HEALTH INA COLD CLIMATEprojectes.camfic.cat/Docs/10_11/Health_in_a_Cold_Climate... · 2017. 2....
16
BRIEFING PAPER JUNE 2009 The NHS in England is faced with the prospect of finding savings of around £15–20bn over the period 2011–2014 the Department of Health and NHS organisations need to adopt an intelligent approach to finding these savings that avoids both ‘salami-slicing’ and ‘slash and burn’ a comprehensive approach to improving efficiency is needed, encompassing actions at the system, organisation, team and practitioner levels at each level, the focus should be on using information and incentives and building capacity to deliver the necessary savings and improvements the principal aim needs to be to reduce variations in clinical practice by engaging doctors and other front-line staff in performance improvement service line reporting shows promise and is contingent on strengthening both operational management and clinical engagement the NHS Institute’s programmes also have an important contribution to make through the use of benchmarking and service improvement methods with over £5bn of potential savings available the Department of Health should review current policies with the aim of deciding what changes are needed as the NHS moves from expansion to contraction experience from other sectors suggests that successful change requires action on several fronts simultaneously and work across a series of ‘dualities’ these dualities include: providing central leadership and supporting NHS organisations to build capacity; using competition and promoting cooperation; supporting commissioners and drawing on the expertise of foundation trusts; valuing clinical engagement and strengthening the role of general managers; emphasising the standardisation of care and ensuring that services are customised around the needs of individuals integrated systems have a potentially important role to play in future, in aligning incentives to facilitate the emergence of new models of care NHS foundation trusts could play an important part in the development of integrated systems, but only if there are changes to the regulatory regime, payment by results and fast-track support for PCTs. Executive summary HEALTH IN A COLD CLIMATE DEVELOPING AN INTELLIGENT RESPONSE TO THE FINANCIAL CHALLENGES FACING THE NHS CHRIS HAM, UNIVERSITY OF BIRMINGHAM INTRODUCTION This paper draws on discussions at a series of seminars held at the Nuffield Trust between March and May 2009 (see back page for details of the series). The aim of the series was to explore the financial context in which the NHS is working, and opportunities for using resources more efficiently. Each seminar was led by experts in NHS management and finance and participants included leaders from the public and private health care sectors. The ideas set out in this paper are based on the presentations at the seminars and the points made in the discussions they generated. The paper also draws on the work of the author, who bears sole responsibility for the views expressed.
Transcript of HEALTH INA COLD CLIMATEprojectes.camfic.cat/Docs/10_11/Health_in_a_Cold_Climate... · 2017. 2....

BRIEF ING PAPERJUNE 2009
� The NHS in England is faced with theprospect of finding savings of around£15–20bn over the period 2011–2014
� the Department of Health and NHSorganisations need to adopt an intelligentapproach to finding these savings that avoidsboth ‘salami-slicing’ and ‘slash and burn’
� a comprehensive approach to improvingefficiency is needed, encompassing actions atthe system, organisation, team andpractitioner levels
� at each level, the focus should be on usinginformation and incentives and buildingcapacity to deliver the necessary savings andimprovements
� the principal aim needs to be to reducevariations in clinical practice by engagingdoctors and other front-line staff inperformance improvement
� service line reporting shows promise and iscontingent on strengthening both operationalmanagement and clinical engagement
� the NHS Institute’s programmes also have animportant contribution to make through theuse of benchmarking and serviceimprovement methods with over £5bn ofpotential savings available
� the Department of Health should reviewcurrent policies with the aim of deciding whatchanges are needed as the NHS moves fromexpansion to contraction
� experience from other sectors suggests thatsuccessful change requires action on severalfronts simultaneously and work across a seriesof ‘dualities’
� these dualities include: providing centralleadership and supporting NHS organisationsto build capacity; using competition andpromoting cooperation; supportingcommissioners and drawing on the expertise offoundation trusts; valuing clinical engagementand strengthening the role of generalmanagers; emphasising the standardisation ofcare and ensuring that services are customisedaround the needs of individuals
� integrated systems have a potentiallyimportant role to play in future, in aligningincentives to facilitate the emergence of newmodels of care
� NHS foundation trusts could play animportant part in the development ofintegrated systems, but only if there arechanges to the regulatory regime, payment byresults and fast-track support for PCTs.
Executive summary
HEALTH IN A COLD CLIMATEDEVELOPING AN INTELLIGENT RESPONSE TO THE FINANCIAL CHALLENGES FACINGTHE NHSCHRIS HAM, UNIVERSITY OF BIRMINGHAM
INTRODUCTIONThis paper draws on discussions at a series of seminars held at the Nuffield Trust between March and May2009 (see back page for details of the series). The aim of the series was to explore the financial context inwhich the NHS is working, and opportunities for using resources more efficiently. Each seminar was led byexperts in NHS management and finance and participants included leaders from the public and privatehealth care sectors. The ideas set out in this paper are based on the presentations at the seminars and thepoints made in the discussions they generated. The paper also draws on the work of the author, who bearssole responsibility for the views expressed.

