
Health in an egalitarian society Espen Dahl Professor Oslo and Akershus University College Harvard...
19
Health in an egalitarian society Espen Dahl Professor Oslo and Akershus University College Harvard Club of New York, April 22th 2015
-
Upload
darcy-kelley -
Category
Documents
-
view
214 -
download
0
Transcript of Health in an egalitarian society Espen Dahl Professor Oslo and Akershus University College Harvard...
Health in an egalitarian society
Espen DahlProfessor Oslo and Akershus University College
Harvard Club of New York, April 22th 2015
Mandate - to analyze social inequalities in health and in the consequences of ill-health; and examine trends and comparisons with other countries
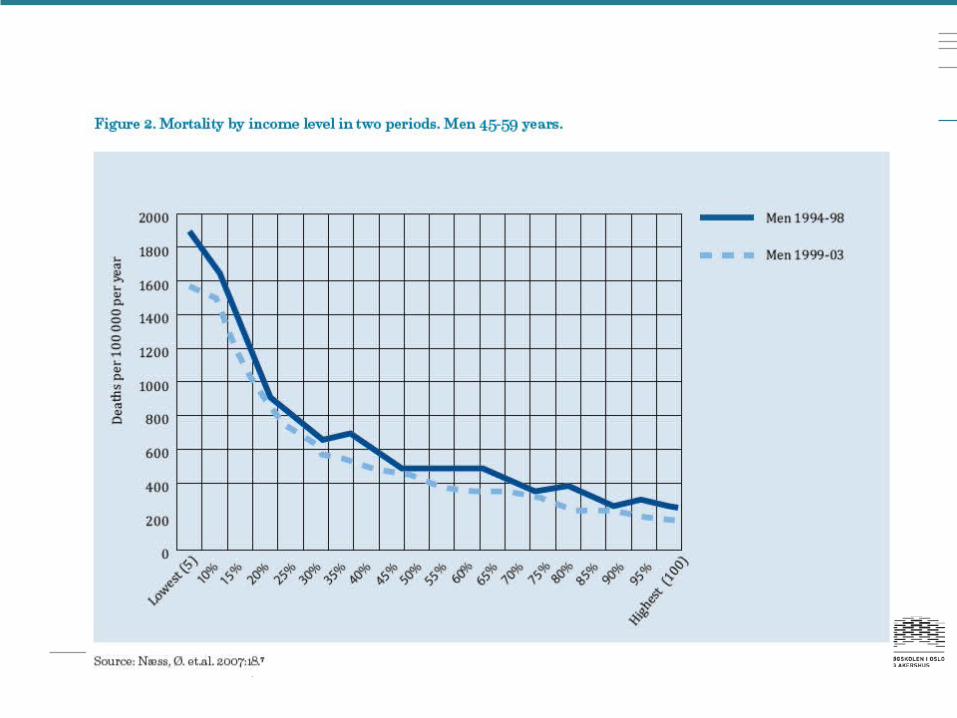
Social inequalities in health exist….…and form a gradient
