Health care in south africa : FOCUSING ON WOMEN AND CHILDREN
23
HALEY BOLING PUBLIC HEALTH IN SOUTHERN AFRICA HEALTH CARE IN SOUTH AFRICA: FOCUSING ON WOMEN AND CHILDREN
description
Health care in south africa : FOCUSING ON WOMEN AND CHILDREN. Haley Boling PUBLIC HEALTH IN SOUTHERN AFRICA. OVERVIEW. POVERTY AND HIV/AIDS PREVALENCE How do these factors affect mothers and children? What is being done to combat these issues? FUNDING OF PUBLIC HEALTH CARE - PowerPoint PPT Presentation
Transcript of Health care in south africa : FOCUSING ON WOMEN AND CHILDREN

H A L E Y B O L I N GP U B L I C H E A LT H I N S O U T H E R N A F R I C A
HEALTH CARE IN SOUTH AFRICA: FOCUSING ON WOMEN
AND CHILDREN

OVERVIEW
• POVERTY AND HIV/AIDS PREVALENCE• How do these factors affect mothers and children?• What is being done to combat these issues?
• FUNDING OF PUBLIC HEALTH CARE• Private healthcare vs. public healthcare
• APARTHEID SIDE EFFECTS• What are the lasting effects of apartheid on the South
African healthcare system• QUESTIONS

HIV/AIDS epidemic
POVERTY
FUNDING OF
PUBLIC HEALTH-
CARE
HEALTH CARE SYSTEM THAT
IS FAILING MOTHERS AND
CHILDREN

HIV/AIDS
epidemic
POVERTY
FUNDING OF
PUBLIC HEALTH-
CARE
HEALTH CARE SYSTEM THAT
IS FAILING MOTHERS AND
CHILDREN

MILLENNIUM DEVELOPMENT GOALS
•4. Reduce child mortality by two thirds by the year 2015•5. Improve maternal health and reduce maternal mortality

MATERNAL MORTALITY
• Currently is estimated between 230 and 702 per 100,000 live births (2010) – many home deaths may not be reported• South Africa’s maternal mortality rate has
INCREASED since the 1990’s largely due to HIV • 50% of maternal deaths are a result of HIV/AIDS• Many women receive insufficient care during
pregnancy• Unsafe birthing conditions

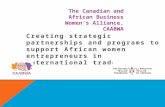
Fig. 2 Causes of maternal death in South Africa *88% indirect causes were non-pregnancy related infections (HIV/AIDS)
Fig. 1 Maternal mortality ratios (per 100,000), 1980-2008.

CARMMA
• Campaign for Accelerated Reduction of Maternal Mortality in Africa • Launched in May 2012 by Republic of South Africa• Aims to reduce infant and maternal mortality rates
throughout Africa• The MDG target is 38 deaths/100,000 by 2015• Plan to address inequality in underserved areas• Strengthen healthcare system• Follow MNCWH strategies

MNCWHSTRATEGIC PLAN FOR MATERNAL, NEWBORN, CHILD AND
WOMEN’S HEALTH AND NUTRITION IN SOUTH AFRICA
• Guidelines to decrease maternal mortality• Decrease infant mortality• Improve care for mother and child

ANTENATAL CARE
• About 90% of women receive some antenatal care (visit, supplements, etc.)
• Only 38% of women receive care within first 20 weeks of pregnancy
• BANC (Basic Antenatal Care approach) Doctors are trying to persuade women to receive 4 visits during pregnancy
• PMTCT (Prevention of Mother to Child Program)• Every women is tested for HIV during first weeks of pregnancy• If positive, given anti-retrovirals
• Stillborn rate is very high (19/1000) due to immaturity, low birth weight, hypoxia• This can be attributed to the health of the mother in some instances

AFTER THE BIRTH
• Intrapartum care • Can be improved by having stronger protocols for
detecting complications• Better access to Cesarian section• Monitoring during labor• Difficult because many hospitals are understaffed
• Postnatal care• Only 29.9% of babies and 27% of mothers were seen six
days after delivery• Visiting a doctor after delivery can decrease risk of
infection, help the mother, etc.• MNCWH recommends kangaroo care, breastfeeding, etc.

