
HEALTH AND HEALTH CARE DISPARITIES SEMINOLE COUNTY MEDICAL SOCIETY MARILYN HUGHES GASTON, MD MAY 23,...
63
HEALTH AND HEALTH CARE DISPARITIES SEMINOLE COUNTY MEDICAL SOCIETY MARILYN HUGHES GASTON, MD MAY 23, 2006
-
date post
22-Dec-2015 -
Category
Documents
-
view
213 -
download
0
Transcript of HEALTH AND HEALTH CARE DISPARITIES SEMINOLE COUNTY MEDICAL SOCIETY MARILYN HUGHES GASTON, MD MAY 23,...

HEALTH AND HEALTH CARE DISPARITIES
SEMINOLE COUNTY MEDICAL SOCIETY
MARILYN HUGHES GASTON, MD
MAY 23, 2006

“NO AREA OF INJUSTICE AND SHAME IS AS GREAT
AS IN THE AREA OF HEALTH”
MARTIN LUTHER KING, JR.

U.S. HEALTH OUTCOMES
• LIFE EXPECTANCY – 19TH AND 25TH IN WORLD (1900 B/W DISPARITY 15 YEARS)
• PREMATURE & PREVENTABLE DEATHS• EPIDEMICS OF CHRONIC ILLNESS –
OBESITY AND DIABETES• DISPARITIES BETWEEN POOR & NON-
POOR, RACE / ETHNICITY, GENDER, GEOGRAPHY

HEALTH OUTCOMES (CONT)
• SOME IMPROVING – HEART DISEASE, CANCER, STROKE, SMOKING
• IMPROVEMENT IN SELF-CARE• OTHERS GETTING WORSE – ASTHMA,
DIABETES, MENTAL HEALTH (STRESS, DEPRESSION), OBESITY
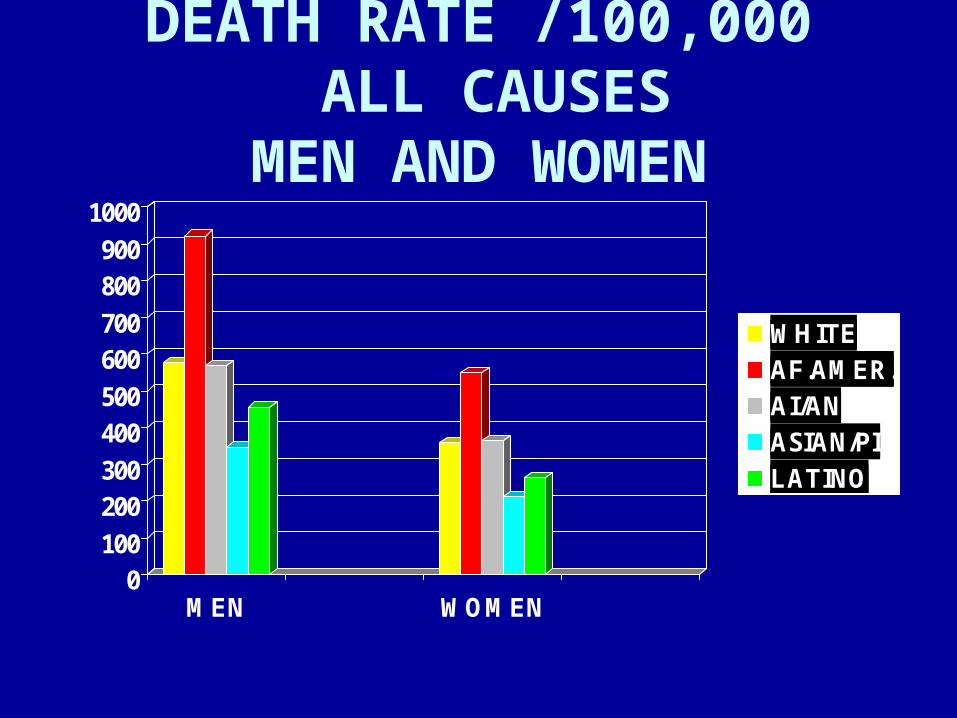
DEATH RATE /100,000 ALL CAUSES
MEN AND WOMEN
0100
200300
400500
600700
800900
1000
MEN WOMEN
WHITEAF.AMER.AI/ANASIAN/PILATINO