Following the 2009 Budget, the NHS faces theprospect of cuts in expenditure from 2011. While theexact scale and duration of these cuts will not beknown until the completion of the current spendingreview, it is likely that NHS spending will decline byaround two per cent a year in real terms until at least2014, and probably for a longer period (Ham, 2009).This suggests that the NHS in England will berequired to find savings of the order of between £15and 20bn over the three years from 2011 (Nicholson,2009). The prospect is therefore of the longest,sustained period of disinvestment in the history ofthe NHS, a mirror image of Tony Blair’s commitmentin 2000 to increase health care spending to bring itinto line with the European Union average.
The NHS is entering this period of retrenchment inmuch better shape than at any time in its history.The programme of investment and reform that has beenundertaken in the last decade has resulted in measurableimprovements in performance in many areas of healthcare. Most notably, waiting times for treatments havefallen dramatically and areas of clinical priority such ascancer and heart disease have improved significantly.These improvements have been accompanied by astrong financial performance. After running into deficitin 2005/06, the NHS is now in surplus and enters amuch tougher period of funding well-placed to dealwith the challenges that lie ahead. Equally important,public confidence in the NHS is now at a high level aftera number of years when it seemed that investment andreform were failing to have a positive impact onattitudes towards the NHS.
The improvements that have occurred are underlinedby the assessments undertaken by the CommonwealthFund of a group of six countries showing that theUnited Kingdom moved from third position to firstbetween 2004 and 2007 on a range of criteria.
Despite the progress made in the last decade, thereare no grounds for complacency. This is illustratedbelow by the United Kingdom’s relatively poorstanding in rankings of countries on mortalityamenable to health care (Nolte and McKee, 2008),and in the OECD’s comparisons of health status. Thelatter indicate that the United Kingdom is in themiddle of the pack and falls short of the results
achieved in countries such as Australia, France, Icelandand Sweden (Joumard et al, 2008). The United Kingdom’sperformance on cancer survival compared with othercountries is further evidence of the room for improvement.
Alongside evidence from international comparisons,analysis by the Office for National Statistics showsdeclining NHS productivity (see Figure 3). This reflectsthe failure to increase output at a comparable rate to thelarge sustained increases in resources made available tothe NHS. With much of the additional funding going intopay increases for staff following the introduction of newcontracts for consultants and GPs and the Agenda forChange reforms for other staff, patients have yet to see thefull benefits of the investment that has been made.
2
THE FINANCIAL CONTEXT
Figure 2. International comparison of rates of mortality amenable tohealthcare
Figure 1. International rankings of health care performance, 2007

3
HEALTH IN A COLD CLIMATE
The silver lining in these trends is that with theNHS in England now spending over £100bn perannum, there is much greater potential forbringing about productivity improvements thana decade earlier when the budget was only£40bn (House of Commons Library, 2009).History suggests that, almost regardless ofactions taken by Government or NHSorganisations, productivity is likely to improveas funding becomes more constrained. This isbecause as input falls output will remain stableor continue to increase in the face of risingdemands from patients, leading productivity torise almost regardless of what Government does.
In this context it is a safe prediction that theDepartment of Health will seek to contain costs byexercising tight control over the workforce. With aroundthree quarters of the NHS budget going on staff costs,there are likely to be vacancy freezes in manyorganisations, steps to reduce the use of agency andlocum staff, and action on pay and possibly pensions.There may also be difficulties findings jobs for newlytrained staff, especially as more doctors, nurses andother staff qualify from the expanded trainingprogrammes that have been put in place.
Other likely targets include:� achieving efficiency improvements in the
procurement of goods and services from externalsuppliers through the new commercial support unitsannounced in May this year
� rationalising back office functions through greateruse of shared services and possibly a reduction inthe number of NHS organisations, notwithstandingthe stated commitment of politicians to avoidfurther restructuring
� improving the use of the NHS estate by identifyingland and buildings surplus to requirements andacting on the proposals set out in the OperationalEfficiency Review commissioned by the Treasury(HM Treasury, 2009).
It is also certain that government will use its controlover the payment by results tariff as a way of puttingfurther pressure on efficiency.
As this happens, there is a clear risk that the quality ofcare may be compromised, especially at such an earlystage in the implementation of the initiatives announcedin High Quality Care for All (Secretary of State forHealth, 2008). The question then becomes: can theDepartment of Health and NHS organisations adopt amore intelligent approach to dealing with the financialchallenges that lie ahead that avoids the ‘salami-slicing’approaches that have characterised past periods of NHSretrenchment in which incremental amounts are takenaway from all budgets? Equally, will it be possible toresist the ‘slash and burn’ instincts of some NHS leaders,in which the focus is on identifying major areas ofspending to be cut back or eliminated?
SAVINGS TARGETS
Figure 3. Trends in NHS productivity

