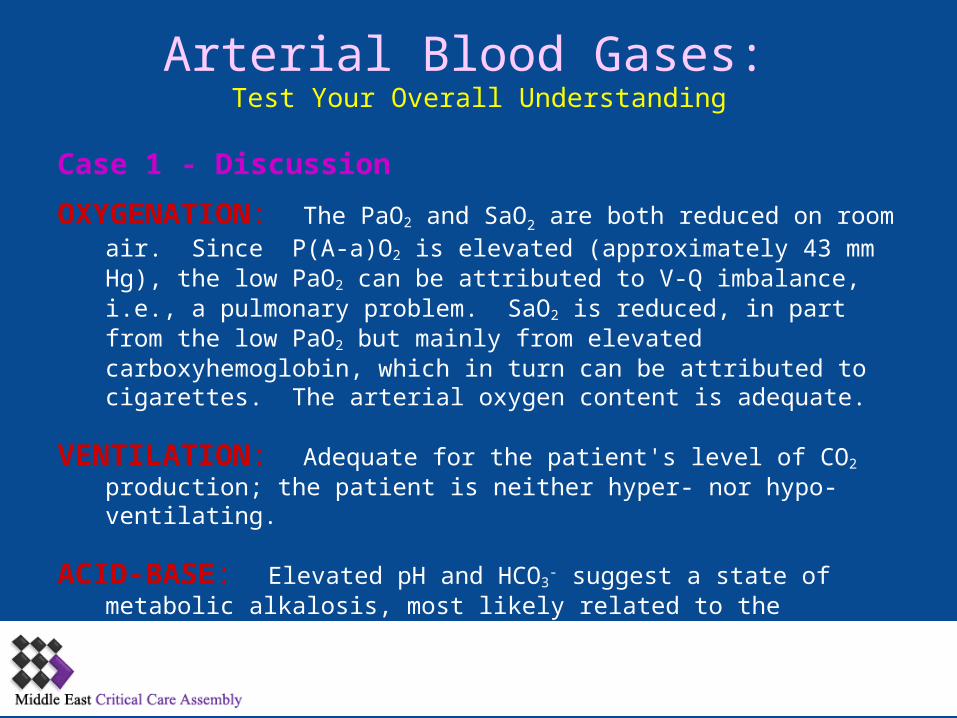
Arterial Blood Gases: Test Your Overall Understanding
Case 1 - Discussion
OXYGENATION: The PaO2 and SaO2 are both reduced on room air. Since P)A-a)O2 is elevated )approximately 43 mm Hg), the low PaO2 can be attributed to V-Q imbalance, i.e., a pulmonary problem. SaO2 is reduced, in part from the low PaO2 but mainly from elevated carboxyhemoglobin, which in turn can be attributed to cigarettes. The arterial oxygen content is adequate.
VENTILATION: Adequate for the patient's level of CO2 production; the patient is neither hyper- nor hypo-ventilating.
ACID-BASE: Elevated pH and HCO3- suggest a state of metabolic alkalosis,
most likely related to the patient's diuretic; his serum K+ should be checked
for hypokalemia.
