Heartworm Haltingimages2.advanstar.com/PixelMags/vetmedicine/pdf/2015-01.pdf ·...
28
Heartworm INCLUDES THE January 2015 | Volume 110 | Number 1 | PEER-REVIEWED | dvm360.com regain control of their AGGRESSIVE, FEARFUL, UNRULY dogs on walks. p15 UNWANTED BEHAVIOR Clinical Exposures Treating a tennis-ball-size tumor in a turkey’s eye 6 Mind the gap! The chasm between client and veterinarian concerns about parasites 4 Leptospirosis When should you suspect this bacterial infection in dogs? 11 Idea Exchange ▸ An alarming way to monitor anesthesia 26 ▸ An office efficiency tip with green benefits 26 Halting on a leash
Transcript of Heartworm Haltingimages2.advanstar.com/PixelMags/vetmedicine/pdf/2015-01.pdf ·...

Heartworm
INCLUDES THE
January 2015 | Volume 110 | Number 1 | PEER-REVIEWED | dvm360.com
regain control of their AGGRESSIVE, FEARFUL, UNRULY dogs on walks.Y p15
UNWANTED
BEHAVIORClinical ExposuresTreating a tennis-ball-size
tumor in a turkey’s eye 6
Mind the gap!The chasm between client
and veterinarian concerns
about parasites 4
LeptospirosisWhen should you
suspect this bacterial
infection in dogs? 11
Idea Exchange▸ An alarming way to
monitor anesthesia 26
▸ An offi ce effi ciency tip
with green benefi ts 26
Halting
on a leash
ES549090_vetm0115_CV1.pgs 12.24.2014 18:45 ADV blackyellowmagentacyan

21/
ES549674_VETM0115_CV2_FP.pgs 12.29.2014 15:15 ADV blackyellowmagentacyan

dvm360.com | Veterinary Medicine | January 2015 | 3
Subscriber Services: Call (800) 815-3400 in the United States, or (888) 527-7008 or (218) 740-6477 in Canada; fax (218) 740-6417; or write to: Veterinary Medicine, 131 W. 1st St., Duluth, MN 55802-2065. If you are un-able to connect with the 800 numbers, email fulfi ll@superfi ll.com. Reprint Services: Call 1-877-652-5295 ext. 121 or email [email protected]. Outside US, UK, direct dial: 281-419-5725. ext. 121 Back Issues: Individual copies are available for one year; to order, call (800) 598-6008. Permissions/International Licensing. Call Maureen Cannon at (440) 891-2742. List Sales: Please contact List Account Executive Renée Schuster at (440) 891-2613. Editorial Offi ces: Write to 8033 Flint, Lenexa, KS 66214; or call (913) 871-3800. Visit our websites: dvm360.com; thecvc.com; industrymatter.com.
MissionVeterinary Medicine is a peer-reviewed journal dedicated
to providing concise, credible, and essential information
on the most common and crucial clinical problems seen
in companion-animal practice.
Editorial Advisory Board
Leading specialists who direct our content and ensure
our editorial quality and integrity
Joseph W. Bartges, DVM, PhD, DACVIM, DACVN
David S. Bruyette, DVM, DACVIM
Barret Bulmer, DVM, MS, DACVIM
John Ciribassi, DVM, DACVB
Timothy M. Fan, DVM, DACVIM
Juliet R. Gionfriddo, DVM, MS, DACVO
Karen A. Moriello, DVM, DACVD
Jennifer Wardlaw, DVM, DACVS
Practitioner Advisory Board
Progressive practitioners who keep our content
practical, timely, and relevant
Mili Bass, DVM, DABVP
Robin Downing, DVM
Corey Entriken, DVM
Wayne L. Hunthausen, DVM
Thomas McCoy, DVM
Melissa M. Mckendry, DVM, DABVP
Fred L. Metzger Jr., DVM, DABVP
Robert M. Miller, DVM
Gary D. Norsworthy, DVM, DABVP
R. Wayne Randolph, VMD
Michael H. Riegger, DVM, DABVP
David Robbins, DVM
Philip VanVranken, DVM
Laura L. Wade, DVM, DABVP
Veterinary Medicine (ISSN 8750-7943 print; ISSN 1939-1919 online) is published monthly by UBM Advanstar, 131 West First St., Duluth, MN 55802-2065. One year subscription rates: $60 in the United States and Possessions; $72 in Canada and Mexico; $97 in all other countries. Single issue orders: $18 in the United States and Possessions; $22 in Canada and Mexico; $24 in all other countries. Periodicals postage paid at Duluth, MN 55806 and additional mailing offi ces. POSTMASTER: Please send address changes to Veterinary Medicine, P.O. Box 6087, Duluth, MN 55806-6087. Canadian GST Number: R-124213133RT001. Publications Mail Agreement Number: 40612608. Return undeliverable Canadian addresses to: IMEX Global Solutions, P.O. Box 25542, London, ON N6C 6B2, Canada. Printed in the U.S.A. © 2015 UBM Advanstar. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specifi c clients is granted by UBM Advanstar. for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected]. UBM Advanstar provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities which may be of interest to you. If you do not want UBM Advanstar to make your contact information available to third parties for marketing purposes, simply call toll-free (866) 529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from UBM Advanstar’s lists. Outside the United States, please call (218) 740-6477. Veterinary Medicine does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance on such content. Publisher assumes no responsibility for unsolicited manuscripts, photographs, art, and other material. Unsolicited material will not be returned. Address correspondence to Veterinary Medicine, 8033 Flint, Lenexa, KS 66214; (913) 871-3800; e-mail [email protected]. To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
Content Group
Editor/Medicine Channel Director | Mindy Valcarcel
Medical Editor | Heather Lewellen, DVM
Content Manager | Adrienne Wagner
Senior Content Specialist | Alison Fulton
Assistant Content Specialists | Katie James | Matthew Kenwright
Technical Editor | Jennifer Vossman, RVT
Consulting Technical Editor | Avi Blake, DVM
Digital Channel Director | Jessica Zemler
Senior Designer/Web Developer | Ryan Kramer
Art Director | Shawn Stigsell
Multimedia Contributor | Troy Van Horn
Advanstar Veterinary
Vice President/General Manager | Becky Turner Chapman
Group Content Director | Marnette Falley
Medical Director | Theresa Entriken, DVM
Director, Electronic Communications | Mark Eisler
Director, Marketing | Brenda Andresen
Director, The CVC Group | Peggy Shandy Lane
Sales Group
Sales Director | David Doherty
Senior Account Managers, Advertising
Terry Reilly | Chris Larsen
Account Manager, Advertising | Angela Paulovcin
Senior Account Manager, Projects | Jed Bean
Sales and Projects Coordinator | Anne Belcher
Books/Resource Guides | Maureen Cannon(440) 891-2742
List Rental Sales | Renée Schuster(440) 891-2613, [email protected]
Chief Executive Offi cer | Joe Loggia
Executive Vice President, Chief Administrative Offi cer
& Chief Financial Offi cer | Tom Ehardt
Executive Vice President | Georgiann DeCenzo
Executive Vice President | Chris DeMoulin
Executive Vice President, Business Systems | Rebecca Evangelou
Executive Vice President, Human Resources | Julie Molleston
Executive Vice-President, Strategy & Business Development | Mike Alic
Senior Vice President | Tracy Harris
Vice-President, General Manager Pharm/Science Group | Dave Esola
Vice President, Legal | Michael Bernstein
Vice President, Media Operations | Francis Heid
Vice-President, Treasurer & Controller | Adele Hartwick
ES549094_vetm0115_003.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

4 | January 2015 | Veterinary Medicine | dvm360.com
Parasitic concerns:
Mind the gap!New research from CAPC compares veterinarians’ and pet owners’ concerns about various parasites. By Mindy Valcarcel, Editor
In 2014, in an ef ort called Con-
necting with Today’s Clients,
the Companion Animal Parasite
Council (CAPC), supported by Bayer
HealthCare, surveyed U.S. veterinar-
ians, veterinary team members, and
pet owners to gain some insight into
whether all groups are on the same page
when it comes to parasite control.
T ey interviewed 401 practicing
veterinarians and 263 veterinary team
members who work at least 30 hours a
week in practices that see 75% or more
small animals in a nonemergency set-
ting. T ey also interviewed 2,000 dog or
cat owners who had taken their pets to
a veterinarian within the past two years.
Here is a sneak peek showing the
level of concern veterinarians have
about various parasites versus the level
of concern of veterinary owners.
What does this mean? It signals a
need for better communication with
clients about parasite control and con-
cerns in your area. At dvm360.com
/CAPCstudy, we have resources ready
for you, as well as more of this study’s
f ndings from us and our sister publica-
tions—dvm360 magazine, Veterinary
Economics, and Firstline.
83%
96%
75%
70%
86%
38%
34%
32%
29%
28%
45%
62%
43%
41%
57%
biggest gaps in concern for
parasites in dogs
5
1. Giardia species
2. Ascarids, hookworms, and roundworms
3. Coccidia species
4. Demodectic mites
5. Tapeworms
Concern for veterinarians Concern for ownersGap
1. Tapeworms
2. Ascarids, hookworms 3. Ear mites
4. Coccidia species
5. Fleas
93%
89%
92%
65%
94%
42%
39%
35%
29%
24%
51%
50%
56%
37%
71%
biggest gaps in concern for
parasites in cats
5
Concern for veterinarians Concern for ownersGap
EDITOR’S NOTE
ES549104_vetm0115_004.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

ES549673_VETM0115_005_FP.pgs 12.29.2014 15:15 ADV blackyellowmagentacyan

CLINICAL EXPOSURES illuminating images from patient fi les
6 | January 2015 | Veterinary Medicine | dvm360.com
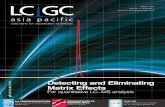
A teratoma in a turkey’s eyeBy Magdalena Szweda, DVM
A 6-week-old male
turkey was presented
for evaluation of an
excrescence the size of a ten-
nis ball (diameter 8 cm) in
the area of the left eye (Figure
1). T e results of a complete
blood count showed evidence
of infection (elevated WBC
count = 49.5 x 109/L; reference
range = 1.7 to 7.5 x 109/L). No
abnormalities were found on
a serum chemistry prof le. Ra-
diographic examination of the
head showed that the tumor
mass was loosely attached to
the sclera but did not pen-
etrate inside the eyeball.
After two days of clinical ob-
servation and therapy, enucle-
ation was performed to remove
the excrescence (Figure 2).
Keep in mind that birds, unlike
mammals, have relatively short
optic nerves, so exaggerated
traction on the globe can result
in damage to the contralateral
optic nerve, causing blindness
in the contralateral eye. Birds
have scleral ossicles, which can
inhibit enucleation.1,2 >>>1. A 6-week-old male turkey with an excrescence the size of a tennis ball in the area of its left eye.
ES549130_vetm0115_006.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

