Heart Failure Waleed AlHabeeb, MD Consultant Heart Failure & Transplantation.

11/21/18
1
Heart failure Overiew
Michael Nassif, MD MScAssistant Professor of Medicine (Cardiology)
Saint Luke’s Mid America Heart InstituteUniversity of Missouri-Kansas City
§ Research grants astra zeneca and boerhinger ingelheim
§ Speaking honoraria Abbott
Relevant Financial Disclosure Statement

11/21/18
2
Prevalence of heart failure for adults ≥20 years by sex
and age (NHANES: 2011–2014)
Emelia J. Benjamin et al. Circulation. 2017;135:e146-e603 Copyright © American Heart Association, Inc. All rights reserved.
Projected US prevalence of HF 2012 to 2030
Circ Heart Fail Volume (3):606-619 May 21, 2013

11/21/18
3
HFrEF or HFpEF
HFpEF• Preserved systolic LV function• No LV dilation• Concentric LV remodeling• Diastolic LV dysfunction
HFrEF• Systolic LV dysfunction• LV dilation• Eccentric LV remodeling• Diastolic LV dysfunction
HFrEF, heart failure with reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; LV, left ventricularJessup M, Brozena S. N Engl J Med .2003;348:2007-2018.

11/21/18
4
Volume Overload
Pressure Overload
Loss of Myocardium
Impaired Contractility
LV DysfunctionEF < 40%
¯ CardiacOutput
Hypoperfusion
End Systolic Volume
End Diastolic Volume
Pulmonary Congestion
Left Ventricular Dysfunction
Hemodynamic Basis for HF Symptoms

11/21/18
5
Initially Adaptive, Deleterious if Sustained
ResponseShort-Term Effects Long-Term Effects
Salt and Water Retention Augments Preload Pulmonary Congestion, Anasarca
Vasoconstriction Maintains BP for perfusion of vital organs
Exacerbates pump dysfunction (excessive afterload), increases cardiac energy expenditure
Sympathetic Stimulation Increases HR and ejection Increases energy expenditure
Neurohormonal Responses to ImpairedCardiac Performance
Jaski, B, MD: Basics of Heart Failure: A Problem Solving Approach
Neurohormonal Model of Heart Failure
N Engl J Med. 1996;334:374-381. Prog Cardiovasc Dis. 1998;41:39-52.
Hypertension MI/CAD Myocarditis
Injury to the Heart
Angiotensin I Norepinephrine
Mortality and disease progression
Angiotensin IIVasoconstriction
Cardiac/vascular hypertrophyAldosterone secretion
Sodium retention
a1-ReceptorsArrhythmia, sudden death,
vascular resistance, adverse lipid effects,
impaired renal blood flow, myocyte cell death,
hypertrophy, Na+ retention
b2-Receptors
Arrhythmia, sudden death,potassium loss
b1-ReceptorsArrhythmia,
myocyte cell death, hypertrophy, LVD
ACEinhibition
Nonselective b-blockade with a1-blockade
Renin-angiotensinsystem (RAS) activation
Selective b-blockade
Sympathetic nervous system(SNS) activation
Nonselective b-blockade
Angiotensic Rec Blocker

11/21/18
6
• EF</=35%, NYHA II - IV• Enalapril (n=1285) v placebo (n=1284)
N Engl J Med. 1991 Aug 1;325(5):293-302.
Angiotensin Receptor Blockers (ARBs)
• Block AT1 receptors, which bind circulating angiotensin II
• RAAS Inhibition
• Ex: losartan, valsartan, candesartan, irbesartan
• Rec’d pts w systolic HF, intolerant to ACE-I (cough or angioedema)
• Same risk of renal impairment or hyperkalemia

11/21/18
7
• EF ≤ 40%, NYHA II-IV, ACE-I Intolerant• Candesartan (n=1013) v placebo (n=1015) for
CV death or HF admit
Lancet 2003; 362: 772–776
Lancet 2003; 362: 772–776

11/21/18
8
Neprilysin Inhibition
PARADIGM-HF
• Sacubitril/valsartan (n=4187) v enalapril (n=4212)
• CV death & HF admit• Mostly NYHA II (70%) & III (24%)• Mean SBP 122 mmHg, mean LVEF ~ 30%• Mean Age ~ 64 years• 93% on BB, 55% on MRAs• Minority (16%) with ICDs
N Engl J Med 2014; 371:993-1004

11/21/18
9
Beta-Blockers
• Cardioprotective effects due to blockade of excessive SNS stimulation
• Carvedilol, metoprolol succinate, bisoprolol
• In the short-term, beta blocker decreases myocardial contractility; increase in EF after 1-3 months of use
• Decr mortality (30-35%), hospitaliztions
• Incr LVEF (reverse remodelling), NYHA status
Sympathetic Activation
b1receptors
b2receptors
a1receptors
Cardiotoxicity
Metoprolol, Bisoprolol, Atenolol
Propranolol
Carvedilol, Bucindolol
Selectivity of b-Blocking Agents

11/21/18
10
• EF ≤ 35%, death or CV hospitalization• Carvedilol (n=696) v placebo (398)• NYHA II - IV
N Engl J Med 1996;334:1349-55
• EF < 35%, NYHA II-IV• All-cause mortality and admit• Metop TARTRATE (n=1518) v
carvedilol (n=1511)
Lancet. 2003 Jul 5;362(9377):7-13.

