Hemodynamic monitoring and Shock Dr. Mohammad Aljawadi PharmD, Msc, PhD PHCL 477 Clinical Pharmacy...
68
Hemodynamic monitoring and Shock Dr. Mohammad Aljawadi PharmD, Msc, PhD PHCL 477 Clinical Pharmacy Department College of Pharmacy King Saud University April 2015 1
-
Upload
margaret-rodgers -
Category
Documents
-
view
235 -
download
0
Transcript of Hemodynamic monitoring and Shock Dr. Mohammad Aljawadi PharmD, Msc, PhD PHCL 477 Clinical Pharmacy...
Hemodynamic monitoring and Shock
Dr. Mohammad Aljawadi PharmD, Msc, PhD
PHCL 477
Clinical Pharmacy Department
College of Pharmacy
King Saud University
April 2015
1

2
3
What is Shock?
Inadequate tissue
perfusion
Cellular Injury
Organ Dysfunction
4
To understand the hemodynamics of shock we need:
To understand the basics of hemodynamics
What is a pulmonary artery catheter and how it is used
Let us start with the latter and go back to the former later
5
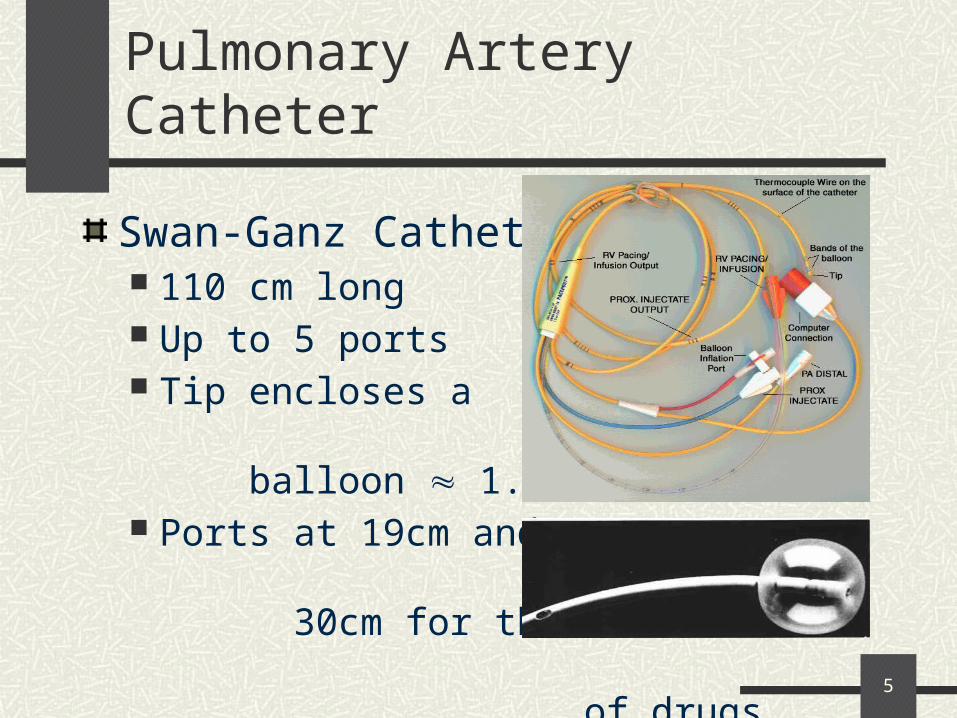
Pulmonary Artery Catheter
Swan-Ganz Catheter 110 cm long Up to 5 ports Tip encloses a
balloon 1.5 mL Ports at 19cm and
30cm for the infusion of drugs.
6
Pulmonary Artery Catheter
Indications Myocardial infarction with
shock/hypotension. Intraoperative cardiac or
vascular surgery patients. Severe trauma.
Relative Indications CHF Pulmonary hypertension Neurosurgical procedures Sepsis/septic shock Respiratory failure
• Uses– Establish Diagnosis– Guide therapies– Monitor Treatment– Assess O2 delivery
7
Central Venous Access Complications
Line sepsisThrombosisPneumothoraxHemothoraxArrhythmias (Swan-Ganz)Air EmbolusInfarctionCatheter Knotting (Swan-Ganz)
8
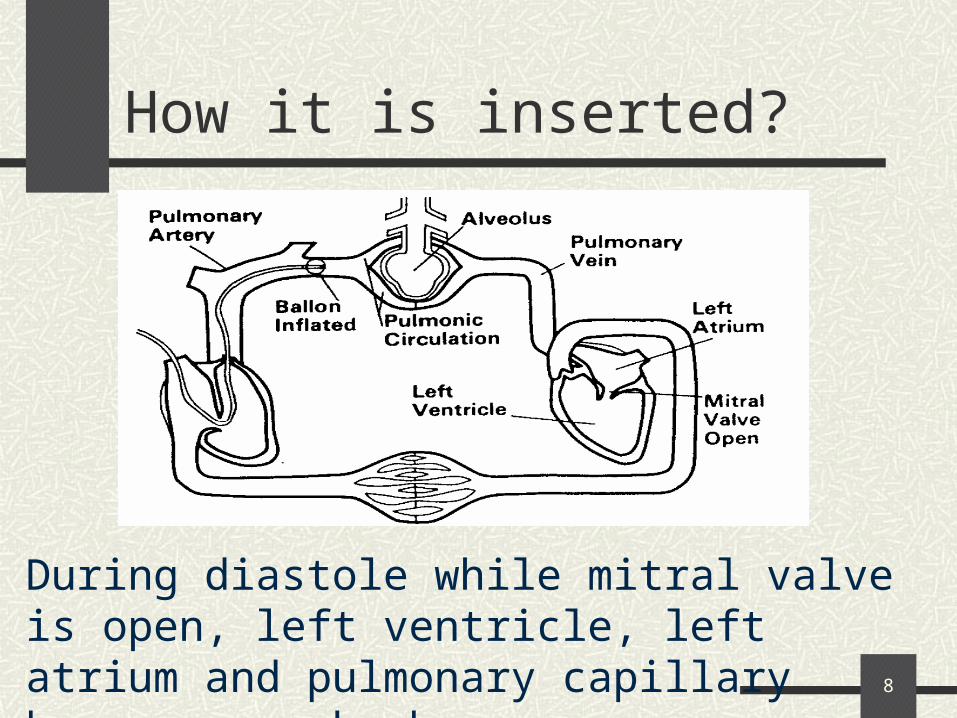
How it is inserted?
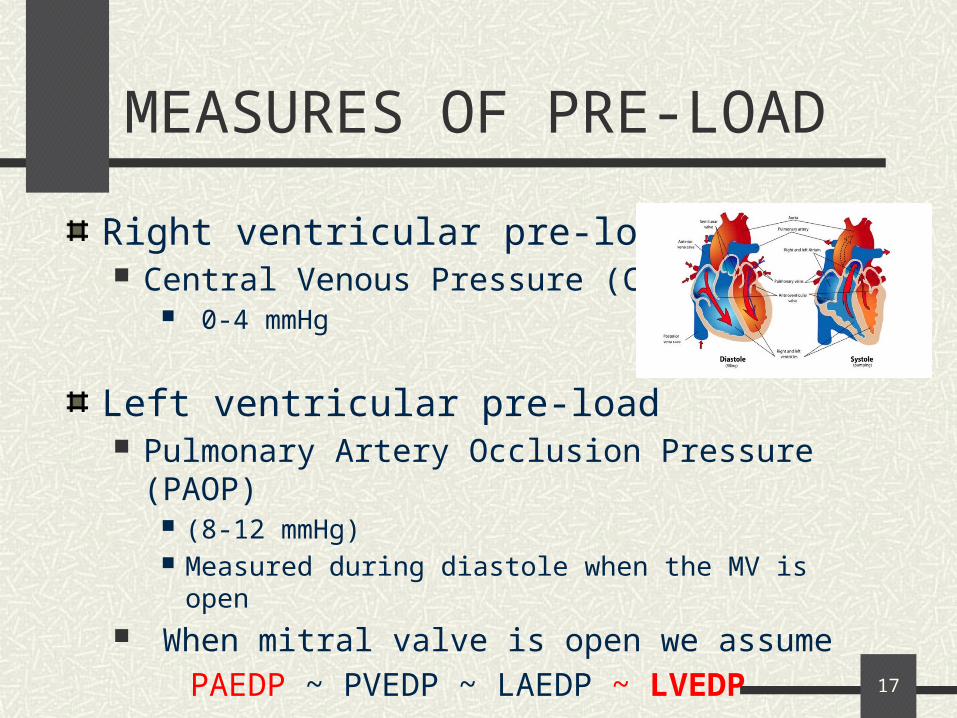
During diastole while mitral valve is open, left ventricle, left atrium and pulmonary capillary become one chamber.
