
Health Care Update and Changes Gayln L Bowers. Agenda Health Care Plan Data Plan Changes Questions...
30
Health Care Update and Changes Gayln L Bowers
-
Upload
michael-caldwell -
Category
Documents
-
view
214 -
download
0
Transcript of Health Care Update and Changes Gayln L Bowers. Agenda Health Care Plan Data Plan Changes Questions...

Health Care Update and Changes
Gayln L Bowers

Agenda
Health Care Plan Data
Plan Changes
Questions and Answers

2004-2005 PUC left Adventist Risk Management Health Care Plan and implemented the Pacific Union College Self Insured Group Health Care Plan.
No employee contribution for the 2004-2005 plan year.
PUC Group Health Care Plan is a bundled plan inclusive of medical, prescription, dental and vision.
Health Care Plan Review

• Health and Wellness Program enhanced during the 2004-2005 plan year to encompass a greater preventative strategy.
Health Care Plan Review

•Employee Contribution Implemented July 1, 2005•Employee Only - $30.00 per month•Employee +One - $50.00 per month•Employee + 2 or more - $75.00 per month
•Employee Contribution Changed July 1, 2009
•Employee Only - $50.00 per month•Employee +One - $80.00 per month•Employee + 2 or more - $110.00 per month
Health Care Plan Review
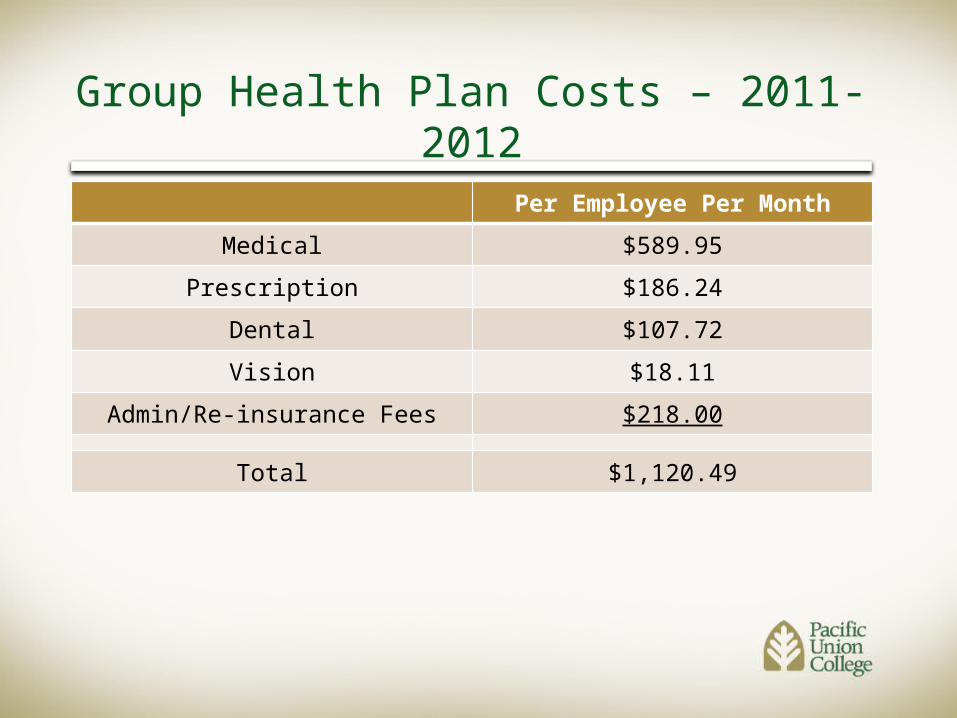
Per Employee Per Month
Medical $589.95
Prescription $186.24
Dental $107.72
Vision $18.11
Admin/Re-insurance Fees $218.00
Total $1,120.49
Group Health Plan Costs – 2011-2012