CHILDREN
• South Africa is one of only 5 countries in which the child mortality rate has increased between 1990 and 2008• Main problem: POVERTY• In 2009 61% of children lived in households that
were income poor• Under 1 mortality 41/1000• Under 5 mortality 57/1000• Neonatal mortality 14/1000 • Accounts for 1/3 of all deaths in children under 5

CONTRACEPTION
• 60% of women ages 15-49 use modern contraceptives• Above global average at 57%
• Still many unplanned pregnancies and contraction of STI/STD
• Problem: Risky behaviors• Improper use of contraception, unprotected sex• SADHS (South African Demographic and Health Survey)
indicated that 97% of sexually active women knew about contraceptives- ignorance is not the reason
• Abortion is legal and over 200,000 terminations are carried out annually- abortion is always an option for “contraception” for many women

HIV/AIDS epidemic
POVERTY
FUNDING OF
PUBLIC HEALTH-
CARE
HEALTH CARE SYSTEM THAT
IS FAILING MOTHERS
AND CHILDREN

FUNDING
• South African government spends 8.7% of GDP on health care- of this 60% goes to privately funded healthcare (14% of population)• Amounts to about 285 dollars/person- U.S. spends
4400 dollars/person (17.6% GDP) (WHO)

HOSPITALS
• Not enough money spent on healthcare to properly staff public hospitals, care for patients, etc.• Standard of care is not comparable to U.S. for
ordinary women and children• Human Rights Watch conducted a survey of 157
women in 2011- Stop Making Excuses• Women were mistreated on grounds of:• HIV/AIDS status• Whether or not they were a migrant• Inadequate conditions (supplies, nurses, doctors)• Poor communication between nurse and patient• Unaccountability by the hospital staff

• Women have complained of being verbally abused, physically abused, taunted, ignored-overall mistreated in public hospitals• Nurses sometimes lack the patience and skill to
adequately treat patients• The level of care is decreased, thus more
complications with the resulting child and delivery• The level of care simply does not meet the standards
that it should • Women hear horror stories about abuses and are
terrified to go to hospitals-SANGOMAS and traditional healers

STOP MAKING EXCUSES’: ACCOUNTABILITY FOR MATERNAL HEALTH CARE IN SOUTH AFRICA
Babalwa L. “The sister said I was lying about being in labor and sent me to the waiting area.” A doctor examined her three hours later, but it was too late. She delivered a stillborn baby. Neither the doctor nor the nurse explained what may have caused the stillbirth.”
Unnamed woman from the study “She was very rude and said I was lazy. After this experience I told myself I will never again go to government hospitals. If I have no money to go to a private hospital, I will deliver at home.”

HIV/AIDS epidemic
POVERTY
FUNDING OF
PUBLIC HEALTH-
CARE
HEALTH CARE SYSTEM THAT
IS FAILING MOTHERS
AND CHILDREN
EFFECTS OF
APARTHEID

HEALTHCARE HISTORY
• Reforms in the late 1990s changed how funds were distributed• Instead of Minister of Health allocating funds, Department of
Finance • Distributed funds base on the Treasury’s “Equitable Shares”
formula• Result: poor provinces have less spending autonomy based on
this policy and received LESS• Based on economic output, not need
• GEAR strategy (Growth, employment and redistribution)• Thabo Mbeki (1999)• Substantial increase in private healthcare sector

EFFECT OF APARTHEID
• Widening of the race boundaries• Access to health professionals and facilities was
poor• Unable to pay for service• Many Africans rely on public health care, where
as whites and Indians rely on the private sector• Poor education-many Africans turned to
sangomas and traditional healers

Poverty
Lack of education about modern
medicine/cannot access hospitals/care
More maternal and under 1/under 5
deaths- decline in the healthcare
system
CONCLUSION

REFERENCES• https://
www.mja.com.au/journal/2008/189/11/south-africa-21st-century-apartheid-health-and-health-care?0=ip_login_no_cache%3D32db43952441569a89fbfef7a38b56c6
• http://www.southafrica.info/about/health/health.htm#.UV4XgVegskJ• http://
www.doh.gov.za/docs/stratdocs/2012/MNCWHstratplan.pdf#page=15&zoom=auto,0,792
• http://www.unaids.org/en/resources/presscentre/featurestories/2012/may/20120508carmma/
• http://epianalysis.wordpress.com/2011/03/01/sainequality/• https://
www.mja.com.au/journal/2008/189/11/south-africa-21st-century-apartheid-health-and-health-care?0=ip_login_no_cache%3D32db43952441569a89fbfef7a38b56c6
• http://shr.aaas.org/loa/hback.htm• http://ajph.aphapublications.org/doi/abs/10.2105/AJPH.2009.184895?view=
long&pmid=21148716&
• http://www.sajog.org.za/index.php/SAJOG/article/view/504/280• http://www.hrw.org/news/2011/08/08/south-africa-failing-maternity-care