Health Problem and Characteristics of the Application Renewing Health: MAST seminar Berlin 5 May...
31
Health Problem and Characteristics of the Application Renewing Health: MAST seminar Berlin 5 May 2010 Josep Roca Hospital Clinic.IDIBAPS.University of Barcelona [email protected]
-
Upload
augustus-jordan -
Category
Documents
-
view
213 -
download
0
Transcript of Health Problem and Characteristics of the Application Renewing Health: MAST seminar Berlin 5 May...

Health Problem and Characteristics of the Application
Renewing Health: MAST seminar Berlin 5 May 2010
Josep RocaHospital Clinic.IDIBAPS.University of Barcelona

TOPICS
CLINICAL & HEALTH ISSUES
TECHNICAL ISSUES
THE APPLICATION
Assessing Technology ?
Assessing Health Services supported by Technology ?

Health care & ICT
Health Service
Technological application

CLINICAL & HEALTH ISSUES
• Rationale• Hypothesis• Aims • Target patients• Study design • Type of intervention • Inclusion criteria• Exclusion criteria• Dimensions to be evaluated
• Clinical dimension•Technical dimension•Organisational dimension•Economic assessment

Well-being and rehabilitation programme
Rationale
• REHAB PROGRAMS INCLUDING MUSCLE TRAINING are highly recommended by all clinical guidelines for highly prevalent chronic diseases
• SUSTAINABILITY OF TRAINING EFFECTS IN A COST-EFFICIENT MANNER IS AN UNMET NEED PRECLUDING ADOPTION OF GUIDELINES

Well-being and rehabilitation programme
Hypothesis
• A standardised self-management program, including muscle training, can be carried out outside the hospital setting and is organisationally and economically sustainable in a long-term perspective.
• This program brings about positive outcomes in: improved quality of life, physical functioning, copying in everyday-life, reduced hospitalisation and readmissions for patients, reduce costs
• The rehab program makes it possible to sustain in the long-term the physiological benefits in muscular training.
• ICT solution favour better sustainability and patient / professional acceptability
• The characteristics of the program can be easily transferred to other chronic conditions that benefit from physical training programs

Well-being and rehabilitation programme
Aims
• Assess the deployment, efficiency and sustainability of a rehabilitation program supported by ICT in clinical stable patients with chronic disease
• Evaluate the effect of an integrated care pathway (combining structured patient education programme, physical exercise and planned follow-up) on quality of life, functional capacity, coping and need of health services and evaluation of the participants` experiences in the project
• Examine the effects (clinical, organisational, costs) when a standard supervised training period is followed by ICT supported monitoring over a period of 6 months and compare the results with a group followed by usual care (ICT monitoring is not used)

Well-being and rehabilitation programme
Target patients
Patients to be enrolled in each of the study locations are those with one or more of the following conditions: COPD, HF and coronary disease, older than the age of 45. Recruitment will take place at primary care and hospital outpatient clinics.
Study design
Randomised controlled trial on individual basis (individual RCT, ratio 1:1) with 2 arms:
• Control group with standard supervised training followed by usual care.
• Standard supervised training in combination with patient education and followed by ICT support / communication.

Well-being and rehabilitation programme
Type of intervention
A standardized self- management education and physical exercise programme will be conducted. The programme will be generic (not diagnosis specific) and group-based. Focus will be on coping in everyday-life with a chronic disease.
The main components will be:
Use of ICT to support the follow-up period after the completion of the standard training sessions to: promote the carrying out of the training plan and facilitate self-monitoring and reporting.
Empowering patients in the use of ICT solutions that support the follow-up period.

CLINICAL & HEALTH ISSUES
• Rationale• Hypothesis• Aims • Target patients• Study design • Type of intervention • Inclusion criteria• Exclusion criteria• Dimensions to be evaluated
• Clinical dimension•Technical dimension•Organisational dimension•Economic assessment

Variable Instrument Source / time
ER Visits (Hospital) DB registers TB, TM, TE
ER Visits (Primary care) DB registers TB, TM, TE
Hospital readmission rate (non-scheduled) DB registers TB, TM, TE
*LOS DB registers
HRQL (general) SF-36 TB, TM, TE
HRQL (specific COPD) SGRQ TB, TS, TM, TE
HRQL (specific HF) MacNew TB, TS, TM, TE
Frailty assessment CFS and NEadlS TB, TM, TE
**Health profile of the patient Clinical notes TB, TM, TE
6MWT (6 minute walking test) Test TB, TS, TM, TE
TB Basal assessment
TS Assessment after supervised training period
TM TS + 6 months
TE TS + 12 months
•* LOS: Length of stay•** Health profile of the patient. Under this heading, we make reference to a set of different data that is available from different databases and applications. This includes the following items: a) demographics, social economic status, urban/rural area; b) risk factors for exacerbation; c) other frailty factors, such as co-morbid conditions, anxiety-depression, educational level, economic status and caregiver support; and, d) treatment, including compliance, observed skills for administration of therapy and physical activity.
Well-being and rehabilitation programme
Clinical variables