Arterial Blood Gases: Test Your Overall Understanding
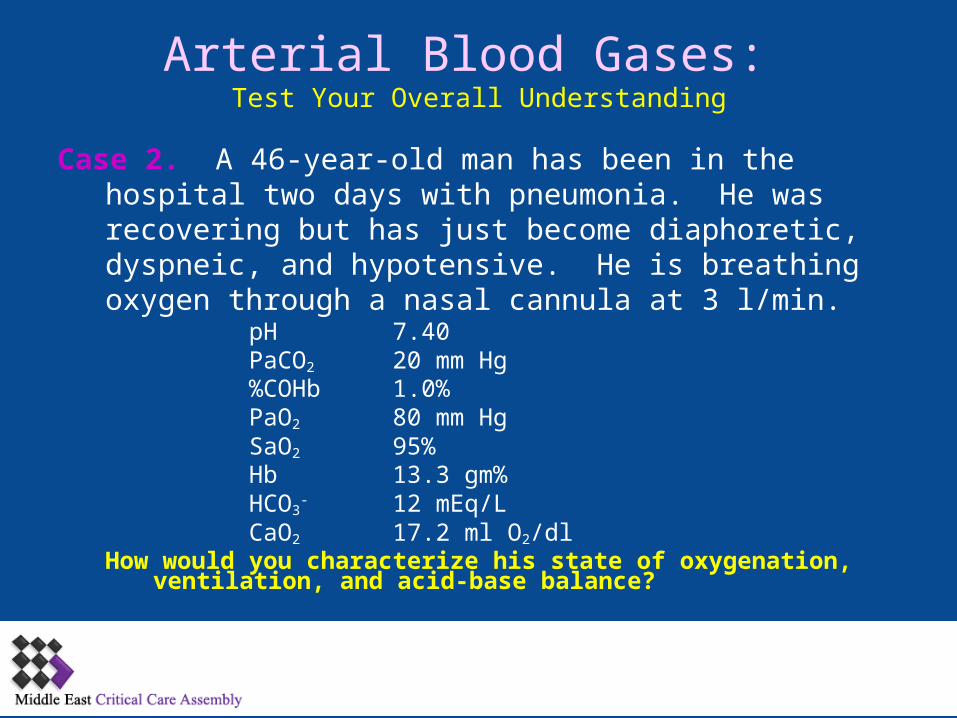
Case 2. A 46-year-old man has been in the hospital two days with pneumonia. He was recovering but has just become diaphoretic, dyspneic, and hypotensive. He is breathing oxygen through a nasal cannula at 3 l/min.
pH 7.40PaCO2 20 mm Hg%COHb 1.0%PaO2 80 mm HgSaO2 95% Hb 13.3 gm%HCO3
- 12 mEq/LCaO2 17.2 ml O2/dl
How would you characterize his state of oxygenation, ventilation, and acid-base balance?
Arterial Blood Gases: Test Your Overall Understanding
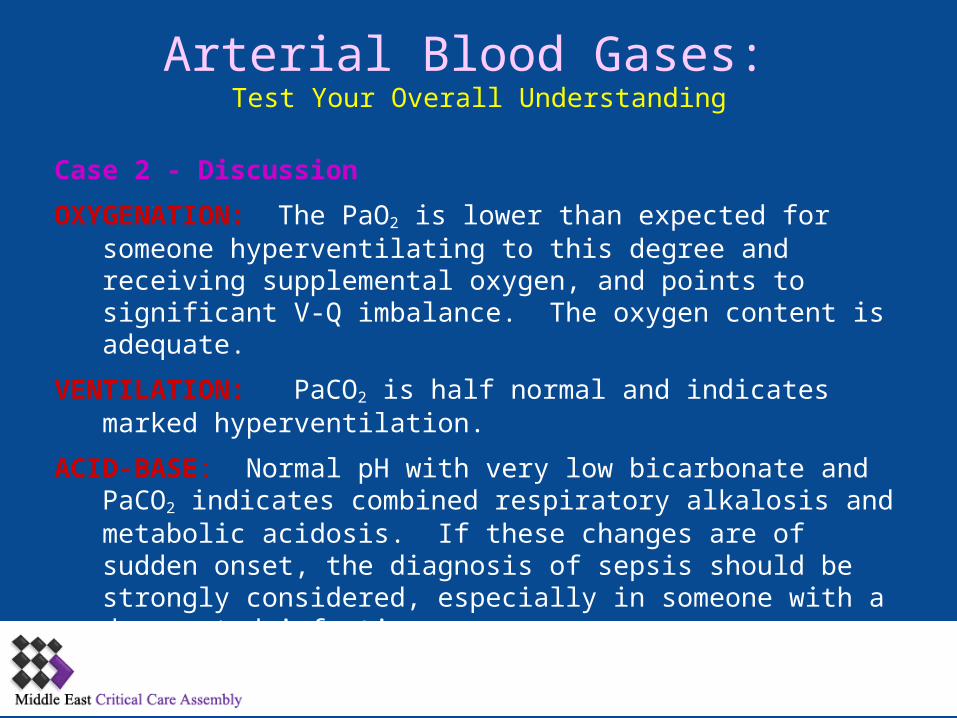
Case 2 - Discussion
OXYGENATION: The PaO2 is lower than expected for someone hyperventilating to this degree and receiving supplemental oxygen, and points to significant V-Q imbalance. The oxygen content is adequate.
VENTILATION: PaCO2 is half normal and indicates marked hyperventilation.
