Hemodynamic effect of dobutamine in patients with severe heart failure
4
REPORTS ON THERAPY Hemodynamic Effect of Dobutamine in Patients with Severe Heart Failure NASIM AKHTAR, MD ESTEBAN MIKULIC, MD JAY N. COHN, MD, FACC M. HAFEEZ CHAUDHRY, MD Washington, DC. Minneapolis, Minnesota From the Hypertension and Clinical Hemody- namics Section, Veterans Administration Hospi- tal, the Department of Medicine, Georgetown University School of Medicine, Washington, DC., and the University of Minnesota Medical School, Minneapolis, Minn. Manuscript accept- ed December 1 I, 1974. Address for reprints: Jay N. Cohn, MD, Uni- versity of Minnesota Medical School, Minneapo- lis, Minn. 55455. Dobutamine, a derivative of dopamine, was infused at a rate of 10 pg/kg per min in 15 patients with severe congestive heart failure. Car- diac output increased from an average of 3.1 to 5.6 liters/min (P <O.OOl) with no change in mean arterial pressure (93.3 to 96.2 mm Hg) and only a slight increase in heart rate (98.5 to 105.2 beats/min) (P <0.02). Pulmonary wedge pressure was decreased from an aver- age of 27.4 to 21.1 mm Hg (P <O.OOl). In seven patients a dose of 5 fig/kg per min also produced a significant increase in cardiac output but the effect was less than with the 10 pg/kg per min dose. No side effects were observed during the infusion. Dobutamine therefore is a potent inotropic drug with limited chronotropic and peripheral vascular effects and deserves therapeutic trial in the short-term management of low output heart failure. Although sympathomimetic amines are the most potent known agents for augmenting myocardial contractility, their clinical applica- tion for this purpose has been limited because of their chronotropic and peripheral vascular actions. Isoproterenol, for example, induces a marked increase in cardiac output but at the expense of a decrease in arterial diastolic pressure, tachycardia and increased myocardial irri- tability. i-a Norepinephrine, on the other hand, produces systemic va- soconstriction, which increases diastolic arterial pressure and thus may limit the increase in cardiac output and result in a reduction of regional perfusion.*m6 Dopamine has been introduced as a sympatho- mimetic inotropic agent with less chronotropic and vasoconstrictive effect7s; however, it has considerable vasoconstrictive properties in large doses, the cardiac output response is variable and arrhythmias have been reported.“-” A derivative of dopamine, dobutamine ([*I -4-[2-] [3-(p-hydrox- phenyl)-l-methyl propyl] amino] ethyl] pyrocatechol hydrochloride), has recently been synthesized by Tuttle and MillsI and has been demonstrated in early animal studies to have a relatively selective in- otropic effect. is In this study we examined the acute hemodynamic response t,o dobutamine in patients with severe left ventricular fail- ure. Our results indicate that this drug has potent cardiac stimulating properties with little effect on heart rate or blood pressure and there- fore may prove to be a useful agent for the management of severe heart failure. Methods Studies were performed in 15 patients with severe chronic class III or class IV (New York Heart Association criteria) heart failure (primary myocardial, rheumatic or ischemic heart disease). Pertinent clinical data are summarized in Table I. All patients were male; their ages ranged from 39 to 76 (average 51) years. Ail were receiving maintenance doses of digitalis and had been treated with diuretic agents. The digitalis and diuretic agents were withheld for 24 hours before the study. 202 August 1975 The American Journal of CARDIOLOGY Volume 36
-
Upload
nasim-akhtar -
Category
Documents
-
view
214 -
download
1
Transcript of Hemodynamic effect of dobutamine in patients with severe heart failure

REPORTS ON THERAPY
Hemodynamic Effect of Dobutamine in Patients with
Severe Heart Failure
NASIM AKHTAR, MD ESTEBAN MIKULIC, MD JAY N. COHN, MD, FACC M. HAFEEZ CHAUDHRY, MD
Washington, DC. Minneapolis, Minnesota
From the Hypertension and Clinical Hemody- namics Section, Veterans Administration Hospi- tal, the Department of Medicine, Georgetown University School of Medicine, Washington, DC., and the University of Minnesota Medical School, Minneapolis, Minn. Manuscript accept- ed December 1 I, 1974.