4
At the seminar series, Peter Smith of theUniversity of York offered the followingframework for thinking about ways ofimproving productivity (see Figure 4).
Alongside these two dimensions, it ishelpful to consider the role ofinformation, incentives and capacity inimproving productivity.
At the system level, the menu of optionsincludes:� using information to produce cost-
effectiveness guidance, for examplethrough NICE, to analyse the use ofresources on different areas of care, asin programme budgeting, and tobenchmark performance, as in the NHSInstitute’s Better Care, Better Value indicators
� using incentives to improve performance, forexample through payment by results, practice basedcommissioning, targets and the use of competition
� building capacity through the work of the NHSInstitute in service improvement and leadershipdevelopment and the work of the regulators, such asthe Care Quality Commission.
At the organisational level, there are various possibilities:� using information to promote service line reporting
in NHS organisations and to develop the electronicpatient care record
� using incentives such as the quality and outcomesframework (QOF) in primary care and the use ofteam-based incentives in all NHS organisations
� building capacity by strengthening the role of boardsin governance, developing the finance function, andimproving the ability of the NHS to usebenchmarking data and undertake statistical analysis
At the team and practitioner level, the options include:� using information to measure and compare
performance both in relation to cost and quality ofcare
� using incentives to reward staff, for example throughthe consultant contract and clinical excellenceawards
� building capacity by development leadership skillsamong managers and clinicians and through clinicalaccreditation and training.
The scale of the challenges facing the NHS calls for acomprehensive rather than piecemeal approach at all ofthese levels. Such an approach was developed by theDepartment of Health at the time of the last financialcrisis in the NHS in 2005, when the Departmentproduced The Efficiency Map setting out actions to betaken in different areas to deliver the savings needed atthat time.
A similar approach is required to enable the NHS toplan for the savings required after 2011. In this context,it is timely to review the potential contribution ofdifferent initiatives and whether the right levers andincentives are in place to enable to the NHS to rise tothese challenges. Monitor’s work on service linereporting and the NHS Institute’s work onbenchmarking and service improvement exemplify someof the opportunities.
A FRAMEWORK FOR IMPROVING PRODUCTIVITY
ComprehensivePiecemeal
System
Organization
Team
Practitioner
Figure 4. Productivity analysis framework

5
HEALTH IN A COLD CLIMATE
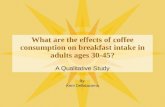
Bill Moyes of Monitor made the casefor service line reporting at theseminar series drawing on Monitor’swork with 35 NHS Foundationtrusts. Experience suggests that tobegin with, trusts need to reorganiseinto distinct and relevant businessunits. They then have to focus onproducing reliable service linefinancial and other data. Havingdone so, trusts can develop aportfolio matrix to identify good andpoor performance (see below). Otheressential elements are strong, capableservice line leaders, beginning withone or two evangelists who have theskill and will to lead the change, anddevolution of decision-makingpowers to service line leaders.
Services in the bottom left are thosewhere boards should be consideringcontraction, repositioning or evenexit from services. Those in thebottom right indicate opportunitiesfor expansion. The ones in the topright represent the high incomeearners.
A similar approach can be used tomap patient experience, with thedifference being an ability to takewhat patients say is important and,by structured questioning andcross-referral, produce a list ofderived satisfaction scores.
Because service line management isa sequential programme of businessmanagement tools, Monitor hasembarked on a three-yearprogramme to fully exploit thepotential for improvement withintrusts, in terms of both efficiencyimprovement (financial andproductivity indicators) and qualityimprovement (patient satisfaction,PROMs). See Figure 7 on next page.
The portfolio matrix approach can be used
to map patient experience and to highlight
priorities for improvement
Stated satisfaction
High
Low
Low High
Doctor
interaction
Patient response to survey in specific care setting or service line
Clinical
quality
Wait times
Nurse
interaction
CleanlinessPrivacyInformation
Facilities
Family
involvement
Pain relief
Support staff
interaction
Safety
Pre-care
Co-ordination
AftercareOther
Convenience
Re-prioritise Emphasise
De-prioritiseNo
investment
‘Performance
engines’
Attributes perceived
at level proportional
to importance
‘Hidden gems’
Underappreciated
attributes.
Reprioritize and
invest
‘Fool’s gold’:
Attributes with over-
emphasized
importance leading
to overinvestment
‘Low priority’
Attributes
appropriately
viewed as not
important
Derived
importance
Parking
0
0.5
1
1.5
2
-40 -30 -20 -10 0 10 20 30 40 50 60
Relative size of
speciality
EBITDA margin
Paediatrics
Ophthalmology
T&O
Neurology
Endocrinology
Rheumatology
Obstetrics
Gastroenterology
Plastic Surgery
Geriatric Medicine
Cardiology
General
Medicine
Gynaecology
General
SurgeryDermatology
Clinical Haematology
Genito-Urinary
Medicine
Diagnostic tool for analysing service portfolio performance promoted by Monitor INDICATIVE DATA
Good performance - maintainDrive better margin
Making money – grow activityImprove, or consider options
Improve cost
position
Benchmark
setter
Potential
growerNegative
return
Boards and clinical leaders are starting to
understand efficiency at service level
MONITOR’S WORK ON SERVICE LINE REPORTING
Figure 5. Diagnostic tool for analysing performance
Figure 6. Patient experience matrix