9
The Basics of Hemodynamics
Blood Pressure
Cardiac Output
Systemic vascular resistance
Stroke Volume
Heart rate
Pre-load
After-load
Contractility
10
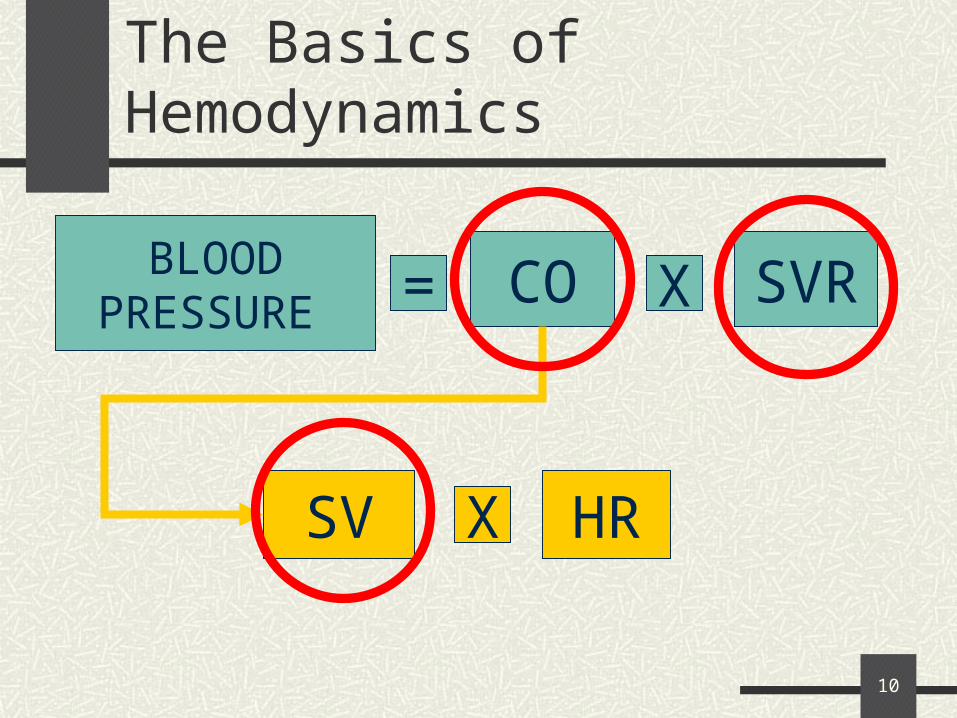
The Basics of Hemodynamics
BLOODPRESSURE
CO= X SVR
SV X HR
11
The Basics of Hemodynamics
Cardiac Output (CO) Amount of blood that is pumped out of the heart in one
minute. 5.6 L/min for a human male and 4.9 L/min for a female
Stroke Volume The quantity of blood pumped out of the ventricles with
every heart beat. ~ 70 mL in a healthy 70-kg man
12
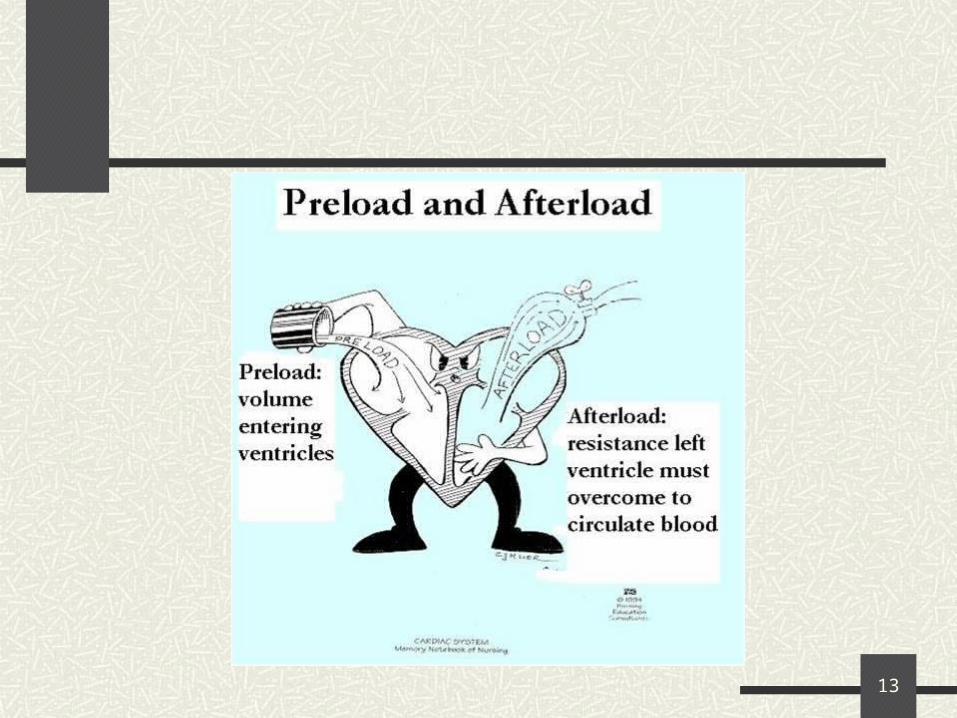
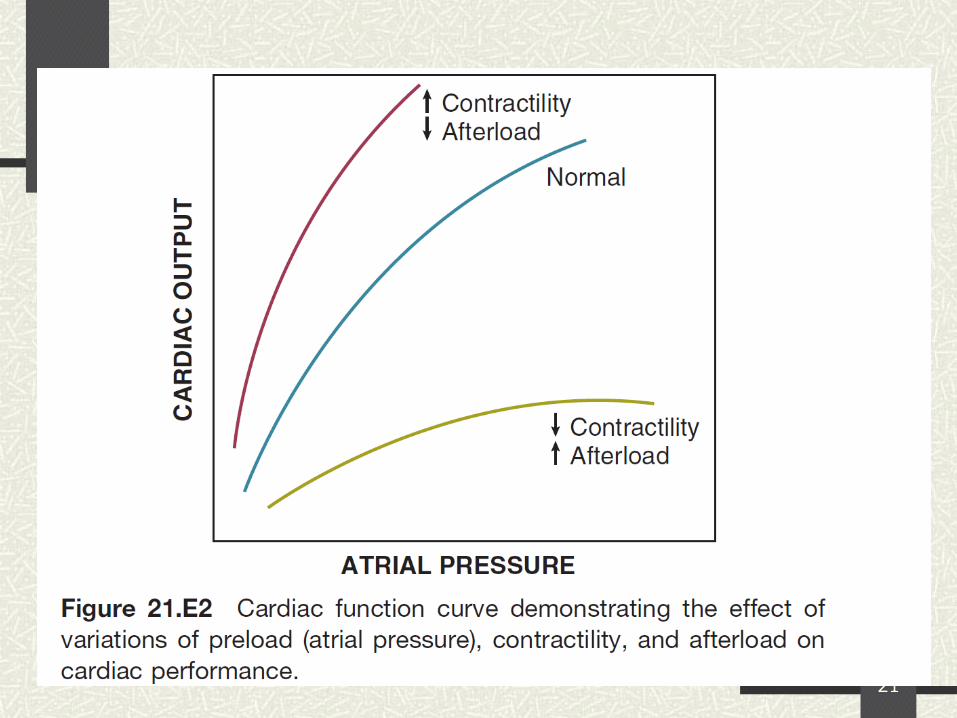
Determinants of stroke volume
PRELOAD
AFTERLOAD
CONTRACTILITY
13
14
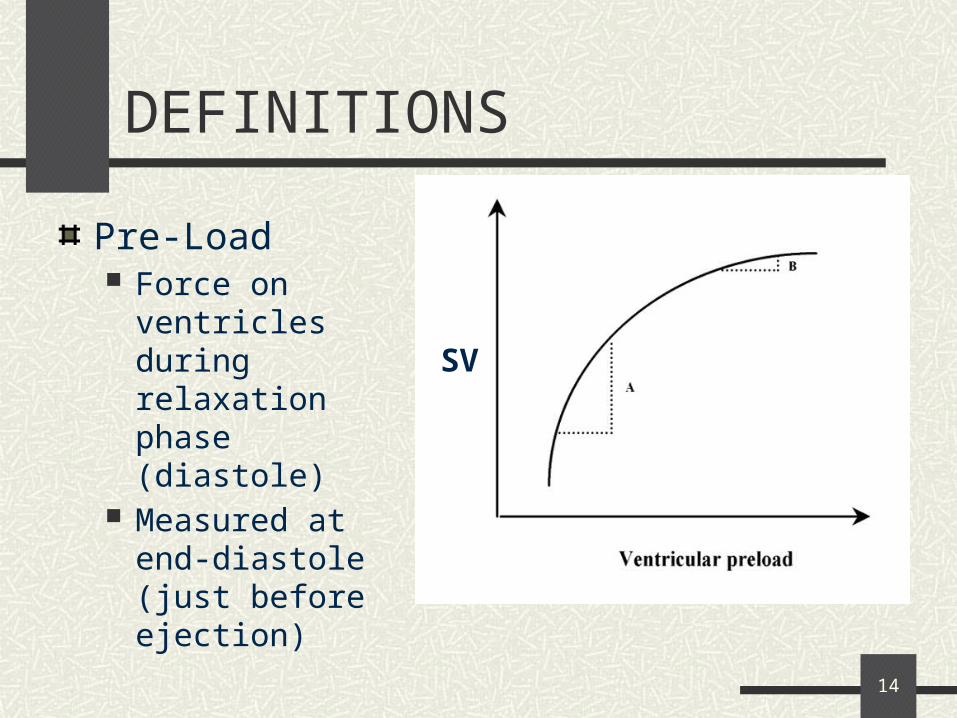
DEFINITIONS