Address for reprints: Jay N. Cohn, MD, Uni- versity of Minnesota Medical School, Minneapo- lis, Minn. 55455.
Dobutamine, a derivative of dopamine, was infused at a rate of 10 pg/kg per min in 15 patients with severe congestive heart failure. Car- diac output increased from an average of 3.1 to 5.6 liters/min (P <O.OOl) with no change in mean arterial pressure (93.3 to 96.2 mm Hg) and only a slight increase in heart rate (98.5 to 105.2 beats/min) (P <0.02). Pulmonary wedge pressure was decreased from an aver- age of 27.4 to 21.1 mm Hg (P <O.OOl). In seven patients a dose of 5 fig/kg per min also produced a significant increase in cardiac output but the effect was less than with the 10 pg/kg per min dose. No side effects were observed during the infusion. Dobutamine therefore is a potent inotropic drug with limited chronotropic and peripheral vascular effects and deserves therapeutic trial in the short-term management of low output heart failure.
Although sympathomimetic amines are the most potent known agents for augmenting myocardial contractility, their clinical applica- tion for this purpose has been limited because of their chronotropic and peripheral vascular actions. Isoproterenol, for example, induces a marked increase in cardiac output but at the expense of a decrease in arterial diastolic pressure, tachycardia and increased myocardial irri- tability. i-a Norepinephrine, on the other hand, produces systemic va- soconstriction, which increases diastolic arterial pressure and thus may limit the increase in cardiac output and result in a reduction of regional perfusion.*m6 Dopamine has been introduced as a sympatho- mimetic inotropic agent with less chronotropic and vasoconstrictive effect7s; however, it has considerable vasoconstrictive properties in large doses, the cardiac output response is variable and arrhythmias have been reported.“-”
A derivative of dopamine, dobutamine ([*I -4-[2-] [3-(p-hydrox- phenyl)-l-methyl propyl] amino] ethyl] pyrocatechol hydrochloride),
has recently been synthesized by Tuttle and MillsI and has been demonstrated in early animal studies to have a relatively selective in- otropic effect. is In this study we examined the acute hemodynamic response t,o dobutamine in patients with severe left ventricular fail- ure. Our results indicate that this drug has potent cardiac stimulating properties with little effect on heart rate or blood pressure and there- fore may prove to be a useful agent for the management of severe heart failure.
Methods
Studies were performed in 15 patients with severe chronic class III or class IV (New York Heart Association criteria) heart failure (primary myocardial, rheumatic or ischemic heart disease). Pertinent clinical data are summarized in Table I. All patients were male; their ages ranged from 39 to 76 (average 51) years. Ail were receiving maintenance doses of digitalis and had been treated with diuretic agents. The digitalis and diuretic agents were withheld for 24 hours before the study.
202 August 1975 The American Journal of CARDIOLOGY Volume 36

DO&JlAM@JE IN SEVERE NART FAILURE-AKHTAR ET AL.
TABLE I
Hemodynamic Effects of Dobutamine (IO pg/kg per min) in 15 Patients with Heart Failure ---____ ~.
Case no. Age (vr) BSA Diagnosis State MAP HR PAP PCW co SVR PVR
1 48
2
3
45
41
4
5
6
7
8
9
10
11
12
13
14
15
50
61
44
46
48
49
50
39
76
63
49
60
Average (+ SE)
1.86
1.52
1.84
1.78
1.94
-1.86
2.18
1.59
1.80
1.80
2.22
1.80
1.64
2.10
2.33
CM
CM
CM
RHD
CM
IHD
CM
CM
CM
IHD
CM
IHD
CM
CM
RHD
BSA = body surface area (ml); C = control; CM = cardiomyopathy; CO = cardiac output (liters/min); D = dobutamine infusion; HR = heart rate (beats/min); IHD = ischemic heart disease; MAP = mean arterial pressure (mm Hg);.NS = not signifi- cant; P = probability; PAP = mean pulmonary arterial pressure (mm Hg); PCW = pulmonary wedge pressure (mm Hg); PVR = pulmonary vascular resistance (dynes set cmm5); RHD = rheumatic heart disease; SE = standard error; SVR = systemic vas- cular resistance (dynes set cm-5).
