Health Information Exchanges: Improving Patient Outcomes ...€¦ · Health Information Exchange:...
10
Health Information Exchanges: Improving Patient Outcomes through Technology & Healthcare A little more than a generation ago, healthcare was characterized as a physician working with a patient; occasionally involving a hospital. Less than 50 years ago, doctors still made house calls. Today, in the 21st century, caring for a single patient could involve a vast network that includes state and local governments, insurance companies, testing laboratories, any number of specialists, medical device manufacturers, pharmacies, immunization records, public health services, Medicare and Medicaid, and home health providers, to mention a few. Healthcare is now a patchwork of people, systems, and information. Consequential patient information, collected by any of the providers could be shared among the entire network when and where it was needed, if there was a system to facilitate that kind of communication. For several years, a vision for improving healthcare has been evolving that makes use of sophisticated technology to compile patient information from multiple sources and stored in a single database or distributed database system. This vision, known as a Health Information Exchange (HIE) is intended to facilitate the electronic movement of health-related information between different organizations according to national standards like HL7 1 . An HIE, not to be confused with the Health Insurance Exchange (HIX), is a tightly controlled exchange that oversees, governs and implements the communication of information among medical stakeholders for the purpose of improving patient care. 1 Health Level 7 (HL7) and its members provide a framework (and related standards) for the exchange, integration, sharing, and retrieval of electronic health information. The latest versions of the standards, which support clinical practice and the management, delivery, and evaluation of health services, are the most commonly used in the world.. ExEcutivE BriEf Health Information Exchanges (HIE) Secure-24 is a leading provider of managed hosting and cloud services, providing highly available IT environments and expert management for the healthcare, lifescience and financial industries. 26955 Northwestern Highway, Southfield, MI 48033 Phone: 800-332-0076 [email protected] www.secure-24.com
Transcript of Health Information Exchanges: Improving Patient Outcomes ...€¦ · Health Information Exchange:...

Health Information Exchanges: Improving Patient Outcomes through Technology & HealthcareA little more than a generation ago, healthcare was characterized as a physician
working with a patient; occasionally involving a hospital. Less than 50 years ago,
doctors still made house calls. Today, in the 21st century, caring for a single
patient could involve a vast network that includes state and local governments,
insurance companies, testing laboratories, any number of specialists, medical
device manufacturers, pharmacies, immunization records, public health services,
Medicare and Medicaid, and home health providers, to mention a few. Healthcare
is now a patchwork of people, systems, and information. Consequential patient
information, collected by any of the providers could be shared among the entire
network when and where it was needed, if there was a system to facilitate that kind
of communication.
For several years, a vision for improving healthcare has been evolving that makes
use of sophisticated technology to compile patient information from multiple
sources and stored in a single database or distributed database system. This
vision, known as a Health Information Exchange (HIE) is intended to facilitate the
electronic movement of health-related information between different organizations
according to national standards like HL71. An HIE, not to be confused with the
Health Insurance Exchange (HIX), is a tightly controlled exchange that oversees,
governs and implements the communication of information among medical
stakeholders for the purpose of improving patient care.
1 Health Level 7 (HL7) and its members provide a framework (and related standards) for the exchange,
integration, sharing, and retrieval of electronic health information. The latest versions of the standards,
which support clinical practice and the management, delivery, and evaluation of health services, are the
most commonly used in the world..
E x E c u t i v E B r i E f
Health Information Exchanges (HIE)
Secure-24 is a
leading provider of
managed hosting and
cloud services,
providing highly
available
IT environments and
expert management for
the healthcare,
lifescience and financial
industries.
26955 Northwestern Highway, Southfield, MI 48033
Phone: 800-332-0076 [email protected]
www.secure-24.com

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 2 o f 1 0
The concept of a Health Information Exchange is a good idea that will certainly
make it easier for medical professionals to deliver excellent healthcare. The
problem is how to make health exchange organizations work, from either a
technical or logistical point-of-reference.