TOPICS
CLINICAL & HEALTH ISSUES
TECHNICAL ISSUES
THE APPLICATION
Well-being and rehabilitation programme
Technological aspects
EHR functionality: Information sharing/exchange of information among professionals (including data on prescription).
CSCW functionality: Capabilities for coordinating professional work in the context of the specific process / programme of services. Also, general tools for professionals work (such as chat or messaging facilities).
CRM functionality: Facilitated access to the health-social services and professionals, typically through a single reference point (call-centre or alike).
E-education functionality: Education and training for professionals and patients.Mobile devices interface and tools: Utilities that enhance patient participation in the
process. This includes making easy the access to information that is relevant for the patient according to his/her condition but also resources that assist the patient to record data on the condition (questionnaires, sensors).
The results of the evaluation of the technology obtained in the different studies will be tracked to this functional level to provide a perspective that could be useful and applicable at different environments irrespective of the specific context.

PatientSupportcenter
pro
vid
ers
net
wo
rk
Overall Scenario
• Triage• Self-management• Remote monitoring
• Target patients • Management by programs• Well standardized interventions• Patient-centered care
Personal Health Folder

Technological platform: functionalities
Nurse’s portable unit
Call-Centre
Patient management unit
Home monitoring
Educational material
Home rehabilitation
Tele-working tools

Wireless mobile system

Patient’s application

The messages

Professional applications: Case Manager Dashboard
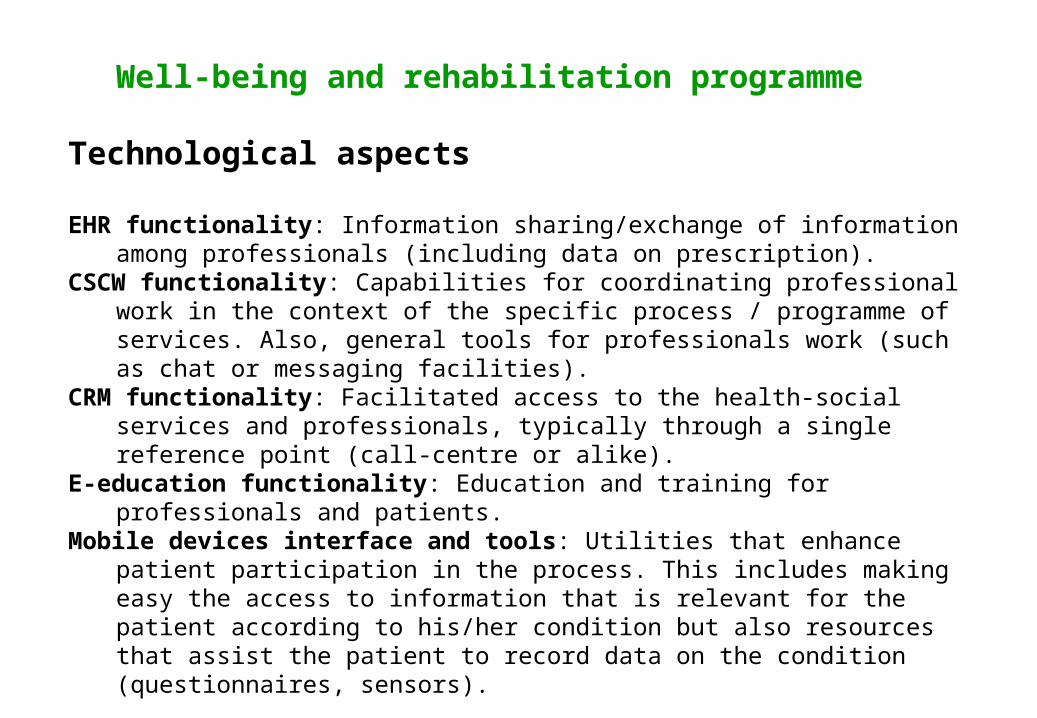
Professional’s application. Data