6
Key elements for 2009/10 include strengtheninginformation systems through patient-level costing, andunderstanding how to provide a better patientexperience and how to ensure accurate and reliablepatient-reported outcome measures are generated.
A practical example of service line management waspresented at the seminar series by Grant Kane fromCounty Durham and Darlington NHS Foundation Trust.The approach initially met with scepticism in the trust
and there were concerns that commercial disciplinescould jeopardise clinical practice and patient care. Ingeneral surgery, the starting position was a deficit of £1million in 2006/07: through service line managementthis became a surplus of £19,000 in 2008/09. The workinvolved analysing the composition of costs and thedifference between services in the north of the trust andthose in the south. The following figures illustrate theresults:
1.
2.
3.
Incrementallyincrease understanding and perfo
rmance
Three-year programme to fully exploit
the potential of SLM
2008/09
2009/10
2010/11
1. Comprehensive review
of organisational
structure
3. Produce reliable SL
financial/other data
2. Assess corporate
strengths/weaknesses
4. Identify (few) SL leaders
5. Devolve real decision
making
6. Coverage: total trust
roll-out plan
7. Complete information
systems on quality
and cost
8.Add quality and patient
experience
returns to scorecard at both
board
and service line
level
9. Complete scorecard with
staff / workforce returns
10. Embed reliable
performance planning/
assessment process
11. Use data to inform 3-year
planning round (critical)
12. Identify clinical process
improvement projects to
deliver better quality and
efficiency returns
Start Now
Figure 7. Three-year performance measurement programme

7
HEALTH IN A COLD CLIMATE
In the light of this analysis, the trustbenchmarked length of stay ingeneral surgery. This showed thetrust performing better than thenational average. However, ifaverage length of stay were in thetop 10 per cent, then there wouldbe scope for improving annualprofitability by £900,000. Ananalysis of the income received bythe trust by length of stay illustratedthis.
As the work progressed, a profitability‘driver tree’ was constructed for bothinpatient and outpatient services.Through this a number of ‘quick wins’were identified. As the followingfigure shows, many of these quickwins relate to clinical practice,including reducing the proportion ofpatients who come in the day beforetheir procedures, increasing day caserates, and cutting the number of beds.Improving recording was also asignificant issue, resulting in the trustincreasing income by almost£300,000.
8
Tariff
income
Nurs-
ing
Medi-
cal staff
Other
staff
Drugs MSE Diag-
nostics
Contri-
bution
Over-
heads
Cost of
Capital
Surplus
-1,6541,276
3,528
1,785531
1,119
1,501
1,633425
11,459
2,948
Tariff income
Direct Costs
Indirect Costs
Contribution
Contribution margin
Loss*
11,459
9,296
531
1,633
14%
-1,654
£000
South
£000
North
Tariff income
Direct Costs
Indirect Costs
Contribution
Contribution margin
Profit*
11,995
8,299
375
3,320
28%
646
2,609
11,995
3473,320
1,566
1,095
3751,109
3,093
1,156 646
… driven by a loss in the South and a smaller profit in the
North
% income
31% 26% 10% 4% 11% 5% 16% 13%
26% 22% 9% 3% 10% 3% 9% 13%
Significant
differenceXX
XX XX XX
* Profit/loss = contribution – overhead – cost of capital
Source: 2006-07 Pbr Income vs. 2006-07 Reference Costs
Figure 8b
7
Tariff income
Direct Costs
Indirect Costs
Contribution
Contribution margin
Loss*
£000
23,454
16,655
906
5,893
25%
-1,008
-1,008
5,556
23,454
7725,893
3,067
6,621
1,407
2,299906
3,834
Tariff
income
Nurs-
ing
Medi-
cal
staff
Other
staff
Drugs MSE Diag-
nostics
Contri-
bution
Over-
heads
Cost of
Capital
Loss
General Surgery Pbr income and reference costs, 2006/07
£000
* Profit/loss = contribution – overhead – cost of capital
Source: 2006-07 Pbr Income vs. 2006-07 Reference Costs
To understand our starting point, we conducted a profitability analysis
of General Surgery that showed an overall loss of £1m in 06/07
Figure 8a
Figures 8a, 8b, 8c, 8d. Service line management profitabilityanalysis: example