Technically, the complex architecture required to integrate an enormous variety
of healthcare data from an enormous number of sources, scattered throughout
the country is daunting to say the very least.
Logistically, the processes required to enable ‘meaningful’ patient information
to be securely exchanged and understood2 among the various stakeholders is
yet another intimidating task.
Add to the technical and logistical issues, an even bigger question looms –
who will pay for it?
This whitepaper will focus on how the organizations that are building these
HIEs are dealing with these three challenges: technical requirements, logistical
hurdles, and long-term funding issues.
____________________
2 A complex health care system like the one in the United States needs an interoperable
data exchange environment to make health information understandable to all
stakeholders. Because there are so many different data formats in use, and one size
GRHV�QRW�¿W�DOO��WKH�2I¿FH�RI�6WDQGDUGV��,QWHURSHUDELOLW\�DW�WKH�8�6��'HSDUWPHQW�RI�Health and Human Services is striving to develop health IT data format standards and
facilitate the seamless exchange of patient data among all stakeholders.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 3 o f 1 0
Health Information Exchanges in practiceThe term Health Information Exchange is both a noun and a verb. It is
an entity, as previously mentioned, that controls the exchange of health
information. It is also a process or act of sharing information between
healthcare stakeholders. Health Information Exchanges have evolved over
the past 10 years as a grassroots type of association that is encouraged and
guided by federal and state governments3, but they are not controlled by the
government.
Government coordination for HIEs began in 2004 when President George
W. Bush issued an executive order for the development and nationwide
implementation of an interoperable health information infrastructure to improve
the quality of healthcare. The primary goal was that all Americans would have
DQ�(OHFWURQLF�+HDOWK�5HFRUG�RQ�¿OH�E\��������,Q�FRQWUDVW��+HDOWK�,QVXUDQFH�Exchanges (HIX) are mandated by law in the Affordable Care Act of 2010,
and they are controlled and governed by the individual States and the Federal
government.
Because the HIEs consist of independent stakeholders, they are structured
differently than a HIX. HIEs have more in common with private sector
organizations than do HIXs, even though the Federal and State governments
are often important stakeholders within any given Health Information
([FKDQJH���+,(V�DUH�JUDQWHG�FRQVLGHUDEOH�ÀH[LELOLW\�E\�WKH�)HGHUDO�government to interconnect with other health networks, if that connection will
help to create a more complete electronic health record. HIEs need to have
WKLV�ÀH[LELOLW\�VR�WKH\�FDQ�ORFDWH�DQG�FRQQHFW�ZLWK�WKH�ZLGH�YDULHW\�RI�KHDOWK�care organizations and services that possess different pieces of a single
patient’s health record.
________________
���7KH�2I¿FH�RI�WKH�1DWLRQDO�&RRUGLQDWRU�IRU�+HDOWK�,QIRUPDWLRQ�7HFKQRORJ\��21&��LV�D�VWDII�GLYLVLRQ�RI�WKH�2I¿FH�RI�WKH�6HFUHWDU\��ZLWKLQ�WKH�8�6��'HSDUWPHQW�RI�+HDOWK�DQG�+X-
man Services. It is primarily focused on coordination of nationwide efforts to implement
and use health information technology and the electronic exchange of health information.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 4 o f 1 0
There are four broad types of government coordinated Health Information
Exchange categories described by the following acronyms:
1. State Level Health Insurance Information Exchange (SLHIE)
The State Health Information Exchange Cooperative Agreement Program,
authorized by the Public Health and Safety Act is designed to promote
health information exchange across the entire spectrum of healthcare. The
purpose of the program is to expand the secure electronic exchange of health
information among organizations according to nationally recognized standards.