Usability
0
10
20
30
40
50
60
70
80

TOPICS
CLINICAL & HEALTH ISSUES
TECHNICAL ISSUES
THE APPLICATION

LOCAL INTEGRATION

Deployment at Barcelona Esquerra

INTEROPERABILITY AMONG PROVIDERS
• Level A - Barcelona – Esquerra• Level B - Spain and Europe
Patient summary record and electronic prescription
EAPsICSEAPsCAPSE
EAP Gesclínic
EAP Les Hortes
EAPsVallplasaHospital Clínic
Hospital SagratCor
Clínica Plató
CAP II Manso (ICS)
CAP II Numància(ICS)
EAPsICSEAPsCAPSE
EAP Gesclínic
EAP Les Hortes
EAPsVallplasaHospital Clínic
Hospital SagratCor
Clínica Plató
CAP II Manso (ICS)
CAP II Numància(ICS)
EAPsICSEAPsCAPSE
EAP Gesclínic
EAP Les Hortes
EAPsVallplasaHospital Clínic
Hospital SagratCor
Clínica Plató
CAP II Manso (ICS)
CAP II Numància(ICS) 3D3G
3A
2A
2C4A
2D
2E4B
5C4C
3E
5D
3C
3B
2B
5A5B
5E
3D3G
3A
2A
2C4A
2D
2E4B
5C4C
3E
5D
3C
3B
2B
5A5B
5E
• 540.000 habitantes
• 18 ABS y 2 CAPs II (5 empresas distintas)
• 4 Hospitales
• 1 Centro Sociosanitario principal y otros de menor dimensión
• 3 Proveedores de Salud Mental
• Servicio de Emergencias Médicas de Cataluña
BARCELONA ESQUERRA
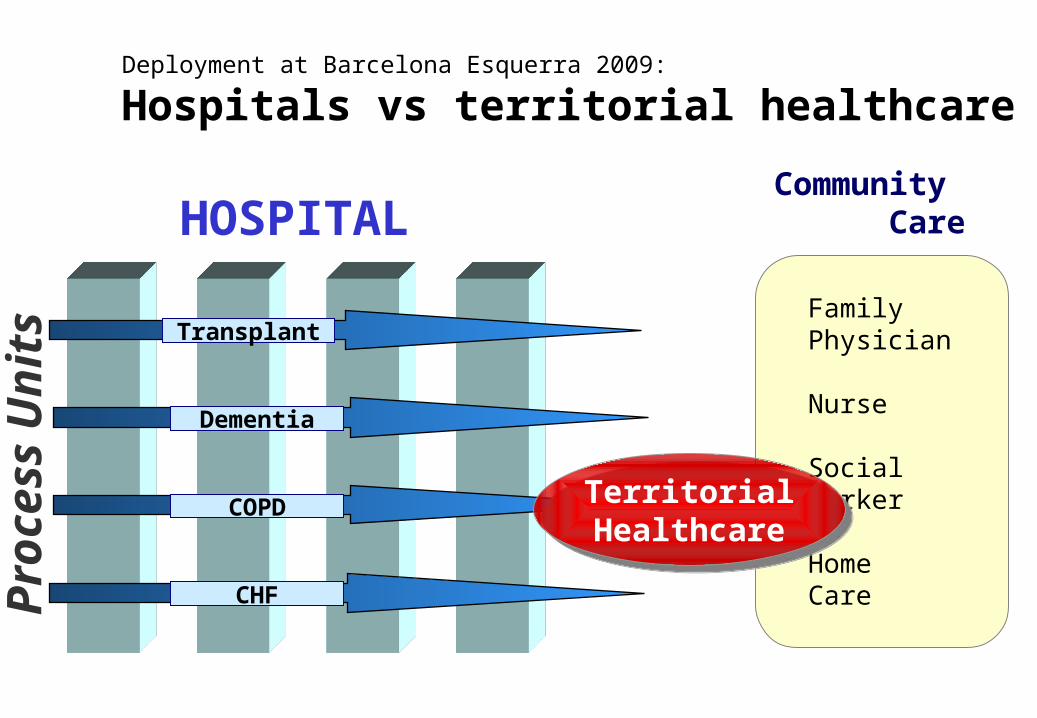
Pro
cess
Un
its
HOSPITALCommunity Care
FamilyPhysician
Nurse
Social Worker
HomeCare
Transplant
Dementia
COPD
CHF
TerritorialHealthcare
TerritorialHealthcare
Deployment at Barcelona Esquerra 2009:
Hospitals vs territorial healthcare

Permanent Comission
TechnicalManagement
Team
TechnicalManagement
Team
Process 1
Process 2
Process 3
Process 4
Em
erge
ncie
s
Soc
ial C
are
Hea
lth T
rans
port
H
ome
Car
e
P
edia
tric
car
e
Pha
rmac
y
RedesignImplementation
& follow-up
M
enta
l hea
lth
IT
Operational Committees
Deployment at Barcelona Esquerra 2009:
Territorial Health Care Comission Barcelona Esquerra
Deployment at Barcelona Esquerra 2009:
Territorial Health Care Comission Barcelona Esquerra
Sp
ecia
lize
d C
are
Institutions representative

Current Deployment at Barcelona Esquerra
Technological challenge
Organizational challenge

Initial questions
1. What kind of information should be included in a description of the health problem (patients) and characteristics of the telemedicine application in MAST (section 6.1. p. 14 in the Manual)?
2. How can interoperability of a telemedicine application be described?
3. Examples of descriptions of health problems and telemedicine applications in literature (p. 48 in the Manual)?
4. How can data be collected?
5. How can the information in this domain be used to select the relevant outcomes in the other domains?
6. What is your experience with description of these aspects of telemedicine in the literature?
7. Other hints to those planning to start an assessment of a telemedicine application?