NURS 347 Towson University. Musculoskeletal Assessment Fundamentals:
Health Assessment - 1 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
University of Kerbala / College of Nursing
Adult Nursing Department
Health Assessment
Musculoskeletal Assessment
ANATOMY AND PHYSIOLOGY
The musculoskeletal system provides both support and mobility for the body
and protection for internal organs. This system also produces blood cells and stores
minerals such as calcium and phosphorus.
SKELETON: Functions of bones include support for soft tissues and organs,
protection of organs such as the brain and spinal cord, body movement, and
hematopoiesis. Bones are continually remodeling and changing the collagen and
mineral composition to accommodate stress placed on them. The function of each
bone dictates its shape and surface features. For example, long bones act as levers;
they have a flat surface for the attachment of muscles, with grooves at the end for
passage of tendons or nerves. Examples of long bones are the humerus, femur,
fibula, and phalanges. Short bones such as carpal and tarsal bones are cube
shaped. Flat bones make up the cranium, ribs, and scapula. The vertebrae are
irregularly shaped bones.
The human skeleton has two major divisions: the axial and appendicular skeletons.
The axial skeleton includes the facial bones, auditory ossicles, vertebrae, ribs,
sternum, and hyoid bone; the appendicular skeleton includes the scapula, clavicle,
bones of the shoulders and arms, and bones of the pelvis and legs. The subsequent
discussion of bones is organized by these divisions.
SKELETAL MUSCLES: Skeletal muscles are composed of muscle fibers that attach to
bones to facilitate movement. Although some skeletal muscles move by reflex, all
are controlled voluntarily. Skeletal muscle fibers are arranged parallel to the long
axis of bones to which they attach, or they are attached obliquely. Muscles attach
to a bone, ligament, tendon, or fascia.
JOINTS: Joints are articulations where two or more bones come together. They
help hold the bones firmly while allowing movement between them. Joints are
classified in two ways: by the type of material between them (fibrous,
cartilaginous, or synovial) and by their degree of movement. Immovable joints are
synarthrodial (e.g., the suture of the skull); slightly movable joints are
amphiarthrodial (e.g., the symphysis pubis); and freely movable joints are

Health Assessment - 2 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
diarthrodial (e.g., the knee and the distal interphalangeal [DIP] joint of the distal
fingers).
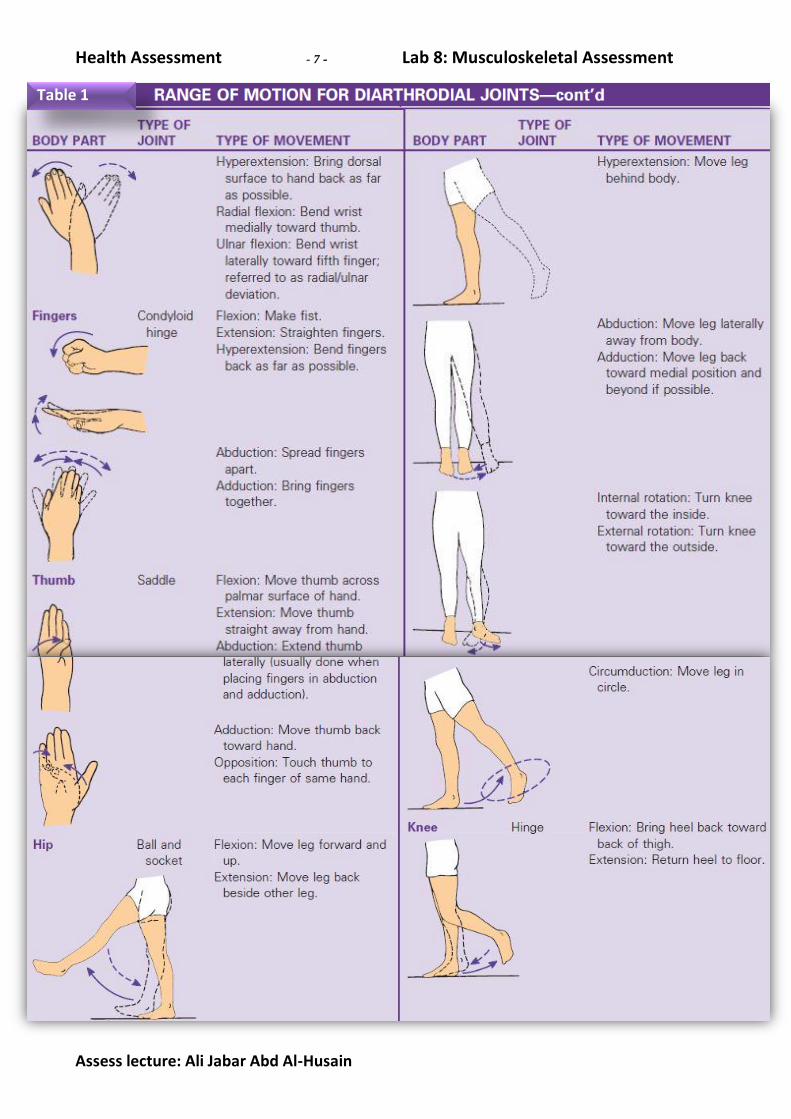
Diarthrodial joints are further classified by their type of movement. Only the
diarthrodial joints have one or more ranges of motion. "See (Table 1) for types of
movement of each diarthrodial joint". (1)Hinge joints (e.g., the knee, elbow, and
fingers) permit extension and flexion. Some hinge joints allow hyperextension;
however, there is variability among individuals, not all hinge joints are able to
hyperextend. (2)Pivot joints permit movement of one bone articulating with a ring
or notch of another bone such as the head of the radius, which articulates with the