AGE ADJUSTED DEATHS/100,000
WOMEN
0
20
40
60
80
100
120
140
160
HEART CANCER STROKE
WHITEAF.AMER.AI/ANASIAN/PILATINO

AGE ADJUSTED DEATHS/100,000
MEN
0
50
100
150
200
250
HEART CANCER STROKE
WHITEAF.AMER.AI/ANASIAN/PILATINO
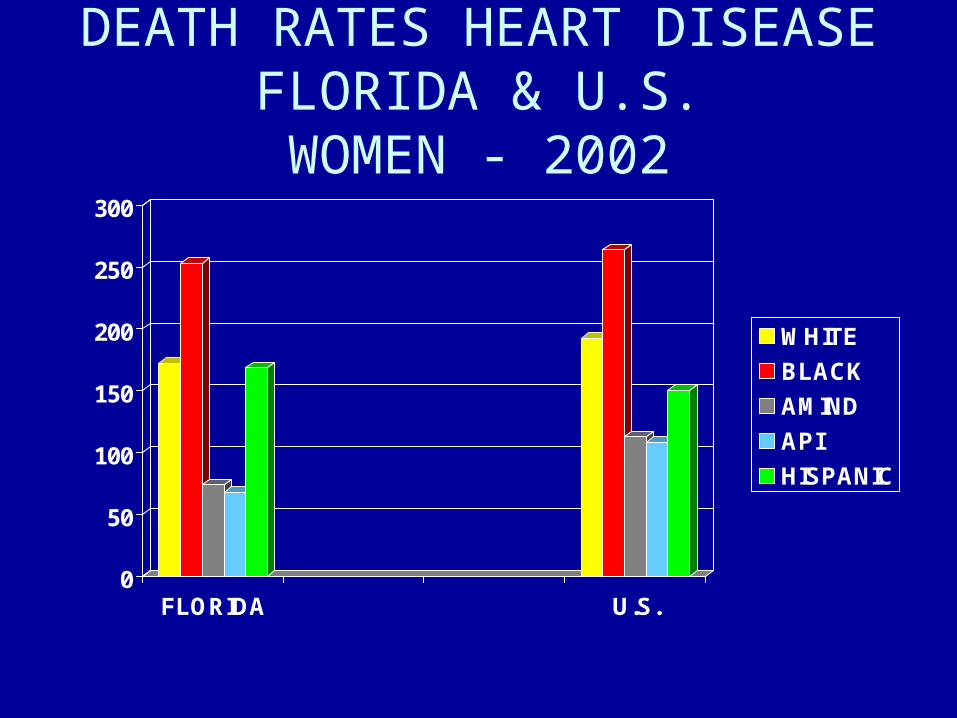
DEATH RATES HEART DISEASEFLORIDA & U.S.WOMEN - 2002
0
50
100
150
200
250
300
FLORIDA U.S.
WHITE
BLACK
AMIND
API
HISPANIC

DEATH RATE HEART DISEASEFLORIDA & US
MEN - 2002
0
50
100
150
200
250
300
350
400
FLORIDA US
WHITE
AF AM
AMIND
API
HISPANIC

CANCER DEATHS/100,000BY RACE/ETHNICITY
0
5
10
15
20
25
30
35
40
45
LUNG COLOREC PROST. BREAST
WHITEAF.AMER.AI/ANASIAN/APLATINO

Source: Mokdad et al., Diabetes Care 2000;23:1278-83.
Diabetes Trends* Among Adults in the U.S.,
(Includes Gestational Diabetes) BRFSS 1990

Diabetes Trends* Among Adults in the U.S.,
(Includes Gestational Diabetes) BRFSS 1993-94
Source: Mokdad et al., Diabetes Care 2000;23:1278-83.

DNPA Graphics:
DNPA Graphics:DNPA
Graphics:
DNPA Graphics:
Diabetes Trends* Among Adults in the U.S.,
(Includes Gestational Diabetes) BRFSS 1999
Source: Mokdad et al., Diabetes Care 2001;24:412.