Pre-Load Force on ventricles
during relaxation phase (diastole)
Measured at end-diastole (just before ejection)
SV
15
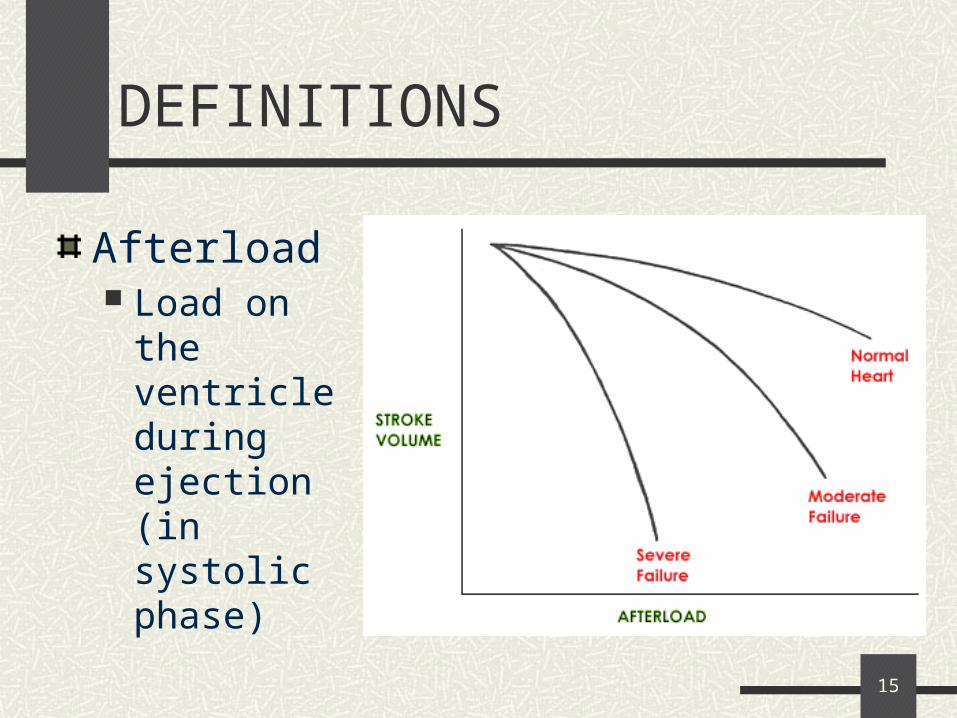
DEFINITIONS
Afterload Load on the
ventricle during ejection (in systolic phase)
16
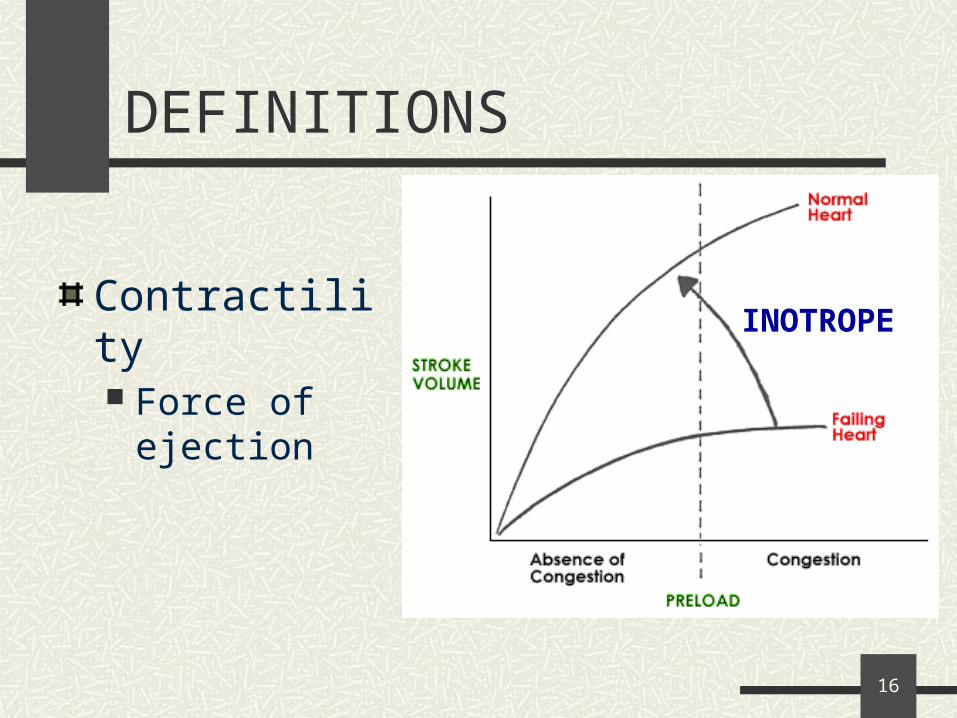
DEFINITIONS
Contractility Force of ejection
INOTROPE
17
MEASURES OF PRE-LOAD
Right ventricular pre-load Central Venous Pressure (CVP)
0-4 mmHg
Left ventricular pre-load Pulmonary Artery Occlusion Pressure (PAOP)
(8-12 mmHg) Measured during diastole when the MV is open
When mitral valve is open we assume
PAEDP ~ PVEDP ~ LAEDP ~ LVEDP
18
Normally, PAOP approximates left atrial pressure, which in turn approximates left ventricular end-diastolic pressure (LVEDP).