This program is a Federal and State collaboration with a long term goal
RI�HQVXULQJ�D�QDWLRQZLGH�+,(�ZLWK�LQWHURSHUDELOLW\���7R�WKLV�HQG��WKH�2I¿FH�RI�1DWLRQDO�&RRUGLQDWRU�IRU�+HDOWK�,QIRUPDWLRQ��21&��DZDUGV�FRRSHUDWLYH�DJUHHPHQWV�WR�6WDWHV�DQG�6WDWH�'HVLJQDWHG�(QWLWLHV���7KH�WRWDO�IXQGLQJ�available to all states and eligible US territories is $564,000,000.
������5HJLRQDO�+HDOWK�,QIRUPDWLRQ�([FKDQJH�2UJDQL]DWLRQ��5+,2�
$�5+,2�LV�D�PXOWL�VWDNHKROGHU�RUJDQL]DWLRQ�FUHDWHG�WR�SURPRWH�WKH�development and growth of health information exchanges. In addition to
LPSURYLQJ�SDWLHQW�FDUH��5+,2V�DUH�DOVR�LQWHQGHG�WR�VXSSRUW�WKH�VHFRQGDU\�XVH�of clinical data for research as well as care providers quality assessment and
LPSURYHPHQW���5+,2�VWDNHKROGHUV�LQFOXGH�VPDOOHU�FOLQLFV��KRVSLWDOV��PHGLFDO�societies and employers within a multi-state region.
3. National Health Information Network (NHIN)
The NHIN, now called the eHealth Exchange, is an initiative developed under
WKH�VSRQVRUVKLS�RI�WKH�21&���7KLV�QDWLRQDO�QHWZRUN�LV�EDVHG�RQ�XWLOL]LQJ�VHFXUH�email to exchange healthcare related information between patient stakeholders
on a nationwide level.
4. Health Information Exchange (HIE) Networks
The HIE Network is the blanket acronym that describes the program,
established during President George W. Bush’s administration, to improve
patient healthcare through better communication between stakeholders. It is
also often used to describe the local information exchanges that are usually
more homogeneous in terms of patients and stakeholders, focused on a
GH¿QHG�JHRJUDSK\��DQG�LV�VSHFL¿F�WR�D�W\SH�RI�VSRQVRU��H�J��WKH�&OHYHODQG�&OLQLF¶V�+,(�FDOOHG�'U&RQQHFW��

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 5 o f 1 0
Each of these categories emerged over the past few years as a result of
hundreds of medical professionals and other sponsors from many different
RUJDQL]DWLRQV�VHDUFKLQJ�IRU�WKH�PRVW�HI¿FLHQW�ZD\V�WR�RUJDQL]H�DQ�+,(�DQG�hold it together.
Any of the four categories of exchanges will also fall into two general types of
organizations:
1. Proprietary, which means the HIE was started and is controlled by a
single organization (e.g. an electronic health record vendor, or a large
hospital or hospital system, etc.)
2. Non-proprietary, which means the HIE was started and is controlled
E\�PXOWLSOH��FRRSHUDWLQJ�EXW�XQDI¿OLDWHG�RUJDQL]DWLRQV��H�J��D�QHWZRUN�consisting of public health agencies, state government, physician
SUDFWLFHV��KRVSLWDO�V\VWHPV��GLVHDVH�VSHFL¿F�UHVHDUFK�RUJDQL]DWLRQV��DQG�health insurance providers)
There are advantages and disadvantages to both types, but by far the most
‘workable’ type of exchange is proprietary. Since a proprietary exchange is
headed by a single organization or company, it has leadership, a funding
source, and provides clear value to the participants. However, a proprietary
exchange has limited access to patient data, because the stakeholders that
are entering information into the exchange database represent only a subset
of the entire scope of healthcare stakeholders that could exist for any given
SDWLHQW��2EYLRXVO\��WKLV�FRXOG�OHDYH�VLJQL¿FDQW�JDSV�LQ�WKH�SDWLHQW¶V�HOHFWURQLF�health record.
The non-proprietary exchanges have the potential to be all inclusive and
present a more complete picture of any given patient’s health status, because
they typically have access to the entire range of healthcare stakeholders.