DNPA Graphics:
DNPA Graphics:DNPA
Graphics:
DNPA Graphics:
Diabetes Trends* Among Adults in the U.S.,
(Includes Gestational Diabetes) BRFSS 2001
Source: Mokdad et al., J Am Med Assoc 2001;286:10.
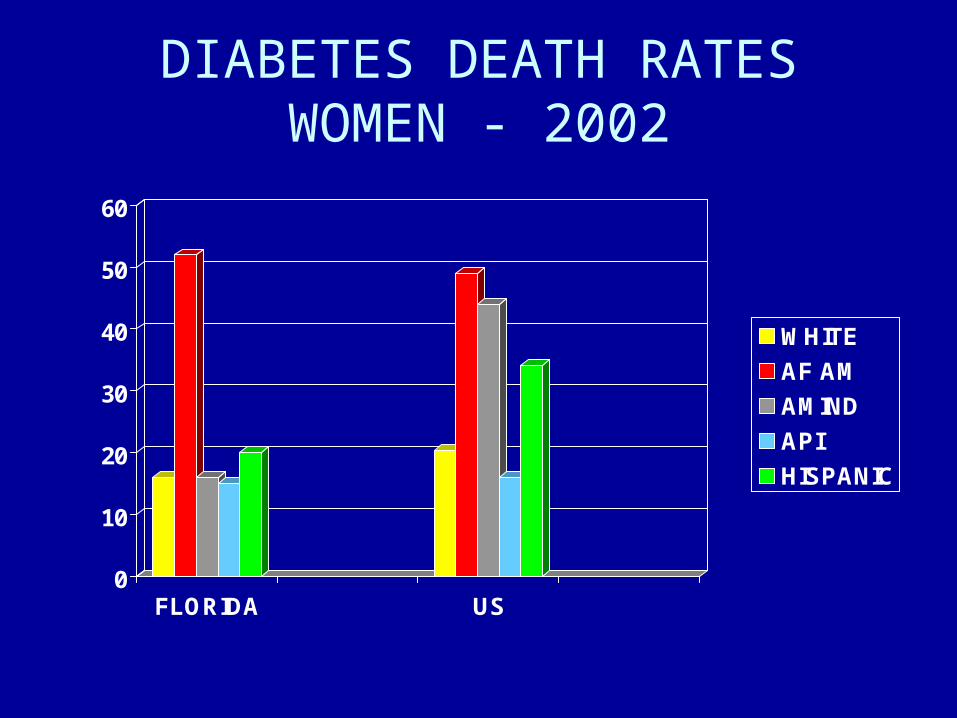
DIABETES DEATH RATESWOMEN - 2002
0
10
20
30
40
50
60
FLORIDA US
WHITE
AF AM
AMIND
API
HISPANIC

DIABETES DEATH RATESMEN - 2002
0
5
10
15
20
25
30
35
40
45
50
FLORIDA US 4th Qtr
WHITE
AF AM
AMIND
API
HISPANIC

Negative Mood by Gender and RaceNegative Mood by Gender and Race
CaucasianMen5.8
CaucasianWomen
8.1
AfricanAmerican
Men10.9
AfricanAmericanWomen
16.4

FACTORS INFLUENCING THESE OUTCOMES
POPULATION LEVEL:
• BARRIERS TO ACCESS TO CARE• BROKEN HEALTH CARE SYSTEM QUALITY - UNEQUAL TREATMENT• SOCIOECONOMIC/ CULTURAL AND
LANGUAGE ASPECTS

FACTORS INFLUENCING THESE OUTCOMES (CONT)
INDIVIDUAL LEVEL:
• LIFESTYLE• GENETICS• EDUCATIONAL• LOW HEALTH LITERACY• ATTITUDINAL

ACCESS
• TO QUALITY CARE FOR EVERYONE
• TO AFFORDABLE MEDICATIONS
• TO MEDICAL INFORMATION

• FINANCIAL• GEOGRAPHIC/CAPACITY• CULTURAL/LINGUISTIC• ATTITUDINAL• EDUCATIONAL – HEALTH
LITERACY• VULNERABLE POPULATIONS• SYSTEMS OF CARE
Barriers to CareBarriers to Care

FINANCIAL BARRIERS
• POVERTY
• UNINSURED – 45 MILLION
FOR ENTIRE YEAR
• 70 MILLION UNINSURED FOR PART OF YEAR
• UNDERINSURED – MILLIONS
• 5TH LEADING CAUSE OF DEATH(IOM)

No Physician ContactIn Past Year With a ProblemNo Physician ContactIn Past Year With a Problem
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Poor Middle High
Hispanic
African/American
White

%TOTAL UNINSURED 2004
0
5
10
15
20
25
30
35
40
45
FLORIDA US
WHITE
AF AM
HISPANIC

Uninsured and MinoritiesUninsured and Minorities
Hispanics35%
African/Americans25%
Asian20%
White12%