LVEDP reflects left ventricular end-diastolic volume (LVEDV).
LVEDV is the actual target
MEASURES OF PRE-LOAD
19
MEASURES OF AFTERLOAD
Afterload on Right Ventricle Pulmonary Vascular Resistance
PVR =MPAP – PAWP x 80 (20-120 dyne x sec / cm-5)
CO
Afterload on Left Ventricle Systemic Vascular Resistance SVR = MAP – CVP x 80 (800-1200 dyne x sec / cm-
5)
CO
MAP = SBP + 2(DBP)
3
20
CONTRACTILITY
CO = SV x HR
CARDIAC OUTPUT (4-7 L/min) Thermodilution: a thermistor near the end of the
catheter injects cold saline into the bloodstream and the temperature change determines CO
CARDIAC INDEX = CO/BSA (2.8-3.6 L/min/m2)
21

22
OXYGEN DEMANDOXYGEN SUPPLY
23
OXYGEN SUPPLY
DO2 = CO X CaO2 (arterial O2 content)
CO = SV x HR CaO2 determined by:
HgB SaO2
24
OXYGEN DEMAND
Determined by metabolic activity of tissues
O2 extraction Usually about 25% for the entire body CvO2 determined by:
HgB SvO2 (60-75%)
SvO2 = increased oxygen consumption• Either decreased delivery, or increased demands• Examples???
25
A word about O2 monitoring
Oxygen Saturation(SpO2)
normal > 90% Non-invasive
Mixed venous oxygen saturation(SvO2)
Normal 65%-75%invasive
26
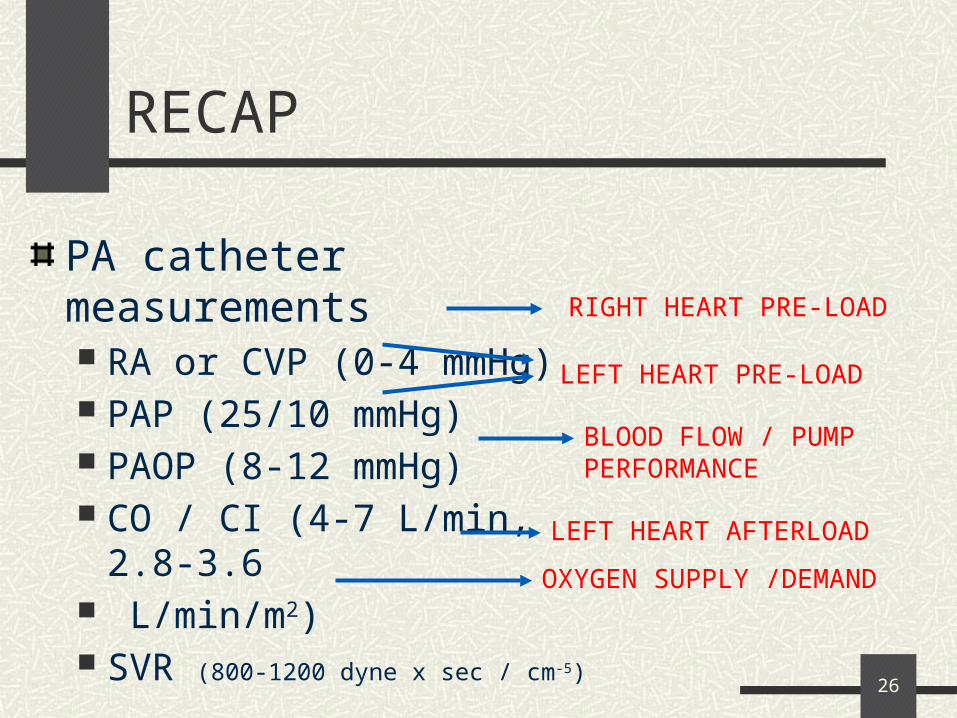
RECAP
PA catheter measurements RA or CVP (0-4 mmHg) PAP (25/10 mmHg) PAOP (8-12 mmHg) CO / CI (4-7 L/min, 2.8-3.6 L/min/m2) SVR (800-1200 dyne x sec / cm-5)
SvO2 (65-75%)
RIGHT HEART PRE-LOAD
BLOOD FLOW / PUMP PERFORMANCE
LEFT HEART AFTERLOAD
OXYGEN SUPPLY /DEMAND
LEFT HEART PRE-LOAD
27
SHOCK IN THE ICU
28
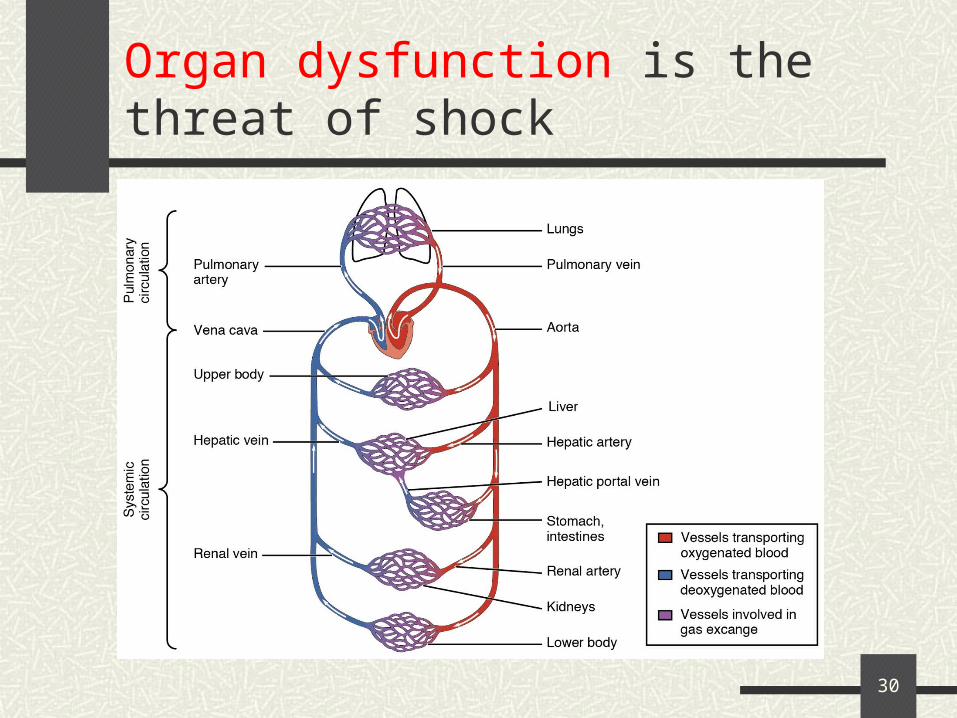
What is Shock?
Inadequate tissue perfusion resulting in cellular injury.
This causes the release of inflammatory mediators that further compromise tissue perfusion, resulting in organ failure and death unless quickly corrected
Circulating volume must be identified and expanded quickly, and the underlying pathological process must be controlled.
