HEALTHCARE PROVIDER EDUCATION ON TRAUMA INFORMED …€¦ · Treatment of mental health concerns...
55
HEALTHCARE PROVIDER EDUCATION ON TRAUMA INFORMED YOGA FOR VETERANS AND ACTIVE DUTY PERSONNEL DIAGNOSED WITH POST-TRAUMATIC STRESS DISORDER AN EVIDENCED-BASED QUALITY IMPROVEMENT PROJECT SUBMITTED TO THE GRADUATE DIVISION OF THE UNIVERSITY OF HAWAI’I AT MĀNOA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF NURSING PRACTICE IN NURSING May 2020 By Julie C. Vosters Evidenced-Based Quality Improvement Project Committee: Joseph Mobley, Chairperson Courtnee Nunokawa Jane Misola Keywords: PTSD, veterans, yoga, yoga therapy
Transcript of HEALTHCARE PROVIDER EDUCATION ON TRAUMA INFORMED …€¦ · Treatment of mental health concerns...

HEALTHCARE PROVIDER EDUCATION ON TRAUMA INFORMED YOGA FOR
VETERANS AND ACTIVE DUTY PERSONNEL DIAGNOSED WITH POST-TRAUMATIC
STRESS DISORDER
AN EVIDENCED-BASED QUALITY IMPROVEMENT PROJECT SUBMITTED TO THE
GRADUATE DIVISION OF THE UNIVERSITY OF HAWAI’I AT MĀNOA IN PARTIAL
FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
DOCTOR OF NURSING PRACTICE
IN
NURSING
May 2020
By
Julie C. Vosters
Evidenced-Based Quality Improvement Project Committee:
Joseph Mobley, Chairperson Courtnee Nunokawa
Jane Misola
Keywords: PTSD, veterans, yoga, yoga therapy

ii
Abstract
Background: Approximately 6% to 14% of veterans suffer from post-traumatic stress disorder
(PTSD) and many continue to experience symptoms with conventional treatment. To improve
patient care outcomes, the Veterans Health Administration set forth a complementary and
integrative health (CIH) directive. Yoga, one of the approved modalities, has been found to
support reduction of PTSD symptoms. As an emerging therapeutic modality, many healthcare
providers and patients may be unaware of yoga, yoga therapy, and trauma informed yoga to the
degree needed to ensure appropriate use for optimal patient care. Purpose: This evidenced
based quality improvement project assessed healthcare providers’ familiarity and knowledge
about the appropriate use of yoga as therapy for veterans and active duty personnel diagnosed
with PTSD before and after an educational session. This project intended to provide healthcare
providers with relevant information about the therapeutic use of yoga to optimize benefits and
reduce risks to patients. Methods: Five full-time PTSD residential recovery program healthcare
providers attended a 2 hour educational program about: the history and current trends of yoga
and yoga therapy, trauma informed yoga, and guidelines for healthcare providers. Participants
completed a pre-educational session questionnaire and a post-educational session questionnaire.
Results: Healthcare providers showed statistically significant improvements in familiarity and
knowledge of yoga and yoga therapy relative to the management of PTSD. Qualitative
responses indicated the education program was generally well received and every individual
indicated they would incorporate the knowledge into clinical practice. Discussion: Educational
programs with pertinent information about the differences between yoga, yoga therapy, and
trauma informed yoga may improve healthcare provider awareness and understanding of the

iii
appropriate use of these modalities. As therapeutic use of yoga is incorporated into clinical care,
improved healthcare provider awareness and understanding may reduce risks and adverse effects
as well as improve benefits, safety, and efficacy for veterans and active duty personnel with
PTSD.

iv
Table of Contents
Abstract ................................................................................................................................ ii
List of Tables ..................................................................................................................... vii
List of Figures ................................................................................................................... viii
Introduction ......................................................................................................................... 1
Description of the Problem .................................................................................................. 1
Literature Review and Synthesis ......................................................................................... 3
Literature Search Strategy and Critique .................................................................. 3
Yoga Intervention Distinctions ................................................................................ 3
Veterans and Active Duty Personnel ....................................................................... 4
PTSD and Related Symptom Outcomes .................................................................. 5
Yoga Therapy as Integrative Care ........................................................................... 6
Quality, Quantity, and Consistency of Evidence ..................................................... 7
Limitations ............................................................................................................... 7
Intervention Recommendations ........................................................................................... 8
Conceptual Framework ..................................................................................................... 10
PICO Question ................................................................................................................... 11
Methods and Procedures .................................................................................................... 11
Purpose Statement & Project Objectives ............................................................... 11
Sampling Plan ........................................................................................................ 12
Setting ........................................................................................................ 12
Sample ....................................................................................................... 12

v
Procedures ............................................................................................................. 13
Human Subjects Considerations ................................................................ 13
Measurements ............................................................................................ 13
Data Collection Procedures ....................................................................... 14
Data Analysis ............................................................................................. 15
Results ............................................................................................................................... 15
Discussion .......................................................................................................................... 16
Limitations ............................................................................................................. 18
Plan for Sustainability ........................................................................................... 19
Recommendations ................................................................................................. 20
Conclusion ......................................................................................................................... 20
Appendix A ....................................................................................................................... 22
Appendix B ........................................................................................................................ 23
Appendix C ........................................................................................................................ 27
Appendix D ....................................................................................................................... 28
Appendix E ........................................................................................................................ 31
Figure E1 ............................................................................................................... 31
Figure E2 ............................................................................................................... 33
Appendix F ........................................................................................................................ 36
Appendix G ....................................................................................................................... 37
Figure G1 ............................................................................................................... 37
Figure G2 ............................................................................................................... 38

vi
Appendix H ....................................................................................................................... 39
References ......................................................................................................................... 41

vii
List of Tables
Table 1. Mean Likert Scale Answers by Staff on Familiarity Questions ......................... 15
Table 2. Percentage of Correct Answers by Staff for Knowledge Questions .................. 16

viii
List of Figures
Figure E1. Pre-Education Questionnaire .......................................................................... 31
Figure E2. Post-Education Questionnaire ........................................................................ 33
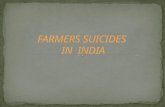
Figure G1. Mean Differences in Familiarity Answers Pre- and Post-Education ............. 37
Figure G2. Percentage of Correct Knowledge Answers Pre- and Post-Education ............ 38

1
Introduction
Many veterans and active duty personnel suffer from mental health concerns, including
post-traumatic stress disorder (PTSD) and suicidal ideation (DeBeer et al., 2014; Goldberg et al.,
2016; Richman, 2019; U.S. Department of Veterans Affairs, 2018; U.S. Department of Veterans
Affairs, Office of Mental Health and Suicide Prevention, 2018). The United States Department
of Veteran’s Affairs (VA) system emphasizes suicide prevention and treatment of mental health
concerns linked to suicide risk (U.S. Department of Veteran Affairs, Office of Mental Health and
Suicide Prevention, 2018). The Veterans Health Administration (VHA) also mandated provision
of Complementary and Integrative Health (CIH) to meet these stated needs and goals
(Department of Veterans Affairs, Veterans Health Administration, 2017). Implementation of
cost effective and sustainable CIH practices could provide accessible interventions with little to
no side effects and help manage mental health concerns and reduce suicides. One such
intervention under investigation for PTSD is yoga. Within the past decade, the field of yoga
therapy has expanded into conventional United States healthcare (Taylor & McCall, 2017).
Identification and awareness of yoga’s safety, efficacy, risks, and benefits specific to
management of PTSD for veterans and active duty personnel (hereinafter referred to as service
members) would provide evidence of viable and feasible supportive care. Hence, this project
intended to provide clinical care providers with education about the appropriate use of trauma
informed yoga as integrative care for veterans and active duty personnel with PTSD.
Description of the Problem
Treatment of mental health concerns and reduction of veteran suicides is an overarching
goal of the VA nationally and locally at the VA Pacific Islands Health Care System (VAPIHCS).

