
Hematuria. HAEMATURIA Common finding Incidental DEFINING HAEMATURIA Visible haematuria Non visible...
42
Hematuria
-
Upload
beatrix-boone -
Category
Documents
-
view
228 -
download
2
Transcript of Hematuria. HAEMATURIA Common finding Incidental DEFINING HAEMATURIA Visible haematuria Non visible...
Hematuria
HAEMATURIACommon finding Incidental
DEFINING HAEMATURIA
Visible haematuria Non visible haematuria (dipstick and
microscopic)
Gross hematuria
Suspected if a red or brown color change of urine
Medications (phenazopyridine)Ingestion of certain dyesMyoglobinuria or hemoglobinuria
If pass clot indicate urinary source
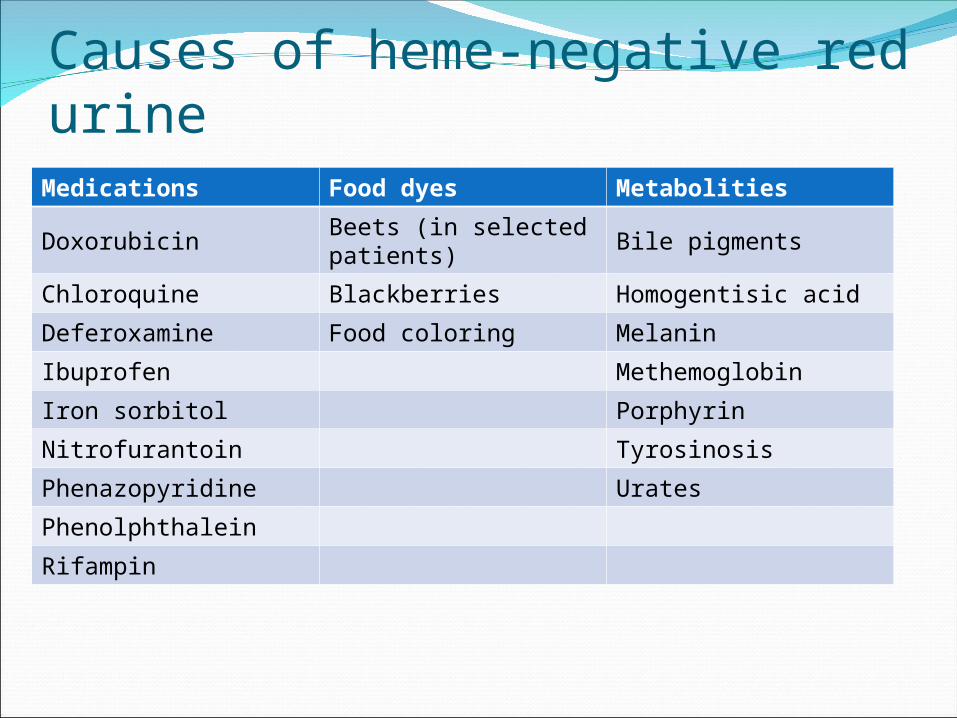
Causes of heme-negative red urineMedications Food dyes Metabolities
DoxorubicinBeets (in selected patients)
Bile pigments
Chloroquine Blackberries Homogentisic acid
Deferoxamine Food coloring Melanin
Ibuprofen Methemoglobin
Iron sorbitol Porphyrin
Nitrofurantoin Tyrosinosis
Phenazopyridine Urates
Phenolphthalein
Rifampin
Microscopic hematuria
Accidental finding from UA or urine dipstick3 or more RBChpf No safe lower limit below which significant disease can be excluded Often asymptomatic
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
HAEMATURIACommon finding Incidental
DEFINING HAEMATURIA
Visible haematuria Non visible haematuria (dipstick and
microscopic)
Gross hematuria
Suspected if a red or brown color change of urine
Medications (phenazopyridine)Ingestion of certain dyesMyoglobinuria or hemoglobinuria
If pass clot indicate urinary source
Causes of heme-negative red urineMedications Food dyes Metabolities
DoxorubicinBeets (in selected patients)
Bile pigments
Chloroquine Blackberries Homogentisic acid
Deferoxamine Food coloring Melanin
Ibuprofen Methemoglobin
Iron sorbitol Porphyrin
Nitrofurantoin Tyrosinosis
Phenazopyridine Urates
Phenolphthalein
Rifampin
Microscopic hematuria
Accidental finding from UA or urine dipstick3 or more RBChpf No safe lower limit below which significant disease can be excluded Often asymptomatic
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Gross hematuria
Suspected if a red or brown color change of urine
Medications (phenazopyridine)Ingestion of certain dyesMyoglobinuria or hemoglobinuria
If pass clot indicate urinary source
Causes of heme-negative red urineMedications Food dyes Metabolities
DoxorubicinBeets (in selected patients)
Bile pigments
Chloroquine Blackberries Homogentisic acid
Deferoxamine Food coloring Melanin
Ibuprofen Methemoglobin
Iron sorbitol Porphyrin
Nitrofurantoin Tyrosinosis
Phenazopyridine Urates
Phenolphthalein
Rifampin
Microscopic hematuria
Accidental finding from UA or urine dipstick3 or more RBChpf No safe lower limit below which significant disease can be excluded Often asymptomatic