ACID-BASE: Normal pH with very low bicarbonate and PaCO2 indicates combined respiratory alkalosis and metabolic acidosis. If these changes are of sudden onset, the diagnosis of sepsis should be strongly considered, especially in someone with a documented infection.
Arterial Blood Gases: Test Your Overall Understanding
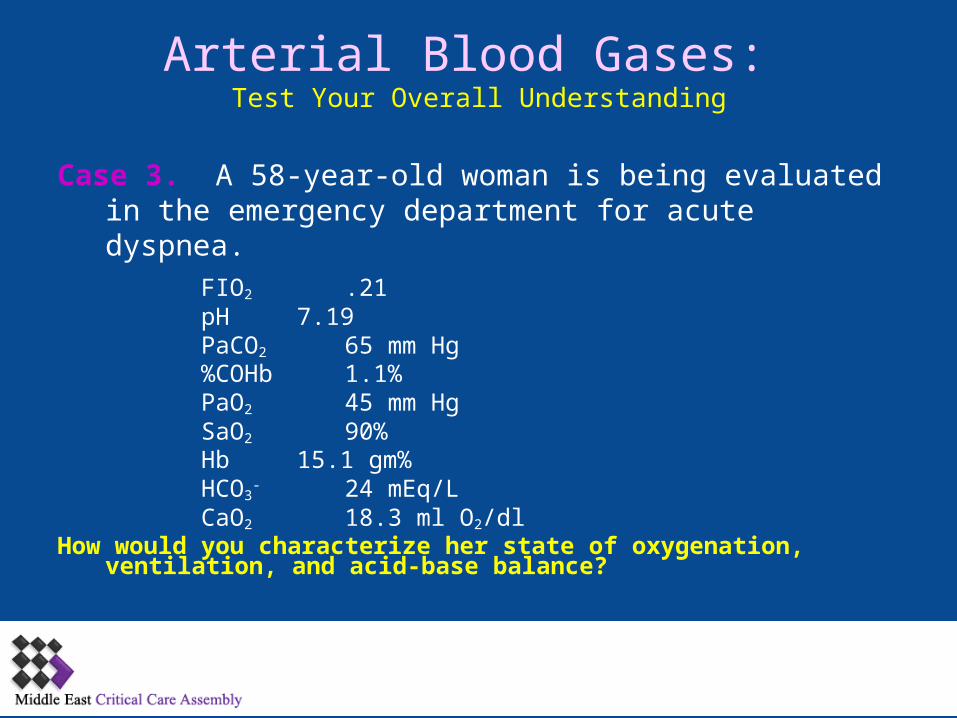
Case 3. A 58-year-old woman is being evaluated in the emergency department for acute dyspnea.
FIO2 .21pH 7.19PaCO2 65 mm Hg%COHb 1.1%PaO2 45 mm HgSaO2 90% Hb 15.1 gm%HCO3
- 24 mEq/LCaO2 18.3 ml O2/dl
How would you characterize her state of oxygenation, ventilation, and acid-base balance?
Arterial Blood Gases: Test Your Overall Understanding
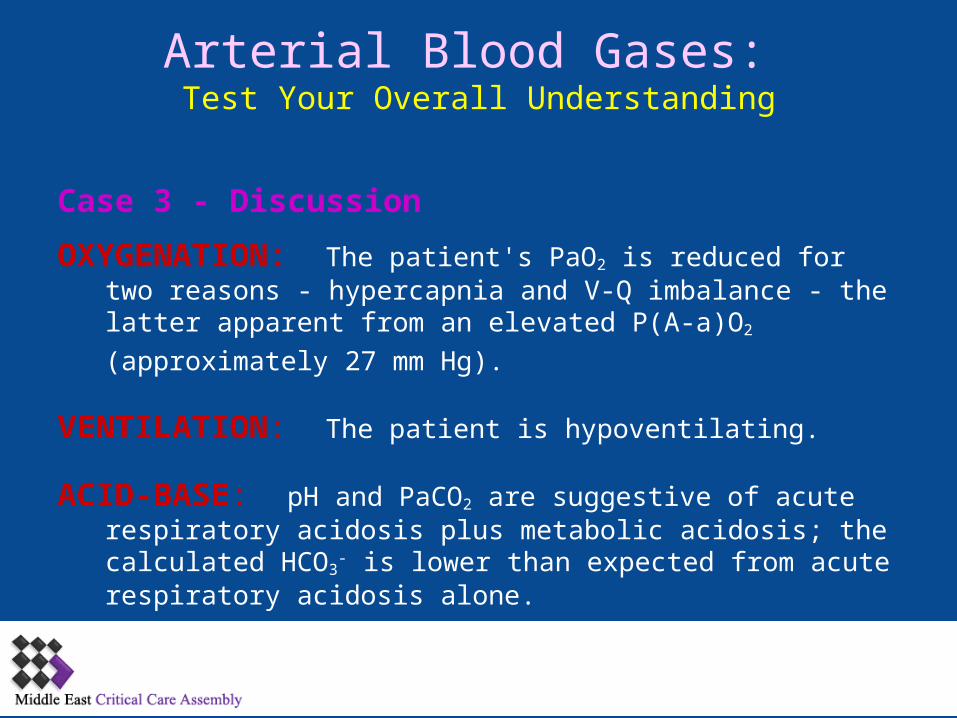
Case 3 - Discussion
OXYGENATION: The patient's PaO2 is reduced for two reasons - hypercapnia and V-Q imbalance - the latter apparent from an
elevated P)A-a)O2 )approximately 27 mm Hg).
