Hearing Voices
39
Hearing Voices Tania Walsh, LCSW Sgt. Terry Tilley MWCPD
description
Hearing Voices. Tania Walsh, LCSW Sgt. Terry Tilley MWCPD. Learning Goals:. Understanding the day to day challenges Learning about the subjective experience of hearing voices Becoming more empathic Changing some of the things we do to address needs of people who hear voices - PowerPoint PPT Presentation
Transcript of Hearing Voices

Hearing Voices
Tania Walsh, LCSWSgt. Terry Tilley MWCPD

Learning Goals:
• Understanding the day to day challenges
• Learning about the subjective experience of hearing voices
• Becoming more empathic • Changing some of the things we do
to address needs of people who hear voices
• Identify the impact of severe emotional disturbance on young people

Overview
• The simulation experience – Word search– Reading comprehension– Crossword– Report interview
GOAL:
The key is to be moving through The key is to be moving through the real world to perform tasks the real world to perform tasks while experiencing the distressing while experiencing the distressing voicesvoices

Rules
• Do not talk to each other• Keep busy• Just be yourself• Do not leave the facility• Do not change the volume• Do not stop the tape until I tell
you the simulation is over.• Take care of yourself and if you
need to, turn the MP3 player off.


Push start now

Development of audiotape
• Patricia E. Deegan, PHD.– Director of Training for the
National Empowerment Center and an experienced voice hearer.
• Sampler of voice hearing• Professional recording studio
– Two females and one male who also hear voices

Experience and QuestionsDiscussion
• How did you feel emotionally?
• How did you feel physically?• Heartbeat?• How long was the simulation?

Now that you have had this experience, what will you do differently in your work with people who hear distressing voices?

Youth Experiencing Sever Emotional Disturbance

Learning Goals:
• Understanding the day to day challenges young people face with severe emotional disturbance
• Becoming more empathic • Changing the way we engage and
address the needs of young people experiencing signs and symptoms of mental illness
• Identify the impact of severe emotional disturbance on young people

Cultural Perspective• “Understanding the cultural dynamics of youth in behavioral
health crisis"
Brain Development
Dynamics
Brain Development
Dynamics
OJA/DHS Case
Worker
OJA/DHS Case
WorkerFamily Dynamics
Family Dynamics
Mental Health Substance
Abuse Dynamics
Mental Health Substance
Abuse Dynamics
History of Trauma
Dynamics
History of Trauma
Dynamics
Poverty DynamicsPoverty
Dynamics
Youth Youth

Brain Research FindingsThe brain continues to develop during adolescence.
Areas under construction:
• Prefrontal cortex – responsible for organizing, setting priorities, strategizing, controlling impulses
• Brain functions that help plan and adapt to the social environment
• Brain functions that help put situations into context; retrieve memories to connect with gut reactions

Their Brains
are being
Re-Wired
Their Brains
are being
Re-Wired
Because…Because…

The Developing Brain, Adolescence and Vulnerability to Drug Abuse

Risk Taking Behavior?
But there is concern – Adolescents overestimate their capacities, rely on their immature ability to judge, or give in to peer pressure
It is normal! - Exploration of new behaviors, decision making skills, identity development

Sensation-seeking Declines with Age

Risk Perception Declines and Then Increases After Mid-Adolescence

Self Harm vs. Harm to Others

Self Harmful Behavior
Examples of self harmful behavior
1. Banging head rapidly and repeated
2. Running into traffic (with the intent to harm self)
3. Suicide attempt4. Actions of self mutilation and
disfigurement

Self Harmful Behavior
Key things to remember
1. Acknowledge the youth’s distress.2. Active listening without interruption.3. Ask open-ended questions.4.Ask less direct question to start:
A. Have you been unhappy lately?
B. Have you been very unhappy lately?4. Ask more direct questions as
communication builds: A. Have you ever wanted to hurt yourself?