29
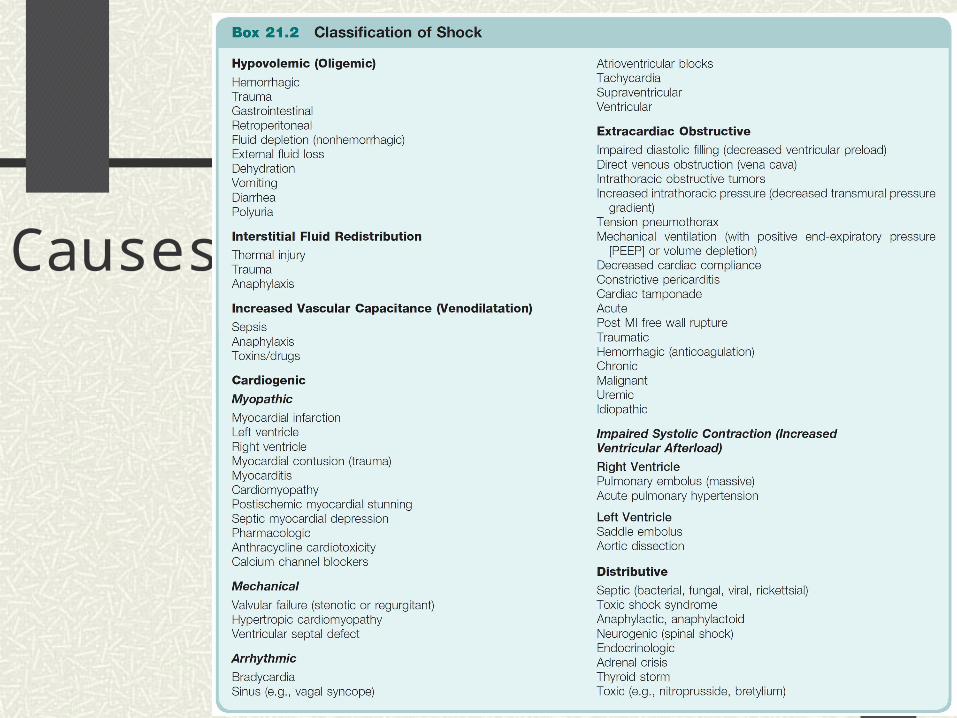
Classification of Shock
Hypovolemic Shock
Cardiogenic Shock
Distributive Shock
Extra-cardiac Obstructive Shock
30
Organ dysfunction is the threat of shock
31
Hypovolemic Shock
Results fromLoss of blood or fluid.
Decreased circulating blood volume decrease in diastolic filling pressure and volume
inadequate CO, hypotension, and shock
32
Hypovolemic Shock
Causes: dehydration, hemorrhage, gastrointestinal fluid
losses, urinary losses, or decreased vascular permeability from sepsis
hypotension with signs of shock indicating tissue hypo-perfusion, activation of the inflammatory cascade, and widespread cellular damage
33
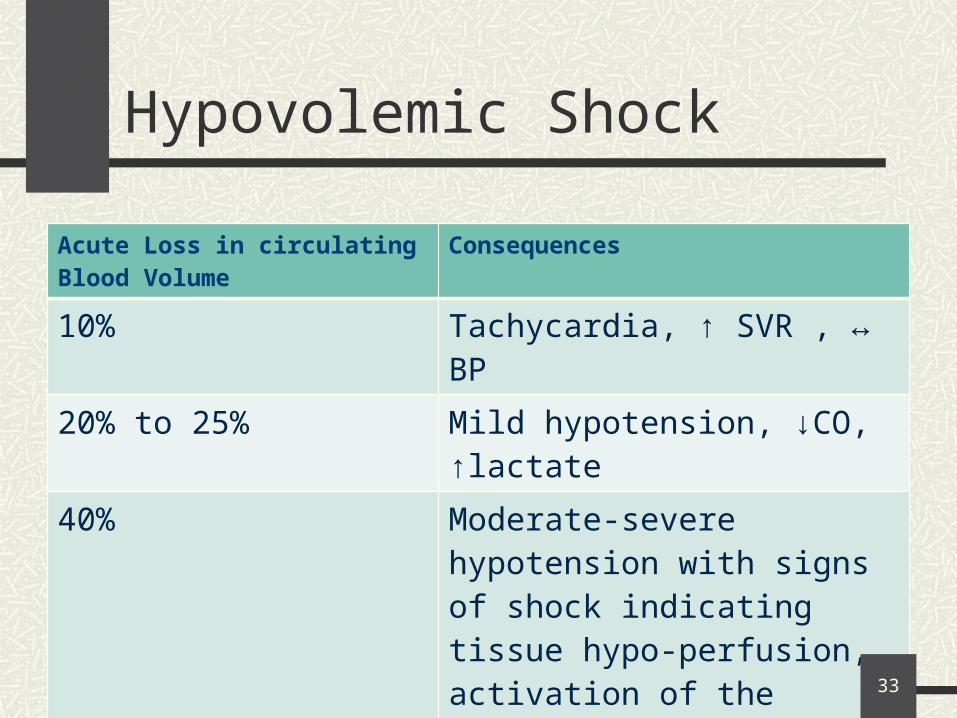
Hypovolemic Shock
Acute Loss in circulating Blood Volume
Consequences
10% Tachycardia, ↑ SVR , ↔ BP
20% to 25% Mild hypotension, ↓CO, ↑lactate
40% Moderate-severe hypotension with signs of shock indicating tissue hypo-perfusion, activation of the inflammatory cascade, and widespread cellular damage
34
Cardiogenic Shock
Myocardial damage or cardiac mechanical abnormality
Reduced cardiac functionDecrease in cardiac output and blood
pressure Shock
35
Cardiogenic Shock
Causes: Q-wave myocardial infarctions.
Special signs: Patients have signs of heart failure, an S3,
elevated neck veins, and peripheral hypo-perfusion
36
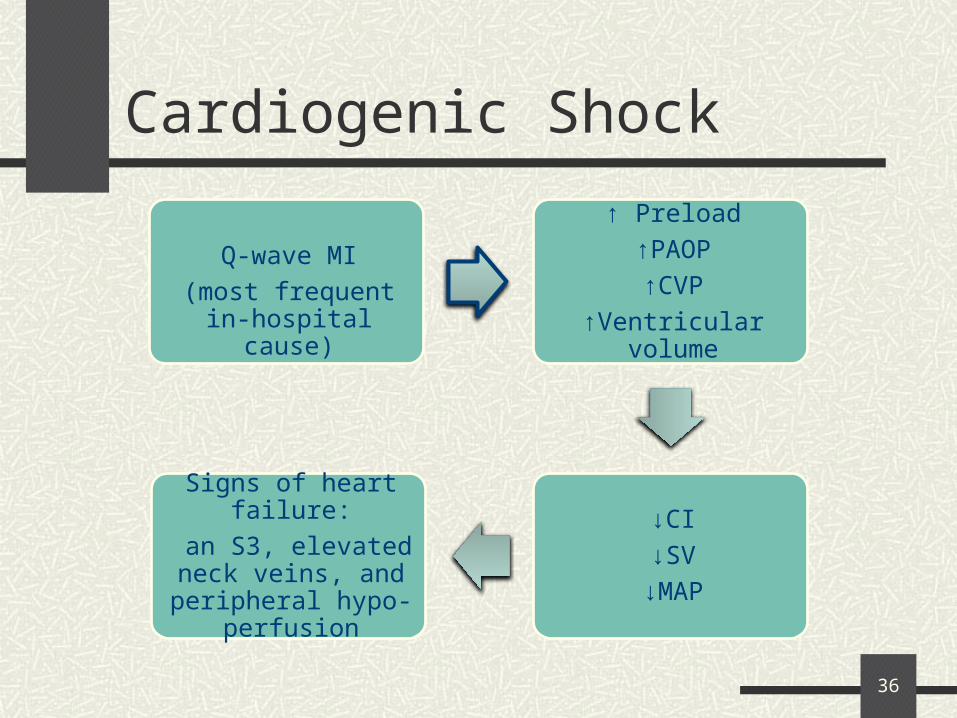
Cardiogenic Shock
Q-wave MI
(most frequent in-hospital cause)
↑ Preload
↑PAOP
↑CVP
↑Ventricular volume
↓CI
↓SV
↓MAP
Signs of heart failure:
an S3, elevated neck veins, and peripheral
hypo-perfusion
37
Distributive Shock
Loss of peripheral resistance fluid leak to extracellular space
Vasodilation Decrease in preload Hypotension Normal or increased CO
Myocardial depression frequently accompanies distributive shock.