8
Action on these ideas led to theturnaround in financialperformance.
Stephen Eames, chief executive ofthe trust, has argued that serviceline management has had ‘adramatic effect on the developmentof clinical leadership and businesssystems’. In the case of generalsurgery, service line management‘successfully delivered an impressiveprogramme of change whichachieves the holy grail of improvingquality and reducing costs’ (Eames,2009).
It is important to emphasise that thewider application of service linereporting is contingent onstrengthening operationalmanagement and clinicalengagement, both of which arepatchy at best in many NHSorganisations. Most of the decisionsthat determine how resources areused are taken within clinicaldirectorates and primary carepractices and the capacity fordriving efficiency needs to besignificantly strengthened. If thisdoes not happen, then it will bemuch more difficult for the NHS toadjust to the tighter financialprospects that lie ahead.
13
Illustrative – cumulative bed profitability by day of patient stay
2 3 4 5 6 7 81
Profit – if patient discharged
within tariff ALOS
… with a significant impact on profitability
Day of patient stay
National
ALOS
National
trim point
No income is received
between tariff ALOS and tariff
‘trim’ point ALOS Income received for
excess bed days
above trim point, but
does not cover bed
costs
Source : Derek Murphy – Associate Director of Finance
Figure 8d
9
23.5
3.7
11.1
6.4
12.0
1.8
5.83.5
0.9
11.5
1.9
5.42.9
1.3 2.2
Total
06/07 General Surgery income*
£m
06/07 General Surgery total activity*
Thousand spells or attendances
South North Total
South North Total
* Excluding Urology
Outpatient
Emergency
Elective
Day cases
… although both sites have broadly comparable levels of activity
and income by POD
36.0
6.02.93.0
16.4
3.11.51.3
19.6
3.01.41.7
103
1,849
2,210
739
110
1,876
2,289
715
97
1,820
2,121
757
06/07 General Surgery income/spell or attendance*
£
South North Total
Figure 8c

9
HEALTH IN A COLD CLIMATE
Bernard Crump of the NHS Institute spoke at theseminar series on how the Institute has supported theNHS through its work on the Better Care, Better Valueindicators, High Volume Care and the Productive Seriesprogramme.
The Better Care, Better Value indicatorsuse routinely available NHS data toillustrate variations in performance.The indicators are updated everyquarter and each NHS organisationreceives a scorecard showing how it isdoing. This translates into aproductivity opportunity based on theorganisation achieving the top quartileof performance. Organisations canchoose comparators against which tobenchmark. The initial clinicalindicators are show in Figure 10.
Analysis had shown the size of theproductivity opportunity for the NHS asa whole fell from £2.2bn in the firstquarter of 2006/07 to £1.9bn in the
second quarter of 2007/08. New indicators were added in2008/09 and this, together with changes in activity andcoding, means that the current productivity opportunity is£3bn. All organisations, including those that are financiallystable, have major opportunities to improve performance,
THE NHS INSTITUTE’S WORK ON BENCHMARKING AND SERVICEIMPROVEMENT
Figure 10. NHS clinical indicators
– Reducing day-before admissions by 95%
– Shifting more elective procedures to higher-margin day cases
– Improving recording and income capture
– Decreasing controllable DNAs
– Decreasing number of beds through decreasing the bed capacity buffer
available to meet variable emergency demand
– Decreasing number of beds through streamlining elective demand
– Increasing discharge timeliness through addressing blocking social factors
– Increasing discharge timeliness through removing weekend holdups
– Matching staffing levels/mix to demand though higher staffing flexibility
– Improving outpatient profitability
– Increasing theatre utilisation
– Decreasing consumables costs ****
––1
––2
––7
––6
––5
––4
––3
––8
––9
––10
Through bottom-up analysis and cross site benchmarking, we identified
several quick-win ideas, and others that require deeper systemic
change
––11
––12
Quick wins(achievable within 6
months)
Longer-term
opportunities(achievable in 12 months;
require process redesign
and/or significant
behavioural change)
Figure 9. Organisational productivity opportunities

10
and it is surprising that the data is not usedmore.
The Better Care, Better Value indicators ledonto the High Volume Care programmefocused initially on eight HRGs thataccount for a high proportion of activitysuch as fractured neck of femur, acutestroke and cholecystectomy. The NHSInstitute visited high-performing andpoorly performing NHS trusts to reviewcare pathways and understand what wasgoing on. Interestingly, in many truststhere were examples of bothhigh-performing and poorly performingservices in different specialties.
The visits were undertaken by clinically-ledteams using structured visits. An examplewas the work on knee replacement thatfound wide differences in length of stay. Thekey here was early mobilisation of patients – within 12 to18 hours of surgery – and active discharge arrangements.In the second phase of work on high-volume care theInstitute worked with 12 trust chief executives andMcKinsey in an improvement network. The improvementsin stroke and fractured neck of femur were rapid andlarge-scale. This led into a third phase concentrating onnew high-volume areas such as renal care,cancer, and diabetes. The work on diabeteshad shown scope for cutting lengths of stayfor patients with diabetes admitted for otherdiagnoses by over two days on average,through better management.
In the Productive Series programme, theInstitute had applied lean thinking torelease resources for patient care. TheProductive Ward ‘Releasing Time to Care’initiative was the first in the series and hadbeen followed by work on theatres, thecommunity hospital and the leadershipteam. Whereas the previous twoprogrammes had been ‘pushing’ data outto the NHS, this work involvedorganisations ‘pulling’ in support to enablethem to improve performance. Over 180hospitals were using the tools and therewas also international interest, fromcountries including Australia and Holland.
Analysis suggested that up to £2.2bn could be saved fromthe High Volume Care and Productive Series work inEngland. Most of this is in the acute sector. This is basedon an estimate done at South West Strategic HealthAuthority that has been scaled up to England – see below.
Work has now started on community services wherethere seems to be huge potential to release resources.
Figure 12. Potential productivity gains from ‘scaling up’ innovation
Figure 11. NHS-wide productivity opportunities