VENTILATION: The patient is hypoventilating.
ACID-BASE: pH and PaCO2 are suggestive of acute respiratory acidosis plus metabolic acidosis; the calculated HCO3
- is lower than expected from acute respiratory acidosis alone.
Arterial Blood Gases: Test Your Overall Understanding
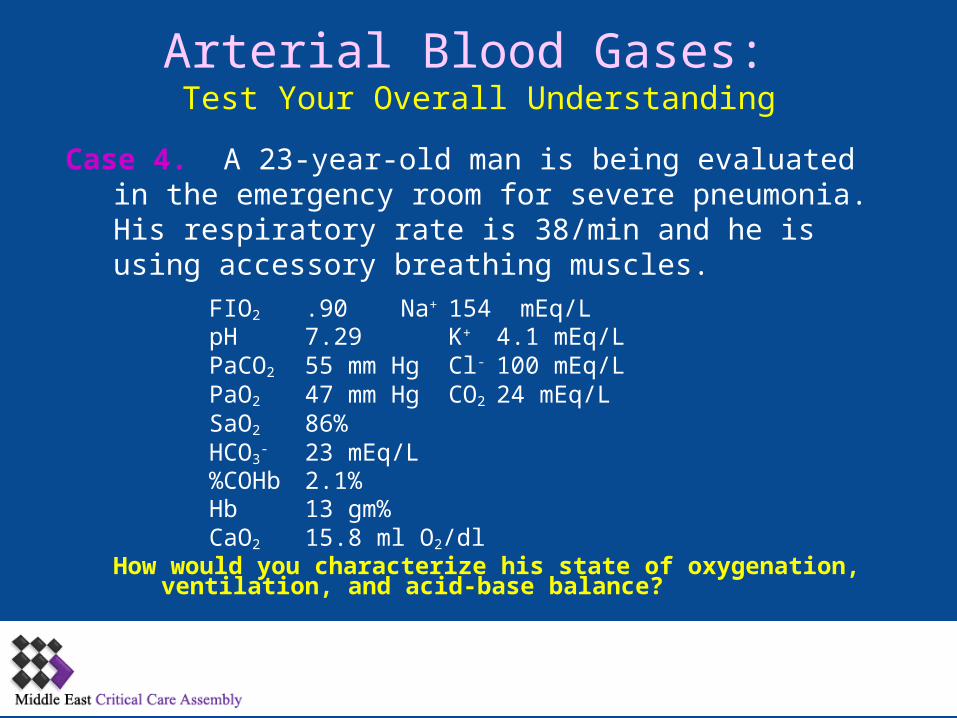
Case 4. A 23-year-old man is being evaluated in the emergency room for severe pneumonia. His respiratory rate is 38/min and he is using accessory breathing muscles.
FIO2.90 Na+ 154 mEq/LpH 7.29 K+ 4.1 mEq/LPaCO2 55 mm Hg Cl- 100 mEq/LPaO2 47 mm Hg CO2 24 mEq/LSaO2 86% HCO3
- 23 mEq/L%COHb 2.1%Hb 13 gm%CaO2 15.8 ml O2/dl
How would you characterize his state of oxygenation, ventilation, and acid-base balance?