Decrease in SVR inadequate blood pressure shock and multi-organ dysfunction
38
Distributive Shock
Causes: Sepsis Anaphylaxis, drug overdose, neurogenic
causes, and Addisonian crisis
39
Extra-cardiac obstructive
Obstruction to flow in the cardiovascular circuit. inadequate diastolic filling or decreased systolic function secondary to an increase in afterload and a drop in CO and blood pressure
40
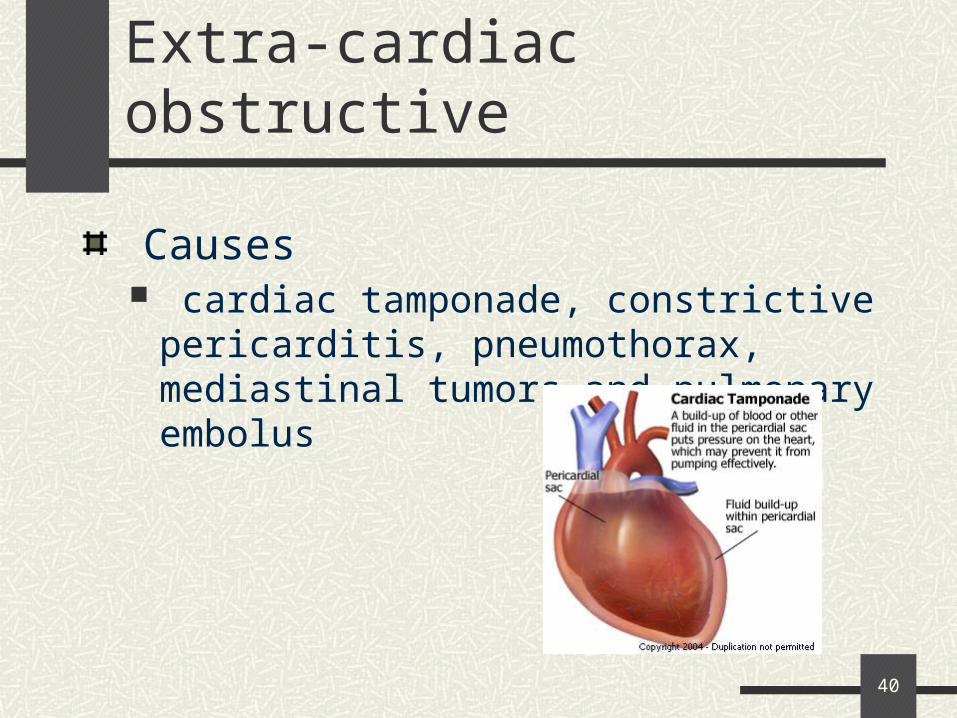
Extra-cardiac obstructive
Causes cardiac tamponade, constrictive pericarditis,
pneumothorax, mediastinal tumors and pulmonary embolus
41
Tip of the mountain
42
Causes:
43
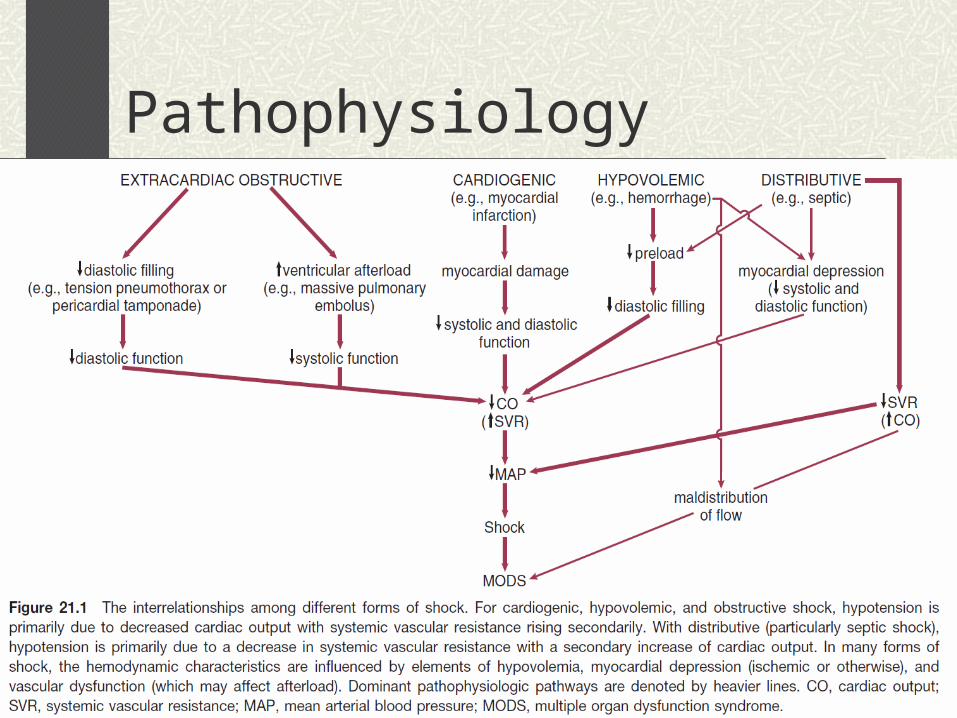
Pathophysiology
44
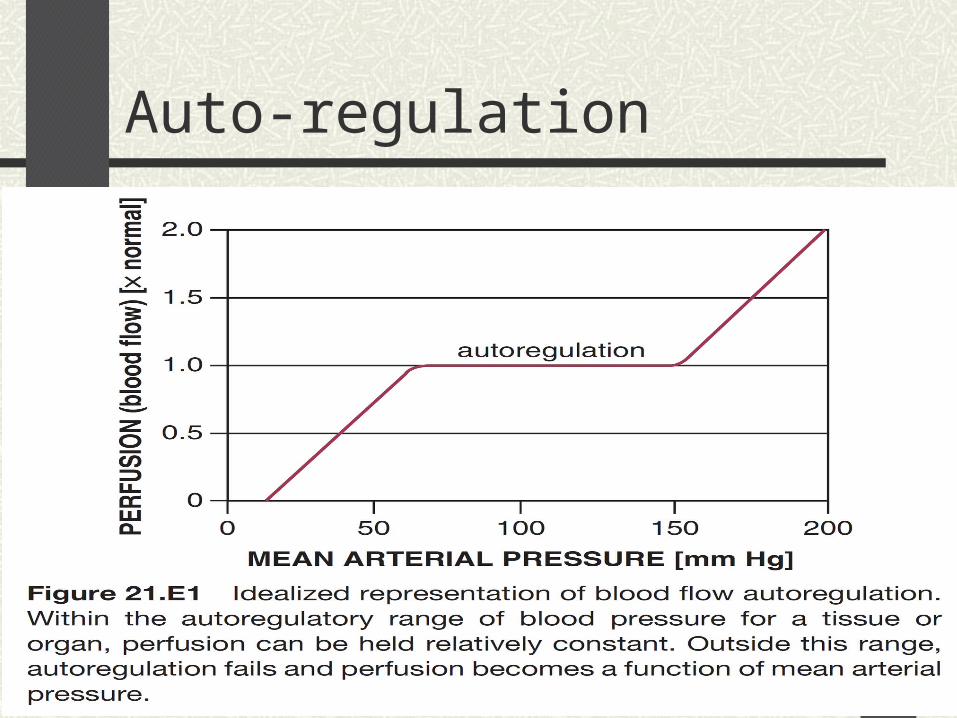
Auto-regulation
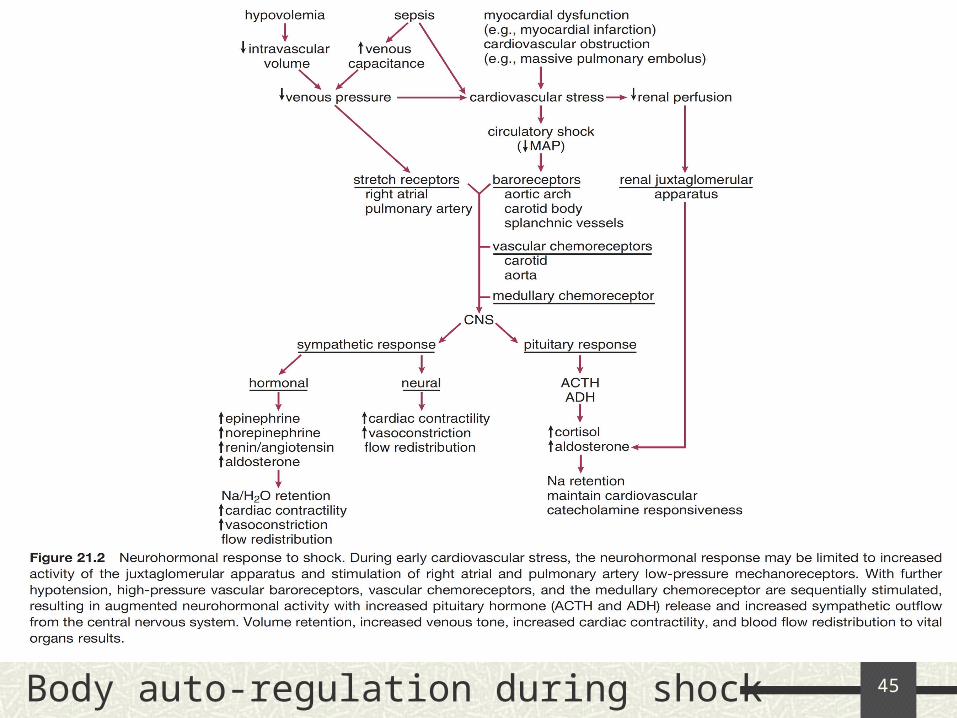
45Body auto-regulation during shock
46
Manifestations of shock
CNS: Alerted level of consciousness from confusion
to coma Ischemia
47
Manifestations of shock
CVS: Hypotension
Decreased coronary artery perfusion pressure Ischemia in patients with coronary artery disease
Tachycardia. (which type of shock is not associated with it?)
Contractility will increase in most typesCardiogenic
48
Manifestations of shock
Respiratory: Increase in minute ventilation
Hypocapnia
Severe hypo-perfusion Respiratory muscle weakness
Respiratory alkalosis
Respiratory Failure
49
Renal: Because of auto-regulation glomerular filtration
is maintained by efferent arteriole constriction Late in shock:
Cortical and medullary ischemia tubular necrosis
↓ urine output followed by ↑ BUN and SCr
Manifestations of shock
50
Manifestations of shock
GI: Very sensitive to sympathetic vasoconstriction:
Ileus Gastritis Pancreatitis Acalculous cholecystitis (not due to stone gallbladder inflammation)
Colonic submucosal hemorrhage Ischemia of the gut can lead to translocation of