EE 2-Party Family
Medical & RX
PPO $636.31 $1,251.64 $1,851.04
HDHP $538.61 $1,059.46 $1,536.35
HSA Fund $83.33 $166.67 $166.67
Dental
PPO $61.85 $122.32 $217.59
Vision
Vision Plan $13.92 $27.39 $39.71
Group Health Plan Costs – 2011-2012Premium Equivalencies per Month

•ALL employees working 37.5+ hours per weeks are offered medical insurance.
•We have 91 full-time faculty and 153 full-time staff.
•TOTAL of 244 full-time employees
•100% of our full-time employees have picked up the college’s health care plan
Employees

• 100 % of full-time faculty members are on the College’s health care plan
• 100 % of full-time staff members are on the College’s health care plan
• 32 faculty members have the single plan
• 26 faculty members have the employee + one plan
• 33 faculty members have the employee + two or more plan
• 60 staff members have the single plan
• 44 staff members have the employee + one plan
• 49 staff members have the employee + two or more plan
Health Care Coverage

• Total of 48 part-time employees
• 9 Faculty Members• 39 Staff Members• Employees working
20+ hours are eligible for a buy-in to the health care plan.
Part-time Employees

• Unlimited Lifetime Maximum Benefit
• No Pre-existing Exclusions
• Dependent Coverage up to age 26
• Affordable Care Act (ACA) Re-defines a full-time employee to at least 30 hours per week
•ACA establishes two fees Qualified Health Plans will be required to pay
•Patient-Centered Outcomes Research Institute (PCORI) Fee
•Transitional Reinsurance Program Fee
Why Plan Changes?

Plan Changes

Hea
lth P
lan • Medical
• Prescription• Dental• Vision

Med
ical
& P
resc
riptio
n • Base Plan• Traditional• High
Deductible Den
tal
Vis
ion

Base PPO Health Care PlanIn-Network Out-of-Network
Annual Deductible $250 Individual$500 Family
Coinsurance 80% 50%
Office Visit Copay $25 per visit Primary Care, Deductible waived$40 per visit Specialist, Deductible waived
Annual Maximum Out-of-Pocket $4,500 Individual$9,000 Family
$8,000 Individual$12,000 Family
Lifetime Maximum Benefit Unlimited

Base PPO Health Care PlanIn-Network Out-of-Network
Outpatient & Inpatient Services
Preventive Care Covered 100%, Deductible waived 50%
Inpatient Hospital Services 80% 50%
Emergency Room($50 copay waived if admitted)
$50 copay then covered 80%(see full list for Level ER service copays)
Outpatient Services (Labs, X-rays) 80% 50%
Additional Services Covered (refer to full plan summaries for benefits and limitations)
Minimum Essential Benefits

Prescriptions/Pharmacy Retail-30 Day Supply
Home Delivery- 90 DaySupply
Generic $10 $15
Brand $40 $40
Non-Formulary $55 $50
Special Medications $85 $50
Base PPO Health Care Plan

Base PPO Health Care PlanEmployee Monthly Contribution
Employee Only $25.00
Employee + One $40.00
Employee + Two or More $55.00

Traditional PPO Health Care PlanIn-Network Out-of-Network
Annual Deductible $350 Individual$700 Family
Coinsurance 80% 50%
Office Visit Copay $25 per visit Primary Care, Deductible waived$40 per visit Specialist, Deductible waived
Annual Maximum Out-of-Pocket $3,000 Individual$6,000 Family
$5,000 Individual$10,000 Family
Lifetime Maximum Benefit Unlimited

Traditional PPO Health Care PlanIn-Network Out-of-Network
Outpatient & Inpatient Services
Preventive Care Covered 100%, Deductible waived 50%
Inpatient Hospital Services 80% 50%
Emergency Room($50 copay waived if admitted)
$50 copay then covered 80%(see full list for Level ER service copays)
Outpatient Services (Labs, X-rays) 80% 50%
Additional Services Covered (refer to full plan summaries for benefits and limitations)
Physical, Occupational & Speech TherapyVision Therapy and Care Durable Medical Equipment Organ & Tissue
Transplant Refractive Eye Surgery