Arterial Blood Gases: Test Your Overall Understanding
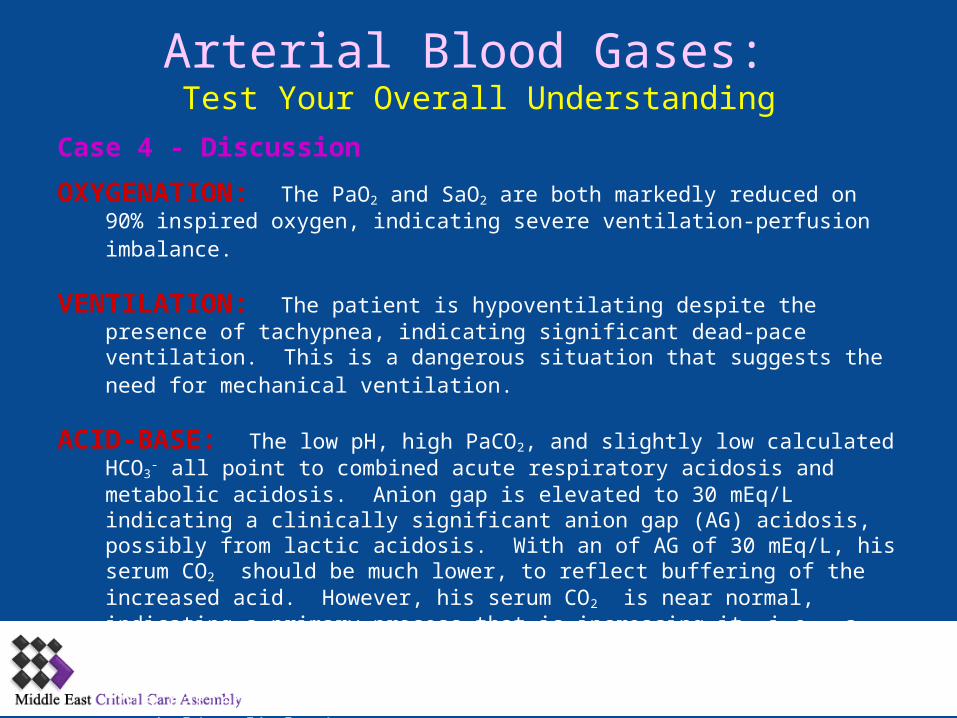
Case 4 - Discussion
OXYGENATION: The PaO2 and SaO2 are both markedly reduced on 90% inspired oxygen, indicating severe ventilation-perfusion imbalance.
VENTILATION: The patient is hypoventilating despite the presence of tachypnea, indicating significant dead-pace ventilation. This is a dangerous situation that suggests the need for mechanical ventilation.
ACID-BASE: The low pH, high PaCO2, and slightly low calculated HCO3- all point to
combined acute respiratory acidosis and metabolic acidosis. Anion gap is elevated to 30 mEq/L indicating a clinically significant anion gap )AG) acidosis, possibly from lactic acidosis. With an of AG of 30 mEq/L, his serum CO2 should be much lower, to reflect buffering of the increased acid. However, his serum CO2 is near normal, indicating a primary process that is increasing it, i.e., a metabolic alkalosis in addition to a metabolic acidosis. The cause of the alkalosis is as yet undetermined. In summary: this patient has respiratory acidosis, metabolic acidosis, and metabolic alkalosis.

50 Thank You















![To do list: Read chapter 2, work problems –Working with molarity, pH, especially –Look at Henderson-Hasselbalch pH = pK a + log([base]/[acid]) Work on.](https://static.fdocuments.net/doc/165x107/56649e3b5503460f94b2e205/to-do-list-read-chapter-2-work-problems-working-with-molarity-ph-especially.jpg)
![Mehrprotonige Säuren (z.B. H2SO4 - uni-marburg.de · [konjugierte Base] pH = pKs + log [konjugierte Säure] Puffergleichung (Henderson-Hasselbalch-Gleichung) Für ein Puffersystem](https://static.fdocuments.net/doc/165x107/5e04c249f3dd6d22fb271ad2/mehrprotonige-suren-zb-h2so4-uni-konjugierte-base-ph-pks-log-konjugierte.jpg)