11
HEALTH IN A COLD CLIMATE
These examples show that there is considerable potentialto improve productivity using information andapproaches that are already available or are underdevelopment. A clear message is that the principal focusshould be on reducing variations in clinical practice byengaging doctors and other front line staff in reviewingthe performance of the services for which they areresponsible. The scale of the savings that can be made,as illustrated by the examples of service linemanagement and the Better Care, Better Valueindicators, adds urgency to the work that is alreadygoing on in these areas. It also underlines the conclusionof High Quality Care for All that doctors need to bemuch more effectively involved in leadership to enablethese savings to be realised.
As previous work by the Nuffield Trust has shown(Ham, 2007a), a key question is whether the policylevers are in place at a system level to support NHSorganisations in taking these approaches forward? Inaddressing this question, it is important to note thatmany of the current policies (such as NICE, nationalservice frameworks and payment by results) were put inplace at a time when the NHS budget was expandingand were designed to support implementation ofobjectives such as the reduction of waiting times. Itremains a moot point whether these policies will enablethe NHS to cope with reductions in resources. It istherefore opportune to consider whether any changes inthe reform programme need to be made.
As this happens, the time lag between developing newpolicies and their full implementation needs to be bornein mind. An example is the policy on payment byresults, which was first announced in 2002 and which isstill being extended to new areas of care. This examplesuggests that existing levers will continue to play animportant part for the foreseeable future, with any majorchanges having an impact further down the track.
In thinking through these issues, it is as well toremember that the improvements in NHS performancethat have occurred to date have been driven mainly bythe use of targets linked to performance management.Policies on choice and competition have so far madeonly a marginal impact (Audit Commission andHealthcare Commission, 2008). Equally important, theagenda set out in Lord Darzi’s report, High Quality Care
for All, of reform being led locally by clinicians, remainsembryonic, not surprisingly so as less than a year haselapsed since publication of the report.
It is also the case that providers occupy a more powerfulposition than commissioners within the NHS. Withworld class commissioning a work in progress, andpractice-based commissioning yet to fully engage GPs onthe scale needed to manage demand and deliver servicescloser to home, is it realistic to expect thatcommissioners can do most of the hard work needed torise to the financial challenges that lie ahead? If not,should more emphasis be placed on the role that NHSfoundation trusts can play, recognising that nearly all ofthe most experienced leaders are in NHS foundationtrusts rather than PCTs?
Experience of bringing about transformational change inother sectors cautions against a simplistic ‘either/or’answer to these questions. Evidence from these sectorssuggests that successful change requires action onseveral fronts simultaneously as well as an approach thatrecognises the need to work across a series of dualities(Pettigrew, 1999). To be more specific, Ministers andcivil servants leading change at a system level need tofocus on:
� providing central leadership and supporting NHSorganisations to build capacity and leadership forchange at a local level
� using competition in areas of health care where it islikely to offer the greatest benefits and promotingcooperation where organisations need to worktogether to improve performance
� supporting commissioners to play an increasing rolein improving productivity and performance anddrawing on the expertise of the best NHSfoundation trusts to take the actions that are needed
� continuing to emphasise the value of clinicalengagement and leadership and strengthening therole of general managers at all levels of the NHS
� emphasising the importance of standardisation ofcare where there is evidence this will bring benefitsand ensuring that services are customised aroundthe needs of individuals.
POLICY LEVERS