radial notch of the ulna. The ends of saddle shaped bones articulate with one
another: the base of the thumb is the only example. (3)Condyloid or ellipsoidal
joints consist of the condyle of one bone that fits into the elliptically shaped
portion of its articulating bone (e.g., the distal end of the radius articulates with
three wrist bones). (4)Balland- socket joints are made of a ball-shaped bone that fits
into a concave area of its articulating bone (e.g., the head of the femur fits into the
acetabulum within the pelvis). (5)Gliding joints permit movement along various axes
through relatively flat articulating surfaces such as joints between two vertebrae.
Diarthrodial joints are synovial joints because they are lined with synovial fluid (Fig.
1). Synovial fluid lubricates the joint to facilitate its movement in various directions.
LIGAMENTS AND TENDONS: The difference between ligaments and tendons is
more functional than structural. Ligaments are strong, dense, flexible bands of
connective tissue that hold bones to bones (Fig. 2). They can provide support in
several ways: by encircling the joint, gripping it obliquely, or lying parallel to the
bone ends across the joint. They can simultaneously allow some movements while
restricting others.
Fig 2
Health Assessment - 3 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
Conversely, tendons are strong, non-elastic cords of collagen located at the ends of
muscles to attach them to bones (see Fig. 1). Tendons support bone movement in
response to skeletal muscle contractions, transmitting remarkable force at times
from the contracting muscles to the bone without sustaining injury themselves.
CARTILAGE AND BURSAE: Cartilage is a semi smooth, gel like supporting tissue that
is strong and able to support weight. The upper seven pairs of ribs are connected
directly to the sternum by costal cartilage. The flexibility of the cartilage allows the
thorax to move when the lungs expand and contract. Cartilage also reinforces
respiratory passages such as the nose, larynx, trachea, and bronchi. It forms a cap
over the ends of long bones, providing a smooth surface for articulation (see Fig. 1).
Because it contains no blood vessels, it receives nutrition from the synovial fluid
forced into it during movement and weight-bearing activities. For this reason,
weight-bearing activity and joint movement are essential to maintaining cartilage
health. Bursae are small sacs in the connective tissues adjacent to selected joints
such as the shoulders (the glenohumeral joint) and knees. Each bursa is lined with
synovial membrane containing synovial fluid, which acts as a lubricant to reduce
friction when a muscle or tendon rubs against another muscle, tendon, or bone
(see Fig. 1).
GENERAL HEALTH HISTORY
1- Present Health Status: 2- Past Health History: (medical & surgical) 3- Family History: 4- Personal and Psychosocial History:
Physical examination (Abdominal)
Begin examination as patient enters rooms, observing gait and posture. During examination, note ease of movement when patient walks, sits, rises, takes off garments, and responds to directions.