ES550624_VETM0115_007_FP.pgs 01.02.2015 18:46 ADV blackyellowmagentacyan

8 | January 2015 | Veterinary Medicine | dvm360.com
CLINICAL EXPOSURES
T e cornea was incised and the lens and vitreous
were extruded to allow the globe to be collapsed. Intra-
surgical observation revealed that the excrescence was
a tumor attached to the eyeball. All the lacrimal tissue,
the globe, and the eyelid margins were excised.
After excision, the skin was sutured routinely with
a gauze swab inside the empty orbit. T e swab was
changed every day during the 14 days of convalescence.
Some surgeons prefer to use an ocular prosthesis to
prevent the sunken appearance characteristic of avian
enucleation.1 After surgery, the turkey received enro-
f oxacin (10 mg/kg intramuscularly) for 14 days and
celecoxib (10 mg/kg orally) for f ve days. T e sutures
were removed 14 days after the enucleation (Figure 3).
>>>3. The patient 14 days after surgery, before removal of the sutures.
>>>2. A preoperative photo of the tumor mass loosely attached to the sclera.
CAUTION: Federal (USA) law restricts this drug to use by or on the order of a licensed veterinarian.
Description:NEXGARD® (afoxolaner) is available in four sizes of beef-flavored, soft chewables for oral administration to dogs and puppies according to their weight. Each chewable is formulated to provide a minimum afoxolaner dosage of 1.14 mg/lb (2.5 mg/kg). Afoxolaner has the chemical composition 1-Naphthalenecarboxamide, 4-[5- [3-chloro-5-(trifluoromethyl)-phenyl]-4, 5-dihydro-5-(trifluoromethyl)-3-isoxazolyl]-N-[2-oxo-2-[(2,2,2-trifluoroethyl)amino]ethyl.
Indications:NEXGARD kills adult fleas and is indicated for the treatment and prevention of flea infestations (Ctenocephalides felis), and the treatment and control of Black-legged tick (Ixodes scapularis), American Dog tick (Dermacentor variabilis), and Lone Star tick (Amblyomma americanum) infestations in dogs and puppies 8 weeks of age and older, weighing 4 pounds of body weight or greater, for one month.
Dosage and Administration:NEXGARD is given orally once a month, at the minimum dosage of 1.14 mg/lb (2.5 mg/kg).
Dosing Schedule:
NEXGARD can be administered with or without food. Care should be taken that the dog consumes the complete dose, and treated animals should be observed for a few minutes to ensure that part of the dose is not lost or refused. If it is suspected that any of the dose has been lost or if vomiting occurs within two hours of administration, redose with another full dose. If a dose is missed, administer NEXGARD and resume a monthly dosing schedule.
Flea Treatment and Prevention:Treatment with NEXGARD may begin at any time of the year. In areas where fleas are common year-round, monthly treatment with NEXGARD should continue the entire year without interruption.
To minimize the likelihood of flea reinfestation, it is important to treat all animals within a household with an approved flea control product.
Tick Treatment and Control:Treatment with NEXGARD may begin at any time of the year (see Effectiveness).
Contraindications:There are no known contraindications for the use of NEXGARD.
Warnings:Not for use in humans. Keep this and all drugs out of the reach of children. In case of accidental ingestion, contact a physician immediately.
Precautions:The safe use of NEXGARD in breeding, pregnant or lactating dogs has not been evaluated. Use with caution in dogs with a history of seizures (see Adverse Reactions).
Adverse Reactions:In a well-controlled US field study, which included a total of 333 households and 615 treated dogs (415 administered afoxolaner; 200 administered active control), no serious adverse reactions were observed with NEXGARD.
Over the 90-day study period, all observations of potential adverse reactions were recorded. The most frequent reactions reported at an incidence of > 1% within any of the three months of observations are presented in the following table. The most frequently reported adverse reaction was vomiting. The occurrence of vomiting was generally self-limiting and of short duration and tended to decrease with subsequent doses in both groups. Five treated dogs experienced anorexia during the study, and two of those dogs experienced anorexia with the first dose but not subsequent doses.
Table 1: Dogs With Adverse Reactions.
1Number of dogs in the afoxolaner treatment group with the identified abnormality.2Number of dogs in the control group with the identified abnormality.
In the US field study, one dog with a history of seizures experienced a seizure on the same day after receiving the first dose and on the same day after receiving the second dose of NEXGARD. This dog experienced a third seizure one week after receiving the third dose. The dog remained enrolled and completed the study. Another dog with a history of seizures had a seizure 19 days after the third dose of NEXGARD. The dog remained enrolled and completed the study. A third dog with a history of seizures received NEXGARD and experienced no seizures throughout the study.
To report suspected adverse events, for technical assistance or to obtain a copy of the MSDS, contact Merial at 1-888-637-4251 or www.merial.com/nexgard. For additional information about adverse drug experience reporting for animal drugs, contact FDA at 1-888-FDA-VETS or online at http://www.fda.gov/AnimalVeterinary/SafetyHealth.
Mode of Action:Afoxolaner is a member of the isoxazoline family, shown to bind at a binding site to inhibit insect and acarine ligand-gated chloride channels, in particular those gated by the neurotransmitter gamma-aminobutyric acid (GABA), thereby blocking pre- and post-synaptic transfer of chloride ions across cell membranes. Prolonged afoxolaner-induced hyperexcitation results in uncontrolled activity of the central nervous system and death of insects and acarines. The selective toxicity of afoxolaner between insects and acarines and mammals may be inferred by the differential sensitivity of the insects and acarines’ GABA receptors versus mammalian GABA receptors.
Effectiveness:In a well-controlled laboratory study, NEXGARD began to kill fleas four hours after initial administration and demonstrated >99% effectiveness at eight hours. In a separate well-controlled laboratory study, NEXGARD demonstrated 100%effectiveness against adult fleas 24 hours post-infestation for 35 days, and was ≥ 93% effective at 12 hours post-infestation through Day 21, and on Day 35. On Day 28, NEXGARD was 81.1% effective 12 hours post-infestation. Dogs in both the treated and control groups that were infested with fleas on Day -1 generated flea eggs at 12- and 24-hours post-treatment (0-11 eggs and 1-17 eggs in the NEXGARD treated dogs, and 4-90 eggs and 0-118 eggs in the control dogs, at 12- and 24-hours, respectively). At subsequent evaluations post-infestation, fleas from dogs in the treated group were essentially unable to produce any eggs (0-1 eggs) while fleas from dogs in the control group continued to produce eggs (1-141 eggs).
In a 90-day US field study conducted in households with existing flea infestations of varying severity, the effectiveness of NEXGARD against fleas on the Day 30, 60 and 90 visits compared with baseline was 98.0%, 99.7%, and 99.9%, respectively.
Collectively, the data from the three studies (two laboratory and one field) demonstrate that NEXGARD kills fleas before they can lay eggs, thus preventing subsequent flea infestations after the start of treatment of existing flea infestations.
In well-controlled laboratory studies, NEXGARD demonstrated >94% effectiveness against Dermacentor variabilis and Ixodes scapularis, 48 hours post-infestation, and against Amblyomma americanum 72 hours post-infestation, for 30 days.
Animal Safety:In a margin of safety study, NEXGARD was administered orally to 8- to 9-week-old Beagle puppies at 1, 3, and 5 times the maximum exposure dose (6.3 mg/kg) for three treatments every 28 days, followed by three treatments every 14 days, for a total of six treatments. Dogs in the control group were sham-dosed. There were no clinically-relevant effects related to treatment on physical examination, body weight, food consumption, clinical pathology (hematology, clinical chemistries, or coagulation tests), gross pathology, histopathology or organ weights. Vomiting occurred throughout the study, with a similar incidence in the treated and control groups, including one dog in the 5x group that vomited four hours after treatment.
In a well-controlled field study, NEXGARD was used concomitantly with other medications, such as vaccines, anthelmintics, antibiotics (including topicals), steroids, NSAIDS, anesthetics, and antihistamines. No adverse reactions were observed from the concomitant use of NEXGARD with other medications.
Storage Information:Store at or below 30°C (86°F) with excursions permitted up to 40°C (104°F).
How Supplied:NEXGARD is available in four sizes of beef-flavored soft chewables: 11.3, 28.3, 68 or 136 mg afoxolaner. Each chewable size is available in color-coded packages of 1, 3 or 6 beef-flavored chewables.
NADA 141-406, Approved by FDA
Marketed by: Frontline Vet Labs™, a Division of Merial Limited.Duluth, GA 30096-4640 USA
Made in Brazil.
1050-4493-02Rev. 4/2014
N1 % (n=415) N2 % (n=200)
Vomiting (with and without blood) 17 4.1 25 12.5
Dry/Flaky Skin 13 3.1 2 1.0
Diarrhea (with and without blood) 13 3.1 7 3.5
Lethargy 7 1.7 4 2.0
Anorexia 5 1.2 9 4.5
Treatment Group
Afoxolaner Oral active control
®NexGard is a registered trademark, and TMFRONTLINE VET LABS is a trademark, of Merial. ©2014 Merial. All rights reserved.
Body Afoxolaner Per Chewables Weight Chewable (mg) Administered
4.0 to 10.0 lbs. 11.3 One
10.1 to 24.0 lbs. 28.3 One
24.1 to 60.0 lbs. 68 One
60.1 to 121.0 lbs. 136 One
Over 121.0 lbs. Administer the appropriate combination of chewables
ES549131_vetm0115_008.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

Killing fleas and ticks can be just this easy.
With NexGard® (afoxolaner), flea and tick
control is convenient for pet owners since
dogs love taking the soft, beef-flavored chew.1
POWERFUL flea and tick killing all month long
CONVENIENT monthly dosing owners are used to
EASY for owners to give1 and for veterinarians to dispense
Prescription only with anti-diversion technology
IMPORTANT SAFETY INFORMATION: For use in dogs only. The most common adverse reaction is vomiting. Other adverse reactions reported are dry/flaky skin, diarrhea, lethargy, and anorexia. The safe use of NexGard in pregnant, breeding, or lactating dogs has not been evaluated. Use with caution in dogs with a history of seizures.
®NexGard is a registered trademark, and FRONTLINE VET LABS is a trademark, of Merial. ©2015 Merial Limited, Duluth, GA. All rights reserved. NEX15TRADEADA (01/15).
1Data on File at Merial.
See brief summary on page 8
ES549738_VETM0115_009_FP.pgs 12.29.2014 21:12 ADV blackyellowmagentacyan