12
Experience in other health care systems underlines therelevance of these observations. High performing healthcare organisations such as the Veteran’s HealthAdministration, Intermountain Healthcare andJonkoping County Council owe their success to theadoption of sustained strategies of improvement, inwhich medical leaders work hand in hand withexperienced managers to bring about change and in sodoing are supported by timely and accurate informationabout their services. These organisations also makejudicious use of incentives to support their strategies(Baker et al, 2008), thereby lending support to theframework of ‘information, incentives and capacity’proposed by Peter Smith and discussed earlier in thispaper.
One of the common characteristics of high-performingorganisations is that they value the role of medicalleaders and use information and incentives as part of anintegrated approach to health care. The same is true ofother organisations such as Kaiser Permanente and theGeisinger Health System that have been recognised asleaders in quality improvement. While the precise formthat integration takes varies, it usually encompasses thecoming together of funding and most elements ofservice provision within the same organisation.Integration enables these organisations to alignincentives to facilitate the provision of care in the mostcost-effective settings.
The benefits of integration were recognised in the HealthStrategy Review undertaken by Adair Turner at therequest of the Prime Minister in 2001/02. Ongoing workby the author and by the Nuffield Trust is exploringhow these benefits can be exploited in the next stage ofNHS reform. The opportunity created by integratedsystems is to enable more care to be provided closer tohome and to reduce the use of expensive and ofteninappropriate hospital services. This has beendemonstrated in comparisons between the NHS andKaiser Permanente that show the latter using only onethird of the hospital bed days as the NHS for peopleaged 65 and over (Ham et al, 2003). With the NHSchief executive highlighting opportunities for reducingthe use of hospitals by people who no longer requirespecialist facilities as one of the most promising meansof delivering the improvements in efficiency required inthe NHS (Nicholson, 2009), it appears that the value ofintegration is at last being recognised.
Making progress on integration depends critically onprimary care practices collaborating in federations ornetworks and investing in the buildings, equipment andinfrastructure needed to support these developments.Fragments of what a new configuration of services mightlook like are beginning to emerge in parts of the NHS,both through the initiative of NHS organisations andthrough joint ventures between the NHS and theindependent sector. To return to an earlier point,integration may gain greater traction as the NHSmigrates from expansion into a cold financial climate,not least because the risks in the current system of cost-shifting and blame-shifting between organisations maybe too great for the system to bear. The challenge now isto convert the small-scale examples of integration thatcurrently exist (Ham, 2007b) into more ambitiousapproaches covering entire health communities.
One way of doing this is to support innovators inprimary care to reach into hospitals and to formstronger links with community health service and socialcare providers (Ham, 2007b). Another approach is tosupport experienced and successful leaders in NHSfoundation trusts to lead the development of integration.The risk in such an approach is that an ‘acute servicesmindset’ may dominate primary care and communityhealth services and suck more resources into hospitals.
To avoid this risk, there must be changes to theregulatory regime for NHS foundation trusts and topayment by results. Monitor’s oversight of foundationtrusts has brought many benefits but has had theconsequence of creating strong incentives for trusts toincrease activity and income in order to meet thefinancial targets set under the regulatory regime. Theseincentives are reinforced by payment by results, whichwas designed to reward trusts that treat more patients inorder to achieve the policy aims of cutting waiting listsand waiting times. The combined effect has been to turnacute hospitals into profit centres whose leaders arefocused on increasing income and surpluses.
As the NHS moves from expansion to contraction, andas the policy focus shifts from improving access toplanned care to achieving improvements in unplannedcare and care for people with long-term conditions, adifferent approach is needed (Ham, 2008). Acutehospitals will continue to play an important part in theprovision of care within the NHS but much moreemphasis needs to be put into delivering the vision set

13
HEALTH IN A COLD CLIMATE
out in the 2006 White Paper, Our Health, Our Care,Our Say (Secretary of State for Health, 2006), of carebeing provided closer to home with resources directedtowards prevention and services in the community.Implementing this vision requires a fundamentalreconceptualisation of acute hospitals as cost centresrather than profit centres. It also means adopting thephilosophy of integrated systems like KaiserPermanente, in which ‘an unplanned admission is a signof system failure’ and where the focus is therefore onadmission avoidance through prevention and earlyintervention.
Alongside changes to the regulatory regime and paymentby results, there needs to be a strong countervailingforce able to act as guardian and sponsor of the visionset out in Our Health, Our Care, Our Say. In theory, thisis the role of PCTs but the results of the world classcommissioning assurance programme demonstrate thatPCTs are on a long-term journey of improvement and inmany areas have much work to do to perform to thestandards expected of them (Department of Health,
2009). Part of the challenge facing PCTs is how toacquire the people and skills they need to commissionto world-class standards. The development ofarrangements such as those emerging in London, wheresix commissioning hubs are being established to supportthe work of 31 PCTs, may be one way of addressing thischallenge, alongside further intensive support to PCTs toenable them to fill the gaps identified in the world classcommissioning assurance programme. The supportprovided to PCTs now needs to be fast-tracked, as the‘NHS recession’ has arrived too soon to allow currentprogrammes simply to run their course.
The key policy question then becomes how to calibratethe role of competition and cooperation in the nextstage of reform, at a time when the recently establishedCooperation and Competition Panel is actively seekingto open up the market in health care, and whenintegrated systems might appear to limit choice andcompetition. Addressing this question needs to be at theheart of the reassessment of policy that must now takeplace.