Physical Exam Normal finding Abnormal finding
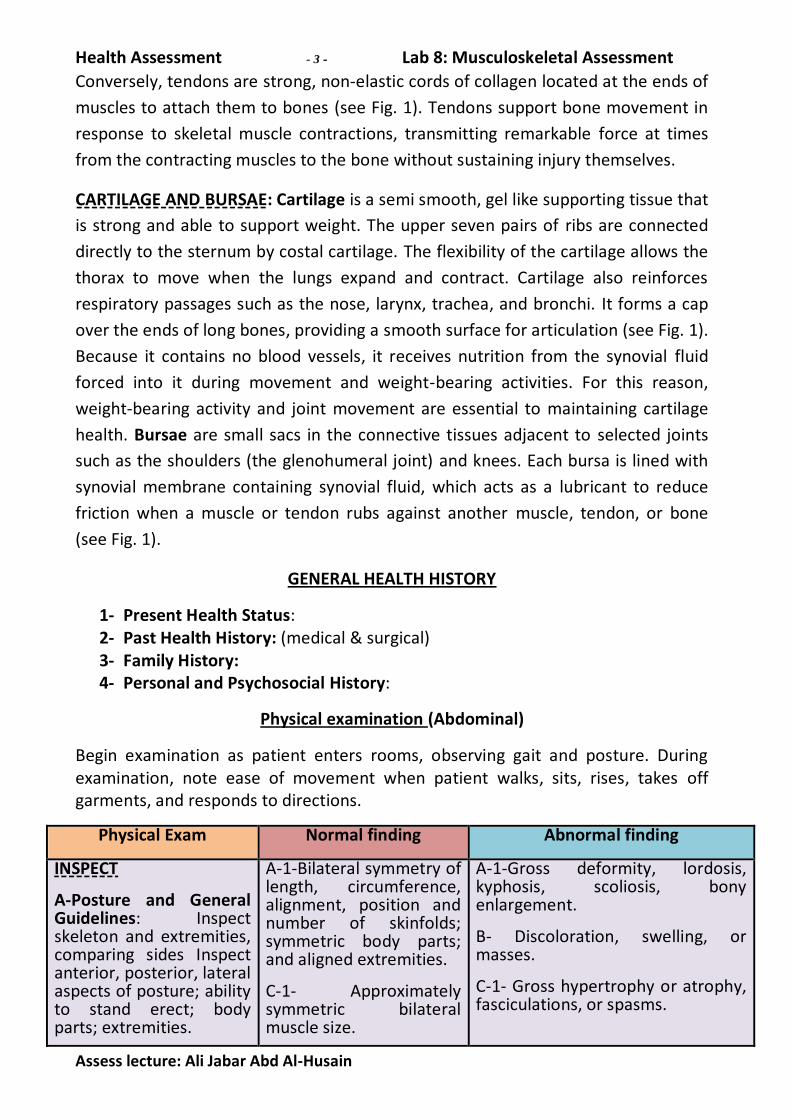
INSPECT
A-Posture and General Guidelines: Inspect skeleton and extremities, comparing sides Inspect anterior, posterior, lateral aspects of posture; ability to stand erect; body parts; extremities.
A-1-Bilateral symmetry of length, circumference, alignment, position and number of skinfolds; symmetric body parts; and aligned extremities.
C-1- Approximately symmetric bilateral muscle size.
A-1-Gross deformity, lordosis, kyphosis, scoliosis, bony enlargement.
B- Discoloration, swelling, or masses.
C-1- Gross hypertrophy or atrophy, fasciculations, or spasms.

Health Assessment - 4 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
1-Size, alignment, contour, symmetry: Measure extremities when lack of symmetry is noted in length or circumference.
B-Inspect skin and subcutaneous tissues over muscles, cartilage, bones, joints
C- Inspect muscles and compare sides
1- Size and symmetry:
A- Palpate: all bones, joints, surrounding muscles (palpate inflamed joints last)
1-Muscle tone.
2-Characteristics.
B-Test each major joint and related muscle groups for active and passive range of motion, and compare sides. Ask patient to move each joint through range of motion (see instructions for specific joints and muscles in individual sections that follow), then ask patient to relax as you passively move same joints until end of range is felt. Goniometer.
C-Test major muscle groups for strength, and compare contralateral sides For each muscle group, Ask patient to contract a muscle by flexing or extending a joint and to resist as you apply opposing force. Compare bilaterally.
A-1-Firm
B- Passive range of motion often exceeds active range of motion by 5 degrees. Range of motion with passive and active maneuvers should be equal between contralateral joints.