2
Estimates of veterans with PTSD range from 5.5% to 13.5% and span from Vietnam to
Operation Enduring Freedom and Operation Iraqi Freedom (Goldberg et al., 2016; U.S.
Department of Veterans Affairs, 2018). With PTSD and depression linked to higher rates of
suicide, especially if post-deployment social support is low (DeBeer et al., 2014), accessible and
effective treatment becomes imperative. With a quarter of Iraq and Afghanistan veterans seeking
treatment for PTSD, just over 20 service member suicides daily (Richman, 2019), and
approximately 22% of all U.S. suicides being veterans (U.S. Department of Veteran Affairs,
Office of Mental Health and Suicide Prevention, 2018), the VA prioritized mental health
treatment policies, programs, and research. Even with conventional treatment, many service
members continue to experience symptoms, which has prompted an emphasis to deliver care
with increased management and resolution of symptoms, including emerging treatments such as
complementary and integrative health (CIH).
In 2017, the Veterans Health Administration (VHA) set forth a directive to implement
CIH care with yoga listed as an approved and recommended modality and parameters delineated
to vet modalities and subsequent routes of integration to ensure safety and efficacy of patient
care (Department of Veterans Affairs, Veterans Health Administration, 2017). Within the
VAPIHCS, integration of yoga into clinical care is emerging and begets pertinent education
about yoga, yoga therapy, and trauma informed yoga as set forth by the VHA directive for
optimal PTSD program development and patient outcomes. With yoga therapy standards
emerging internationally and nationally, many clinical healthcare providers are likely unfamiliar
with yoga therapists’ scope of practice and how to best integrate yoga therapy into patient care.

3
The VHA directive to utilize CIH modalities for reduction of PTSD and suicide is a problem-
focused trigger. And research indicating trauma informed yoga supports reduction of PTSD
symptoms is a knowledge-focused trigger (Pilkington et al., 2016).
Literature Review and Synthesis
Literature Search Strategy and Critique
Literature was identified and critiqued to determine if sufficient evidence supported
implementation of a pilot evidence-based practice program. The following key words were
utilized in a PubMed search without any publication date parameters: veterans, active duty,
military, PTSD, and yoga. A broader search utilized only yoga and PTSD terms and yielded 69
articles: 19 repeat articles from the initial search, 27 new articles, and 23 not specifically
applicable articles.
Review of abstracts determined relevancy and review of 14 articles. Additional articles
were obtained through a snowball approach using articles’ reference lists. A total of 19 relevant
research articles (dated 2011 to 2019) were critiqued and categorized according to their level of
evidence (see Appendix A); three articles were systematic reviews. The grading tool used to
assess study level of evidence was an evidence hierarchy from Facchiano and Hoffman Snyder
(2012) (see Appendix A). Details of all articles were organized into a literature matrix for
efficient comparison and reference.
Yoga Intervention Distinctions
Yoga interventions varied in type, duration, frequency, and longevity, yet similar
outcomes of reduced PTSD symptoms prevailed. While most types of yoga included
combinations of movement, breath, and mindfulness, the amount of time focused on each

4
component varied; for instance, Sudarshan Kriya Yoga was primarily a breath-focused practice
(Seppala et al., 2014; Walker & Pacik, 2017). Interventions ranged in class duration from 1 to 4
hours, with a total of 5 to 20 sessions over the course of 5 days to 16 weeks. And some
interventions were defined with trauma informed or sensitive parameters (Cushing, Braun, &
Alden, 2018; Justice, & Brems, 2019; Cushing, Braun, Alden, & Katz, 2018; van der Kolk et al.,
2014) and/or service member orientations (Avery, et al., 2018; Cushing, Braun, & Alden, 2018;
Cushing, Braun, Alden, & Katz, 2018).
Consensus about the most effective protocols for PTSD, including yoga type, practice
duration, session frequency, and overall duration, had yet to be deciphered. And many studies
recommended forthcoming research build on preliminary indicators of yoga’s effectiveness in
relieving PTSD symptoms to further clarify these key components (Libby et al., 2012; Niles et
al., 2018; Staples et al., 2013; van der Kolk et al., 2014; Zalta et al., 2018).
Veterans and Active Duty Personnel
According to Pilkington et al. (2016), yoga therapy for PTSD research has focused on
three populations to include those who experienced either trauma related to natural disasters,
other traumas in general, or military trauma. Relative to military trauma, 52% of veterans
reported use of complementary and integrative health (CIH) modalities and 25% of veterans
reported use of yoga (Taylor, Hoggatt, & Kligler, 2019). Of studies reviewed that incorporated
service members, 100% included veterans and 23% mentioned inclusion of active duty
populations. Five of these 13 studies (38%) were published between 2012 and 2015 and eight
studies (62%) were published between 2017 and 2019. The more recent burst of research
appears to have coincided with the VHA’s 2017 CIH directive.

5
In the two most recent systematic reviews, yoga interventions were found to be
acceptable and feasible by veterans and non-veterans (Niles et al., 2018) with high rates of
satisfaction, generally high retention rates, and compliance rates higher than conventional
psychotherapy in studies with veterans (Cushing & Braun, 2018). Perceived benefits and
motivators, such as mental stillness, body awareness, and social connections, may have
supported these findings, yet perceived barriers, such as time, location, social unacceptability,
and physically unchallenging practices have been noted by participants as well (Justice & Brems,
2019; Cushing, Braun, & Alden, 2018).
PTSD and Related Symptom Outcomes
Overall, evidence suggests yoga may effectively reduce PTSD symptoms in service
members. Statistically significant decreases in total PTSD measurement scores were found in
most of the studies reviewed (Avery et al., 2018; Cushing, Braun, Alden, & Katz, 2018; Johnston
et al., 2015; Justice & Brems, 2019; Reinhardt et al., 2018; Staples et al., 2013; Steele et al.,
2018; van der Kolk et al., 2014; Walker & Pacik, 2017; Zalta et al., 2018). More specifically,
many studies also noted reductions in PTSD symptom cluster subscales of hyperarousal, re-
experiencing, numbness, and avoidance were experienced by service members (Cushing, Braun,
Alden, & Katz., 2018; Johnston et al., 2015; Reinhardt et al., 2018; Staples et al., 2013; Walker
& Pacik, 2017).
Yoga interventions were often adjuvant to other treatments, such as psychotherapy,
medications, and treatment for other comorbidities. Improvements in other symptoms such as
anxiety, depression, dissociation, adult attachment, anger, moral injury, fatigue, alcohol use,
substance use, sleep, mindfulness, and quality of life (Cushing & Braun, 2018; Cushing, Braun,

6
Alden, & Katz, 2018; Johnston et al., 2015; Justice & Brems, 2019; Staples et al., 2013; Steele et
al., 2018; Zalta et al., 2018) demonstrated how yoga interventions may have benefited additional
realms of well-being related to other comorbidities. Taken together, these results indicate yoga
therapy as integrative care may be effective in prevention and treatment of PTSD symptoms for
service members.
Yoga Therapy as Integrative Care
Traditionally, yoga facilitates liberation from suffering mentally, physically, and
emotionally. Though yoga has been utilized to promote multifaceted well-being for thousands of
years, a foundation of recent research created a platform to integrate yoga practices into
evidenced-based healthcare and supported creation of a medically oriented textbook (Khalsa et
al., 2016). Through practice of mindfulness, movement, and structured breathing appropriated to
specific health concerns, yoga therapy supports management, recovery, and optimization of well-
being parameters related to clinical health concerns. Growing evidence suggests yoga therapy is
a viable means to improve patient safety, care quality, and cost effectiveness for some clinical
populations (Kaoverii Weber & Sculthorp, 2016) and is represented by an International
Classification of Disease—10 procedure code (Taylor & McCall, 2017). And national and
international organizations have instituted rigorous parameters to uphold professional inclusion
of yoga therapy in clinical care and extend information to care providers through educational
standards, certification qualifications, and a peer-reviewed journal of published research.
A request for awareness, development, and standardization of yoga therapy for clinical
populations has been called for. Recommendations to educate healthcare providers and yoga
professionals about the other’s scope of practice (Cushing, Braun, & Alden, 2018; Forbes et al.,