Percent of US Under Age 65 Who Say in Past 12 Months They Have . . .Percent of US Under Age 65 Who Say in Past 12 Months They Have . . .
0
10
20
30
40
50
60
70
80
RoutinePhysical Exam
Pap Smear Mammogram ProstateExam
Source: Kaiser Family Foundation National Survey on the Uninsured, April 2000
70 76 40 2047 49 16 12
Insured
Uninsured

INSURANCE & STAGE OF DISEASE AT DIAGNOSIS OF BREAST CANCER
0
5
10
15
20
25
30
35
40
45
I II A II B III IV
UNINSUREDINSURED

Physicians who treat Medicaid or Uninsured PatientsPhysicians who treat Medicaid or Uninsured Patients
Hispanics33%
African/Americans48%
Asian34%
White24%

NATL. HEALTHCARE DISPARITIES REPORT
• ACCESS MEASURES - 31
• AA – WORSE ON 40%
• LATINOS – WORSE 90%
• AIAN – 50%
• API – 30%
• POOR PEOPLE – 80%

Health Professional ShortagesHealth Professional Shortages
0
500
1000
1500
2000
2500
3000
1990 1992 1994 1996 1998 2000
Rural
Urban

BROKEN HEALTH CARE SYSTEM
• NON-SYSTEM – NOT COORDINATED, IS FRAGMENTED
• QUALITY OF CARE NEEDS IMPROVING
• DISCRIMINATION, BIAS, PREJUDICE
• FOCUSED ON TREATMENT – NOT
PREVENTION
• TOO FEW MINORITY PROVIDERS

How We Have to Change Our Health Care System!How We Have to Change Our Health Care System!
Tertiary Care
SecondaryCare
PrimaryCare
Tertiary Care
SecondaryCare
PrimaryCare
100%/0 is the movement where communities are flipping the pyramid!
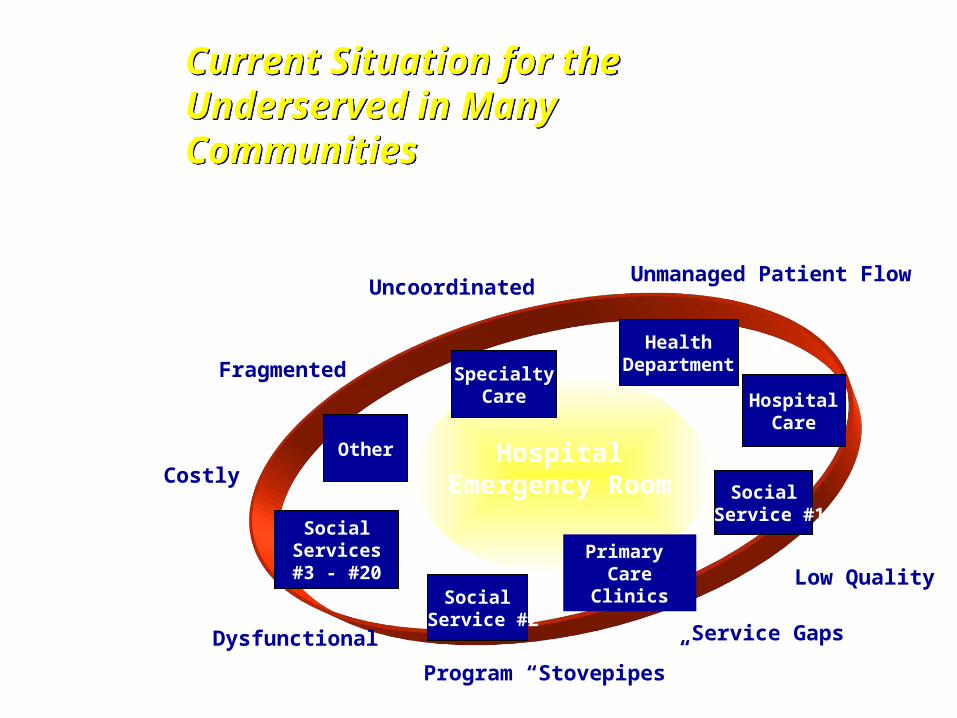
HospitalEmergency Room
SpecialtyCare
Social Service #1
Primary Care Clinics
Other
Social Service #2
Social Services #3 - #20
HospitalCare
Unmanaged Patient Flow Uncoordinated
Low Quality
Service Gaps Dysfunctional
Fragmented
Costly
Emergency Room At the Center of the “System”
Program “Stovepipes”
HealthDepartment
Current Situation for the Underserved in Many Communities
Current Situation for the Underserved in Many Communities