C- Bilaterally symmetric strength with full resistance to opposition.
D-1- Palmar and phalangeal creases, palmar surfaces with central depression with prominent, rounded mound on thumb side (thenar eminence) and less prominent hypothenar eminence on little-finger side.
A-1- Hard or doughy, spasticity.
A-2- Heat, tenderness, swelling, fluctuation of a joint, synovial thickening, crepitus, resistance to pressure, or discomfort to pressure on bones and joints.
B- Pain, limitation of motion, spastic movement, joint instability, deformity, contracture, discrepancies greater than 5 degrees between active and passive range of motion. When increase or limitation in range of motion is found, measure angles of greatest flexion and extension with goniometer, as shown in figure below, and compare with values as described for specific joints in individual extremities.
C- Inability to produce full resistance. Grade muscular strength according to the (Table2).
D-2- Deviation of fingers to ulnar side or inability to fully extend fingers; swan neck or boutonnière deformities.
D-3- Spindle-shaped fingers, bony overgrowths at phalangeal joints.
E- Nodules, swelling, bogginess,
Goniometer
Health Assessment - 5 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
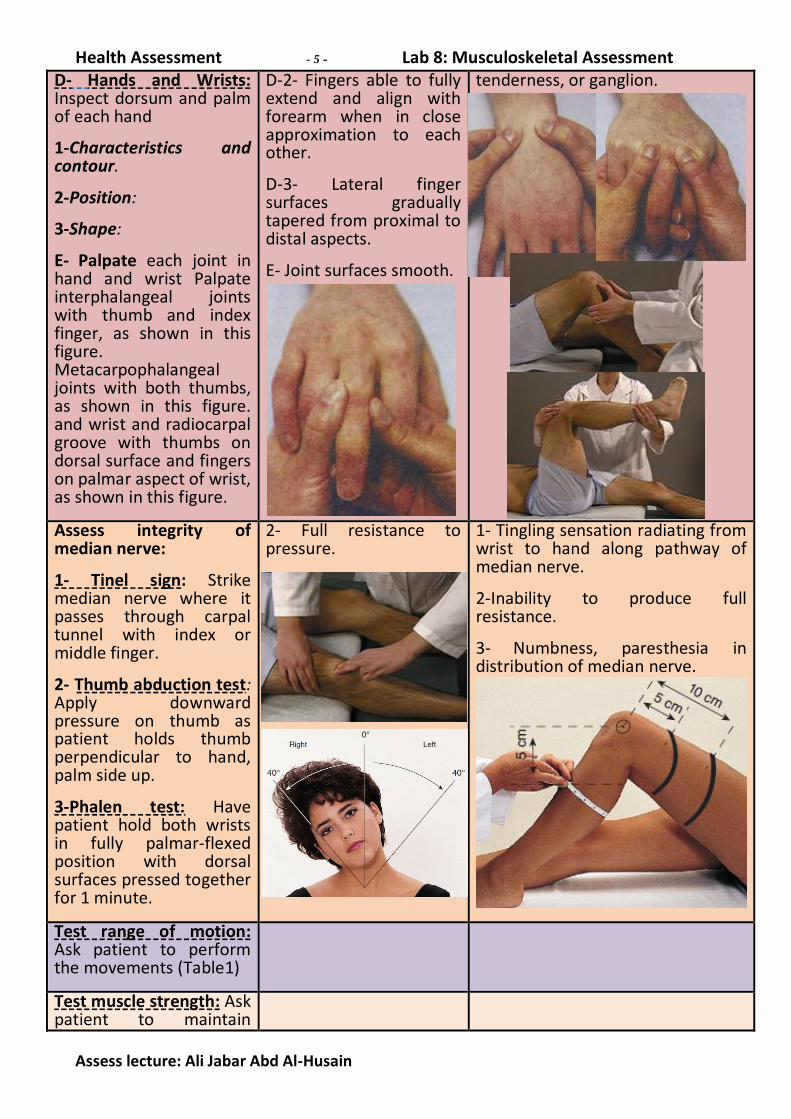
D- Hands and Wrists: Inspect dorsum and palm of each hand
1-Characteristics and contour.
2-Position:
3-Shape:
E- Palpate each joint in hand and wrist Palpate interphalangeal joints with thumb and index finger, as shown in this figure. Metacarpophalangeal joints with both thumbs, as shown in this figure. and wrist and radiocarpal groove with thumbs on dorsal surface and fingers on palmar aspect of wrist, as shown in this figure.