Traditional PPO Health Care PlanPrescriptions/Pharmacy Retail-30 Day
SupplyHome Delivery- 90 Day
SupplyGeneric $10 $15
Brand $35 $40
Non-Formulary $40 $50
Special Medications $80 $50

Traditional PPO Health Care PlanEmployee Monthly Contribution
Employee Only $50.00
Employee + One $80.00
Employee + Two or More $110.00

High Deductible Health Plan with Health Savings Account
In-Network Out-of-Network
Employer HSA Funding $1,000 Individual$2,000 Family
Annual Deductible $2,000 Individual$4,000 Family
Coinsurance 90% 50%
Office Visit Copay $25 per visit Primary Care$40 per visit Specialist
Annual Maximum Out-of-Pocket $3,000 Individual$6,000 Family
$5,000 Individual$10,000 Family
Lifetime Maximum Benefit Unlimited

High Deductible Health Plan with Health Savings Account
In-Network Out-of-Network
Outpatient & Inpatient Services
Preventive Care Covered 100%, Deductible waived 50%
Inpatient Hospital Services 90% 50%
Emergency Room($50 copay waived if admitted)
$50 copay then covered 90% (see full list for Level ER service copays)
Outpatient Services (Labs, X-rays) 90% 50%
Additional Services Covered (refer to full plan summaries for benefits and limitations)
Physical, Occupational & Speech TherapyVision Therapy and Care Durable Medical Equipment Organ & Tissue
Transplant Refractive Eye Surgery

High Deductible Health Plan with Health Savings Account
Prescriptions/Pharmacy Retail Delivery – 30 DaySupply
Home Delivery- 90 DaySupply
Generic $10 $15
Brand $35 $40
Non-Formulary $40 $50
Special Medications $80 $50

Annual Deductible $75 Individual$150 Family
Coinsurance 80%
Preventive Care Covered 100%, Deductible waived
Annual Maximum $3000 Individual$6000 Employee + One
$9000 Employee + FamilyOrthodontia 50% Coinsurance
$2400 Lifetime Maximum Covered up
to age 26Employee Monthly Contribution
Employee Only $15.00
Employee + One $30.00
Employee + Two or More $60.00
Dental Plan

Annual Deductible None
Coinsurance 80%
Preventive Care N/A
Annual Maximum $560
Employee Monthly Contribution
Employee Only $5.00
Employee + One $10.00
Employee + Two or More $15.00
Vision Plan

Enrollment Form
2010
GROUP HEALTH PLAN ENROLLMENT/CHANGE FORM EMPLOYEE ENROLLMENT
Male Female
Last Name First Name MI Social Security Number
Street # & Name Telephone Number
City, State, Zip Code Date of Birth
New E n r o llm e n t
Q u a lify in g E v e n t
Change Eff. D a t e :
SELECT ONE FROM EACH DEPENDENT SELECTION Medical Traditional Plan Employee Only
High Deductible Plan Employee + One Base Plan Employee + Family Waived
Dental Employee Only Employee + One Employee + Family W a iv e d
Vision Employee Only Employee + One Employee + Family Waived

Enrollment Form
DEPENDENT ENROLLMENT (Complete, if enrolling, for each eligible dependent)
Relationship First and Last Name of Dependent Social Security Number Gender Date of Birth Coverage Elected
Husband Wife
Male Female
Medical/Rx Dental Vision
Child Step-Child Other: please specify
Male Female
Medical/Rx Dental Vision :
Child Step-Child Other: please specify
Male Female
Medical/Rx Dental Vision
Child Step-Child Other: please specify
Male Female
Medical/Rx Dental Vision
Does dependent have other group coverage including Medicare or Medicaid? If yes, please complete information on opposite page.

Questions


