10 | January 2015 | Veterinary Medicine | dvm360.com
CLINICAL EXPOSURES
Histopathologic examinationMicroscopically, the tumor was
composed of glandular struc-
tures similar to the intestine, cili-
ated epithelium resembling that
of the respiratory system, and
hyaline cartilage that formed
various sizes of islands scattered
throughout the tumor mass.
T ere were also areas of the
embryonal hyaline cartilage and
endochondral ossif cation. T e
ossicles in the avian sclera were
focally hyperplastic. All the tis-
sues comprising the tumor were
mature. Based on these f ndings,
a teratoma was diagnosed.
DiscussionTeratomas arise from totipo-
tential germ cells and can give
rise to two or more embryonic
layers (endoderm, mesoderm,
ectoderm) with dif erent types
of tissues being present.3 T ese
tumors are not of uniform
histologic structure but are a
mixture of various randomly
intermingled tissues. T e exact
mechanism of development
of teratomas is still unclear.
Teratomas are classif ed as im-
mature (the tissue is not fully
mature histologically; malig-
nant) or mature (comprised
of mature, fully dif erentiated
tissues; benign).4
In this case, histopathologic
examination together with the
bird’s young age suggested that
the tumor could be congenital.
T e head surface location of the
teratoma is rarely described in
avian species.5-8 T e most com-
mon locations in birds are the
ovary, testicle, and coelom.9-11
REFERENCES
1. Rosenthal KL, Forbes NA, Frye FL, et
al. Rapid review of exotic animal medi-
cine and husbandry. London, Manson
Publishing, 2008.
2. Gabrisch K, Zwart P. Praktyka
kliniczna: Zwierzeta Egzotyczne. Łódz:
Galaktyka, 2009.
3. Kennedy PC, Cullen JM, Edwards JF.
Histological classifi cation of tumors of
the genital system of domestic animals
(World Health Organization Classifi ca-
tion of Tumors of Domestic Animals).
2nd Series, Volume IV. Washington:
American Registry of Pathology, 1998.
4. Lo Curto M, D’Angelo P, Cecchetto G,
et al. Mature and immature teratomas:
results of the fi rst paediatric Italian study.
Pediat Surg Int 2007;23(4)315-322.
5. Bolte AL, Burkhardt E. A teratoma in a
Muscovy duck (Cairina moschata). Avian
Pathol 2000;29(3):237-239.
6. Cullen JM, Newbold JE, Sherman GJ.
A teratoma in a duck infected congeni-
tally with duck hepatitis B virus. Avian Dis
1991;35(3):638-641.
7. Ford SL, Wentz S, Garner M. Intracoe-
lomic teratoma in a juvenile bald eagle
(Haliaeetus leucocephalus). J Avian Med
Surg 2006;20(3):175-179.
8. Homer BL, Riggs MW. Cranial
teratomas in two domestic ducks (Anas
platyrhynchos domesticus). Avian Dis
1991;35(4):994-998.
9. Cooper JE, Watson J, Payne LN.
A mixed cell tumour in a Seychelles
kestrel (Falco araea). Avian Pathol
1987;7(4):651-658.
10. Gupta BN. Teratoma in a chicken
(Gallus domesticus). Avian Dis
1976;20(4):761-768.
11. Hamir AN. Teratoma in a duck. Vet
Rec 1985;117(12):314.
Magdalena Szweda, DVM
Department of Pathophysiology
Forensic Veterinary Medicine
and Administration
Faculty of Veterinary Medicine
University of Warmia and Mazury
Olsztyn, Poland
Teratomas are not of uniform
histologic structure but are a
mixture of various randomly
intermingled tissues.
Speaking of poultry ... Getting lots of requests to treat
backyard chickens? At the 2015
CVC San Diego, April 23-26, we have
a whole lecture series dedicated
to backyard poultry conducted by
Lauren Powers, DVM, DABVP (avian
practice). Get more details and
register to attend at thecvc.com.
GETTY IMAGES/FINN O’HARA
ES549132_vetm0115_010.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

CvC highlight
dvm360.com | veterinary Medicine | January 2015 | 11
Canine leptospirosis: When to suspect it, how to manage itYou know that leptospirosis can be a chameleon. Here’s a review to help you know when to suspect it and what to do about it. By Mary Bowles, DVM, DACVIM
The dog is the primary
companion animal in the
United States afected
by Leptospira species infection
and can experience illness that
ranges from mild to severe. Te
risk of infection has been shown
to be greater for intact male,
outdoor, working dogs, but
dogs of any age, breed, or sex
can become infected. Even dogs
that live predominantly in the
house can become infected—
wild animals act as reservoirs
for some serovars, and increas-
ing encroachment on wildlife
habitats by people increases
the likelihood of interaction
between pets and wildlife.
Although transmission can
occur through bite wounds
from infected animals, most
dogs acquire infection when
their mucous membranes or
abraded skin comes into contact
with soil, food, water, or other
materials contaminated by urine
from Leptospira species-infected
domestic or wild animals.
Clinical signsClinical signs seen with lepto-
spirosis can be mild or severe.
Although general manifesta-
tions of illness such as fever
and malaise may be present,
signs related to the acute
development of renal failure or
hepatopathy should raise your
index of suspicion for leptospi-
rosis. Manifestations of acute
renal failure frequently include
polyuria/polydipsia (PU/PD)
or oliguria/anuria, gastrointes-
tinal (GI) signs, and abdominal
pain. PU/PD can also be seen
without renal failure and may
be a consequence of acquired
nephrogenic diabetes insipidus.
Manifestations of hepatopathy
often include GI signs, icterus,
and bilirubinuria.
Be sure to perform an oph-
thalmologic evaluation since
conjunctivitis and uveitis can
be identifed in some patients.
Reluctance to move related to
muscle pain may be present.
Also be aware that vasculitis
can occur,
producing pe-
ripheral edema
or cavitary ef-
fusion and hemorrhage
manifested as petechiae,
GI or urinary tract
bleeding, hemoptysis,
or epistaxis. In some
cases, tachypnea or
dyspnea may develop
because of pulmonary
hemorrhage or acute respi-
ratory distress syndrome.
HistoryAsk about the patient’s environ-
ment, including travel history
and the status of additional
household pets. Determine the
pet’s vaccination status—if lep-
tospirosis is a potential diagno-
sis, information about vaccina-
tion for leptospirosis, including
the date of administration
and the serovars included in
the vaccine, could be particu-
larly important. Although most
patients with leptospirosis have
GeTTY imaGes/mlorenzpHoToGrapHY
ES549144_vetm0115_011.pgs 12.24.2014 18:51 ADV blackyellowmagentacyan

CvC highlight
12 | January 2015 | veterinary Medicine | dvm360.com
a history and clinical fndings
compatible with acute disease,
leptospirosis should also be
considered as an underlying
cause in patients with chronic
renal and hepatic disease.
Laboratory findingsTe most common clinicopath-
ologic abnormalities identifed
in patients with leptospirosis
are related to acute kidney and
liver injury. Azotemia has been
reported in ≥ 80% of afected
dogs in multiple regions of the
United States and Canada.1
Elevated liver enzyme activities
and bilirubinemia frequently
accompany azotemia—a com-
bination of abnormalities that
should prompt you to move
leptospirosis higher on your list
of diferential diagnoses that
should also include toxicoses,
neoplasia, hypoadrenocorti-
cism, and other infectious dis-
eases such as systemic mycoses.
Evidence of renal failure is fur-
ther supported by the frequent
fndings of hyperphosphatemia
and isosthenuria along with the
possible fndings of hyposthenu-
ria, glucosuria, proteinuria, and
cylindruria. Multiple electrolyte
abnormalities may be pres-
ent, particularly hypokalemia.
However, hyperkalemia can be
found if the patient develops
oliguria or anuria.
One of the most common
complete blood count (CBC)
fndings is thrombocytopenia.
Neutrophilia with or without a
left shift and anemia may also
be identifed. Te anemia is
generally mildly to moderately
nonregenerative but occasion-
ally can be severe and regen-
erative in instances in which
GI or pulmonary hemorrhage
has occurred. In addition to
thrombocytopenia, other co-
agulation profle abnormalities
may be found such as increases
in fbrin degradation products,
D-dimer, prothrombin time,
and partial thromboplasin time
values, especially if disseminat-
ed intravascular coagulopathy
becomes a complication.
Imaging and histologic examinationImaging and histopathology
can be considered as additional
diagnostic procedures in cases
of suspected leptospirosis. Re-
nal ultrasonographic fndings
compatible with Leptospira spe-
cies infection include bilateral
renal enlargement, increased
renal echogenicity that some-
times includes a more distinct
band in the medullary area,
and perirenal fuid. Toracic
radiography frequently reveals
difuse lung changes that can
include an interstitial or alveo-
lar pattern.
Renal and hepatic histologic
fndings in leptospirosis typi-
cally include varying degrees of
renal interstitial nephritis, renal
tubular necrosis, neutrophilic
periportal hepatitis, and hepatic
necrosis. Leptospira species or-
ganisms can sometimes be iden-
tifed in tissue by using special
stains (e.g. silver, peroxidase).
Specialized tests
MAT. Te most common
diagnostic test performed in
patients suspected of having
leptospirosis is the microscopic
agglutination test (MAT), which
uses patient sera and multiple
serovars to detect antibody
formation in acute and conva-
lescent phases of illness. Te
highest serum dilution caus-
ing 50% agglutination of the
organisms for each serovar
tested is reported. False negative
results can occur if the infecting
serovar has not been included
in the serovars tested. Tis pos-
sibility will be decreased if the
laboratory selected for testing
uses serovars more commonly
found in the region from which
the patient sample originated.
For a variety of reasons, it
has been difcult to establish
a precise titer level indicat-
ing defnitive infection with a
particular serovar. However,
a single titer > 800 is highly
suggestive of infection with
the leptospire being tested,
especially if compatible clinical
signs are present and no recent
vaccination for leptospirosis
has occurred. Cross-reactivity
can occur among serovars and
lower titers, depending on the
time of vaccination, are often
present for serovars included
Hear all
about it!to hear Dr.
Bowles describe
how to diagnose
leptospirosis
using microscopic
agglutination
testing, scan the QR
code below or visit
dvm360.com
/CVC14Bowles.
ES549145_vetm0115_012.pgs 12.24.2014 18:51 ADV blackyellowmagentacyan