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Causes of heme-negative red urineMedications Food dyes Metabolities
DoxorubicinBeets (in selected patients)
Bile pigments
Chloroquine Blackberries Homogentisic acid
Deferoxamine Food coloring Melanin
Ibuprofen Methemoglobin
Iron sorbitol Porphyrin
Nitrofurantoin Tyrosinosis
Phenazopyridine Urates
Phenolphthalein
Rifampin
Microscopic hematuria
Accidental finding from UA or urine dipstick3 or more RBChpf No safe lower limit below which significant disease can be excluded Often asymptomatic
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Microscopic hematuria
Accidental finding from UA or urine dipstick3 or more RBChpf No safe lower limit below which significant disease can be excluded Often asymptomatic
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Dx
The urine sediment is the gold standard for the detection of microscopic hematuria
Dipsticks for heme are as sensitive as urine sediment examination but result in more false positive tests due to the following
A positive dipstick test must always be confirmed with microscopic examination of the urine
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
The evaluation should address the following three questions 1 Are there any clues from the history or physical examination that suggest a particular diagnosis
2 Does the hematuria represent glomerular or extraglomerular bleeding
3 Is the hematuria transient or persistent
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Urethral First 10-15 mLBladder Final 10-30 mLUpper urinary tract Throughout
a three-tube test may also help to locate the source of bleeding in selected cases
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Goal is to quickly identify
1Infection2Kidney stone3Malignant
Need immediate attention
History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

History and Physical
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
History
Abdominal or flank pain1048708 Dysuria frequency urgency1048708 Trauma1048708 Strenuous exercise 1048708 Menstruation1048708 Recent URI sore throat1048708 Skin rashes skin infection1048708 Diarrhea (especially bloody)1048708 Joint painsswellings1048708 Medicationstoxins1048708 ho sickle cell disease or sickle trait
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Family history
Hematuria Hearing loss HTN Stones Renal disease Dialysis or transplant Sickle cell trait Coagulopathy
Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Medication Hx
Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Physical Exam
1048708 Vital sign BP T HR Skin Rashes evidence or trauma bruising1048708 Abdomen for masses tenderness (flank suprapubics) bruits1048708 CVS irregular irregular1048708 Edema (especially periorbital)1048708 Joint erythema swelling warmth1048708 Paleness jaundice1048708 Careful inspection of external genitalia ProstatebullIf BP is elevated further evaluation is immediately warranted
Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Physical Examination Findings and Associated Causes of Hematuria Physical examination finding Cause of hematuria General (systemic) examination
Severe dehydration Renal vein thrombosis
Peripheral edema Nephrotic syndrome vasculitis
Cardiovascular system
Myocardial infarction Renal artery embolus or thrombus
Atrial fibrillation Renal artery embolus or thrombus
Hypertension Glomerulosclerosis with or without proteinuria
Abdomen
Bruit Arteriovenous fistula
Genitourinary system
Enlarged prostate Urinary tract infection
Phimosis Urinary tract infection
Meatal stenosis Urinary tract infection
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
1 Concurrent pyuria and dysuria indicate UTI may also occur with bladder
malignancy
2 A recent URI raise the possibility of either post infectious glomerulonephritis
or IgA nephropathy
3 A positive family history of renal disease give suspicion of hereditary nephritis
polycystic kidney disease or sickle cell disease
4 Unilateral flank pain radiating to the groin suggesting ureteral obstruction
due to a calculus or blood clot but can occasionally be seen with malignancy
Flank pain that is persistent or recurrent can also occur in the rare loin pain
hematuria syndrome
5 Symptoms of prostatic obstruction in older men such as hesitancy and
dribbling The cellular proliferation in BPH is associated with increased
vascularity and the new vessels can be fragile
Clues from the history that point toward a specific diagnosis
6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

6 Recent vigorous exercise or trauma
7 History of a bleeding disorder or bleeding from multiple sites
due to uncontrolled anticoagulant therapy
8 Cyclic hematuria in women that is most prominent during and
shortly after menstruation suggesting endometriosis of the
urinary tract
9 Medications that might cause nephritis (usually with other
findings typically with renal insufficiency)
1o Travel or residence in areas endemic for Schistosoma
hematobium
11Sterile pyuria with hematuria which may occur with renal
tuberculosis analgesic nephropathy and other interstitial
diseases
Clues from the history that point toward a specific diagnosis
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Glomerular or Extra Glomerular bleeding
Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Glomerular
ARFprimary nephritis (post streptococcal glomerulonephritis Ig A nephropathy
Anti-GBM disease)2nd nephritis(SLE goodpasturersquos syndrome ANCA related vasculitis)Alportrsquos syndrome (hereditary nephritis)thin basement membrane nephropathy (benign familial hematuria) bull