However, it has one almost insurmountable obstacle, and that is a lack of
reliable long-term funding. Beyond the lack of money, the non-proprietary
exchanges also have serious technical challenges when it comes to
integrating so much data from so many sources. Although that challenge
can be overcome, it takes a lot more coordination and cooperation between
stakeholders to be successful.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 6 o f 1 0
State Level HIE projects2QH�RI�WKH�PRVW�VXFFHVVIXO�SURSULHWDU\�6WDWH�/HYHO�+,(V�LQ�WKH�FRXQWU\�LV�LQ�the state of Indiana. The Indiana Health Information Exchange focuses on
SURYLGLQJ�¿QDQFLDO�DQG�WHFKQLFDO�VXSSRUW�WR�H[LVWLQJ�ORFDO�H[FKDQJHV���7KH�PHPEHU�ORFDO�H[FKDQJHV�DUH�XVXDOO\�VPDOO�ZLWK�YHU\�VSHFL¿F�SDWLHQW�SURYLGHU�needs, but they have comprehensive coverage within a geographic area.
At a National eHealth Collaborative meeting earlier this year, John Kansky,
vice president of product management for the Indiana HIE (IHIE), said the
key to Indiana’s success is keeping their focus on providing clear value to
its customers. “We approach it and sustain it as a business,” he said. The
IHIE connects 90 Indiana hospitals, and 19,000 physicians use it. The IHIE’s
'2&6�'2&64 subscription service provides lab and radiology results to
physicians in a Web-based inbox. The IHIE also offers a service that enables
hospitals and physicians to electronically share clinical images.
The state of Maine started a non-proprietary state-level health information
exchange (SLHIE) in 2004 called the HealthInfoNet. This is a good example of
a state-wide HIE that stores all health information in a single shared database.
Where most states use a federated model of data storage in multiple locations,
which doesn’t always have standard formats; Maine preferred the centralized
PRGHO�WR�HOLPLQDWH�WKDW�LVVXH����³2QH�NH\�SUREOHP�ZLWK�WKH�IHGHUDWHG�PRGHO�LV�WKDW�WKH�GDWD�LV�QRW�VWDQGDUGL]HG�´�VDLG�'HY�&XOYHU��&(2�RI�+HDOWK,QIR1HW��“They can’t create a view of the patient. We put a lot of time into mapping all
that data to standards. In a federated model, that is impossible to do.”
It’s expected that all of Maine hospitals will be under contract to HealthInfoNet
by 2012 and will be connected by the end of 2013. The exchange is planning
for at least 80 percent of the state’s ambulatory and outpatient providers will be
connected by 2014.
________________
���,QGLDQD�KDV�OHYHUDJHG�WKHLU�FOLQLFDO�PHVVDJLQJ�VHUYLFH��'2&6�'2&6���WR�LPSURYH�the communication of information between public health agencies and health care pro-
YLGHUV��'2&6�'2&6��LV�D�V\VWHP�GHVLJQHG�DQG�GHYHORSHG�E\�WKH�5HJHQVWULHI�LQVWLWXWH�to deliver clinical results to physicians.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 7 o f 1 0
Tennessee is a good example of a regional HIE organization that did a mid-
course correction. In June of this year, the board of directors for the Health
Information Partnership for Tennessee (HIP TN) decided to shut down its
operations. The partnership was created in 2009 to help Tennessee create
D�QRQ�SURSULHWDU\�5+,2���+RZHYHU��WKH�WDVN�SURYHG�WR�EH�PRUH�FRPSOH[�DQG�ambitious for their level of readiness. The state wanted to offer enterprise
services, including links to an immunization registry, electronic lab results and
compiled patient medication histories, but was unable to create the exchange.
Instead of a Regional HIE organization, Tennessee decided to pursue a
simpler strategy that uses email messaging systems to communicate with
provides.