C D C D C D C D C D C D C D C d C D C D C D C D C D C D C D C
D
P
98
88 120 124 104 114
.70 80 80 90 85 85 92 84 84 93
112 114
90 100 118 117 104
94 82 86 81
111 80 80 93.3 k4.0 98.2 +3.8 NS
90 26 20 2.8 2800 229 100 20 16 5.6 1257 57 110 - - 3.5 2743 -
110 - - 6.1 1574 -
110 - 3.5 2377 -
110 - 5.2 1753 -
96 17 12 2.9 1931 138 108 15 10 3.8 1684 105
90 25 18 3.3 1939 170 96 19 13 4.7 1532 102 84 35 28 4.5 1511 124 90 35 25 5.5 1236 145
120 46 34 1.9 2918 497 120 31 18 5.6 943 186 100 43 34 2.1 2430 308
96 38 28 4.1 1662 196 120 43 34 4.0 1836 179 120 40 28 4.6 1669 207
90 38 30 4.5 1372 142 120 25 14 7.8 923 108
94 40 22 3.1 2837 464 94 34 14 4.7 1923 339
120 53 34 2.0 3390 737 124 39 26 3.4 1929 305
88 . . 1.6 . . . . . 92
3k’ 29’ 5.8 .
75 3.1 1820 189’ 87 38 27 8.7 966 99 90 45 34 3.5 1826 251 90 45 34 4.3 1488 204 98.5 37.3 27.4 3.1 2237 281 k3.7 k2.9 k2.0 to.2 +157 t60
105.2 31.6 21.1 5.6 1418 162 k3.3 +3.0 22.1 to.4 +112 k25
<0.02 <O.Ol <O.OOl <O.OOl <O.OOl <O.OOl
Right heart catheterization was performed using a Swan- Ganz flow-directed balloon-tipped catheter inserted percu- taneously by way of an antecubital vein. In 12 patients the pulmonary artery was successfully entered, but in 3 the catheter could not be advanced beyond the right atrium. The brachial artery was cannulated with a Teflon@ needle. Arterial, pulmonary arterial and pulmonary capillary wedge (occluded) pressures were recorded using Statham P23 Db strain gauge transducers and a Hewlett-Packard recorder. Cardiac output in liters per minute was deter- mined by the indicator-dilution technique using indocya- nine green dye injected into the pulmonary artery and sam- pled from the brachial artery through a Gilford cuvette densitometer. Systemic vascular resistance in dynes set crnd5 was calculated from the formula: (MAP - RAP) X
SO/CO, where MAP is the mean arterial pressure in mm Hg, RAP is the mean right atria1 pressure in mm Hg and CO is the cardiac output in literslmin. Pulmonary vascular
resistance was calculated from the formula: (MPAP - PCW) X SO/CO, where MPAP is the mean pulmonary arte- rial pressure in mm Hg and PCW is the mean pulmonary capillary wedge pressure in mm Hg. Stroke work in g-m was calculated from the formula: (MAP - PCW) (SV) (0.0136) where SV is the stroke volume in ml.
After control hemodynamic measurements were ob- tained dobutamine (200 mg in 500 ml of dextrose in water) was administered intravenously as a continuous infusion at a rate of 10 Kg/kg per min. In seven patients dobutamine was given at two dose levels, 5 and 10 wg/kg per min. He- modynamic measurements were repeated after at least 15 minutes of constant infusion of the drug at each dose level.