D-2- Fingers able to fully extend and align with forearm when in close approximation to each other.
D-3- Lateral finger surfaces gradually tapered from proximal to distal aspects.
E- Joint surfaces smooth.
tenderness, or ganglion.
Assess integrity of median nerve:
1- Tinel sign: Strike median nerve where it passes through carpal tunnel with index or middle finger.
2- Thumb abduction test: Apply downward pressure on thumb as patient holds thumb perpendicular to hand, palm side up.
3-Phalen test: Have patient hold both wrists in fully palmar-flexed position with dorsal surfaces pressed together for 1 minute.
2- Full resistance to pressure.
1- Tingling sensation radiating from wrist to hand along pathway of median nerve.
2-Inability to produce full resistance.
3- Numbness, paresthesia in distribution of median nerve.
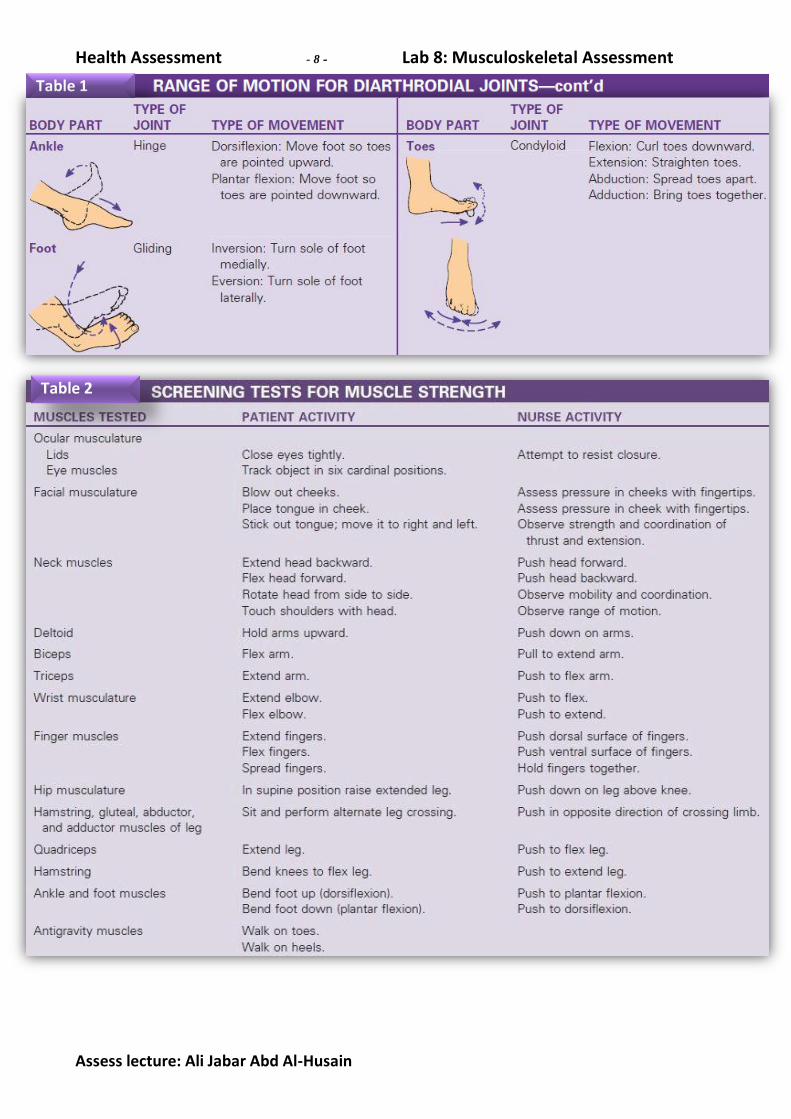
Test range of motion: Ask patient to perform the movements (Table1)
Test muscle strength: Ask patient to maintain

Health Assessment - 6 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
flexion and extension, while you apply opposing force see (Table 2). And to assess the grade of muscle strength function see (Table3).
Table 1
Health Assessment - 7 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
Table 1
Health Assessment - 8 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
Table 1
Table 2

Health Assessment - 9 - Lab 8: Musculoskeletal Assessment
Assess lecture: Ali Jabar Abd Al-Husain
Table 3