….appear in all phases of life
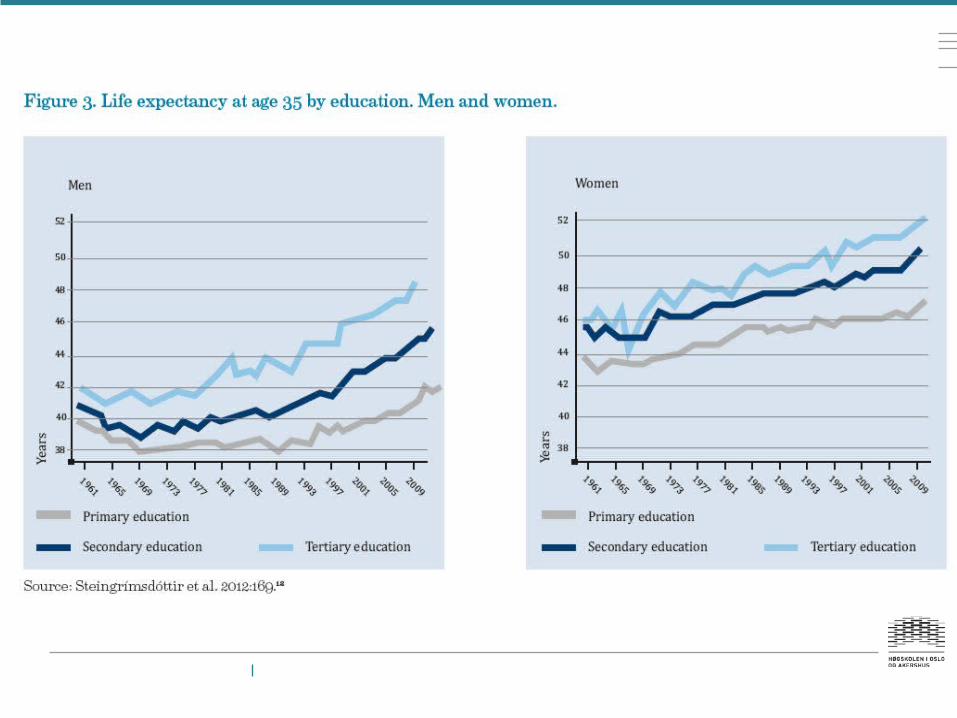
… for men and women
….for most socioeconomic indicators
….for most, but not all indicators of health
….and persist over time; increase for some health outcomes and decline for others
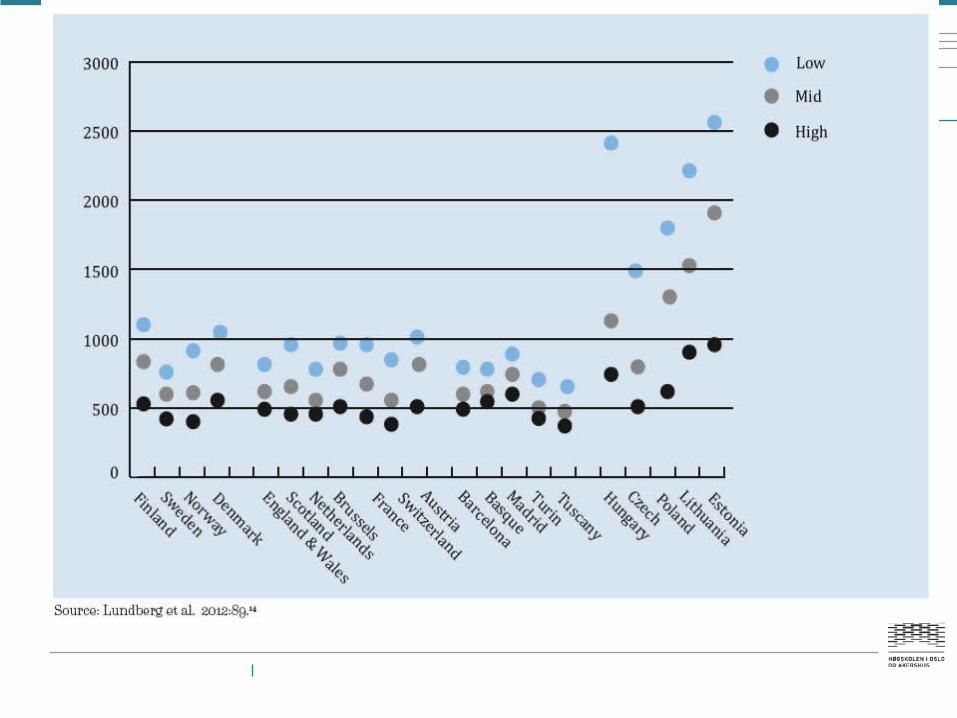
….and are not necessarily smaller in Norway and in Nordic countries than in other countries in Western-Europe
The social determinants of health
“Health inequities arise from the societal conditions in which people are born, grow, live, work and age, referred to as social determinants of health. These include early years' experiences, education, economic status, employment and decent work, housing and environment, and effective systems of preventing and treating ill health.”