11/21/18
11
Aldosterone
Cardiac MyocyteHypertrophyNorepinephrine release
FibroblastHyperplasiaCollagen SynthesisFibrosis
Peripheral ArteryVasoconstriction
Endothelial DysfunctionHypertrophy
Decreased Compliance
KidneyPotassium Loss
Sodium Retention
Aldosterone Antagonists• Competitive inhib aldo rec Na-K exchange in distal
convuluted tubule• Spironolactone/Eplerenone
• Reduce heart failure-related morbidity and mortality
• NYHA Class II-IV HF
• Side effects include hyperkalemia and gynecomastia, K+/Cr levels should be closely monitored

11/21/18
12
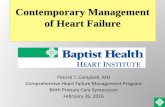
• Spironolactone (n=822) v placebo (n=841)• 1 EP – all-cause death
N Engl J Med 1999:341:709-17.
Days Since Baseline Visit Date0 100 200 300 400 500 600
85
90
95
100
Surv
ival
(%)
P=.01
Fixed-dose HYD/ISDN
Placebo
Hazard ratio=0.57
N Engl J Med. 2004;351:2052.
43% Decrease in Mortality
86% on ACE/ARB74% on B-blocker

11/21/18
13
• 1 EP – composite score• Isordil/hydral (n=518) v • placebo (n=532)• African-American patients, NYHA III, IV
N Engl J Med. 2004;351:2052.
SHIFT - Ivabridine

11/21/18
14
HFpEF: Prevalence Is IncreasingGWTG-HF: N=110,621 patients hospitalized with HFP<0.0001 for trend of increased HFpEF prevalence
EF, ejection fraction; HF, heart failure; HFpEF, heart failure with preserved ejection fractionOktay AA et al. Curr Heart Fail Rep. 2013;10:401-410/
Metabolic Traits Must Stronger Predicting HFpEF vs HFrEF
Savji N et al, JACC Heart Fail. 2018;6:701-709.

11/21/18
15
Lung Chest wall restriction, reduced vital capacity, impaired ventilation and diffusion Obstructive sleep apnea Pulmonary hypertension
Liver Non-alcoholic fatty liver disease Promotes generalized inflammatory state
Visceral adiposity Inflammatory cytokines Adverse neurohormones Increased BNP clearance
Kidney Direct toxic effects of perinephric fat Glomerulomegaly with glomerular dysfunction
Skeletal muscle Increased adipose infiltration Impaired perfusion Decreased diffusive O2 transport Mitochondrial dysfunction
Heart Direct and indirect myocardial lipotoxicity Worsened cardiac mechanics Diastolic dysfunction; increased filling pressures/ volume overload, increased afterload
HFpEF in 2018
HFpEF, heart failure with preserved ejection fractionKitzman D, Shah SJ. JACC. 2016;68:200–203; Borlaug B. Nat Rev Cardiol. 2014;11:507-515.
HFpEF
Obesity, insulin resistance
Pathogenesis of HFpEF
HFpEF, heart failure with preserved ejection fraction

11/21/18
16
HFpEF
Abnormal cardiac mechanics
Obesity, insulin resistance
HFpEF, heart failure with preserved ejection fraction
Pathogenesis of HFpEF
Obesity, Insulin Resistance, and Cardiac Mechanics in HyperGEN
P<0.0001 P<0.0001 P<0.0001
Abso
lute
glob
al lo
ngitu
dina
l stra
in (%
)
Body-massindex
Fasting glucose
HOMA-IR
N=2,150
HOMA-IR, homeostatic model assessment of insulin resistanceShah SJ, et al. AHA 2012 [abstract]

11/21/18
17
HFpEF: No Treatments?
HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fractionBorlaug BA, Redfield MM. Circulation 2011;123:2006-2013
Caloric Restriction and 7-kg Weight Loss Improve HFpEF
AT, aerobic exercise training; CR, caloric restrictionKitzman D, et al. JAMA. 2016;315:36-46.

11/21/18
18
Take home points
• Myocardial injury is only the first step in development LV dilitation and HF
• HFpEF appears to have a very different etiology than HFrEF
• Lots of evidence for HFpEF as a metabolic disease (many ongoing trials