Microscopic hematuria DDx
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
non glomerular
Renalmalignancyvascular disease (malignant hypertension AVM nutcracker syndrome renal vein thrombosis sickle cell traitdisease papillary necrosis)infection (pyelonephritis TB CMV EBV)hypercalciuriahereditary disease (polycystic kidney disease medullary sponge kidney)
Microscopic hematuria DDx
Nonrenalmalignancy (prostate ureter bladder)BPHNephrolithiasisCoagulopathyTrauma
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Rare cause of Microscopic Hematuria
Arteriovenous malformations and fistulas
Nutcracker syndrome
Loin pain-hematuria syndrome
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Arteriovenous malformations and fistulas mdash An AV malformation (AVM) or fistula of the urologic tract may be either congenital or acquired The primary presenting sign is gross hematuria but high-output heart failure and hypertension also may be seen The latter is presumably due to activation of the renin-angiotensin system resulting from ischemia distal to the AVM
Nutcracker syndrome mdash The nutcracker syndrome refers to compression of the left renal vein between the aorta and proximal superior mesenteric artery Nutcracker syndrome can cause both microscopic and gross hematuria primarily in children (but also adults) in Asia The hematuria is usually asymptomatic but may be associated with left flank pain Nutcracker syndrome has also been associated with orthostatic proteinuria
Loin pain-hematuria syndrome mdash The loin pain-hematuria syndrome is a poorly defined disorder characterized by loin or flank pain that is often severe and unrelenting and hematuria with dysmorphic red cell features suggesting a glomerular origin Affected patients usually have normal kidney function
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
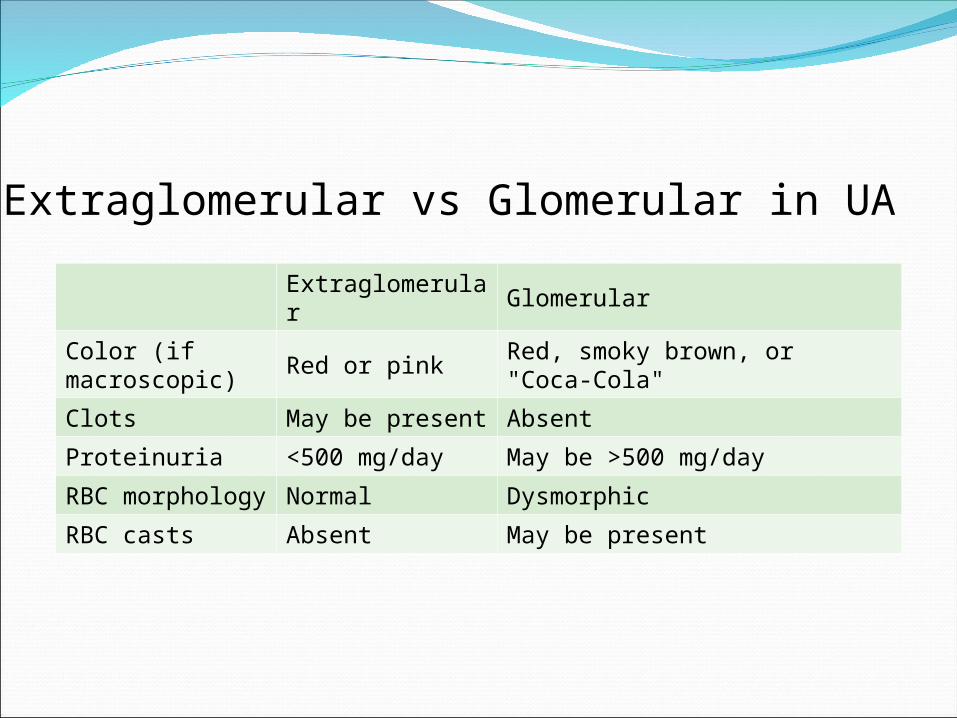
Extraglomerular Glomerular
Color (if macroscopic)
Red or pinkRed smoky brown or Coca-Cola
Clots May be present Absent
Proteinuria lt500 mgday May be gt500 mgday
RBC morphology
Normal Dysmorphic
RBC casts Absent May be present
Extraglomerular vs Glomerular in UA
Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Findings on Microscopy
FIGURE 1 Typical morphology of erythrocytes from a urine specimen revealing microscopic hematuria (phase contrast microscopy 3100 )
Erythrocytes of uniform character are classified as isomorphic and suggest hematuria of lower urinary tract origin
Microscopic clots of clumped erythrocytes in urine are also suggestive of lower urinary tract bleeding
FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

FIGURE 2 Dysmorphic erythrocytes from a urine specimen These cells suggest a glomerular cause of microscopic hematuria (phase contrast microscopy 3 100)