Results
Hemodynamic data at rest and during infusion of 10 pg/kg per min of dobutamine in the 15 patients
August 1975 The American Journal of CARDIOLDGY Volume 36 203

DOBVTAW IN SEVERE HEART FAILURE-AKHTAR ET AL.
s 80-
5 60-
P - d 40
H 20-
0 I 4 , 1 , I L I 0 5 10 15 20 25 30 35 40
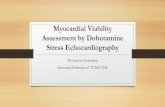
PCW (mm Hg) FIGURE 1. Effect of dobutamine (IO pglkg per min) on the relation between stroke volume and pulmonary capillary wedge pressure (PCW). Closed circles represent control observations, open circles observations during dobutamine infusion. Heavy line represents the average values for all patients studied.
studied are shown in Table I. Cardiac output in- creased in every patient (P <O.OOl), from an average of 3.1 to 5.6 liters/min (81.8 percent), whereas heart rate changed only slightly (average 98.5 to 105.2 beatslmin, P <0.02), indicating that the increase in cardiac output was due mainly to the alteration in stroke volume, which increased by an average of 65.8 percent. The cardiac index was less than 2.5 liters/ min per m2 in all subjects during the control period and was restored to the normal range in 10 (67 per- cent) of the patients during dobutamine infusion. Mean pulmonary capillary wedge pressure in 12 pa- tients decreased from 27.4 to 21.1 mm Hg during infusion of the drug (P <O.OOl) (Fig. 1).
Mean arterial pressure was not significantly al- tered (93.3 to 98.2 mm Hg) during infusion of dobu- tamine, but systolic pressure increased from an aver- age of 120 f 5.5 (standard error) to 136 f 5.5 mm Hg (P <0.05) whereas diastolic pressure was unaltered (79 f 3.5 to 82 f 3.2 mm Hg). Cardiac work almost doubled as indicated by an increase in mean stroke work from 28.3 to 57.5 g-m (P <O.Ol). The values for both systemic and pulmonary vascular resistance de- creased during the drug infusion, from an average of 2,237 to 1,418 dynes set crnB5 (P <O.OOl) and from 281 to 162 dynes set cmP5 (P <O.OOl), respectively.
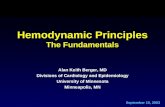
The 10 pg/kg per min infusion produced a greater hemodynamic effect than the 5 fig/kg per min infu- sion in the seven patients who were studied at both dose levels (Fig. 2). No arrhythmias or untoward side effects were observed in any patients during dobuta- mine infusion.
Discussion
Our data indicate that dobutamine possesses phar- macologic properties that make it an ideal sympatho- mimetic agent for producing a selective improvement in myacardial function. In the doses employed in these patients with severe congestive heart failure, cardiac output was restored to normal levels, pulmo-
HR MAP
(beats/min) lmm Hg)
PCW
(mm Hgl
co SVR
(L/min) (“5)
FIGURE 2. Average hemodynamic measurements in seven patients during control period (open bar) and infusions of 5 pg/kg per min (middle bar) and 10 @g/kg per min of dobutamine (right bar). As- terisk indicates significant difference from control (P <0.05); triangle indicates significant difference from values during 5 fig/kg per min infusion (P <0.05). CO = cardiac output: HR = heart rate; L = liters: MAP = mean arterial pressure; PCW = pulmonary wedge pressure; SVR = systemic vascular resistance.
nary capillary wedge pressure was reduced, heart rate was only slightly increased whereas mean arterial pressure was unchanged.
Since myocardial oxygen consumption is directly related to aortic pressure and heart rate as well as to the contractile state of the myocardium,14 sympatho- mimetic amines that increase heart rate (isoprotere- 1101) or systemic vascular resistance (norepinephrine) may have a deleterious effect on the ischemic left ventricle.3,1”J6 Use of dobutamine in this clinical set- ting may be advantageous because this drug does not have prominent chronotropic or peripheral vascular effects but retains a potent inotropic effect. The re- duction in peripheral vascular resistance during dobutamine infusion is consistent with either a direct vasodilating effect of the drug or a reflex relaxation of vascular tone.