14
It is clear from the work reported here that there isconsiderable scope to use the current budget for theNHS in England of over £100bn more efficiently. Theprincipal focus should be on reducing variations inclinical practice by engaging doctors and otherfront-line staff in performance improvement. The workof the NHS Institute has highlighted opportunities tosave over £5bn in this way, even before theproductivity gains in the community health servicesare quantified. Realising these savings requires astrengthening of operational management and clinicalengagement and the systematic use of incentives andinformation.
An intelligent response to the challenges facing theNHS would entail action on several frontssimultaneously and work across a series of dualities.As this happens, there is a need to support the mostexperienced and successful NHS leaders to developintegrated approaches to care to facilitate the
provision of services in the most cost-effective settingsand to avoid cost-shifting and blame-shifting. Theseapproaches need to go beyond the small-scaleexamples of integration that currently exist toembrace more ambitious initiatives covering wholehealth communities.
Alongside integrated approaches to service provision,there is a need to ensure that there is a countervailingforce able to avoid ‘provider capture’ and to promotethe delivery of services in the most cost-effectivesettings.
The Department of Health must urgently reviewcurrent policies, many of which were devised tosupport the considerable expansion of provision thathas occurred in the last decade. This includesreassessing the role of competition and cooperation incontributing to service improvement.
CONCLUSION

15
HEALTH IN A COLD CLIMATE
� Audit Commission and Healthcare Commission (2008)Is the Treatment Working?
� Baker, R et al (2008) High Performing HealthcareSystems. Toronto: Longwood Publishing.
� Department of Health (2005) The Efficiency Map.
� Department of Health (2009) World ClassCommissioning monthly update, May.
� Eames, S (2009) ‘Opinion’, Health Service Journal,5 March.
� Ham, C et al (2003) ‘Hospital bed utilisation in theNHS, Kaiser Permanente and the US MedicareProgramme: analysis of routine data’ BMJ 327:1257–60.
� Ham, C (2007a) Increasing NHS efficiency. TheNuffield Trust.
� Ham, C (2007b) Clinically Integrated Systems: Thenext step in English health reform? The Nuffield Trust.
� Ham, C (2008) ‘Incentives, priorities and clinicalintegration in the NHS’, Lancet, 371: 98–100.
� Ham, C (2009) ‘The 2009 Budget and the NHS’ BMJ,338: 1024–5.
� HM Treasury (2009) Operational Efficiency Review:Final report.
� House of Commons Library (2009) NHS Expenditurein England.
� Joumard, I. et al (2008) Health Status Determinants:Lifestyle, environment, health care resources andefficiency. Paris: OECD.
� Nicholson, D (2009) The Year 2008/09. Department ofHealth.
� Nolte, E. and McKee, M. (2008) ‘Measuring the healthof nations: updating an earlier analysis’ Health Affairs,27(1): 58–71.
� Pettigrew, A. (1999) ‘Organising to improve companyperformance’, Warwick Business School Hot Topics1(5).
� Secretary of State for Health (2006) Our Health, OurCare, Our Say. TSO
� Secretary of State for Health (2008) High Quality Carefor All: NHS Next Stage Review final report. CM7432.TSO.
REFERENCES

For more information contact:
The Nuffield Trust59 New Cavendish StreetLondon W1G 7LP
Tel: 020 7631 8450Email: [email protected]
www.nuffieldtrust.org.uk
© Nuffield Trust 2009
HEALTH IN A COLD CLIMATE
THE SEMINAR SERIESThursday 19 March:NNHHSS PPrroodduuccttiivviittyy:: rreecceenntt ttrreennddss aanndd tthhee cchhaalllleennggee ooff mmeeaassuurreemmeenntt, Peter Smith, University of York
Thursday 2 April:SSeerrvviiccee LLiinnee MMaannaaggeemmeenntt:: iimmpprroovviinngg eeffffiicciieennccyy iinn NNHHSS FFoouunnddaattiioonn TTrruussttss, Bill Moyes, Monitor, and Grant Kane,County Durham and Darlington NHS Foundation Trust
Wednesday 29 April:TTaacckklliinngg VVaarriiaattiioonnss iinn PPeerrffoorrmmaannccee:: wwhhaatt hhaass bbeeeenn aacchhiieevveedd aanndd aarree tthhee rriigghhtt iinncceennttiivveess iinn ppllaaccee?? Bernard Crump,NHS Institute, and Andy McKeon, Audit Commission
Tuesday 19 May:HHooww CCaann CCoommmmiissssiioonneerrss DDrriivvee IImmpprroovveemmeennttss iinn PPeerrffoorrmmaannccee?? Mark Britnell, Department of Health, andNick Hicks, Milton Keynes PCT
New Frontiers in NHS EfficiencyIn July, the Nuffield Trust will be launching a major new programme of research and policy analysis that focuses on howcommissioners and providers can cross new frontiers in making the NHS more efficient at a time of severe financialconstraint.
Rigorous analysis of existing UK and international research evidence forms the core of this programme of work, and willbe supplemented by newly-commissioned empirical research. A set of linked projects will draw upon this researchevidence in making policy recommendations about how the NHS can seek to sustain and improve service quality in theeconomic downturn.
Topics to be explored in the New Frontiers programme include:
� learning from international experience of priority-setting
� setting funding priorities within PCTs
� lessons from past experience of technical efficiency and cost improvement
� the potential of integrated care to improve efficiency
� new frontiers in the use of data; and the implications for the future of commissioning in the NHS.
Further details will be announced on our website www.nuffieldtrust.org.uk, or contact Dr Judith Smith, Head of Policy [email protected]