Intentional Harm to Others
Example of intentional harm to others
1.A detailed plan to intentionally harm family members, neighbors and/or animals with weapons or objects.
http://www.youtube.com/watch?v=H55Oz92Kh-A&feature=results_main&playnext=1&list=PL9F0592A142852ED2
http://www.youtube.com/watch?v=ME2wmFunCjU&feature=mfu_in_order&list=UL

Functional and Problem Solving Scales
• Things to consider when investigating a youth’s functional and/or problem solving ability.
• Problem Solving Questions 1. Is the young person arguing with others and threaten to
murder an individual 2. Is the young person getting into fights and threaten
individuals with a weapons3. Is the young person yelling, swearing, or screaming at
others erratically 4. Is the young person displaying fits of anger and aggressive
behavior that’s unprovoked and unpredictable5. Is the young person causing trouble for no reason6. Is the young person using drugs or alcohol7. Is the young person a repeat offender of breaking rules or
breaking the law (out past curfew, stealing)
• Functional Questions1. Is the young person getting along with friends2. Is the young person getting along with family3. Is the the young person able to care for themselves
(taking medicines or brushing teeth)4. Is the young person controlling emotions and staying
out of trouble5. Is the young person feeling good about oneself6. Is the young person thinking clearly and making good
decisions7. Is the young person able to concentrate, pay attention,
and completing tasks
Problem Problem Solving Solving
Behavioral Behavioral HealthHealth
FunctionaFunctional Abilityl Ability

Common Behavioral Health Challenges for Youth and Young People
OPPOSITIONAL DEFIANT OPPOSITIONAL DEFIANT DISORDERDISORDER
ADJUSTMENT DISORDERADJUSTMENT DISORDER
ATTENTION DEFICIT/ ATTENTION DEFICIT/ HYPERACTIVITY DISORDERHYPERACTIVITY DISORDER(ADHD)(ADHD)
MAJOR DEPRESSION DISORDERMAJOR DEPRESSION DISORDER
CONDUCT DISORDERCONDUCT DISORDER
ANXIETY DISORDERANXIETY DISORDER
OBSESSIVE COMPULSIVE OBSESSIVE COMPULSIVE DISORDERDISORDER
BIPOLAR DISORDERBIPOLAR DISORDER
BORDERLINE PERSONALITY BORDERLINE PERSONALITY DISORDER (BPD)DISORDER (BPD)
SCHIZOPHRENIASCHIZOPHRENIA

SAMHSA National Survey Any Mental Illness in the Past Year Among Adults (18+), By Age and Gender
Percent with Serious Mental Illness (SMI) in the Past Year
4.8
7.3
5.9
2.83.2
6.4
0
1
2
3
4
5
6
7
8
Age Group Gender
18 or Younger
18 to 25 26 to 49 50 or Older
Male Female

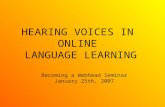
SAMHSA National Survey Any Mental Illness in the Past Year Among Adults (18+), By Age and Gender
Gender
18 or Younger
18 to 25 26 to 49 50 or Older
Male Female
Age Group
19.9
30.0
13.715.6
23.822.3
0
4
8
12
16
20
24
28
32
Percent with Any Mental Illness in the Past Year (2009)