© 2014 Abbott Laboratories. AlphaTRAK is a trademark of Abbott Group of companies in various jurisdictions. AT2-2109
Humans sharea lot of things with their pets.Blood glucose meters shouldn’t be one of them.
Portable blood glucose meters designed for blood glucose monitoring in humans are not validated for veterinary use on pets.
AlphaTRAK is specifi cally calibrated and validated for dogs and cats for accurate readings.
Now with a reduced price, accuracy is affordable for your practice and your clients. With a recommended Starter Kit price of just $70 to pet owners, there is no better time than now to upgrade to AlphaTRAK.
For more information call 866-257-8807 or visit www.AlphaTRAKmeter.com
NOW AT A REDUCED
PRICE
ES550618_VETM0115_013_FP.pgs 01.02.2015 18:44 ADV blackyellowmagentacyan

CvC highlight
14 | January 2015 | veterinary Medicine | dvm360.com
in the vaccine. MAT results can be
negative in the acute phase of illness,
so obtaining convalescent titers about
two to four weeks after acute phase
testing is advisable. Remember when
evaluating acute and convalesent titers
that a fourfold increase or decrease in
Leptospira species serovar titer is con-
sidered indicative of recent infection.
PCR and culture. Leptospirosis can
also be diagnosed by polymerase chain
reaction (PCR) and culture methods.
Tese methods can be especially useful
in acute phase patients with negative
or questionable MAT results that have
not yet received antimicrobial therapy
and patients with chronic renal or he-
patic disease. Although blood is usu-
ally the sample of choice for PCR and
culture techniques, a urine sample is
often a better choice later in the course
of disease when organisms reach a
higher concentration in the urine.
Although culture can be a more
accurate way of serotyping Leptospira
species organisms, this diagnostic
procedure requires aseptic sample
collection, special culture media and
handling, and three to six months for
growth and identifcation of leptospires.
PCR testing will identify Leptospira
nucleic acid but not necessarily the
specifc serovar. Both false positive and
negative results can occur with PCR
testing, making concurrent acute and
convalescent titer evaluation desirable.
TreatmentIf leptospirosis is a reasonable diferen-
tial diagnosis, initiate appropriate ther-
apy immediately without waiting for
confrmation of the diagnosis. Hospital-
ization is generally needed for adequate
treatment. Terapy most commonly
encompasses specifc therapy for the
Leptospira species organism as well as
supportive care for acute renal failure
and, in some cases, hepatic damage.
Keep in mind that leptospirosis is a
zoonotic disease and that appropriate
measures should be taken to prevent
disease transmission through disinfec-
tion and protected handling of both the
patient and waste materials. In addition,
treatment of other dogs in the patient’s
household with a two-week course of
doxycycline is recommended.
PrognosisTe prognosis for most patients is
favorable for recovery with appropriate
medical care. Discharge from the hos-
pital setting can occur after tapering
fuid therapy and when the patient is
stable, is not showing serious outward
clinical signs of illness, has normal
or consistently improved laboratory
values, and is able to adequately eat
and drink. Azotemia may not com-
pletely resolve for weeks. Occasion-
ally, patients will sustain permanent
impairment of kidney function.
Recognition of which serovar is
most likely responsible for infection of
the patient will help identify envi-
ronmental risk factors for reinfection
and infection of additional dogs in the
household. Annual vaccination of the
recovered patient with a four-serovar
vaccine starting one year after recov-
ery is currently recommended.2
References
1. Greene Ce. leptospirosis. in: Infectious
diseases of the dog and cat. 3rd ed. philadelphia:
elsevier, 2006.
2. sykes Je, Hartmann K, lunn KF, et al. 2010
aCVim small animal Consensus statement
on leptospirosis: Diagnosis, epidemiology,
Treatment, and prevention. J Vet Intern Med
2011;25(1):1-13.
Mary Bowles, DVM, DACVIM
Emeritus Faculty
Department of Veterinary
Clinical Sciences
Center for Veterinary Health Sciences
Oklahoma State University
Stillwater, Oklahoma
although leptospirosis appears to be primarily a disease in dogs in the
household pet population, cats can be infected but have been thought to
experience mild manifestations of disease. Leptospira canicola, pomona,
and grippotyphosa have been isolated from cats. leptospires have been
identified in the blood and urine of experimentally infected cats along with
evidence of renal and hepatic inflammation.
results from a recent Canadian study looking at Leptospira species in
healthy cats and cats with kidney disease suggested that Leptospira or-
ganisms may play a role in the development of acute and chronic kidney
disease in cats and that cats may play a role in transmission of these or-
ganisms through urine shedding.1 in endemic areas, leptospirosis should
be a consideration in cats with evidence of renal or hepatic disease or
nonspecific illness. Doxycycline therapy may be an effective means of
treating cats with leptospirosis.
Reference
1. rodriguez J, Blais mC, lapointe C, et al. serologic and urinary pCr survey of leptospirosis
in healthy cats and cats with kidney disease. J Vet Intern Med 2014;28(2):284-293.
Leptospirosis in cats
ES549143_vetm0115_014.pgs 12.24.2014 18:51 ADV blackyellowmagentacyan

LEASH TRAINING peer-reviewed
dvm360.com | Veterinary Medicine | January 2015 | 15GETTY IMAGES/ERIC ISSELÉE
A better walk: Training dogs NOT to lunge, growl, and pull on a leashNew Year’s resolutions often involve getting more exercise—and this includes dogs as well. But reactivity on a leash is a common problem, making it less likely for owners to venture out with their dogs. This step-by-step training plan will help you help owners take control and enjoy walking their dogs again. By Wayne Hunthausen, DVM
M s. G’s dog, Tommy,
was slowly becom-
ing
grossly over-
weight. He
weighed 10 lb more
than the last time I saw him
and at least 20 lb more
than he should weigh.
“Tommy needs to pass on
the midnight snacks,” I told her,
“but just as important, he needs
to be getting more exercise.”
Ms. G appeared distressed
as well as concerned. “I know
he needs more exercise,” she
said, “and I want to get him
out more. But he’s a big boy
and I just can’t control him
when I walk him on a leash.
He constantly barks and lunges
ES549100_vetm0115_015.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

LEASH TRAINING peer-reviewed
16 | January 2015 | Veterinary Medicine | dvm360.com
at everything he sees. It’s so
embarrassing!”
Ms. G is not alone in her
dilemma. Reactivity on a leash
is a common canine behavior
problem and is often stressful
for owners. It can be caused by
a variety of underlying prob-
lems, including aggression,
fear, unruliness, play-soliciting
behavior, or inadequate train-
ing. T e problem can usually
be successfully treated if the
owners have the commitment,
tools, and correct information
to get the job done. Outlined
below is a typical plan that I use
to address this problem.
Training overviewT e purpose of these exercises
is to give owners more control
over their dogs on walks and
to replace lunging, barking, or
aggressive or fearful behav-
iors with calm, quiet, and
relaxed behaviors. Training at
a distance beyond the response
threshold (see “Response
threshold distances” below) is
absolutely necessary. Dogs are
less manageable and have dif-
f culty learning when they are
highly aroused.
Owners need to stay as
relaxed as possible and think
of these exercises as games to
play with their dogs. If aggres-
sion is part of a dog’s reactive
behavior, the person walk-
ing the dog is responsible for
others’ safety and must ensure
that leashes and halters are
secure and that there is no op-
portunity for physical contact
with other dogs or people.
PreparationBefore the social conditioning
process begins, the dog must be
taught to dependably come, sit,
stay, and heel on a leash. T is
training may require the help
of a private trainer since these
dogs usually do poorly in a class
situation. It should be noted
that throughout the entire
training process, only positive
reinforcement types of training
techniques should be used.
Next, owners need to teach
their dogs that they are in
control. By setting boundaries,
the owner will obtain better
compliance and dependability
from obedience cues. T is can
be accomplished by initiating a
social structure or a nothing-in-
life-is-free program.
As part of this program, the
owner should request that the
dog sit before getting any-
thing it wants or needs, the
dog should be ignored when
it demands attention, and the
dog should frequently be asked
to stay before being allowed to
follow owners around the home
or yard or before going in or
out of the home. During train-
ing, all commands should be
given in an upbeat and relaxed
tone of voice.
ToolsIn addition to having a social
conditioning plan (see “Phase
1: Counterconditioning at a
distance” below to begin the
training plan), other tools that
owners will need when train-
ing their dogs against reactive
behaviors are positive rein-
forcers and instruments for
maintaining physical control
(e.g. an appropriate leash, a
head halter).
Reinforcers. Owners must
determine their dogs’ most
desirable food (e.g. very tasty
If aggression is part of a dog’s reactive
behavior, the person walking the
dog is responsible for others’ safety
and must ensure that leashes and
halters are secure and that there is no
opportunity for physical contact with
other dogs or people.
ES549105_vetm0115_016.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

Rapinovet™ (propofol)
Smooth induction. Quick recovery. Great value.
©2014 Bayer HealthCare LLC, Animal Health, Shawnee Mission, Kansas 66201
Bayer (reg’d), the Bayer Cross (reg’d) and Rapinovet™ are trademarks of Bayer. RP141006
For customer service or to place an order, call 1-800-633-3796. For product information, call 1-800-422-9874.
CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
WARNINGS: Induction of anesthesia with Rapinovet™ injection is frequently associated with apnea and respiratory depression. Hypotension
and oxygen desaturation can occur also, especially following rapid bolus administration. Apnea is observed less frequently following
maintenance doses of Rapinovet™ injection when given as the sole maintenance agent, or when a maintenance dose is administered during
inhalant anesthesia. To report adverse efects, call 1-800-422-9874.
When using Rapinovet™ injection, patients should be continuously monitored, and facilities for the maintenance of a patent airway, artificial ventilation, and oxygen supplementation must be immediately available. The clinical use of propofol without available supplemental oxygen and artificial ventilation has not been adequately evaluated and is not recommended.See brief summary on page 18
ES549698_VETM0115_017_FP.pgs 12.29.2014 15:37 ADV blackyellowmagentacyan