7
2011; Libby et al., 2012) have precipitated and coincided with national and global initiatives.
Delineation of differences in yoga instructors’ and yoga therapists’ education and experience
standards (Justice et al., 2018) can help healthcare providers recognize responsible ways to
integrate care. While building bridges of collaboration between both types of care providers
could be sufficient, recommendations have been set forth for yoga therapists to receive specific
training in mental health and, if other healthcare providers seek to directly guide yoga therapy,
then to be formally trained in yoga therapy before directly guiding yoga therapy interventions
(Forbes et al., 2011).
Quality, Quantity, and Consistency of Evidence
Relative to research in yoga and yoga therapy being relatively new, the quantity of yoga-
based practices for service members with PTSD has risen in recent years. Though the quality of
research methodology has improved, there remains a need to further strengthen methodological
rigor. Overall, yoga practices have consistently indicated support of PTSD symptom reduction
in service members; yet consistency in the most effective dose, frequency, duration, and type of
yoga has yet to be determined. In time, and with improved quality and quantity of research
studies, further clarification and consistency of evidence is likely.
Limitations
Three systematic reviews stated common study limitations: small sample sizes, low or no
report of effect size, lack of randomized controlled studies, lack of methodological rigor,
participants and/or study personnel not blinded to intervention, treatment modalities varied, and
interventions concurrently adjuvant to other non-study treatments (Cushing & Braun, 2018; Niles
et al., 2018; Telles et al., 2012). Most studies echoed limitations of small sample sizes coupled

8
with additional limitations: recruitment barriers and biases (Avery, et al., 2018; Justice &
Brems, 2019; Reinhardt et al., 2018), psychiatric and medical comorbidities along with lack of
monitoring adherence to psychotherapy and medications not measured (Avery et al., 2018;
Johnston et al., 2015; Reddy et al., 2014), frequency and lack of long-term post-intervention
outcome measurement follow-up (Avery, et al., 2018; Cushing, Braun, Alden, & Katz, 2018;
Steele et al., 2018; Walker & Pacik, 2017; van der Kolk et al., 2014), and individual versus
group effects not measured (Justice & Brems, 2019; Justice et al., 2018; Walker & Pacik, 2017 ).
A few other limitations were noted, albeit less frequently: no baseline measurements (Justice &
Brems, 2019), yoga practice outside intervention not measured (Avery, et al., 2018), high drop
out rate (Reinhardt et al., 2018), lack of treatment fidelity measurement to ensure intervention
protocol followed (Zalta et al., 2018), and lack of clarity about how intervention components,
individually or collectively, contributed to outcomes (Steele et al., 2018; Zalta et al., 2018).
Consideration of other limitations could include elements such as variable intervention types,
lack of safety or adverse effect reporting, and education and experience of yoga instructor or
therapist.
Intervention Recommendations
Much of the literature indicates yoga practices support reduction of PTSD symptoms.
Yet similar to the five rights of medication administration (right patient, right drug, right dose,
right route, and right time), further clarification of specific elements (types, doses, frequencies,
and durations) of trauma informed yoga will help establish PTSD treatment guidelines. Evolving
research will help distinguish and confirm best practice standards to enhance prescriptive

9
protocols and better inform care providers who seek to integrate trauma informed yoga within
patient care for PTSD.
The integration of yoga therapy into clinical healthcare settings has been moving forward
at various degrees in different countries with approaches reflecting very conscious efforts to
ensure appropriate and consistent use of terminology, protocols, and accountability. For
instance, The Institut de YogaTherapie in France has undertaken a project introducing yoga
therapy into a few hospitals and clinics while legislature and regulatory measures are discussed
(Jacobi, 2019) and the National Health Service in the United Kingdom has set forth Social
Prescribing where general practitioners can refer patients to community support sources such as
yoga therapy services (Schnackenberg, 2019). Globally, yoga therapy educational and training
standards range internationally from bachelor, master, and doctoral degrees and licensure in
India to development of baseline standards in other countries (Kepner, 2019). In the United
States, the International Association of Yoga Therapists standardized yoga therapist certification
competencies, created educational program requirements, mandated continuing educational
requirements, and is creating a certification exam. The World Health Organization recognizes
the need for and is currently developing global yoga training standards to support safe, effective,
and quality use of yoga within traditional and complementary medicine (Kepner, 2019).
Increased recognition and use of yoga therapy within healthcare globally and nationally
precipitates educating healthcare providers to ensure appropriate use and integration of yoga
therapy for optimal patient care. Identification and definitions of scope of practice will help
distinguish professional roles, support collaborative relationships, ensure safety, efficacy, and
reduce risks or adverse effects, especially within mental health (Forbes, et al., 2011; Jacobi,

10
2019; Kaley-Isley, 2019; Libby et al., 2012; Schnackenber, 2019). Educational resources
designed for healthcare use, such as the PubMed indexed International Journal of Yoga Therapy,
have begun to distinguish and support the clinical relevancy and utility of yoga therapy for
patient care (U.S. National Library of Medicine, National Center for Biotechnology Information,
2019; Taylor, 2019). And clinical tools, such as the Pain Pocket Guide, Patient-Reported
Outcome Measurement Information System, and electronic medical record yoga therapy
templates, also indicate the increased use of yoga therapy within healthcare programs (Bethel,
2019; Bethel, Moonaz, & Sullivan, 2019; Taylor, 2019; Zador et al., 2019).
Yoga therapy, as a field, has been emerging as a viable and feasible form of integrative
care for a variety of clinical populations. However, clinical care providers may often be unaware
of differences between yoga and yoga therapy, differences between yoga instructors’ and yoga
therapists’ scope of practice, training, and education, as well as the benefits, risks, and
contraindications of yoga practices (Cushing, Braun, & Alden, 2018; Forbes et al., 2011; Justice
et al., 2018; Libby et al., 2012; Taylor & McCall, 2017). To appropriately recommend, refer,
and integrate yoga therapy into clinical care, increased health care provider familiarity and
knowledge of yoga therapy is needed. Hence, educating healthcare providers about yoga therapy
could promote reduced risk of adverse side effects or contraindicated practices and increase
benefits and health outcomes when yoga as therapy is referred, recommended, or integrated into
patient care.
Conceptual Framework
A conceptual framework can facilitate an evidence-based approach to address depression
in veterans. The Iowa Model Revised (Iowa Model Collaborative, 2017) has been used

11
worldwide and is the current model utilized by the VAPIHCS. A combination of elements
distinguishes The Iowa Model Revised from the others: main decision points highlighted with
feedback loops, incorporation of various types of evidence, important factors listed with freedom
to adapt flow to situation, pilot inclusion, sustainability guidance, and result dissemination.
Consideration of topic priority before moving forward engenders assurance of stakeholders.
Multiple junctures to reassemble, redesign, and reinfuse the project are outlined and emphasized.
PICO Question
With increased use of yoga therapy for clinical populations and evidence yoga therapy
helps alleviate PTSD symptoms, the foundation of the following clinical question is underscored.
For the interdisciplinary clinical care team within the Veterans Affairs Pacific Island Health Care
System (VAPIHCS) Post-Traumatic Stress Disorder (PTSD) Residential Recovery Program
(PRRP), does education on yoga and yoga therapy, compared to no prior education, increase
awareness and confidence levels of understanding yoga and yoga therapy as appropriate for
veterans and active duty personnel diagnosed with PTSD?
Methods and Procedures
Purpose Statement and Project Objectives
The purpose of this evidenced-based (EBP) quality improvement project was to increase
an interdisciplinary clinical care team’s awareness and confidence level of understanding yoga
and yoga therapy as appropriate for veterans and active duty personnel diagnosed with PTSD
who receive care at the VAPIHCS PRRP (see Appendix B and Appendix C). Project objective
included one effect-based initiative: by December 20, 2019, 75% of VAPIHCS PRRP licensed
independent providers (LIPs) and support staff who participated in the yoga and yoga therapy