Tennessee may not be the only state that is changing direction. With limited
grant funding and many technical challenges, other states are also re-
evaluating their larger goals of creating a state-wide or regional infrastructure
that would allow searching of patient records from both hospitals and doctors’
RI¿FHV�
2QH�FKDOOHQJH�WKDW�SXEOLF�VHFWRU�+,(V�IDFH�LV�FRPSHWLWLRQ�IURP�SULYDWH�+,(V�being set up by independent health systems to support primary care and
home-healthcare organizations. In Connecticut, the three main hospital
systems are expanding rapidly by buying smaller hospitals and large physician
practices, and building out their own proprietary HIE architectures that are tied
WR�VSHFL¿F�HOHFWURQLF�KHDOWK�UHFRUG�YHQGRUV���
“That is changing the thought process about the role the state HIE will play,”
VDLG�'DYLG�*LOEHUWVRQ��&(2�RI�WKH�+HDOWK�,QIRUPDWLRQ�7HFKQRORJ\�([FKDQJH�RI�&RQQHFWLFXW���³:KDW�LV�WKH�LQFHQWLYH�IRU�SURYLGHUV�WR�FRQQHFW�WR�XV"�2QH�LV�WR�¿OO�WKH�JDSV�DQG�RIIHU�DFFHVV�WR�WKH�SURYLGHUV�WKDW�DUH�QRW�SDUW�RI�WKHVH�organizations,” he said. “Another is to provide access to public health and
Medicaid data. Those are the value propositions.”

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 8 o f 1 0
HIE Technical architectureAs mentioned in the beginning of this whitepaper, the vision of any Health
Information Exchange is to improve healthcare across the board by
exchanging patient information. To share meaningful patient information,
securely, on a scale this large is a complex and multifaceted undertaking.
The only way to do it is with sophisticated technology. And, the only way
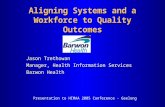
WHFKQRORJ\�ZLOO�ZRUN�LV�ZLWK�D�VFDODEOH�DQG�ÀH[LEOH�LQIUDVWUXFWXUH��+,(�WHFKQLFDO�architecture models fall into three categories: centralized, hybrid, and
federated. The diagram below explains the differences of each type:
HIEs: Technical Architecture Models (3 Types)
Centralized Hybrid Federated
1 Data is accumulated/managed in a single, centralized repository
1 State HIO has full control over data and ability to authenticate.
1 HIO is responsible for management of patient ID, data storage and privacy.
1 MPIs used to link patient records across databases.
1 Centralization or distribution is dependent &%�*'��!2��)�(,!)�$�%+*�
1 User interface connects patient information from various sources.
1 Multiple patient !��%+!2��+!&%�technologies: Master patient Indices and Record Locator Service (RLS)
1 Network permits users access only when needed.
1 Peet-to-peer architecture.
Each architecture has its pros and cons, but whichever architecture is chosen,
the hardware, software and IT personnel required to run the exchange plays a
key role in the success or failure of the HIE.
Additionally, because the infrastructure has to be secure, the HIE must to be
hosted in a HIPAA compliant environment that can meet the administrative,
technical and physical requirements of a structure containing patient
information. The trail of security extends to a variety of entities, such as the
hospitals, physicians, various vendors that are entrusted with data storage, the
systems performing the transmission of patient data over networks, as well as
those who are responsible for the physical security of the building housing the
HTXLSPHQW��2QH�ZHDN�OLQN�FDQ�OHDG�WR�D�GDWD�EUHDFK�DQG�H[SRVH�WKRXVDQGV�RI�medical records to the public or to someone trying to hack into the system.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 9 o f 1 0
There are two options for hosting an HIE architecture: 1) it can be hosted
internally by one of the participating stakeholders, or 2) it can be hosted by a
third-party managed hosting provider. Either way, the technical and logistical
requirements of the HIE architecture will be the same. The question to answer
is – which of the two options will do the best job and stay within the budget?