18 | January 2015 | Veterinary Medicine | dvm360.com
LEASH TRAINING peer-reviewed
dog treats, freeze-dried liver, cooked chicken or turkey,
cheese, fat-free turkey hot dogs) and give that food only
during the dogs’ social and obedience conditioning
training. It is helpful to always say a specif c word or
phrase, such as “good dog,” as the food is given. By fre-
quently associating specif c words with food, the words
can be used as relatively strong reinforcers even when
food is not present.
Physical control. To maintain physical control of dogs
during training, owners should keep their dogs on 4- to
6-ft leashes. Owners should have one hand in the loop,
and the other hand should be holding the leash a few
feet from the collar. Retractable leashes are unreliable
and unwieldy and should not be used. Devices that
cause discomfort—such as pinch collars, shock collars,
and choke collars—should be avoided because own-
ers want their dogs to develop positive associations
with people or other dogs they react toward and avoid
unpleasant associations. Leash corrections or leash pops
are not appropriate.
If more control is needed, the dog should be trained to
wear a head halter. Owners may also consider a basket
muzzle if there is any chance an aggressive dog might
inadvertently have contact with another person or dog.
Response threshold distancesT ere are two threshold distances of concern: orienting
threshold distance and reactive threshold distance. Train-
ing takes place between the two threshold distances.
T e orienting threshold distance is the distance at
which the dog barely recognizes and begins to focus
toward the trigger stimulus (e.g. dog, person, bike). T is
distance should be signif cantly farther than the distance
at which the owner begins to lose control of the dog.
T e reactive threshold distance is the distance at
which the dog begins to exhibit the unwanted behaviors
(e.g. barking, growling, lunging). T is distance may vary
depending on the stimulus. For example, a dog that is
aggressive to people might be reactive to most men at
100 ft but reactive to men with hats at 60 ft. Or a dog
that is reactive to other dogs might react to large dogs at
a farther distance than it does to small dogs.
For Animals Only
Rapinovet™ (propofol) Anesthetic InjectionEmulsion for intravenous use in dogs and cats.
BRIEF SUMMARY: Before using Rapinovet™ (propofol), please consult the product insert, a summary of which follows:
CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
WARNINGS: Induction of anesthesia with Rapinovet™ injection is frequently associated with apnea and respiratory
depression. Hypotension and oxygen desaturation can occur also, especially following rapid bolus administration.
Apnea is observed less frequently following maintenance doses of Rapinovet™ injection when given as the sole
maintenance agent, or when a maintenance dose is administered during inhalant anesthesia.
When using Rapinovet™ injection, patients should be continuously monitored, and facilities for
the maintenance of a patent airway, artificial ventilation, and oxygen supplementation must be
immediately available. The clinical use of propofol without available supplemental oxygen and
artificial ventilation has not been adequately evaluated and is not recommended.
SIDE EFFECTS: The primary side effect of Rapinovet™ injection in dogs is respiratory depression and apnea. Apnea was
observed in 20% of the dog cases in the clinical trial. Apnea was observed in 1.4% of the cat cases in the clinical trial.
All apnea cases responded satisfactorily to oxygen supplementation and/or controlled ventilation.
The primary side effect of Rapinovet™ injection in cats is paddling during recovery. Paddling was observed in 11% of
the cat cases in the clinical trial.
Other transient side effects in dogs or cats are observed infrequently or rarely:
t�Respiratory:�QBOUJOH �SFWFSTF�TOFF[JOH �DZBOPTJT�t�Musculoskeletal: paddling during recovery, tremors, tenseness,
NPWFNFOUT � GBTDJDVMBUJPOT�t�Cardiovascular: bradycardia, hypotension, cyanosis, tachycardia, premature ventricular
DPOUSBDUJPOT� t�Central Nervous System:�FYDJUBUJPO �PQJTUIPUPOVT �TFJ[VSF� t� Injection Site:�QBJO�EVSJOH� JOKFDUJPO� t�
Gastrointestinal:�FNFTJT�SFUDIJOH� t� Other: rubbing at face or nose during recovery, vocalization during recovery,
chewing or licking the injection site during recovery.
PRECAUTIONS:
1. Rapinovet™ injection contains no antimicrobial preservatives. Strict aseptic techniques must always be maintained
during handling since the vehicle is capable of supporting rapid growth of microorganisms. Failure to follow aseptic
handling procedures may result in microbial contamination causing fever, infection/sepsis, and/or life-threatening
illness. Do not use if contamination is suspected.
2. When using Rapinovet™ injection, patients should be continuously monitored, and facilities for the maintenance
of a patent airway, artificial ventilation, and oxygen supplementation must be immediately available. The clinical use
of propofol without available supplemental oxygen and artificial ventilation has not been adequately evaluated and is
not recommended.
3. Anesthesia effects: Careful monitoring of the patient is necessary when using Rapinovet™ injection as a
maintenance anesthetic due to the possibility of rapid arousal. Apnea may occur following maintenance doses of
Rapinovet™ injection.
4. Physiological effects: During induction of anesthesia, mild hypotension and increased heart rate may occur when
Rapinovet™ injection is used alone.
5. Premedicants: Premedicants may increase the anesthetic or sedative effect of Rapinovet™ injection and result in
more pronounced changes in systolic, diastolic, and mean arterial blood pressures. The use of ketamine (an approved
compound for restraint in cats) is not recommended as a preanesthetic prior to propofol due to an increased number of
patients experiencing apnea.
6. Breeding Animals: Adequate data concerning the safe use of Rapinovet™ injection in pregnant, lactating, and
breeding dogs and cats have not been obtained. Propofol crosses the placenta, and as with other general anesthetic
agents, the administration of propofol may be associated with neonatal depression.
7. Puppies and Kittens: The use of propofol has not been evaluated in puppies or kittens.
8. Compromised or debilitated dogs and cats: Doses may need adjustment for geriatric or debilitated patients. The
administration of Rapinovet™ injection to patients with renal failure and/or hepatic failure has not been evaluated.
As with other anesthetic agents, caution should be exercised in dogs or cats with cardiac, respiratory, renal or hepatic
impairment, or in hypovolemic or debilitated dogs and cats.
9. Sighthounds: Rapinovet™ injection induction followed by inhalant anesthetic agents produced satisfactory
anesthesia and recovery times in sighthounds. Propofol alone in 6 greyhounds and 7 non-greyhounds showed
satisfactory, but longer recovery times in the greyhounds (averages of 47 and 18 minutes, respectively).2 In a propofol
pharmacokinetics study, greyhounds had higher propofol levels in plasma, a lower volume of distribution, slower total
body clearance rates, and longer recovery times than did mixed-breed dogs. The elimination half-life was similar in both
groups.3
10. Arrhythmogenicity: In one study in dogs, propofol increased myocardial sensitivity to the development of
epinephrine-induced ventricular arrhythmias in a manner similar to other anesthetics.4
11. Consecutive day treatment: Heinz bodies increased dramatically in cats following repeat administration of propofol
on consecutive days and were associated with decreases in RBC count and hematocrit. Large numbers of Heinz bodies
can lead to hemolytic anemia.5,6 In one study in cats, treatment with propofol once a day for 3 days led to a marked
increase in Heinz bodies. Treatment for 5 or more consecutive days resulted in generalized malaise and/or facial edema;
clinical signs of illness resolved within 24 to 48 hours after cessation of propofol.
12. Concurrent Medication: No significant adverse interactions with commonly used drugs have been observed.
13. Perivascular Administration: Perivascular administration does not produce local tissue reaction.
CONTRAINDICTIONS: Rapinovet™ injection is contraindicated in dogs and cats with a known hypersensitivity to
propofol or its components, or when general anesthesia or sedation are contraindicated.
HUMAN USER SAFETY: Not for human use. Keep out of reach of children.
Rapinovet™ injection should be managed to prevent the risk of diversion, through such measures as restriction of access
and the use of drug accountability procedures appropriate to the clinical setting. Rare cases of self-administration of
propofol have been reported, including dose-related fatalities.
The material safety data sheet (MSDS) contains more detailed occupational safety information. For customer service,
and/or a copy of the MSDS, call 1-800-633-3796. To report adverse effects, call 1-800-422-9874.
/"%"����������t��/FU�$POUFOUT�����N-��t���/%$�������������
Bayer (reg’d), the Bayer Cross (reg’d) and Rapinovet are trademarks of Bayer.
Mfd. In Italy For: Bayer HealthCare LLC, Shawnee Mission, KS 66201 Rev0913 52398B
ES549666_vetm0115_018.pgs 12.26.2014 19:50 ADV blackyellowmagentacyan

LEASH TRAINING peer-reviewed
dvm360.com | Veterinary Medicine | January 2015 | 19
Phase 1: Counterconditioning at a distanceOwners should begin by walk-
ing their dogs in relatively
quiet spots where trigger stimuli
appear intermittently. (See the
sidebar “Training away from the
neighborhood.”) Crowded areas
should be avoided. Varying the
time of the walk can be helpful,
but owners should make sure it
is at a time when there is a low
density of people or dogs. Own-
ers should be careful to keep
their dogs beyond the reactive
threshold distance.
When a dog orients toward
a stimulus, the owner should
immediately say the dog’s name
in an upbeat tone and present a
treat at the same time. T e owner
should request the dog sit or stay
for no more than two seconds,
give the treat, and say, “good dog.”
T e owner and dog should then
continue slowly walking ahead.
When the dog orients toward
the stimulus again, the sequence
should be repeated.
Before the stimulus crosses
the second threshold distance
(reactive threshold distance)
and the dog becomes reac-
tive, the owner should turn
with the dog and walk in the
opposite direction or down a
side street. Over time, the dog
should gradually be allowed to
get closer to the stimulus before
changing direction. (Hint:
T e dog is getting close to its
personal reactive threshold if it
takes the treat slowly or overly
rough or fast, is slow to sit,
whines, yawns, or maintains a
strong focus on the stimulus
even while taking the food.)
Phase 2: Passing by across the streetOnce the dog will consistently
perform a relaxed sit or stay
about 40 ft from the stimulus,
the next step is to continue to
walk straight ahead but across
the street from the stimulus
as the stimulus passes in the
opposite direction. T e owner
should request the dog sit or
stay for treats several times as
he or she walks the dog in the
direction of the stimulus. When
about 40 ft from the stimulus,
the owner should place a large
treat in front the dog’s nose, re-
peatedly say “heel” in an excited
and upbeat tone, and briskly
walk forward, keeping the dog
Social conditioning training does not always
have to take place on neighborhood side-
walks, and it can be benefi cial to work in a
wide variety of environments. In some areas,
especially those where the neighborhood envi-
ronment is congested or busy, it may be help-
ful to actually begin away from home. Owners
can perform the training exercises wherever
there might be a trigger stimulus. Here are
some instructions to give owners when imple-
menting this training in other environments.
Walking trails> Take a position in an open area near the
trail at the orienting threshold distance.
> Ask the dog to sit or stay for a treat when-
ever it sees a trigger stimulus.
> Gradually move closer to the trail.
Malls> Train dogs during quiet times of the day.
> Take a position along the edge of the
parking lot at the orienting threshold
distance.
> Ask the dog to sit or stay for a treat
whenever it sees a trigger stimulus step
out of a car or walk out of the mall toward
the dog.
> Gradually move closer, but not into
the mall.
Training away from the neighborhood
ES549103_vetm0115_019.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