12
educational session will indicate increased awareness (familiarity) and confidence (knowledge)
levels of understanding yoga and yoga therapy as appropriate for veterans and active duty
personnel diagnosed with PTSD.
Sampling Plan
Setting. This EBP project took place in the VAPIHCS PRRP located within Tripler
Army Medical Center in Honolulu, Hawai’i. The VAPIHCS serves an estimated 31,000 veterans
(U.S. Department of Veterans Affairs, 2019) and the VAPIHCS PRRP serves up to 72
individuals in 1 year. From 2006 to 2017, PRRP served a total of 802 male veterans and active
duty personnel representing the Army, Marines, Navy, Air Force and included: 481 Persian
Gulf/Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF) active duty
personnel, 228 Persian Gulf/OIF and OEF veterans, and 93 Vietnam veterans diagnosed with
PTSD from military trauma (Post-Traumatic Stress Disorder Residential Recovery Program,
2017).
Sample. The population was derived via convenience sampling of the VAPIHCS
PRRP’s interdisciplinary care providers and administrative staff composed of male and female
LIPs and support staff who are 18 years or older. The 19 PRRP staff (five LIPs and 14 support
staff) were full-time employees and included: one Psychiatrist/Senior Program Manager, one
Adult-Geriatric Nurse Practitioner/Nurse Manager, two Staff Psychologists, one Mental Health
Clinical Nurse Specialist, one Registered Nurse/Admissions Coordinator, five Licensed Practical
Nurses (one vacancy), two Nurse Aids, one Rehabilitation Technician; two Readjustment
Counselors, one Peer Support Specialist, one Medical Support Assistant, and one Program
Specialist. The sample size was determined by the number of full-time staff working in PRRP

13
with availability to attend the 2-hour educational session on December 20, 2019. The final
convenience sample consisted of three LIPs and two support staff (total five staff members).
Inclusion criteria was based on current VAPIHCS PRRP full-time employment status and
availability to be physically present for the educational session. Exclusion criteria included staff
who were not currently working within PRRP.
Procedures
Human Subjects Considerations. The author completed the Collaborative Institutional
Training Initiative (CITI) Training for research ethics and compliance, and Health Insurance
Portability and Accountability Act (HIPAA) Training on patient privacy protections. This DNP
project involved making judgments about a program to improve or further develop program
effectiveness and inform decisions about future programming within an organization (University
of Hawaii Human Studies program, personal communication, August 2, 2018). All these tasks
were related to quality improvement and did not produce generalizable knowledge. Thus, this
project did not require IRB application and review.
Measurements. Measurements included two questionnaires developed by the DNP
student. Both questionnaires were reviewed by University of Hawai’i and VAPIHCS content
experts for content, clarity, and format and vetted by non-PRRP VAPIHCS staff to ensure
readability and difficulty of question content. Both pre- and post-educational session
questionnaire questions reflected the educational session content (see Appendix D) and were
completed by PRRP LIPS and support staff, the pre-education questionnaire before the
educational session and the post-education questionnaire after the educational session. The pre-
education questionnaire (see Appendix E, Figure E1) was composed of 10 items: the first four

14
familiarity-based questions included Likert scales from 1 (almost none to none) to 5 (very much)
and the last six knowledge-based questions provided true/false/unsure answer options. The post-
education questionnaire (see Appendix E, Figure E2) contained the same 10 questions from the
pre-questionnaire along with five qualitative questions to assess the educational experience.
Both pre- and post-education questionnaires assessed awareness (familiarity) and confidence
(knowledge) levels of understanding: yoga, yoga therapy, trauma informed yoga; yoga
instructors’ and yoga therapists’ education, training, and scope of practice; safe and effective
recommendation and/or referral to yoga, yoga therapy, or trauma informed yoga for veterans and
active duty personnel recovering from PTSD. The information garnered from the completed
questionnaires helped determine the degree to which PRRP staff awareness and confidence
levels of understanding yoga and yoga therapy were affected by the educational sessions.
Data Collection Procedures. During an all staff meeting, PRRP LIPs and support staff
participated in the 2-hour educational session (see Appendix F for Educational Program
Schedule). At the start of the first educational session, the DNP student informed staff they
would remain anonymous, provided each staff member with a pre-education questionnaire, asked
the staff to complete the questionnaire, and collected the questionnaires from the staff prior to the
start of the educational session. PRRP staff took part in the educational sessions on site, on the
same day, and at the same time during an all staff meeting. At the end of the educational session,
the DNP student provided each staff member with a post-education questionnaire and asked the
staff to complete the questionnaire, and collected the questionnaires from the staff members prior
to the participants leaving the educational session. The DNP student grouped the questionnaires

15
into two categories: pre-education and post-education and manually entered questionnaire
results into a spreadsheet for data analysis.
Data Analysis. Pre- and post-education total scores for familiarity questions and total
score for knowledge questions were manually calculated. For familiarity questions, Likert scale
answers ranged 1 (none to almost none) to 5 (very much) and were added to obtain total
familiarity score. For knowledge questions, true, false, and unsure answers were scored 1, 0, and
0 respectively, then added to obtain the total knowledge score. Using these scores, a matched
t-test was conducted on the difference across participants.
For the first four familiarity questions (Likert scale), the related means were calculated
and compared for each question. For the last six knowledge (true, false, and unsure) questions,
the percentages of correct, incorrect, and unsure were calculated and compared to pre to post.
For the qualitative analysis (five open ended questions), responses were grouped according to
topic similarity and listed from most to least mentioned.
Results
Familiarity and knowledge scores increased from pre- to post-education. Results for
familiarity means per question are listed in Table 1. Familiarity total mean improved 25%.
Table 1
Mean Likert Scale Answers by Staff on Familiarity Questions
Question Pre Post 1 3 3.6 2 3.7 3.4 3 2 3.6 4 2 3.6 Total 10.7 14.2 Average 2.7 3.6

16
Results for knowledge percentages correct per question are listed in Table 2. Knowledge total
percentage correct improved 31%.
Table 2
Percentage of Correct Answers by Staff for Knowledge Questions
Question Pre Post 1 60 10 2 40 80 3 80 10 4 20 60 5 80 10 6 80 80 Total 360 520 Average 60 87
A matched t-test yielded statistically significant increases for familiarity and knowledge
questions from pre- to post-education. For familiarity questions, staff demonstrated a
statistically significant improvement from pre- to post-education (t(4) = 4.77, p < 0.05) (see
Figure G1), and for knowledge questions, staff demonstrated a statistically significant increase in
knowledge (t(4) = 4.0, p < 0.05) (see Figure G2).
Discussion
This project demonstrates that a 2-hour educational program on the therapeutic use of
yoga for PTSD can increase healthcare provider familiarity and knowledge. Qualitative
responses indicated the education program was generally well received and a longer time frame
was recommended to further discuss information. In particular, every individual indicated they
would incorporate the knowledge into clinical practice. Overall, the responses indicated a
behavior or practice change in staff is likely. This was demonstrated by a response to, What will

17
you most likely do with the information learned? A staff member’s answer, “Change how I
educate patients on recommending yoga.”
The largest increase in staffs’ familiarity occurred with two topics: trauma informed
yoga and the difference between yoga instructors’ and yoga therapists’ education, training, and
scope of practice. The importance of this improvement rests within the clinical nature for which
yoga as therapy would be recommended. Though healthcare providers may be aware of yoga,
they may not be fully aware of more specific yogic options, both in terms of type of yoga and
type of yoga professional, that may render different approaches and possibly differences in
outcomes for patients. These results show there is an opportunity to educate providers about
trauma informed yoga as a particular type of yoga specifically designed to support those affected
by trauma, and there is a difference in yoga professionals, especially related to the care of
clinical populations. Interestingly, there was a slight decrease in familiarity with yoga therapy.
Perhaps this decline was due to an initial belief of knowing a topic until one receives education
about the topic. In other words, one might believe they know a subject until after being
educated, when they realize there was more to the topic than initially perceived.
Knowledge gains were equally high for three topics: risks of general yoga classes for
clinical populations, vigorous physical yoga cautioned for PTSD population, and yoga
instructors’ versus yoga therapists’ scope of practice. The results support the need previously
identified in the literature, to educate healthcare providers about the effective use of and
differentiation between yoga and yoga therapy for clinical populations. The results also
demonstrate the ability of healthcare providers to learn and differentiate between yogic options
as a means to increase benefit and reduce risk to patients.