Dysmorphic erythrocytes are characterized by an irregular outer cell membrane and suggest hematuria of glomerular origin
Red blood cell casts are also associated with a glomerular cause of hematuria
Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Transient or persistent hematuria
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Exception
Malignancy risk in older patients with transient hematuria
In older patients even transient hematuria carries an appreciable risk of malignancy (assuming no evidence of glomerular bleeding)
The risks includes age gt50 smoker and Hx of analgesic abuse
Transient hematuriaTransient microscopic hematuria is a common problem in adults Fever infection trauma and exercise are potential causes It is reasonable to repeat an abnormal urinalysis in a few days
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
When persistent hematuria is essentially the only manifestation of glomerular disease one of three disorders is most likely
IgA nephropathy in which there is often gross hematuria and sometimes a positive family history but without any clear pattern of autosomal inheritance Alport syndrome (hereditary nephritis) in which gross hematuria can occur in association with a positive family history of renal failure and sometimes deafness or corneal abnormalities
Thin basement membrane nephropathy (also called thin basement membrane disease or benign familial hematuria) in which gross hematuria is unusual and the family history may be positive (with an autonomic dominant pattern of inheritance) for microscopic hematuria but not for renal failure
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Persistent hematuria
Underlying malignancy is greater in patients with persistent hematuria in whom there is no obvious cause from the history
The primary underlying cancers are bladder renal and much less often prostate
Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Laboratory Tests (initial work up)
bull UA and microscopy to determine the number and morphology of RBC crystal and castsbull Consider urine Cxbull CBC PT INR electrolytes kidney functionbull Serum chemistries and serologic studies for glomerular causes of hematuria as directed by the medical historybull Repeat UA in a few days
Further urologic evaluation is warranted if more than three RBCphf are found on at least two of three properly collected urine specimens or if high-grade microscopic hematuria (more than 100 red blood cells per high-power field) is found on a single urinalysis17
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
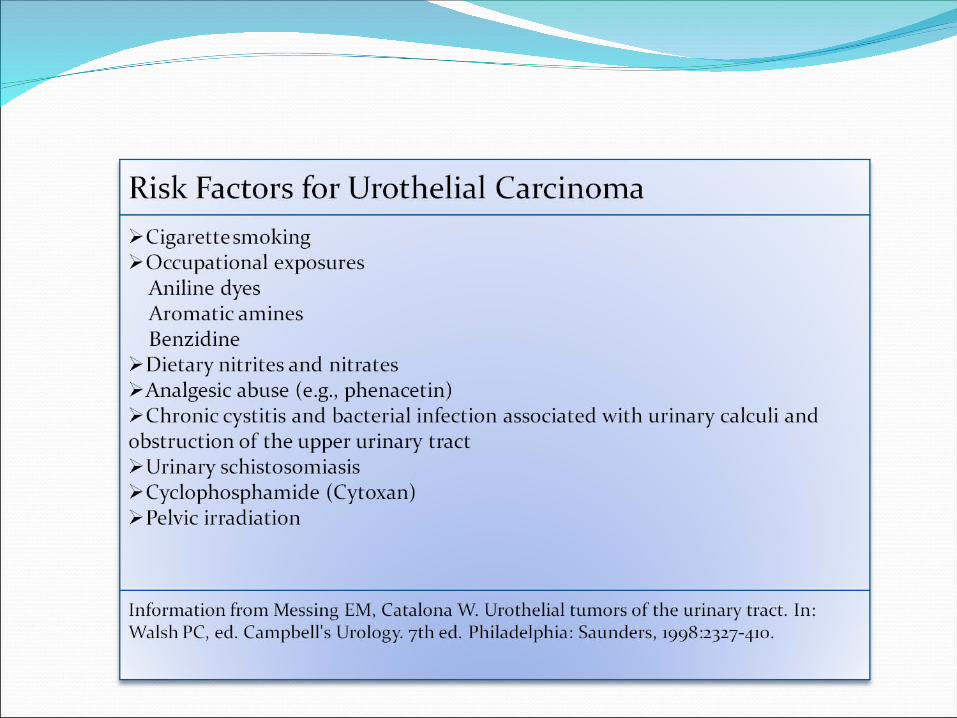
Further Work up bull Glomerular causes
Consider a refer to nephrology for further evaluation and possible renal biopsy
A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