LEASH TRAINING peer-reviewed
20 | January 2015 | Veterinary Medicine | dvm360.com
Help owners treat their dog’s reactive behav-
iors—whether the dog is exhibiting aggres-
sion, fear, or unruly behavior—by recom-
mending they follow these ABCs.
Avoidance Owners should manage their dogs and the
environment so that the dogs have little or no
opportunity to perform the undesirable be-
haviors. Avoidance keeps situations safe and
prevents the problem from worsening.
Behavioral control Owners should review obedience training, set
social boundaries, and institute a nothing-in-
life-is-free program to maintain more control
over an aggressive or unruly dog. Putting the
owners in control takes the weight off the
shoulders of the fearful dog because it learns
its owners control social situations and it does
not need to assert control.
Condition desirable behaviorReplace problem behaviors with acceptable
behaviors by using desensitization, counter-
conditioning, and operant training methods
that emphasize positive methods and avoid
aversive ones.
Desensitization. The process of diminish-
ing responsiveness to a stimulus through
repeated exposure to it at a low enough level
that no or minimal response is seen.
Counterconditioning. The replacement
of an unwanted behavior or response to
a stimulus with a desirable behavior or
response by associating something positive
with the stimulus.
Operant conditioning. A method of
learning that occurs through rewards and
punishments for a behavior. Through these
rewards and punishments, an association
is made between a behavior and a con-
sequence for that behavior, causing the
behavior to either increase or decrease in
frequency. It is sometimes referred to as
instrumental conditioning.
Resources for these behavior modifi cation techniques> Bowen J, Heath S. Learning theory and
behaviour modifi cation. In: Behaviour prob-
lems in small animals. Edinburgh, Scotland:
Elsevier, 2005;37-48.
> Lindsay SR. Handbook of applied dog
behavior and training. Vol. 1-3. Ames,
Iowa: Iowa State University Press, 2000,
2001, 2005.
> Mills DS. Training and learning protocols. In:
Horwitz DF, Mills DS, ed. BSAVA manual of
canine and feline behavioural medicine. 2nd
ed. Gloucester, UK: BSAVA, 2009;49–64.
> Pryor K. Don’t shoot the dog. The new art of
dog training. Gloucester: Ringpress, 2002.
> Pryor K. Reaching the animal mind: clicker
training and what it teaches us about all
animals. New York: Scribner, 2009.
> Reid P. Excel-erated leaning. Explaining in
plain English how dogs learn and how best
to teach them. Oakland, California: James
and Kenneth Publishers, 1996.
The ABCs of treating reactive behaviors
ES549106_vetm0115_020.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

dvm360.com | Veterinary Medicine | January 2015 | 21
LEASH TRAINING peer-reviewed
oriented toward the food and
its nose pointing straight ahead.
Phase 3: Sitting or staying beside the sidewalkWhen the dog consistently
ignores the stimulus across the
street, the owner can proceed
to Phase 3. As the stimulus
approaches directly toward the
dog from the front, the dog is
commanded to sit or stay at a
position about 20 ft to the side
of the sidewalk. A treat is held
in front of the dog’s nose until
the stimulus passes, and then
the dog is given the treat and re-
leased. An alternative approach
for a dog that might have dif-
f culty maintaining a long stay
would be to have the owner
give a series of sit or stay cues
for treats as the stimulus passes.
Slowly and gradually, the dog
moves closer to the sidewalk
during subsequent passes.
Other considerations
No scolding. Owners should
avoid scolding dogs or saying,
“leave it,” “watch me,” or “look
at me,” in tense or agitated
tones as a stimulus approach-
es. T ese types of responses
will typically increase a dog’s
arousal and reactivity. Owners
should maintain safe con-
trol, stay beyond the reactive
threshold distance, be calm but
f rm, and try to keep the leash
as loose as possible.
Exhibiting reactive behav-
ior. If a dog exhibits a reactive
behavior (lunging, barking,
growling) during a walk, the
owner should immediately turn
and briskly walk or jog out of
the situation. T e owner should
be f rm and calm and not yell,
scold, give a leash correction, or
punish the dog.
Stranger petting. If a dog has a
history of aggression or a strong
fear response and someone asks
to pet the dog during a walk, the
owner should decline. However,
if the owner, the approach-
ing person, and the dog are all
relaxed, the owner can say, “I’m
training this dog, so you can’t
pet him, but would you mind
tossing treats to him when I
ask him to sit?” and allow the
person to toss a treat to the dog.
If anyone, including the dog, is
not relaxed, the owner should
decline the request, maintain
a safe distance, and walk away
with the dog.
Territorial behavior. Allow-
ing a dog to aggressively lunge,
bark, or growl while standing
at windows, fence lines, or on
tie-downs in the yard will undo
the training done on walks. T e
dog should not be given the
opportunity to perform these
behaviors. Preventing or block-
ing access to window, doors,
and fences can prevent this be-
havior. If this is not possible and
the reactive behavior occurs, it
should be interrupted. T at can
be done by having the owner
use novel, loud noises that
are appropriate for the dog’s
temperament (e.g. a shake can,
a hiker’s emergency whistle,
InteroSTOP—Meridian Animal
Health, an air horn) or by hav-
ing the dog wear a citronella
spray antibark collar. Shock
collars should be avoided.
Once the dog stops the
unacceptable behavior, it can be
redirected to another acceptable
behavior. T e owner should al-
ways reward the dog with praise
or a treat if the dog notices dogs,
people, or other stimuli passing
by the home and does not react.
Medication. Drugs may be
necessary for dogs with unsta-
ble temperaments or for dogs in
situations in which it is dif cult
or impossible to stay beyond
the reactive threshold distance
(e.g. dogs with extremely long
reactive threshold distances,
dogs that live in condominiums
or apartment complexes, dogs
that must be walked in crowded
urban areas).
If medication is
needed,
I usually
prescribe a
selective sero-
tonin reuptake
inhibitor (SSRI). Own-
ers can give f uoxetine,
paroxetine, or sertraline to
their dogs at 0.5 to 2 mg/
kg once a day.
ES549101_vetm0115_021.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

LEASH TRAINING peer-reviewed
22 | January 2015 | Veterinary Medicine | dvm360.com
Since SSRIs can take up to
six weeks to become ef ective, I
often recommend that owners
give dogs a second medication
as needed to reduce arousal. For
those situations, clonidine (0.01
to 0.05 mg/kg b.i.d.) or trazo-
done (2 or 3 mg/kg q.i.d.) given
about an hour before walks can
be helpful. Start at a low dosage
and increase to ef ect.
Trazodone has an ef ect on
the serotonin system, so lower
dosages may be required for
ef ect and to avoid serotonin
syndrome, a serious and poten-
tially fatal condition that may
arise when antidepressants that
inhibit serotonin reuptake are
given at high doses or in combi-
nation with other drugs and
dietary supplements that may
increase serotonin. T e sero-
tonin syndrome results mainly
in neurologic, autonomic, and
gastrointestinal signs, including
restlessness, mental confusion,
hyperesthesia, shivering, shak-
ing, hyperthermia, tachycardia,
tachypnea, abdominal pain,
diarrhea, vomiting, hyper-
salivation, twitching, tremors,
seizures, coma, and death.
Pretreatment and follow-
Attempting to rush the dog through
the treatment stages may actually
delay progress and can be dangerous
if aggression is involved.
A healthy dose of reality Concerned about the behavior tips your clients might be
picking up from popular cable TV shows? Visit dvm360.com
/BehaviorReality to hear veterinary behaviorist Dr. John
Ciribassi’s advice on speaking with clients about these shows.
up diagnostic tests should be
considered depending on the
age and health of the dog, the
type of medication given, and
if multiple drugs are being
administered concurrently.
T e duration of training
required to resolve this type of
problem depends on the pet’s
temperament, the duration of
the problem, the severity of the
problem, and the expertise and
time dedicated by the owner.
Training may take several weeks
to many months. T e owner
needs to understand this and
that patience is very important.
Attempting to rush the dog
through the treatment stages
may actually delay progress and
can be dangerous if aggression
is involved. Encouragement and
timely follow-ups or progress
reports from the owner can be
essential for accomplishing a
satisfactory, safe outcome.
Suggested Reading
1. Bain M. Aggression toward unfamiliar
people and animals. In: Horwitz DF, Mills
DS, eds. BSAVA manual of canine and
feline behavioural medicine. 2nd ed.
Gloucester, UK: BSAVA, 2009;211-222.
2. Haug LI. Canine aggression toward unfa-
miliar people and dogs. Vet Clin North Am
Small Anim Pract 2008;38:1023-1041.
3. Landsberg GL, Hunthausen WL, Acker-
man L. Handbook of behavior problems of
the dog and cat. 3rd ed. Philadelphia, Pa:
Saunders, 2013;95-112, 134, 181-210,
297-326.
Wayne Hunthausen, DVM
Animal Behavior Consultations
4820 Rainbow Blvd.
Westwood, KS 66205
ES549107_vetm0115_022.pgs 12.24.2014 18:50 ADV blackyellowmagentacyan