18
The results suggest the differentiations between yoga, yoga therapy, and trauma informed
yoga are important concepts for healthcare providers to become familiar with. Current gaps in
healthcare provider knowledge may lead to well-intended, yet suboptimal or unsafe use of yoga
for clinical populations. The results underscore the need for improved awareness and
demonstrate an effective approach in response to the recommendations set forth by yoga, yoga
therapy, and conventional healthcare professionals.
Limitations
This project has a few limitations to consider. One limitation of this convenience sample
was the relatively small number of participants (n = 5), which may not be representative of age,
education, experience, knowledge, or role in patient care compared to VAPIHCS staff at large.
The educational session date likely affected staff availability and though the educational session
was scheduled during an all staff meeting, the date was before the winter holidays on a day when
many staff members had scheduled vacation and were not present to participate. Out of 19
PRRP staff members, five (26%) were available and participated in the training. A second
limitation is the unknown minimal education session duration needed to be effective in
improving knowledge. A third limitation, long-term follow-up was not employed to determine
staff retention of new knowledge and renders uncertainty of last impact. A fourth limitation,
results may not be generalizable or representative of other healthcare providers outside
VAPIHCS PRRP.
Potential biases may also have affected the results. The level of PRRP staff’s general
knowledge of yoga prior to the educational session may have been higher than other staff since
PRRP has incorporated yoga-based practices within structured patient care and therapeutic

19
milieu for many years. Results may not be representative of general VAPIHCS staff working in
other patient clinics. If PRRP pre-questionnaire results were elevated due to prior awareness and
knowledge of yoga, the degree to which their familiarity and knowledge increased may have
been smaller. Also, DNP student is a certified yoga therapist and registered yoga teacher who
completed Trauma Sensitive Yoga training and who is a VAPIHCS employee who worked with
PRRP staff for 8 months prior to project implementation.
Plan for Sustainability
Within the VAPIHCS, sustainment pathways have been discussed with PRRP LIPs and
Whole Health Lead. Additional avenues for dissemination of educational presentations and
healthcare providers who may benefit from the information have been identified. Approval, as
appropriate, for project continuation and coordination with identified providers to schedule
educational presentations has been and will continue to be employed by the DNP student who is
also an employee of VAPIHCS. For example, Whole Health workgroup presentation on the
second component of the PRRP educational session, Trauma Informed Yoga, took place
subsequent to the PRRP educational session and reached healthcare providers who work with
veterans in various capacities outside of PRRP. Other considerations for sustainability include
educational sessions to healthcare providers who work with veterans with PTSD in VAPIHCS
inpatient and outpatient settings, such as Traumatic Stress Recovery Program (TSRP), primary
care, and pain management. Additionally, the information may be relevant to peer support
specialists and social workers who discuss supportive interventions and resources with veterans.
If the duration of the educational session is prohibitive, the 2-hour format utilized in this project
could be broken down into three shorter educational sessions of approximately 30 minutes each.

20
The shorter duration could fit into a lunch and learn series or departmental meetings more easily.
This is exemplified by the aforementioned individual educational session presented to the Whole
Health workgroup.
Recommendations
Though yoga as therapy may not yet be widely recognized, as the field of yoga therapy
and related research continues to grow and advances understanding of what is most effective,
innovative approaches to integrative healthcare will likely continue. Integrative programs, such
as the VA Whole Health program, might consider incorporating healthcare provider education of
yoga therapy and other CIH modalities to effectively improve access to care, quality of care, and
cost effectiveness of care for service members with PTSD. Innovative approaches to informing
healthcare providers may be found within other countries’ initiatives. Future educational
programs might determine what topics are most important and which delivery method is most
feasible for healthcare providers. As yoga teacher standards are enhanced, updates may be
relevant to educational content. Additionally, educators might consider supplying healthcare
providers with a reference sheet and/or an informational handout for patient education.
Conclusion
Though this evidence-based quality improvement project, the eight Essentials of Doctoral
Education for Advanced Nursing Practice (American Association of Colleges of Nursing, 2006)
were fulfilled and supported interprofessional collaboration for improved health outcomes of
service members affected by PTSD (see Appendix H). This educational intervention provided a
means to inform healthcare providers and increase understanding of the appropriate use of yoga
as therapy to improve outcomes for service members with PTSD. Since the distinction between

21
yoga, yoga therapy, and trauma informed yoga is a relatively recent development, it is important
for healthcare providers to understand the difference to better optimize benefits and reduce risks
for their patients.
The educational approach employed within the VAPIHCS could perhaps be a model for
other VAs, other healthcare organizations, yoga therapists, and governing organizations, such as
Yoga Alliance, International Association of Yoga Therapists, and the World Health
Organization, who seek to fortify collaborative efforts toward integrative health programs and
patient care. Perhaps other research and/or evidence-based quality improvement projects will
incorporate healthcare provider educational interventions. Educational endeavors would help
lead innovative and collaborative approaches to improving care quality.
When healthcare providers are informed about best practice guidelines based on current
evidence, especially in an emerging field such as yoga therapy, they are better equipped to
appropriately recommend, refer, and incorporate yoga as therapy into patient treatment plans. As
a result, patients will be guided toward safer and more effective use of yoga-based practices to
enhance their health and well-being—ultimately the goal of both patients and healthcare
providers alike.

22
Appendix A
Levels of Evidence Level Type Reviewed Level I Systematic reviews, meta-analysis, clinical practice guidelines 3 Level II Randomized control trials (RCTs) 4 Level III Controlled studies without randomization 2 Level IV Case controlled studies, cohort studies, cohort examples 4 Level V Case reports, case series, case controlled studies 5 Level VI Expert opinions 1 Adapted from Facchiano, L. & Hoffman Snyder, C. (2012). Evidence-based practice for the busy nurse practitioner: Part one: Relevance to clinical practice and clinical inquiry process. Journal of the American Academy of Nurse Practitioners, 24.

23
Appendix B
Logic Model
Situation: The purpose of this evidenced base (EBP) quality improvement project is to increase an interdisciplinary clinical care team’s awareness and confidence level of understanding yoga and yoga therapy as appropriate for veterans and active duty personnel diagnosed with PTSD who receive care at the Veterans Affairs Pacific Island Healthcare System (VAPIHCS) Post-Traumatic Stress Disorder Residential Rehabilitation Program (PRRP).
Inputs
Outputs
Outcomes -- Impact Activities Participation
Short Medium Long -1 VA EBP Project Policy NO.00-16-038 (VA facility) -1 nurse scientist (VA staff) -1 clinic manager (VA staff) -meeting room w/audio/visual capability of
-Garner VA EBP Committee approval of EBP project & related paperwork
-complete VA EBP Project Policy NO.00-16-038: overview, template, guidelines, & appraisal sheet
-submit VA EBP Project document(s) to
-VA nurse scientist, PRRP clinic manager, DNP student -DNP student
-increased awareness & understanding of historical & current trends of yoga & yoga therapy -increased awareness & understanding of yoga & yoga therapy educational standards & scope of practice
-by October 30, 2019, 75% of VAPICHS PRRP LIPs who participated in yoga and yoga therapy educational sessions will indicate increased awareness and confidence level of understanding yoga and yoga therapy as appropriate for veterans and active duty personnel
-increased use of trauma-informed yoga via implementation into PRRP treatment programming -decreased veteran & active duty personnel relying on medication to manage PTSD symptoms