A biopsy is not usually performed for isolated glomerular hematuria (ie no proteinuria or renal insufficiency) since there is no specific therapy for these conditions unless the patient is considering becoming a kidney donor
However biopsy should be considered if there is evidence of progressive disease as manifested by an elevation in the plasma creatinine concentration increasing protein excretion or an otherwise unexplained rise in blood pressure even when the values remain within the normal range
Renal Biopsy
Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Further Work up
bullNon-glomerular causes
CT renal US andor IVP to search for lesions in the kidney collecting system ureters and bladder
Urine cytology if increased risk for urothelial cancers
Consider a referral to urology for cystoscopy especially for pt at risk of malignancies
Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Radiologic and other tests for the evaluation of hematuriaTest Advantages Disadvantages
Intravenous pyelogram (IVP)
Excellent visualization of the kidney collecting system and ureter
May miss bladder lesions can cause nephrotoxicity idiosyncratic reactions (110000)
Cystoscopy
Best way to examine the bladder which is not as well visualized by IVP or ultrasound
Invasive uncomfortable and expensive
Ultrasound
If of good quality as sensitive as IVP for renal lesions with less morbidity and cost
Less sensitive than IVP for ureter and bladder
Retrograde pyelographyThe best test for examing the ureters can be combined with cystoscopy
Invasive not useful for examining other parts of the urinary collecting system
Urinary cytologySensitivity 67 percent specificity 96 percent for uroepithelial cancer
Useful only for cancer mainly of the bladder
CT scanExcellent for examining the renal parenchyma
Expensive
Angiography
Useful for gross hematuria when other tests have not revealed the cause the only good test for vascular malformations
Invasive expensive
The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

The combination of negative radiologic examination(s) ( IVP US CT scan cytology and cystoscopy) is usually sufficient to exclude malignancy in the urinary tract
However approximately 1 of older pt with an initially negative evaluation will at 3 to 4 years have a detectable urinary tract malignancy
Recommendation
Initial and then periodic urine cytology and UA should be performed in pt at high risk for malignancy (at 6 12 24 and 36 months)
Follow up
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
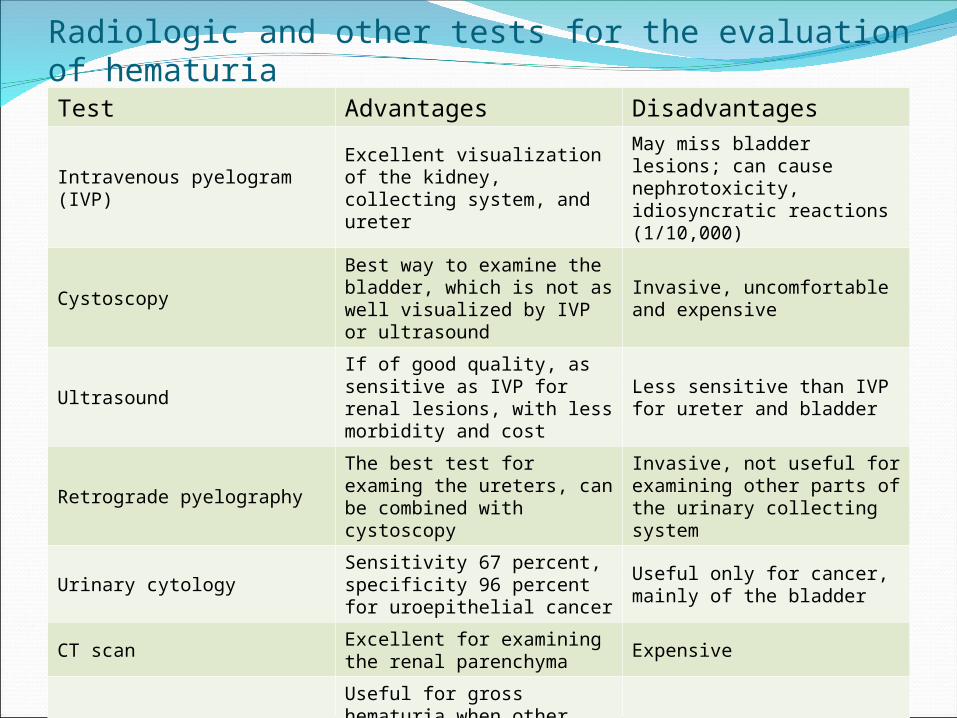
SCREENING FOR HEMATURIA
Not recommended
Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you

Initial Evaluation of Asymptomatic Microscopic Hematuria
Thank you
Thank you


