090340591/0
NADA 141-273, Approved by FDA
Vetmedin®
(pimobendan) Chewable TabletsCardiac drug for oral use in dogs only
Caution: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Description: Vetmedin (pimobendan) is supplied as oblong half-scored chewable tablets containing 1.25, 2.5, 5 or 10 mg pimobendan per tablet. Pimobendan, a benzimidazole-pyridazinone derivative, is a non-sympathomimetic, non-glycoside inotropic drug with vasodilatative properties. Pimobendan exerts a stimulatory myocardial effect by a dual mechanism of action consisting of an increase in calcium sensitivity of cardiac myoÀlaments and inhibition of phosphodiesterase (Type III). Pimobendan exhibits vasodilating activity by inhibiting phosphodiesterase III activity. The chemical name of pimobendan is 4,5-dihydro-6-[2-(4-methoxyphenyl)-1H-benzimidazole-5-yl]-5-methyl-3(2H)-pyridazinone. The structural formula of pimobendan is:
Indications: Vetmedin (pimobendan) is indicated for the management of the signs of mild, moderate, or severe (modiÀed N<HA Class IIa, IIIb, or IVc) congestive heart failure in dogs due to atrioventricular valvular insufÀciency (AVVI) or dilated cardiomyopathy (DCM). Vetmedin is indicated for use with concurrent therapy for congestive heart failure (e.g., furosemide, etc.) as appropriate on a case-by-case basis.
a A dog with modiÀed New <ork Heart Association (N<HA) Class II heart failure has fatigue, shortness of breath, coughing, etc. apparent when ordinary exercise is exceeded.
b A dog with modiÀed N<HA Class III heart failure is comfortable at rest, but exercise capacity is minimal.
c A dog with modiÀed N<HA Class IV heart failure has no capacity for exercise and disabling clinical signs are present even at rest.
Dosage and Administration: Vetmedin should be administered orally at a total daily dose of 0.23 mg/lb (0.5 mg/kg) body weight, using a suitable combination of whole or half tablets. The total daily dose should be divided into 2 portions that are not necessarily equal, and the portions should be administered approximately 12 hours apart (i.e., morning and evening). The tablets are scored and the calculated dosage should be provided to the nearest half tablet increment.
Contraindications: Vetmedin should not be given in cases of hypertrophic cardiomyopathy, aortic stenosis, or any other clinical condition where an augmentation of cardiac output is inappropriate for functional or anatomical reasons.
Warnings: Only for use in dogs with clinical evidence of heart failure. At 3 and 5 times the recommended dosage, administered over a 6-month period of time, pimobendan caused an exaggerated hemodynamic response in the normal dog heart, which was associated with cardiac pathology (See Animal Safety).
Human Warnings: Not for use in humans. Keep this and all medications out of reach of children. Consult a physician in case of accidental ingestion by humans.
Precautions: The safety of Vetmedin has not been established in dogs with asymptomatic heart disease or in heart failure caused by etiologies other than AVVI or DCM. The safe use of Vetmedin has not been evaluated in dogs younger than 6 months of age, dogs with congenital heart defects, dogs with diabetes mellitus or other serious metabolic diseases, dogs used for breeding, or pregnant or lactating bitches.
Adverse Reactions: Clinical Àndings/adverse reactions were recorded in a 56-day Àeld study of dogs with congestive heart failure (CHF) due to AVVI (256 dogs) or DCM (99 dogs). Dogs were treated with either Vetmedin (175 dogs) or the active control enalapril maleate (180 dogs). Dogs in both treatment groups received additional background cardiac therapy (See Effectiveness for details and the difference in digoxin administration between treatment groups).
The Vetmedin group had the following prevalence (percent of dogs with at least one occurrence) of common adverse reactions/new clinical Àndings (not present in a dog prior to beginning study treatments): poor appetite (38%), lethargy (33%), diarrhea (30%), dyspnea (29%), azotemia
(14%), weakness and ataxia (13%), pleural effusion (10%), syncope (9%), cough (7%), sudden death (6%), ascites (6%), and heart murmur (3%). Prevalence was similar in the active control group. The prevalence of renal failure was higher in the active control group (4%) compared to the Vetmedin group (1%).
Adverse reactions/new clinical Àndings were seen in both treatment groups and were potentially related to CHF, the therapy of CHF, or both. The following adverse reactions/new clinical Àndings are listed according to body system and are not in order of prevalence: CHF death, sudden death, chordae tendineae rupture, left atrial tear, arrhythmias overall, tachycardia, syncope, weak pulses, irregular pulses, increased pulmonary edema, dyspnea, increased respiratory rate, coughing, gagging, pleural effusion, ascites, hepatic congestion, decreased appetite, vomiting, diarrhea, melena, weight loss, lethargy, depression, weakness, collapse, shaking, trembling, ataxia, seizures, restlessness, agitation, pruritus, increased water consumption, increased urination, urinary accidents, azotemia, dehydration, abnormal serum electrolyte, protein, and glucose values, mild increases in serum hepatic enzyme levels, and mildly decreased platelet counts.
See Table 1 for mortality due to CHF (including euthanasia, natural death, and sudden death) and for the development of new arrhythmias (not present in a dog prior to beginning study treatments) by treatment group and type of heart disease (AVVI or DCM) in the 56-day Àeld study.
Table 1: CHF Death and New Arrhythmias
in the 56-Day Field Study
Vetmedin®
Group
Active Control
Group
Dogs that
died
due to CHF
14.3% n = 175
14.4% n = 180
9 of 126 dogswith AVVI
16 of 130 dogs with AVVI
16 of 49 dogs with DCM
10 of 50 dogs with DCM
Dogs that
developed
new
arrhythmiasa
39.4% n = 175
45.0% n = 180
45 of 126 dogs with AVVI
59 of 130 dogswith AVVI
24 of 49 dogs with DCM
22 of 50 dogs with DCM
a New arrhythmias included supraventricular premature beats and tachycardia, atrial Àbrillation, atrioventricular block, sinus bradycardia, ventricular premature beats and tachycardia, and bundle branch blockFollowing the 56-day masked Àeld study, 137 dogs in the Vetmedin group were allowed to continue on Vetmedin in an open-label extended-use study without restrictions on concurrent therapy. The adverse reactions/new clinical Àndings in the extended-use study were consistent with those reported in the 56-day study, with the following exception: One dog in the extended-use study developed acute cholestatic liver failure after 140 days on Vetmedin and furosemide.
In foreign post-approval drug experience reporting, the following additional suspected adverse reactions were reported in dogs treated with a capsule formulation of pimobendan: hemorrhage, petechia, anemia, hyperactivity, excited behavior, erythema, rash, drooling, constipation, and diabetes mellitus.
To report suspected adverse reactions, to obtain a Material Safety Data Sheet, or for technical assistance call 1-866-638-2226.
Clinical Pharmacology: Pimobendan is oxidatively demethylated to a pharmacologically active metabolite which is then conjugated with sulfate or glucuronic acid and excreted mainly via feces. The mean extent of protein binding of pimobendan and the active metabolite in dog plasma is >90%. Following a single oral administration of 0.25 mg/kg Vetmedin tablets the maximal mean (± 1 SD) plasma concentrations (Cmax) of pimobendan and the active metabolite were 3.09 (0.76) ng/ml and 3.66 (1.21) ng/ml, respectively. Individual dog Cmax values for pimobendan and the active metabolite were observed 1 to 4 hours post-dose (mean: 2 and 3 hours, respectively). The total body clearance of pimobendan was approximately 90 mL/min/kg, and the terminal elimination half-lives of pimobendan and the active metabolite were approximately 0.5 hours and 2 hours, respectively. Plasma levels of pimobendan and active metabolite were below TuantiÀable levels by 4 and 8 hours after oral administration, respectively. The steady-state volume of distribution of pimobendan is 2.6 L/kg indicating that the drug is readily distributed into tissues. Food decreased the bioavailability of an aqueous solution of pimobendan, but the effect of food on the absorption of pimobendan from Vetmedin tablets is unknown.
In normal dogs instrumented with left ventricular (LV) pressure transducers, pimobendan increased LV dP/dtmax (a measure of contractility of the heart) in a dose dependent manner between 0.1 and 0.5 mg/kg orally. The effect was still present 8 hours after dosing. There was a
delay between peak blood levels of pimobendan and active metabolite and the maximum physiologic response (peak LV dP/dtmax). Blood levels of pimobendan and active metabolite began to drop before maximum contractility was seen. Repeated oral administration of pimobendan did not result in evidence of tachyphylaxis (decreased positive inotropic effect) or drug accumulation (increased positive inotropic effect). Laboratory studies indicate that the positive inotropic effect of pimobendan may be attenuated by the concurrent use of a β-adrenergic blocker or a calcium channel blocker.
Effectiveness: In a double-masked, multi-site, 56-day Àeld study, 355 dogs with modiÀed N<HA Class II, III, or IV CHF due to AVVI or DCM were randomly assigned to either the active control (enalapril maleate) or the Vetmedin (pimobendan) treatment group. Of the 355 dogs, 52% were male and 48% were female; 72% were diagnosed with AVVI and 28% were diagnosed with DCM; 34% had Class II, 47% had Class III, and 19% had Class IV CHF. Dogs ranged in age and weight from 1 to 17 years and 3.3 to 191 lb, respectively. The most common breeds were mixed breed, Doberman Pinscher, Cocker Spaniel, Miniature/Toy Poodle, Maltese, Chihuahua, Miniature Schnauzer, Dachshund, and Cavalier King Charles Spaniel. The 180 dogs (130 AVVI, 50 DCM) in the active control group received enalapril maleate (0.5 mg/kg once or twice daily), and all but 2 received furosemide. Per protocol, all dogs with DCM in the active control group received digoxin. The 175 dogs (126 AVVI, 49 DCM) in the Vetmedin group received pimobendan (0.5 mg/kg/day divided into 2 portions that were not necessarily equal, and the portions were administered approximately 12 hours apart), and all but 4 received furosemide. Digoxin was optional for treating supraventricular tachyarrhythmia in either treatment group, as was the addition of a β-adrenergic blocker if digoxin was ineffective in controlling heart rate. After initial treatment at the clinic on Day 1, dog owners were to administer the assigned product and concurrent medications for up to 56±4 days.
The determination of effectiveness (treatment success) for each case was based on improvement in at least 2 of the 3 following primary variables: modiÀed N<HA classiÀcation, pulmonary edema score by a masked veterinary radiologist, and the investigator’s overall clinical effectiveness score (based on physical examination, radiography, electrocardiography, and clinical pathology). Attitude, pleural effusion, coughing, activity level, furosemide dosage change, cardiac size, body weight, survival, and owner observations were secondary evaluations contributing information supportive to product effectiveness and safety. Based on protocol compliance and individual case integrity, 265 cases (134 Vetmedin, 131 active control) were evaluated for treatment success on Day 29. See Table 2 for effectiveness results.
Table 2: Effectiveness Results
for the 56-Day Field Study
Vetmedin®
Group
Active Control
Group
Treatment
Success on
Day 29
80.7%n=134
76.3%n=131
88 of 101 dogs with AVVI
77 of 100 dogs with AVVI
20 of 33 dogs with DCM
23 of 31 dogs with DCM
Treatment
Success on
Day 56
71.1%n=113
67.2%n=110
66 of 85 dogs with AVVI
56 of 85 dogs with AVVI
13 of 28 dogs with DCM
17 of 25 dogs with DCM
No increase
in furosemide
dose between
Day 1 and
Day 29
78.3%n=130
68.6%n=126
At the end of the 56-day study, dogs in the Vetmedin group were enrolled in an unmasked Àeld study to monitor safety under extended use, without restrictions on concurrent medications.
Vetmedin was used safely in dogs concurrently receiving furosemide, digoxin, enalapril, atenolol, spironolactone, nitroglycerin, hydralazine, diltiazem, antiparasitic products (including heartworm prevention), antibiotics (metronidazole, cephalexin, amoxicillin-clavulanate, ÁuoroTuinolones), topical ophthalmic and otic products, famotidine, theophylline, levothyroxine sodium, diphenhydramine, hydrocodone, metoclopramide, and butorphanol, and in dogs on sodium-restricted diets.
Palatability: In a laboratory study, the palatability of Vetmedin was evaluated in 20 adult female Beagle dogs offered doses twice daily for 14 days. Ninety percent (18 of 20 dogs) voluntarily consumed more than 70% of the 28 tablets offered. Including two dogs that consumed only 4 and 7% of the tablets offered, the average voluntary consumption was 84.2%.
Animal Safety: In a laboratory study, Vetmedin chewable tablets were administered to 6 healthy Beagles per treatment group at 0 (control), 1, 3, and 5 times the recommended dosage for 6 months. See Table 3 for cardiac pathology results. The cardiac pathology/histopathology noted in the 3X and 5X dose groups is typical of positive inotropic and vasodilator drug toxicity in normal dog hearts, and is associated with exaggerated hemodynamic responses to these drugs. None of the dogs developed signs of heart failure and there was no mortality.
Table 3: Incidence of Cardiac Pathology/
Histopathology in the Six-month Safety Study
Severe left ventricular hypertrophy with multifocal subendocardial ischemic lesions
One 3X and two 5X dogsa
Moderate to marked myxomatous thickening of the mitral valves
Three 5X dogs
Myxomatous thickening of the chordae tendineae
One 3X and two 5X dogs
Endocardial thickening of the left ventricular outÁow tract
One 1X, two 3X, and two 5X dogs
Left atrial endocardial thickening (jet lesions) in 2 of the dogs that developed murmurs of mitral valve insufÀciency
One 3X and one 5X dog
*ranulomatous inÁammatory le-sion in the right atrial myocardium
One 3X dog
a Most of the gross and histopathologic Àndings occurred in these three dogs
Murmurs of mitral valve insufÀciency were detected in one 3X (Day 65) and two 5X dogs (Days 135 and 163). These murmurs (grades II-III of VI) were not associated with clinical signs.
Indirect blood pressure was unaffected by Vetmedin at the label dose (1X). Mean diastolic blood pressure was decreased in the 3X group (74 mmHg) compared to the control group (82 mmHg). Mean systolic blood pressure was decreased in the 5X group (117 mmHg) compared to the control group (124 mmHg). None of the dogs had clinical signs of hypotension.
On 24-hour Holter monitoring, mean heart rate was increased in the 5X group (101 beats/min) compared to the control group (94 beats/min). Not counting escape beats, the 3X and 5X groups had slightly higher numbers of isolated ventricular ectopic complexes (VEs). The maximum number of non-escape VEs recorded either at baseline or in a control group dog was 4 VEs/24 hours. At either Week 4 or Week 20, three 3X group dogs had maximums of 33, 13, and 10 VEs/24 hours, and two 5X group dogs had maximums of 22 and 9 VEs/24 hours. One 1X group dog with no VEs at baseline had 6 VEs/24 hours at Week 4 and again at Week 20. Second-degree atrioventricular heart block was recorded in one 3X group dog at Weeks 4 and 20, and in one dog from each of the 1X and 5X groups at Week 20. None of the dogs had clinical signs associated with these electrocardiogram changes.
Treatment was associated with small differences in mean platelet counts (decreased in the 3X and 1X groups), potassium (increased in the 5X group), glucose (decreased in the 1X and 3X groups), and maximum blood glucose in glucose curves (increased in the 5X group). All individual values for these variables were within the normal range. Three 1X and one 5X group dogs had mild elevations of alkaline phosphatase (less than two times normal).Loose stools and vomiting were infrequent and self-limiting.
Storage Information: Store at 20° to 25°C (68° to 77°F), excursions permitted between 15° and 30°C (between 59° and 86°F).
How Supplied:
Vetmedin® (pimobendan) Chewable Tablets:Available as 1.25, 2.5, 5 and 10 mg oblong half-scored chewable tablets - 50 tablets per bottle.
NDC 0010-4480-01-1.25 mg - 50 tabletsNDC 0010-4481-01-2.5 mg - 50 tabletsNDC 0010-4482-01-5 mg - 50 tabletsNDC 0010-4479-01-10 mg - 50 tablets
Manufactured by: Boehringer Ingelheim Promeco S.A. de C.V. Mexico City, Mexico
Manufactured for: Boehringer Ingelheim Vetmedica, Inc. St. Joseph, MO 64506 U.S.A.
Vetmedin® is a registered trademark of Boehringer Ingelheim Vetmedica GmbH licensed to Boehringer Ingelheim Vetmedica, Inc.
Copyright © 2013 Boehringer Ingelheim Vetmedica, Inc. or an afÀliated company. All 5ights 5eserved.
448005-00 Revised 06/2013
ES549670_VETM0115_023_FP.pgs 12.29.2014 15:15 ADV black