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ISSUES ASSOCIATED ISSUES OR CHARTERISTICSOR CHARTERISTICS
OPPOSITIONAL DEFIANT DISORDER
(ODD)
Difficulty or conflict with other people;
Disobedient;
Lose temper;
Argue with adults;
Refuse to follow rules;
Annoy others;
Blame others for their mistakes,
Angry.
Consistently in conflict with others.
Need to be evaluated for possible learning disabilities.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/ SYMPTOMS/ BEHAVIORSBEHAVIORS
ASSOCIATED ISSUES ASSOCIATED ISSUES OR CHARTERISTICSOR CHARTERISTICS
ADJUSTMENT DISORDER
(AD)
Reduced productivity – decline in school performance.
Somatic complaints – headaches, stomachaches.
Social maladaptation-truancy, violations of the rights of others, destruction of property.
They occur equally in males and females.
Reaction to the stressor seems to be in excess of a normal reaction.
Adolescent symptoms of adjustment disorders are more behavioral such as acting out.
Associated with higher risk of attempted as well as completed suicide.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
ATTENTION DEFICIT/ HYPERACTIVITY DISORDER
(ADHD)
TWO CORE CATEGORIES:
1. Inattention (difficulties in sustaining attention, listening, following instructions, attending to details, forgetfulness, impaired organization, and
2. Hyperactivity/ impulsivity (squirming or fidgeting, running & climbing excessively, difficulty in playing quietly, talking excessively.
It’s a developmental failure in brain circuitry; typically diagnosed in school years.
Features of motor activity may diminish in late adolescence/early adulthood.
Consistently found more often in males.
Co-occurring associated with CD or Bipolar disorder predicts substance use in adolescence.
Focus on immediate over delayed gratification may increase substance use risk.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
CONDUCT
DISORDERS
(CD)
Aggression to people or animals;
Destruction of property;
Lying & theft;
Serious rule violations;
Bullying or intimidation;
Initiation of fights; Tend to be loners.
Childhood onset (before age 10) have more aggression, family history of anti-social behavior, early temperamental difficulties.
In males, more evidence of direct behaviors; in females, more relational or ‘indirect’ forms may be observed.
Strong association with development of substance use disorders in adolescence.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
ANXIETY DOSORDER Excessive fear;
Worry about things before they happen;
Uneasiness that
interferes with their daily
Lives;
Physical complaints;
Inability to relax;
Lack of concentration;
Frequent stomach aches, headaches, or other physical complaints;
Irritability.
Found to frequently run in families.
Can dramatically reduce productivity and significantly diminish an individual's quality of life.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
OBSESSIVE COMPULSIVE DISORDER
(OCD)
Recurrent, unwanted thoughts (obsessions)
or
rituals (compulsions), which adolescents feel they cannot control.
EX: hand washing, counting, checking, or cleaning.
OCD is often a chronic, relapsing illness. Begins in adolescence or early childhood. OCD is sometimes accompanied by depression, eating disorders, SA, ADHD, or other anxiety disorders. Adolescents may often feel shame and embarrassment about their OCD & fear it means they’re crazy. Hesitant to talk about their thoughts or behaviors.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
BIPOLAR DISORDER Cycling of manic and depressive episodes.
Manic symptoms include:
Irritability & agitation;
Sleep disturbance;
Distractibility / impaired concentration;
Grandiosity;
Reckless behavior;
Suicidal thoughts.
Presentation in youth may be characterized by ‘very rapid, brief, recurrent episodes lasting hours to a few days;
Early onset appears to have greater frequency in males;
Stronger association with co-occurring SA, anxiety and CD than with bipolar depression.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
BORDERLINE PERSONALITY DISORDER
(BPD)
Intense anger;
Persistent feelings of emptiness;
Fears of abandonment; Always seem to be in a crisis;
Disturbed thinking patterns;
Tend to be rational & calm one moment, & then explode into inappropriate anger;
Persistent unstable self-image;
Self-damaging Impulsivity (spending, sex, binge eating);
Repeated suicidal behavior;
Self-mutilation.
Unstable personal relationships.
BPD should be made with great care to this population due to personality of adolescents is still developing.
Occurs in all races.
Prevalent in females.
Typically presents by late adolescence.
A combination of disruptive behavioral problems, mood & anxiety symptoms, and cognitive symptoms.

MENTAL MENTAL HEALTH HEALTH DISORDERSDISORDERS
SYMPTOMS/SYMPTOMS/
BEHAVIORSBEHAVIORS
ASSOCIATED ASSOCIATED ISSUES OR ISSUES OR CHARTERISTICSCHARTERISTICS
SCHIZOPHRENIA Little range of emotions; Few facial expressions; Poor eye contact;
Delays in language,
Unusual motor behaviors;
Odd speech, both in content and tone;
May hear voices, ‘see’ things, problems with abstraction;
May demonstrate confusion, suspicion, paranoia;
Unusual fears.
Onset of full disorder before 6-7.
Difficulty in school functioning may be an early sign.
Substance use may facilitate otherwise impaired peer group interaction.
May have few friends or be withdrawn from peers.

Strategies to Communicate with Youth

Mental Health Response vs. Criminal Arrest
• If crime, but no mental illness = Arrest
• If mental illness, but no crime = Diversion
• If crime + mental illness, consider: 1. Seriousness of crime2. Lethality of risk to self or others3. Capability of jail/lockup to manage/treat person4. Mental health history5. Availability of services

Thank you for Participating
Questions?
• Contact Information
Tania Walsh, [email protected]
Sgt. Terry Tilley [email protected]
Marqus Butler [email protected]