Source: The Rio Declaration on Social determinants of health
Three challenges to existing knowledge
Challenge 1: Persistent social inequalities in health in Norway
Challenge 2: Increasing educational inequalities in mortality and longevity - in all Nordic countries
Challenge 3: Not smaller social inequalities in health in Norway and the other Nordic countries than in other Western European nations and populations
Persisting social inequalities in Norway
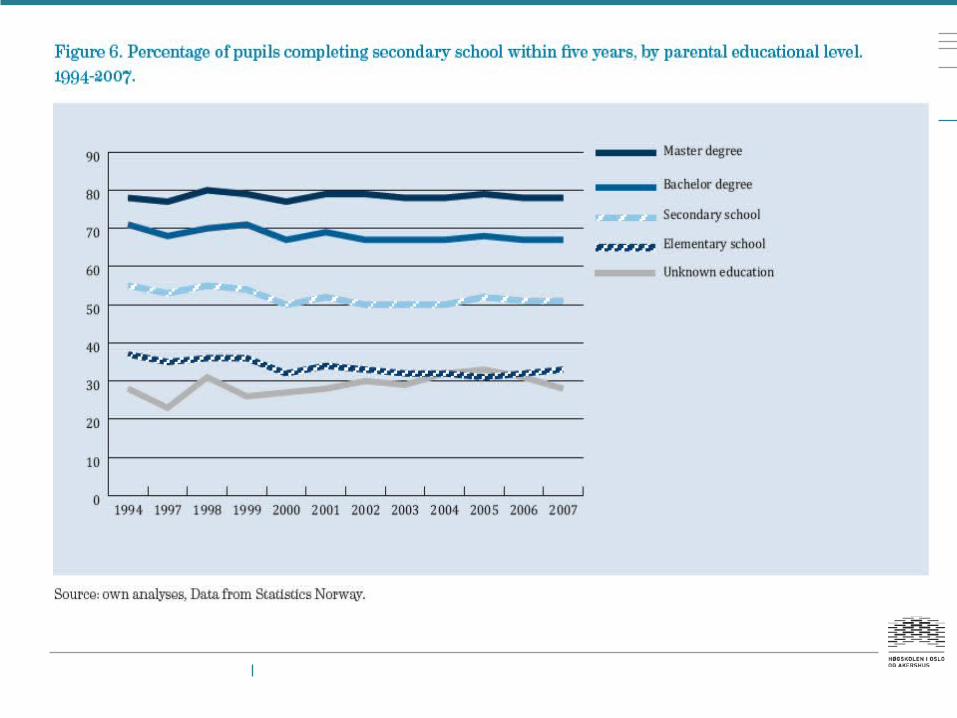
1. Early year’s experience and learning conditions
2. Distribution of economic resources
3. Work environment
4. Health-related behaviour
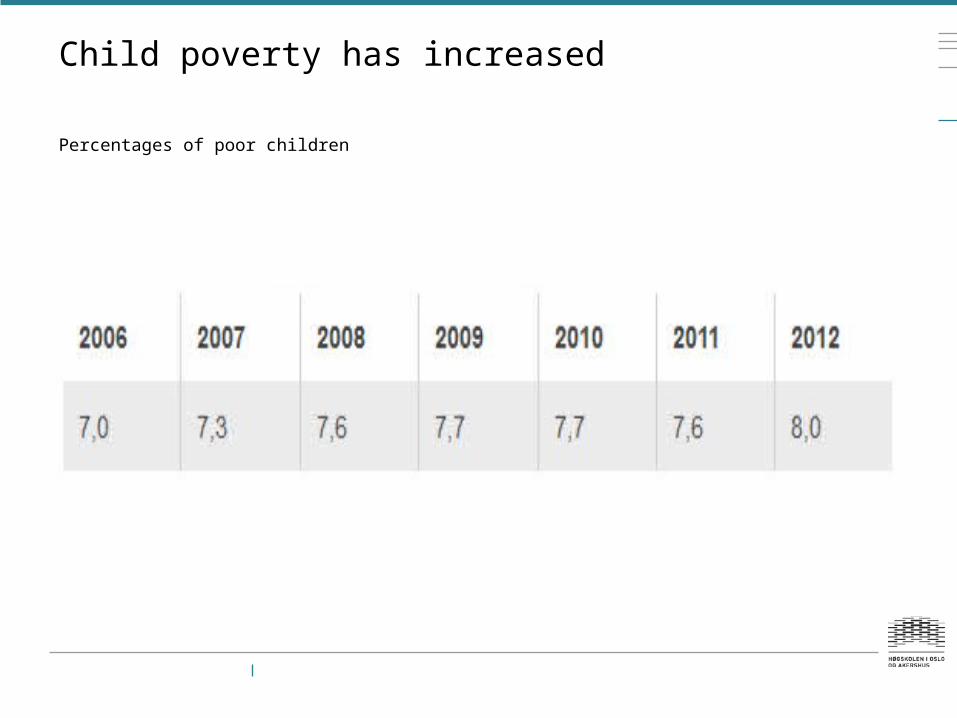
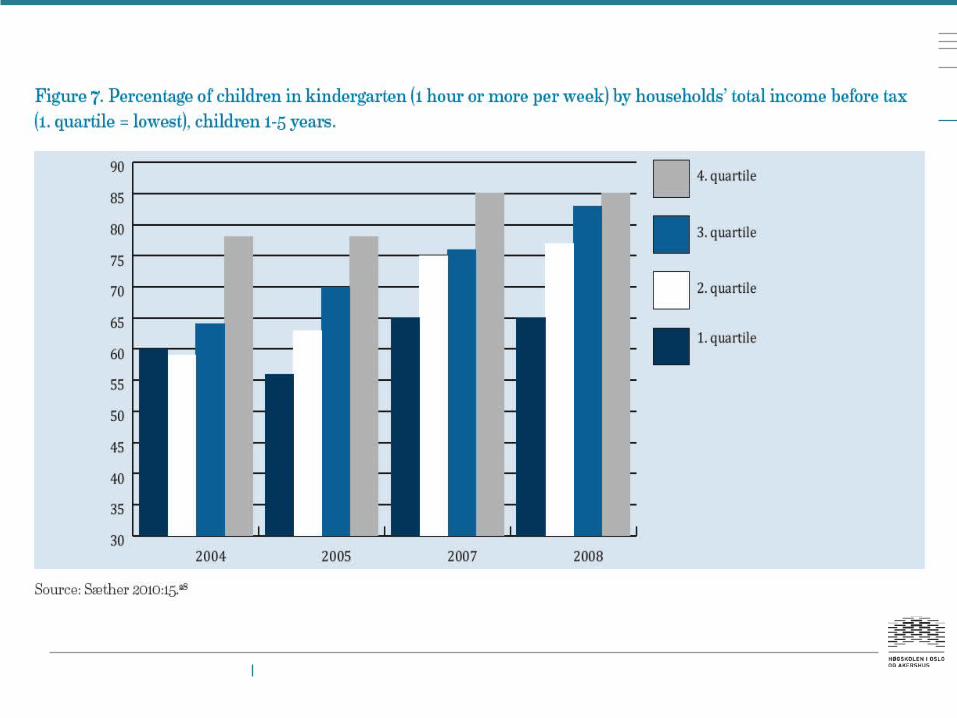
Child poverty has increased
Percentages of poor children
Wealth, income and earnings
Wealth
Norway: Rich: 472,8. Super-rich 63,6 persons per million inhabitants. USA : Rich 124,6. Super-rich 36,5 persons per million inhabitants.
IncomeIncome poverty: Stable around 8 per cent
Household disposable income: Gini 1986 = 0.21, 2011 = 0.24
Market incomes: Gini: Norway =0.38. OECD average = 0,41
Earnings
Since late 1990s have montly wages among lower educated groups been lagging behind the higher educated (from 90 Per cent to 80 per cent of the average of all groups).
The same development is seen among different occupational groups: low status occupations are lagging behind
Sources: Dahl et al 2014, Moene 2014, Pedersen 2013
Rich > 30 million dollar. Super-rich > 100 million dollar.