Products & Services SHOWCASE | dvm360.com/products
Se
arc
h f
or
the
co
mp
an
y n
am
e y
ou
se
e i
n e
ac
h o
f th
e a
ds i
n t
his
se
cti
on
fo
r FR
EE
IN
FO
RM
AT
ION
!
24 | January 2015 | Veterinary Medicine | dvm360.com
D E N T A L P R O D U C T S
Searchlebalab
ES550082_vetm0115_024_CL.pgs 12.30.2014 19:49 ADV blackyellowmagentacyan

dvm360.com | MARKETPLACE
dvm360.com | Veterinary Medicine | January 2015 | 25
ANESTHESIA EQUIPMENT
MEDICAL EQUIPMENT
dvm360.com
Content Licensing for
Every Marketing Strategy
• Outdoor • Tradeshow/POP Displays• Direct Mail • Social Media• Print Advertising • Radio & Television
Marketing solutions ft for:
Logo Licensing | Reprints | Eprints | Plaques
Leverage branded content from Veterinary Medicine
to create a more powerful and sophisticated
statement about your product, service, or company
in your next marketing campaign. Contact Wright’s
Media to fnd out more about how we can
customize your acknowledgements and
recognitions to enhance your marketing strategies.
For more information, call Wright’s Media at
877.652.5295 or visit our website at
www.wrightsmedia.com
ES550083_vetm0115_025_CL.pgs 12.30.2014 19:49 ADV blackyellowmagentacyan

IDEA EXCHANGE tips from the trenches
26 | January 2015 | Veterinary Medicine | dvm360.com
Set the alarm for anesthesia changes
You can never be too safe or have too many oversight proto-
cols in place when administering anesthesia. T at is why we
placed a timer, which is automatically set to two minutes,
on the vaporizer. When someone increases or decreases the
vaporizer setting, he or she also touches the start button on the
timer, so the alarm will sound in two minutes. Even with a techni-
cian monitoring anesthesia, our practice has greatly benef ted
from the simple reminder of the two-minute alarm.
Julie McCreadie, LVT
Rochester, Michigan
Use laminated appointment sheets to be green and save green
We use laminated sheets of paper both for our notes and
the checkout sheet during appointments. T e techni-
cians can jot down each animal’s clinical signs, weight,
and any required vaccines with a water-based pen. After the visit
when the medical record has been updated on our computer, the
sheets can be erased and reused. We f gure we have saved thou-
sands of dollars on paper supplies with this method. Notes can be
color-coded by doctor, by visit, or by needed procedure.
Laura Wiglusz, LVT
Melissa Campbell, assistant
Beth McCrea, receptionist
Grand Island, New York
Read Miller onlineThe price for a competitive edgeDr. Robert Miller discusses
how some modern
horsemanship methods
have adversely affected
the industry. Find this and
previous columns by visiting
dvm360.com/Miller.
An update on the AAFP’s
Cat Friendly Practice initiative
dvm360.com/MedicineVideos
CAPC video of the month:
Checking for heartworm disease
dvm360.com/capc
Also online …
We need your ideas!
We’ll pay $50 for
regular submissions and
$75 for video
submissions that we
publish in print or online.
Email [email protected],
fax us at (913) 273-9876,
or write to Idea
Exchange
Editor at 8033
Flint, Lenexa, KS
66214.
ES549095_vetm0115_026.pgs 12.24.2014 18:49 ADV blackyellowmagentacyan

IMPORTANT SAFETY INFORMATION: VETMEDIN should not be given in case of hypertrophic cardiomyopathy, aortic stenosis, or any other clinical condition where an augmentation of cardiac output is inappropriate for functional or anatomical reasons. The safety of VETMEDIN has not been established in dogs with asymptomatic heart disease or in heart failure caused by etiologies other than atrioventricular valvular insufficiency or dilated cardiomyopathy. Use only in dogs with clinical evidence of heart failure. The most common side effects reported in field studies were poor appetite, lethargy, diarrhea, dyspnea, azotemia, weakness, and ataxia. If side effects should occur, pet owners should contact their veterinarian. Please refer to the package insert for complete product information or visit www.vetmedin.com.
ACT NOW. Use VETMEDIN at the first clinical signs of CHF in dogs of any size or shape.
Now VETMEDIN offers convenient dosing options for dogs of all sizes. DON’T WAIT.
Simon, 12O lbTwo 10 mg in morning andone 10 mg in evening*
Clyde, 65 lb10 mg in morning and half a 10 mg in evening*
Lucky, 22 lb2.5 mg (2x day) ORhalf a 5 mg (2x day)*
Busby, 12 lb1.25 mg (2x day) ORhalf a 2.5 mg (2x day)*
VETMEDIN is a well-established treatment for CHF caused by atrioventricular
valvular insufficiency and dilated cardiomyopathy.1,2 Now, no matter the size
of the dog, our new dosing options can help you give owners convenient,
cost-effective choices that help encourage compliance.
VETMEDIN is now available in four sizes:
1.25 mg, 2.5 mg, 5 mg, and 10 mg.
15186VETMEDIN is a registered trademark of Boehringer Ingelheim Vetmedica GmbH, licensed to Boehringer Ingelheim Vetmedica, Inc. © 2015 Boehringer Ingelheim Vetmedica, Inc. VET0214007
* All doses are provided as tablets.
References: 1. Häggström J, Boswood A, O’Grady M, et al. J Vet Intern Med. 2008;22(5):1124 –1135. 2. Lombard CW, Jöns O, Bussadori CM; for the VetSCOPE study. J Am Anim Hosp Assoc. 2006;42(4):249–261.
See brief summary on page 23
ES549701_VETM0115_CV3_FP.pgs 12.29.2014 15:37 ADV blackyellowmagentacyan

ES549671_VETM0115_CV4_FP.pgs 12.29.2014 15:15 ADV blackyellowmagentacyan