24
presenting a PowerPoint (VA facility) -funding (no additional funds necessary)
nurse scientist for approval: VAPICHS Professional Practice QI/PI Project Template
-obtain VA EBP committee signatures
-Garner VA EES approval of EBP project & related paperwork
-complete VA EES documentation (detailed synopsis of project’s purpose, intervention, & objectives
-supervisor, EBP council member, chief of staff or associate director of patient care services/nurse executive -VA nurse educator, DNP student
-increased awareness & understanding of yoga therapy & trauma-informed yoga -increased awareness & understanding of yoga & yoga therapy resources & references -increased awareness & understanding of guidelines for LIPS to safely & effectively refer & recommend yoga &/or yoga therapy
diagnosed with PTSD. -by October 30, 2019, 75% of VAPICHS PRRP support staff who participated in yoga and yoga therapy educational sessions will indicate increased awareness and confidence level of understanding yoga and yoga therapy as appropriate for veterans and active duty personnel diagnosed with PTSD.
-decreased veteran & active duty personnel with PTSD -decreased veteran & active duty personnel suicidality -VA program model of trauma-informed yoga for other PTSD treatment programs -increased evidence demonstrating effectiveness of yoga therapy for PSTD with veterans & active duty personnel to advance the field within clinical settings -increased evidence of

25
-submit VA Employee Education System (EES) document(s) to nurse educator for approval by EES to ensure scientific rigor
-coordinate dates & times for educational sessions -reserve room for educational classes -construct educational session presentations -construct educational resource & guideline handout(s) -create questionnaires: Likert scales & open ended questions questionnaires for educational sessions evaluation
-VA nurse educator, DNP student -DNP student, clinic manager, program specialist, and room availability -DNP student -DNP student -DNP student, content expert
sustainable yoga therapy as integrative medicine practice within a clinical setting

26
-create a system for logging questionnaires
-DNP student
Assumptions
External Factors -growth of yoga therapy as an emerging field -growth of yoga therapy research for clinical populations -yoga therapy’s benefits for clinical populations, including those affected by PTSD and related comorbidities -growth of referrals to yoga therapy and clinical health care program inclusion of therapeutic yoga interventions -increased familiarity of yoga based practices by the general public and health care providers -national and international call for and current composition of guidelines for clinical care provider awareness and referral of yoga/yoga therapy for clinical populations -PRRP interdisciplinary staff interest in yoga/yoga therapy for treatment for PTSD -VAPIHCS incorporation of Whole Health model into patient and employee wellness -PRRP interest, familiarity, and current use of integrative care programming, including current Warriors at Ease yoga classes
-unforeseen and planned PRRP clinical staff changes during intervention period -PRRP clinical staff availability during intervention period

27
Appendix C
Gantt Chart & Timeline
2019 2020 Activity May June July Aug. Sept. Oct. Nov. Dec. Jan. Feb. Mar. Apr.
Committee Consultations
Proposal Defense
Project Proposal to VA Council
Pre-Assessment
Educational Session (Intervention)
Post-Assessment
Data Collection
Data Analysis
Final Paper to Committee
Final Presentation to Committee
VA Final Report to Council
UH Project Defense

28
Appendix D
Educational Session Outline
I. PRE-EDUCATION QUESTIONNAIRE II. YOGA & YOGA THERAPY: HISTORICAL & CURRENT TRENDS (Presentation)
A. Yoga 1. What is Yoga? 2. Classically Defined Yoga 3. Koshas: Sheaths/Layers of Well-Being 4. Eight Limbs: #1 & #2 5. Eight Limbs: #3 & #4 6. Eight Limbs: #5, 6, 7, & 8 7. Historical Timeline 8. Tree of Yoga 9. National Center for Health Statistics 10. 2016 Yoga in America Study 11. 2016 Yoga in America Study (continued) 12. 2016 Yoga in America Study (continued) 13. 2016 Yoga in America Study (continued) 14. 16 Yoga in America Study (continued)
B. Yoga Therapy 1. What is Yoga Therapy? 2. Yoga Therapy Sessions 3. Historical Timeline 4. Modern Timeline 5. Clinical Applications
C. Yoga or Yoga Therapy? D. Gratitude & Contemplations… E. References F. References (continued)
III. TRAUMA INFORMED YOGA (Presentation) A. Yoga Therapy Attributes B. Trauma Informed Yoga C. What is Trauma-Sensitive Yoga? D. Trauma-Sensitive Yoga Theoretical Basis E. History of Trauma-Sensitive Yoga F. Literature Search G. Literature Review & Synthesis

29
H. Yoga Interventions I. Yoga Interventions (continued) J. Veterans & Active Duty Personnel K. Veterans & Active Duty Personnel (continued) L. PTSD & Related Symptom Outcomes M. PTSD & Related Symptom Outcomes (continued) N. Gratitude & Contemplations… O. References P. References (continued) Q. References (continued)
IV. YOGA AS THERAPY: GUIDELINES FOR HEALTHCARE PROVIDERS (Presentation)
A. Practice Change B. Integration Initiatives C. Healthcare Education D. Yoga Instructor Education & Training
1. Yoga Alliance (YA) 2. Core Curriculum 3. Core Curriculum (continued)
E. Yoga Therapist Education & Training 1. International Association of Yoga Therapists (IAYT) 2. C-IAYT Grandparenting 3. Yoga Therapy: Certification 4. C-IAYT Scope of Practice 5. C-IAYT Scope of Practice (continued) 6. C-IAYT Scope of Practice (continued) 7. Scope of Practice: Differentiation
F. Scope of Practice: Differentiation G. Health Concerns & Research H. Yoga Therapy Sessions I. Safety J. Injuries & Adverse Effects K. Contraindications & Cautions L. Contraindications & Cautions in PTSD M. Prescriptions N. Referrals O. Recommendations P. Healthcare Concern in Veterans & Active Duty Personnel Q. Statistics

30
R. VA & VHA Initiatives S. VAPIHCS Whole Health T. Pathways Moving Forward U. Gratitude & Contemplations… V. References W. References (continued) X. References (continued)
V. RESOURCE LIST (Handout) VI. POST-EDUCATION QUESTIONNAIRE

31
Appendix E
Measurement Tools
Figure E1
Pre-Education Questionnaire
Directions: Circle the answer that most closely represents your current understanding.
# Content
1 none to almost none
2 minimal
3 moderate
4 much
5 very much
1 To what degree are you familiar with yoga? 1 2 3 4 5
2 To what degree are you familiar with yoga therapy? 1 2 3 4 5
3 To what degree are you familiar with trauma informed yoga? 1 2 3 4 5
4
To what degree are you familiar with the difference between yoga instructors’ and yoga therapists’ education, training, and scope of practice?
1 2 3 4 5
Directions: Circle the answer that most closely represents your current understanding.
# Content True False Unsure
5 General yoga classes do not pose risks to individuals with health concerns.
True False Unsure
6 Vigorous physical yoga practice is cautioned for individuals with post-traumatic stress disorder.
True False Unsure
7 Trauma informed yoga encourages participants to make their own choices during a guided practice.
True False Unsure
8 Yoga instructors and yoga therapists can assess an individual’s health and provide therapeutic plans.
True False Unsure
9 Some yogic breathing practices can trigger individuals who have experienced trauma.
True False Unsure

32
10 There is little difference between a referral to yoga versus a referral to yoga therapy.
True False Unsure
Mahalo for you feedback~

33
Figure E2
Post-Education Questionnaire
Directions: Circle the answer that most closely represents your current understanding.
# Content
1 none to almost none
2 minimal
3 moderate
4 much
5 very much
1 To what degree are you familiar with yoga? 1 2 3 4 5
2 To what degree are you familiar with yoga therapy? 1 2 3 4 5
3 To what degree are you familiar with trauma informed yoga? 1 2 3 4 5
4
To what degree are you familiar with the difference between yoga instructors’ and yoga therapists’ education, training, and scope of practice?
1 2 3 4 5
Directions: Circle the answer that most closely represents your current understanding.
# Content True False Unsure
5 General yoga classes do not pose risks to individuals with health concerns.
True False Unsure
6 Vigorous physical yoga practice is cautioned for individuals with post-traumatic stress disorder.
True False Unsure
7 Trauma informed yoga encourages participants to make their own choices during a guided practice.
True False Unsure
8 Yoga instructors and yoga therapists can assess an individual’s health and provide therapeutic plans.
True False Unsure
9 Some yogic breathing practices can trigger individuals who have experienced trauma.
True False Unsure
10 There is little difference between a referral to yoga versus a referral to yoga therapy.
True False Unsure

34
Please turn page over to complete questionnaire.
Directions: Provide a statement to reflect your opinion. If you prefer not to answer, write ‘NA.’
11
What did you find most helpful, informative, or supportive about this training?
12
What improvements would you recommend?
13
What will you most likely do with the information learned?
14
In terms of the presentation of the information, what would you like to share with the presenter?