bacteria from the gut to the circulation
51
Liver: LFTs elevations
Hematological: Disseminated intravascular coagulation Dilutional thrombocytopenia due resuscitation
Metabolic: Hyperglycemia due ↓ insulin production Protein catabolism negative nitrogen balance
Manifestations of shock
52
Cardiogenic shock: jugular venous distension, an S3 and S4, and regurgitation murmurs.
Pulmonary embolus: patients present with hypoxia, dyspnea, and elevated right heart pressures.
Septic shock patients may have fevers, chills, and usually a nidus of infection ( a source of infection)
Manifestations of shock
53
Labs:
Low or high WBC count with a left shift and bands
High or normal hemoglobin levels
High to low platelets
Low serum bicarbonate
High anion gap
High or normal creatinine
High lactate
(unless hemorrhagic shock)
Why?
54
Hemodynamic monitoring:
Arterial pressure and CVP monitor vasopressors effect
Mixed venous oxygen saturation (Svo2) Normal 65%-75% Inversely proportional to perfusion level
Pulmonary artery catheter no evidence of decreased mortality
55
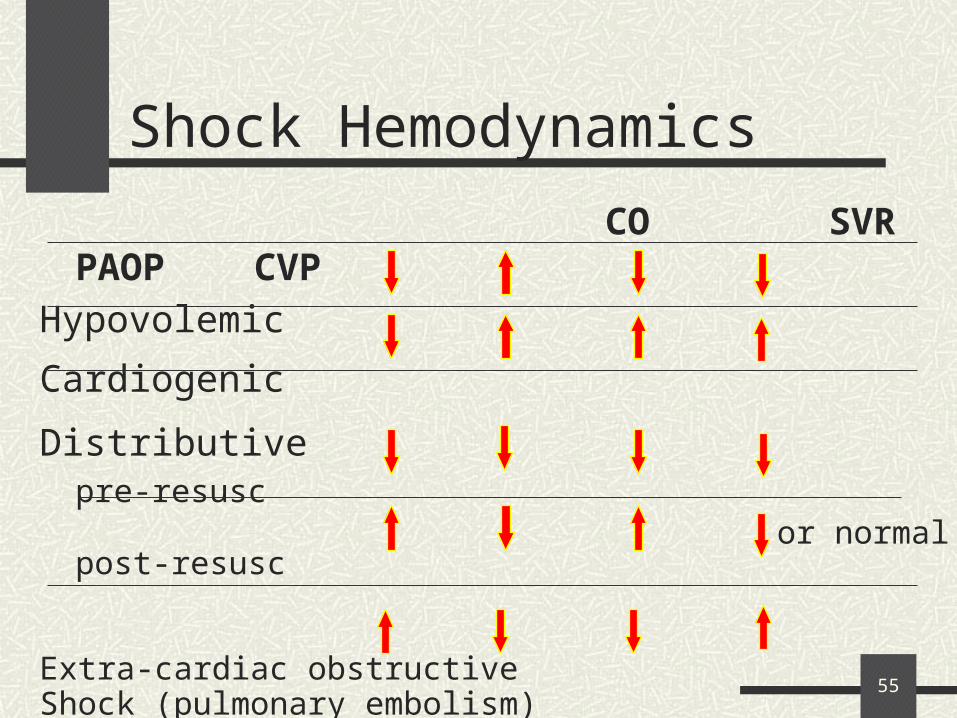
CO SVR PAOP CVP
Hypovolemic
Cardiogenic
Distributivepre-resusc
post-resusc
Extra-cardiac obstructiveShock (pulmonary embolism)
Shock Hemodynamics
or normal
56
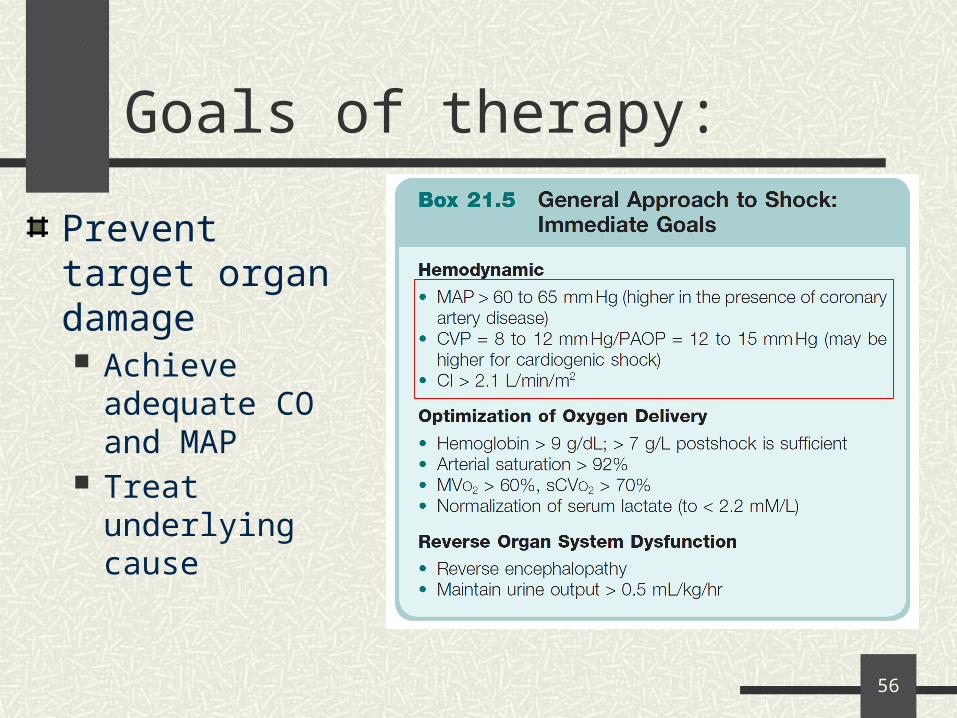
Goals of therapy:
Prevent target organ damage Achieve adequate
CO and MAP Treat underlying
cause
57
Therapy
Adequate oxygenation (mechanical ventilation) Goal: Oxygen saturation 90% or greater
Volume resuscitation Mainly crystalloids (NaCl 0.9%) Colloids
(Albumin) Good in severe sepsis
Hetastarch Limited use in renal failure

58
Therapy
Once volume resuscitation is optimized vasopressors and inotropes
What happened if you start with a vasopressor before fluid resuscitation?