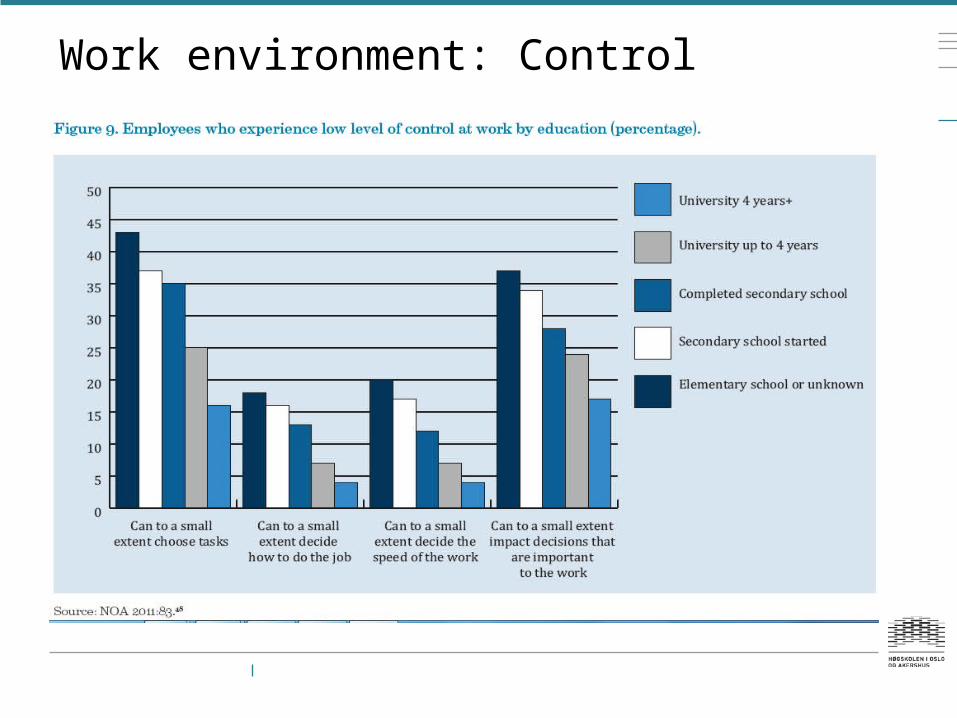
Work environment: Control
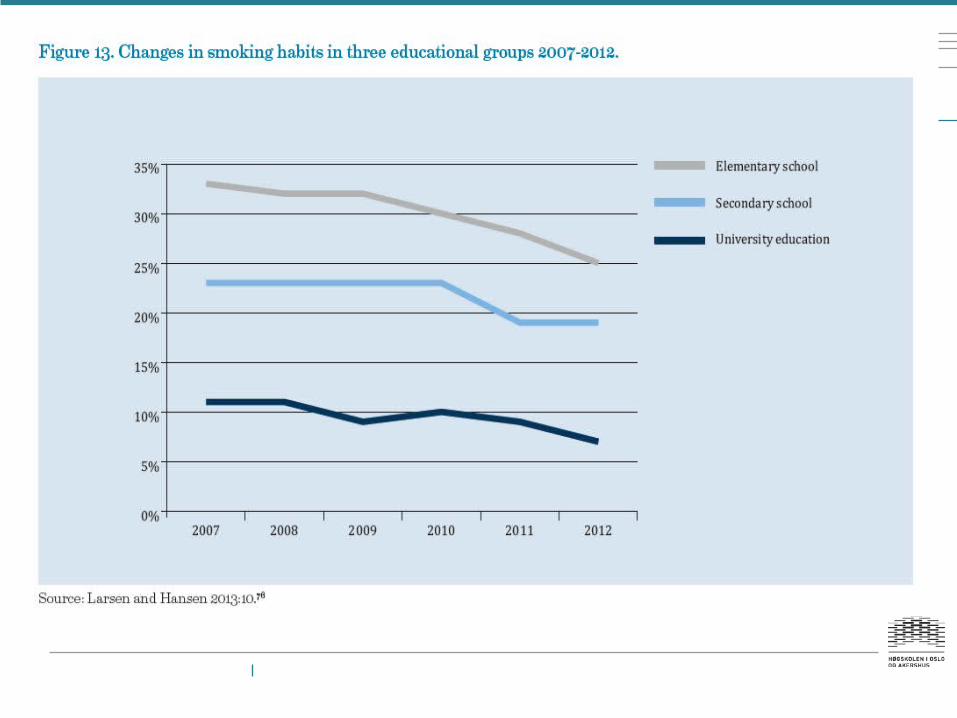
Health-related behaviour: smoking
Educational inequalities in smoking are particularily large in Norway
Estimated that they account for 25 per cent of educational inequalites in over-all mortality
The increase in educational inequalities in mortality is largely due to smoke-related causes of mortality, i.e. COPD and lung cancer.
The smoking epidemic seems to follow the pattern of «diffusion of innovations». Now, at the end of the epidemic, the educational inequalities in smoking are about to decline.
The three challenges revisited
1. An «infrastructure» of inequalities in material and immaterial goods, resources and exposures
+2. Large (and growing) inequalities in smoking between educational groups.
= 3. Explain the three challenges
Thank you for your attention
www.hioa.no/helseulikhet


