35
15
Your feedback is welcomed, please indicate other questions or comments.
Mahalo for you feedback~

36
Appendix F
Educational Program Schedule
Time Duration (Total 1 hour 55
minutes)
Topics & Content Props & Slides
1000 - 1040 40 min. • Welcome • Pre-Education Questionnaire • Yoga & Yoga Therapy:
Historical & Current Trends
• Pre-Education Questionnaires
• 25 slides (27 w/refs)
1040 - 1110 30 min. • Trauma-informed yoga • 15 slides (18 w/refs)
1110 - 1155 45 min. • Yoga as Therapy: Guidelines for Healthcare Providers
• Resources for providers & patients
• Post-Education Questionnaire
• 19 slides (22 w/refs)
• Pre-Education Questionnaires
• Resource handouts • Resource examples

37
Appendix G
Figure G1
Mean Differences in Familiarity Answers Pre- and Post-Education
3
3.7
2 2
3.63.4
3.6 3.6
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4
MeanDifferenceValues
(LikertScale)
FamiliarityQuestions
Pre-Education Post-Education

38
Figure G2
Percentage of Correct Knowledge Answers Pre- and Post-Education
0%10%20%30%40%50%60%70%80%90%100%
1 2 3 4 5 6
PercentageofCorrectAnswers
KnowledgeQuestions
Pre-Education Post-Eudcation

39
Appendix H
DNP Essentials
DNP Essentials DNP Student Project
I. Scientific Underpinnings for Practice
• Evaluated and integrated evidence-based knowledge from science-based fields to advance nursing strategies to enhance healthcare delivery to veterans and active duty personnel affected by post-traumatic stress disorder (PTSD).
• Utilized scientific concepts and theories to develop and lead new practice approaches to improve healthcare provider knowledge and delivery of patient care.
II. Organizational and Systems Leadership for Quality Improvement and Systems Thinking
• Utilized leadership principles, program management strategies, and communication skills to assess, create, implement, and sustain practice change via a collaborative organizational model within the Veteran’s Affairs Pacific Island Health Care System (VAPIHCS).
• Demonstrated sincerity and sensitivity when communicating with healthcare providers from diverse career backgrounds as a means to improve organizational standards of practice and enhance healthcare outcomes of veterans and active duty personnel.
III. Clinical Scholarship and Analytical Methods for Evidence-Based Practice
• Investigate, evaluated, and translated new scientific evidence into practice to improve healthcare practice and outcomes.
• Applied findings to make connections across disciplines and develop and improve practice guidelines within an emerging field of integrative care.
• Served as a practice specialist/consultant to direct practice improvement.
IV. Information Systems/Technology and Patient Care Technology for the Improvement and Transformation of Health care
• Evaluated and selected healthcare consumer information resources for accuracy and appropriateness to improve clinical care quality, cost, and efficiency.
• Communicated critical elements of emerging healthcare information, web-based interventions, and support tools for clinical decision making.
• Designed a healthcare provider educational program to improve quality of care.
V. Health Care Policy for Advocacy in Health Care
• Engaged proactively in the process of policy and educated other healthcare providers to address healthcare disparities of veterans and active duty personnel.
• Designed, implemented, and advocated for institutional healthcare policy change to address healthcare disparities and to support improvements in practice safety, quality, and efficacy relative to the Veterans Health Administration’s Complementary and Integrative Health Directive 1137.

40
VI. Interprofessional Collaboration for Improving Patient and Population Health Outcomes
• Facilitated collaborative interprofessional team discussion and feedback on practice guidelines to improve patient care.
• Employed effective consultative and leadership skills during interprofessional communication with psychiatrists, nurse practitioners, psychologists, clinical nurse specialists, rehabilitation technicians, readjustment counselors, nurse aids, peer support specialists, and health promotion and disease specialists.
VII. Clinical Prevention and Population Health for Improving the Nation’s Health
• Analyzed and synthesized scientific data related to individual and population health to address biopsychosocial health parameters and outcomes of veterans and active duty personnel affected by PTSD.
• Evaluated clinical care prevention, management, and delivery strategies to reduce comorbidities and symptoms related to PTSD in veterans and active duty personnel.
VIII. Advanced Nursing Practice
• Evaluated the use of yoga, yoga therapy, and trauma informed yoga as a therapeutic intervention within an emerging field of integrative care.
• Exhibited expertise, advanced knowledge, and assessment and planning skills within an integrative approach to clinical patient care, program development, and policy establishment.

41
References
American Association of Colleges of Nursing. (2006). The essentials of doctoral education for
advanced nursing practice.
https://www.aacnnursing.org/Portals/42/Publications/DNPEssentials.pdf
Avery, T., Blasey, C., Rose, C., & Bayley, P. (2018). Psychological flexibility and set-shifting
among veterans participating in a yoga program: A pilot study. Military Medicine,
183(11/12). https://doi.org/10.1093/milmed/usy045
Bethel, K. (2019, Spring). Measurement in clinical practice: Part 2—The PROMIS tool. Yoga
Therapy Today, 30-31.
Bethel, K., Moonaz, S. & Sullivan, M. (2019, Winter). Measurement in clinical practice: An
introduction. Yoga Therapy Today, 38-56.
Cushing, R.E. & Braun, K.L. (2018). Mind-body therapy for military veterans with post-
traumatic stress disorder: A systematic review. The Journal of Alternative and
Complementary Medicine, 24, 106-114. doi: 10.1089/acm.2017.0176
Cushing, R.E., Braun, K.L., & Alden, S.W. (2018). A qualitative study exploring yoga in
veterans with PTSD symptoms. International Journal of Yoga Therapy, 28, 63-70. doi:
10.17761/2018-00020
Cushing, R.E., Braun, K.L., Alden, S.W., & Katz, A.R. (2018). Military-tailored yoga for
veterans with post-traumatic stress disorder. Military Medicine, 183, 5-6. doi:
10.1093/milmed/usx071
DeBeer, B.B., Kimbrel, N.A., Meyer, E.C., Gulliver, S.B., & Morissette, S.B. (2014).
Combined PTSD and depressive symptoms interact with post-deployment social support

42
to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom
Veterans. Psychiatry Research, 216(3), 357-362. doi:10.1016/j.psychres.2014.02.010
Department of Veterans Affairs, Veterans Health Administration. (2017, May 18). Provision of
Complementary and Integrative Health (CIH). (VHA Directive 1137).
https://www.va.gov/VHAPUBLICATIONS/ViewPublication.asp?pub_ID=5401
Facchiano, L. & Hoffman Snyder, C. (2012). Evidence-based practice for the busy nurse
practitioner: Part one: Relevance to clinical practice and clinical inquiry process.
Journal of the American Academy of Nurse Practitioners, 24, 579-586.
Forbes, B., Akhtar, F., & Douglass, L. (2011). Training issues in yoga therapy and mental
health treatment. International Journal of Yoga Therapy, 21(1), 7-11.
Goldberg, J., Magruder, K.M., Forsberg, C.W., Friedman, M.J., Litz, B.T., Vaccarino, V., …
Smith, N.L. (2016). Prevalence of post-traumatic stress disorder in aging Vietnam-era
veterans: Veterans Administration Cooperative Study 569: Course and consequences of
post-traumatic stress disorder in Vietnam-era veteran twins. American Journal of
Geriatric Psychiatry, 24(3), 181-191. doi:10.1016/j.jagp.2015.05.004
Iowa Model Collaborative. (2017). Iowa model of evidence-based practice: Revisions and
validation. Worldviews on Evidence-Based Nursing, 14(3), 175-182.
doi:10.1111/wvn.12223
Jacobi, M. (2019, Spring). Notes on yoga therapy in France. Yoga Therapy Today, 8.
Johnston, J.M., Minami, T., Greenwald, D., Li, C., Reinhardt, K., & Khalsa, S.B.S. (2015).
Yoga for military service personnel with PTSD: A single arm study. Psychological
Trauma: Theory, Research, Practice, and Policy, 7(6), 555-562.