Before moving ahead with plans to create a Health Information Exchange, it is
advisable to decide how the hardware and software should be hosted and who
should provide the hosting environment. The option to utilize an independent
hosting provider and have the HIE hosted in a private cloud is one that should
EH�VHULRXVO\�HYDOXDWHG��7KLV�RSWLRQ�KDV�D�QXPEHU�RI�SRWHQWLDO�EHQH¿WV�OLNH�ORZHU�FRVW�������VXSSRUW��FRQWLQXDO�PRQLWRULQJ�RI�V\VWHP��DQG�D�VROLG�GLVDVWHU�recovery plan. A third party provider will also build the technical platform and
dedicate the necessary resources to the HIE to insure that it performs at an
optimal level. This approach is opposed to an in-house provider that might
VLPSO\�µ¿W¶�WKH�+,(�HQYLURQPHQW�LQWR�WKHLU�H[LVWLQJ�DUFKLWHFWXUH���$GGLWLRQDOO\��most enterprise level hosting providers are compliant with all federal and state
regulations governing data security.
A cloud environment, such as those hosted by Secure-24, can facilitate any
of the typical HIE architectures (centralized, hybrid, or federated). Whatever
architecture is best for the HIE business processes can be designed, tested,
and deployed in a virtual cloud production environment in less time than using
a typical in-house environment. From rapid deployment to tighter security, from
better integration with diverse systems to higher performance, a cloud solution
is an excellent option for hosting Health Information Exchanges.
The diagram on the next page illustrates that patient information is collected
from various sources (top) and can be compiled and integrated in a cloud
(center) so that it can be understood by various constituencies (bottom).
ConclusionThe challenges to provide meaningful and secure patient information
electronically online are substantial and the jury is out on how to build the best
W\SH�RI�+HDOWK�,QIRUPDWLRQ�([FKDQJH���2YHU�WKH�\HDUV�D�QXPEHU�RI�GHVLJQV�DQG�PRGHOV�KDYH�EHHQ�WULHG��EXW�D�GH¿QLWLYH�DSSURDFK�KDV�QRW�HPHUJHG���7KHUH�DUH�FOHDU�EHQH¿WV�WR�DOO�SDWLHQWV�LI�D�VXVWDLQDEOH�+,(�PRGHO�FDQ�EH�IRXQG��EXW�WKHUH�will be more trial and error as the various approaches are vetted.

E x E c u t i v E B r i E fHealth Information Exchange: Improving Patient Outcomes through Technology & Healthcare
p a g E 1 0 o f 1 0
To learn more about how
outsourcing your applications and
infrastructure to Secure-24 can
help your organization achieve its
business goals, contact us at:
Phone: 800.332.0076
Info: [email protected]
Sales: [email protected]
www.secure-24.com
Patients
Hospitals
Physicians
Physicians
Hospitals
Patients
Patients
Patients
Insurance Companies Patients
Hospitals
Insurance Companies
Patients
Hospitals
PhysiciansPhysicians
Hospitals
PatientsPatients Patients
Insurance Companies
Patients
Hospitals
Insurance Companies
Physicians Physicians Physicians
Insurance Companies
Hospitals Hospitals
HIE Hosting Cloud
HIE Core Services — Conceptual Model
As can been seen throughout this whitepaper, there are serious technical,
logistical and funding challenges facing all Health Information Exchanges.
However, each exchange can deal with their unique challenges in creative
ZD\V��ZKLFK�XOWLPDWHO\�ZLOO�KHOS�DOO�H[FKDQJHV�¿QG�WKH�EHVW�PRGHO�WR�XVH���7KH�)HGHUDO�JRYHUQPHQW�LV�SURYLGLQJ�VRPH�JXLGDQFH�DQG�¿QDQFLDO�DVVLVWDQFH�LQ�the early stages of designing and building a HIE, but the success or failure of
an exchange will come down to how much value the HIE provides and how
broadly supported it is by the stakeholders.
Inp
ut b
y V
ario
us S
ou
rce
s2XWSXW�IRU�YDULRXV�FRQVWLWXHQFLHV