59
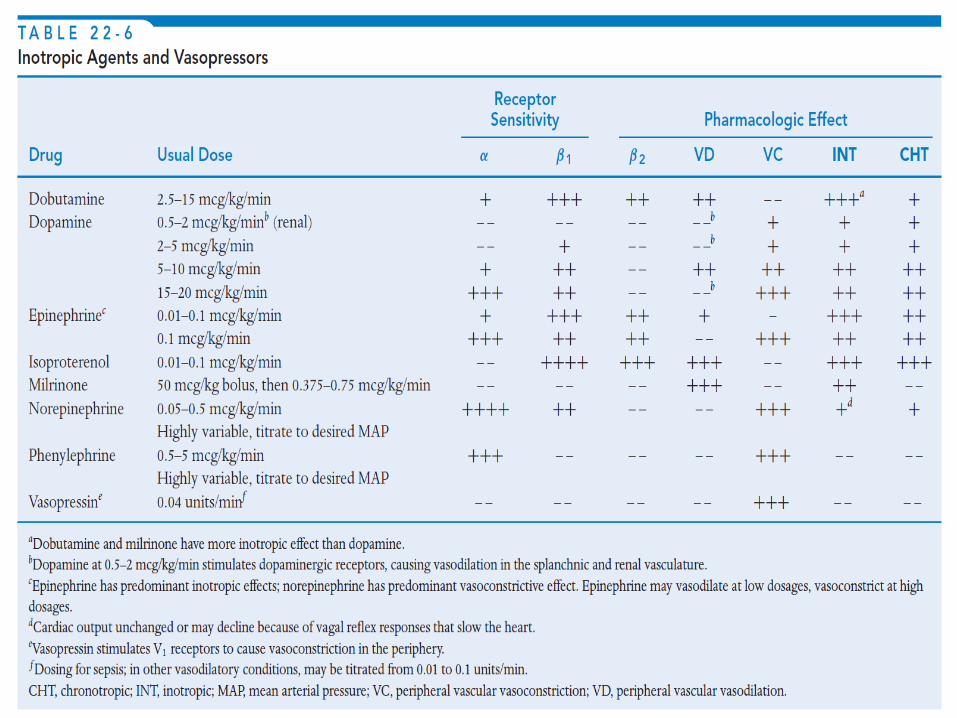
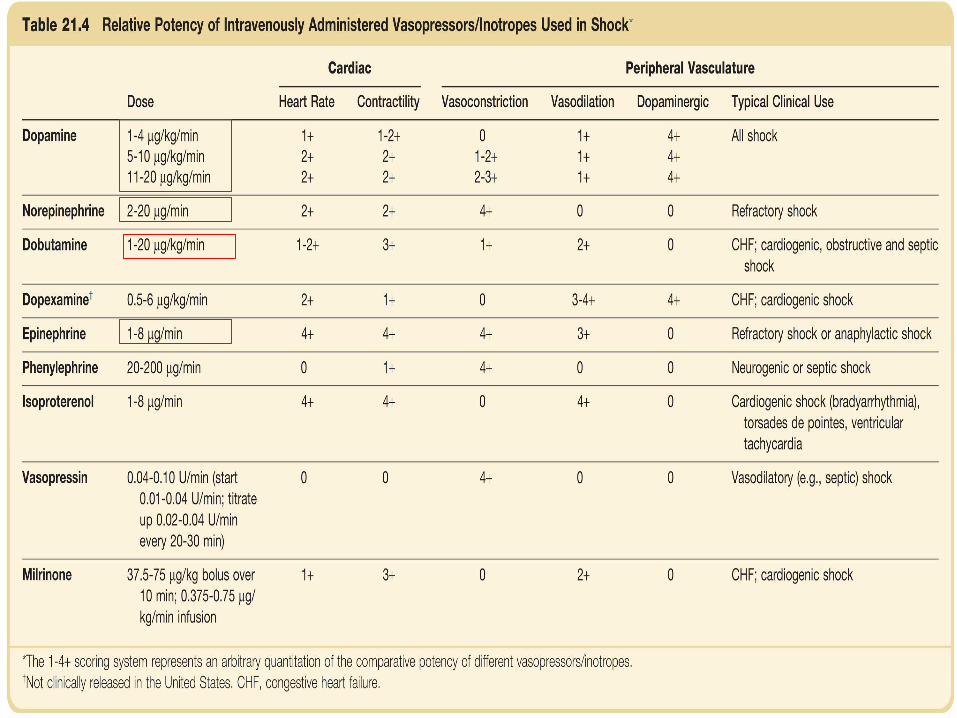
Vasopressors:
Norepinephrine: Reliable increase in blood pressure and
inotrope
Dopamine: Low dose: mild inotropic effect as well as some
renal effects. high dose: vasoconstriction Higher incidence of mesenteric ischemia than
norepinephrine
60
Vasopressors:
Epinephrine: 1st choice in anaphylactic shock Watch for:
Tachycardia and arrhythmia Mesenteric ischemia
Phenylephrine: Pure α-agonist
Good for patients with underlying tachycardia
61
Vasopressors:
Vasopressin: In refractory cases not responding to previous
vasopressors ↓ heart rate and cardiac output ↑ blood pressure and pulmonary artery pressure May lead to myocardial ischemia due a
decrease in coronary artery blood flow
62
Inotropes:
Dobutamine: β1 and β2 agonists
CO SVR
Milrinone: phosphodiesterase inhibitor It is a potent vasodilator
Decreases both pulmonary vascular resistance and SVR.
63
64
65
Therapy
Hypovolemic Shock: Rapid reversal with blood, colloid, or
crystalloid
Cardiogenic: Left ventricular MI:
Intra-aortic balloon pump, cardiac angiography, and revascularization
Right ventricular MI: Fluids and inotrops
66
Therapy
Extra-cardiac obstructive shock: Cardiac tamponade:
Pericardiocentesis or surgical drainage Pulmonary embolism:
Thrombolytics, Heparin and embolectomy
67
Therapy
Distributive shock: Septic:
Antibiotics + fluid resuscitation+ vasopressors or inotropes
Anaphylactic: Steroids, diphenhydramine, H1 and H2 blockers,
and epinephrine
68
Questions