43
Justice, L. & Brems, C. (2019). Bridging body and mind: Case series of a 10-week trauma-
informed yoga protocol for veterans. International Journal of Yoga Therapy, 29.
https://doi.org/10.17761/D-17-2019-00029
Justice, L., Brems, C., & Ehlers, K. (2018). Bridging body and mind: Considerations for
trauma-informed yoga. International Journal of Yoga Therapy, 28, 39-50. doi:
10.17761/2018-00017R2
Kaley-Isley, L. (2019, Spring). Yoga as therapy: The global spread of training standards for
yoga therapists. Yoga Therapy Today, 12-14.
Kaoverii Weber, K. & Sculthorp, B. (2016). Yoga therapy: Meeting the needs of the Triple
Aim. Yoga Therapy Today, 12(1), 22-23.
Kepner, J. (2019, Spring). “Benchmarking training standards for yoga in healthcare” with the
World Health Organization: Well-intentioned but so far not aligned with contemporary
yoga therapy standards. Yoga Therapy Today, 10.
Khalsa, S.B.S., Cohen, L., McCall, T. & Telles, S. (Eds.). (2016). The principles and practice
of yoga in health care. Handspring Publishing Limited.
Libby, D.J., Reddy, F., Pilver, C.E., & Desai, R.A. (2012). The use of yoga in specialized VA
PTSD treatment programs. International Journal of Yoga Therapy, 22, 79-88.
Niles, B.L., Mori, D.L., Polizzi, C., Pless Kaiser, A., Weinstein, E.S., Gershkovich, M., & Wang,
C. (2018). A systematic review of randomized trials of mind-body interventions for
PTSD. Journal of Clinical Psychology, 74, 1485-1508. doi: 10.1002/jclp.22634

44
Pilkington, K., Gerbarg, P.L., & Brown, R.P. (2016). Yoga therapy for anxiety. In Khalsa,
S.B.S., Cohen, L., McCall, T. & Telles, S. (Eds.), The principles and practice of yoga in
health care (pp. 95-116). Handspring Publishing Limited.
Post-Traumatic Stress Disorder Residential Recovery Program. (2017). PTSD Residential
Recovery Program. [Poster]. Veterans Affairs Pacific Island Health Care System.
Honolulu, HI.
Reddy, S., Dick, A.M., Gerber, M.R., & Mitchell, K. (2014). The effect of a yoga intervention
on alcohol and ddrug abuse risk in veteran and civilian women with posttraumatic stress
disorder. The Journal of Alternative and Complementary Medicine, 20(10), 750-756.
doi: 10.1089/acm.2014.0014
Reinhardt, K., Noggle Taylor, J.J., Johnston, J., Zameer, A., Cheema, S., & Khalsa, S.B.S.
(2018). Kripalu yoga for military veterans with PTSD: A randomized trial. Journal of
Clinical Psychology, 74, 93-108. doi: 10.1002/jclp.22483
Richman, M. (2019, January 16). Review study points to most effective mind-body therapies
for PTSD. VA Research Currents. https://www.research.va.gov/currents/0119-Mind-
body-therapies-for-PTSD.cfm
Schnackenberg, N. (2019, Spring). Yoga in Healthcare Alliance Conference 2019:
Collaboration, compassion and a call to action. Yoga Therapy Today, 14-16.
Seppala, E.M., Nitschke, J.B., Tudorascu, D.L., Hayews, A., Goldstein, M.R., Nguyen, D.T.H.,
Perlman, D., & Davidson, R.J. (2014). Breathing-based meditation decreases
posttraumatic stress disorder symptoms in U.S. military veterans: A randomized

45
controlled longitudinal study. Journal of Traumatic Stress, 27, 397-405. doi:
10.1002/jts.21936
Staples, J.K., Hamilton, M.F., & Uddo, M. (2013). A yoga program for the symptoms of post-
traumatic stress disorder in veterans. Military Medicine, 178(8), 854-860.
https://academic.oup.com/milmed/article-abstract/178/8/854/4259693
Steele, E., Wood, D.S., Usadi, E., & Applegarth, D.M. (2018). TRR's warrior camp: An
intensive treatment program for combat trauma in active military and veterans of all eras.
Military Medicine, 183(3/4), 403-407. https://academic.oup.com/milmed/article-
abstract/183/suppl_1/403/4959937
Taylor, M.J. (2019, Spring). News from the 2018 Integrative Pain Care Policy Congress. Yoga
Therapy Today, 16.
Taylor, M.J. & McCall, T. (2017). Implementation of yoga therapy into U.S. healthcare
systems. International Journal of Yoga Therapy, 27, 115-119.
Taylor, S.L., Hoggatt, K.J., & Kligler, B. (2019). Complementary and integrated health
approaches: What do veterans use and want. Journal of General Internal Medicine.
https://doi.org/10.1007/s11606-019-04862-6
Telles, S., Singh, N., & Balkrishna, A. (2012). Managing mental health disorders resulting from
trauma through yoga: A review. Depression Research and Treatment. doi:
1155/2012/401513
U.S. Department of Veterans Affairs. (2019). Locations: VA Pacific Islands Health Care
System. https://www.va.gov/directory/guide/facility.asp?id=151

46
U.S. Department of Veterans Affairs. (2018). Public Health: PTSD in Iraq and Afghanistan
veterans. https://www.publichealth.va.gov/epidemiology/studies/new-
generation/ptsd.asp
U.S. Department of Veteran Affairs, Office of Mental Health and Suicide Prevention. (2018).
National strategy for preventing veteran suicide: 2018—2028.
https://www.mentalhealth.va.gov/suicide_prevention/docs/Office-of-Mental-Health-and-
Suicide-Prevention-National-Strategy-for-Preventing-Veterans-Suicide.pdf
U.S. National Library of Medicine, National Center for Biotechnology Information. (2019).
NLM Catalog.
https://www.ncbi.nlm.nih.gov/nlmcatalog/?term=100965420[nlmid]&report=journal
van der Kolk, B.A., Stone, L., West, J., Rhodes, A., Emerson, D., Suvak, M., & Spinazzola, J.
(2014). Yoga as an adjunctive treatment for posttraumatic stress disorder: A randomized
controlled trial. Journal of Clinical Psychology, 75(6), e559-e565. doi:
10.4088/jcp.13m08561
Walker, J. & Pacik, D. (2017). Controlled rhythmic yogic breathing as complementary
treatment for post-traumatic stress disorder in military veterans: A case series. Medical
Acupuncture, 29(4), 232-238. doi: 10.1089/acu.2017.1215
Zador, V., Zador, L, & Anderson, M. (2019, Spring). Deign and implementation of electronic
medical record (EMR) templates for yoga therapy. Yoga Therapy Today, 32-35.
Zalta, A.K., Held, P., Smith, D.L., Klassen, B.J., Lofgreen, A.M., Normand, P.S., Brennan,
M.B., Rydberg, T.S., Boley, R.A., Pollack, M.H., & Karnik, N.S. (2018). Evaluating
patterns and predictors of symptom change during a three-week intensive outpatient

47
treatment for veterans with PTSD. Psychiatry, 18(242). http://doi.org/10.1186/s12888-
018-1816-6