Clinical implications: The incremental circulato- ry effect demonstrated when the dose was increased from 5 to 10 pg/kg per min indicates that within this dose range the hemodynamic response is linearly re- lated to dose. Because of the prompt response to the drug, its reliability in restoring cardiac output to nor- mal levels and the absence of side effects during these short-term infusions, further evaluation of the use of dobutamine in the treatment of low output syndromes is indicated. Since most of the patients in our series were less than 50 years old and had cardio- myopathy, additional data are needed on the re- sponses in older patients with ischemic heart disease.
Acknowledgment
The technical assistance of Ms. Eleanor Garlisi, Helen Bazaz and Sally Rubenstone and the secretarial help of Ms. Santa Ferraro are gratefully acknowledged. Dobutamine was kindly supplied by A. F. Fasola, MD, Lilly Research Laboratories, Eli Lilly and Co., Indianapolis, Ind.
204 August 1975 The American Journal of CARDIOLOGY Volume 36

DOBUTAMNE IN SEVERE HEART FAILURE-AKHTAR ET AL.
References
1.
2.
3.
4.
Dodge Jl, Lord JD, San&r H: Cardiovascular effects of iso- proterenol in normal subjects with congestive heart failure. Am Heart J 60:94-1051960 EMott WC, Gorfln R: lsoproterenol in treatment of heart disease. Hemodynamic effects in circulatory failure. JAMA 197:315- 320, 1966 Gunnar RM, Loeb HS, Pfetras RJ, et al: Ineffectiveness of iso- proterenol in shock due to acute myocardial infarction. JAMA 202:1124-1128, 1967 Goldenberg M, Ptnes KE, Baldwin EF, et al: The hemodynamic response of man to nor-epinephrine and epinephrine and its rehtion to the problem of hypertension. Am J Med 5792-806, 1948
10.
11.
12.
13.
5.
6.
7.
8.
Cohn JN, Lurfa MH: Studies in clinical shock and hypotension. II. Hemodynamic effects of norepinephrine and angiotensin. J Clin Invest 44: 1494- 1504, 1965 Cohn JN: Blood pressure and cardiac performance. Am J Med 55:351-361, 1973 Goldberg Lk Cardiovascular and renal actions of dopamine: po- tential clinical applications. Pharmacol Rev 24: l-29, 1972 MacCannell KF, McNay JL, Meyer MB, et al: Dopamine in the treatment of hypotension and shock. N Engl J Med 275:1389- 1398, 1966
14.
15.
16.
9. Hfgglns CB, Mlllard RW, Braunwald E, et al: Effects and mech-
anisms of action of dopamine on regional hemodynamics in the conscious dog. Am J Physiol225:432-437, 1973 Talky RC, Goldberg LI, Johnson CE, et al: A hemodynamic comparison of dopamine and isoproterenol in patients in shock. Circulation 39:361-378, 1969 Llpp H, Fallcov RE, Reanekov L, et al: The effects of dopamine on depressed myocardial function following coronary emboliza- tion in the closed chest dog. Am Heart J 84:208-214, 1972 Tuttle RR, Mills J: Derives de la dopamine. Belgium Patent 798: 051.1973 Vatner SF, McRltchle RJ, Braunwald E: Effects of dobutamine on left ventricuiar performance, coronary dynamics and distribu- tion of cardiac output in conscious dog. J Clin Invest 53:1265- 1273, 1974 Sonnenbllck EH, Skelton CL: Myocardial energetics: basic prin- ciples and clinical implications. N Engl J Med 285:668-675, 1971 Maroko PR, Llbby P, Braunwald E: Effect of pharmacologic agents on the function of the ischemic heart. Am J Cardiol 32: 930-936, 1973 Mueller HS, Ayers SM, Gregory JJ, et al: Hemodynamics. coro- nary blood flow, and myocardial metabolism in coronary shock; responses to I-norepinephrine and isoproterenol. J Clin Invest 49:1885-1902, 1970
August 1975 The American Journal ot CARDIOLOGY Volume 36 205