QUALITY OF CARE
• INSTITUTE OF MEDICINE (IOM) REPORT –CROSSING THE QUALITY CHASM
• WORLD HEALTH ORGANIZATION (WHO) REPORT
• PATIENT SATISFACTION NOT GOOD• “UNEQUAL TREATMENT”

UNEQUAL TREATMENT
• IOM REPORT• DISPARITIES IN HEALTH CARE PRESENT
AND UNQUESTIONED• WITH ELIMINATION OF SES DIFFERENCES
AND ACCESS DISPARITIES STILL REMAIN• EVIDENCE OF BIAS, PREJUDICE AND
DECISIONS INFLUENCED BY PATIENTS’ RACE AND ETHNICITY.

QUALITY OF CARE (CONT)
• INFORMATION EXPLOSION
• EXPLOSION IN NEW CLINICAL TECHNOLOGIES
• INCREASING CONSUMER DEMAND AND INCREASING LITIGATION
• INCREASING DATA WITHOUT EXPLOSION IN INFORMATION TECHNOLOGY

The Institute of MedicineThe Institute of Medicine
“Between the health care we have and the care we could have lies not just a gap,
but a chasm.” To fill that chasm requires we work together to
“redesign health care processes”
Crossing the Quality Chasm, A New Health System for the 21st CenturyIOM March, 2001
Care Should Be:
• Safe• Effective• Patient-Centered• Timely• Efficient• Equitable
The Institute of MedicineCrossing the Quality Chasm
The Institute of MedicineCrossing the Quality Chasm

NATL. HEALTH CARE DISPARITIES REPORT
• QUALITY MEASURES – 38
• AA – POORER QUALITY 66%
• LATINOS – 50%
• AIAN – 30%
• ASIANS – 10%
• POOR PEOPLE – 60%

SOLUTIONS

Primary Care Centered Community Health System: Primary Care Centered Community Health System:
Hospital
SpecialtyCare
Social Services
Primary Primary Care and PreventionCare and Prevention
IntegrativeReferralSystem
Other
Case Management of Chronic Conditions
Insurance Partnerships
Medical Homes
Disease Management
Disparity Elimination Campaigns
“Share The Savings” Plans
Organized Pharmacy
Common Sliding Fee Scales
Outreach & Common Enrollment
Automated Appointment Systems
Guiding Coalition, Collaborative
Patients in Primary Care Medical Homes
Specialty Referralfor Uninsured

InformationSystems
Guiding Coalition
100% Access System
TranslationOutreach
EnrollmentTransportation
Health Education
HospitalServicesCore Services
• preventive• primary care• oral health• lab & x-ray• pharmacy• primary mental health
SpecialtyCare
Mental Health
CommunitySocial Services
Clinics
NHSCHospitals
AHEC Universities
VoluntaryHealth
Association
LocalGovernment
School-basedPrograms
Maternal & ChildHealth Programs
Faith-basedPrograms
Public HealthDepartment
CommunityDevelopmentPartnerships
Comprehensive Primary Care and Prevention
Veterans Administration
Ryan WhitePrograms
Health CentersFQHC
SubstanceAbuse
Case-Managed,Integrative
ReferralSystem
Complementaryand Alternative
Therapies
EnvironmentalHealth
Medical Society
Foundations
Unions
Primary Care Centered Community Health SystemPrimary Care Centered Community Health System

Galveston, Texas Primary CareCentered Health SystemGalveston, Texas Primary CareCentered Health System
Galveston’s 100% Access System
Comprehensive Primary Care and Prevention
St. Vincent’s Episcopal House & Clinic
SocialServices
ReligiousMinistries
MedicalServices St. Agustine of Hippa Episcopal
Moody Memorial Methodist First Presbyterian St. Patrick Catholic Holy Rosary Shilo AME Temple B’nai Israel University Baptist Trinity EpiscopalUnitarian Universalist Fellowship
TX Dept. HumanServices
Salvation Army
Catholic Charities
Community Action Council
University of Texas Medical Branch
Galveston CountyHealth District
Case-Managed, Integrative Referral SystemTranslation
Outreach
Enrollment
Transportation
Health Education
Core Services
•Preventive•Primary care•Dental•Lab & Radiology•Pharmacy•Primary Mental Health
Complementaryand Alternative
Therapies
Hospital
Services
Specialty
Care
Substance
AbuseMental
HealthSCAN
Southeast CostalArea Network
InformationSystems
GuidingCoalition
CommunityDevelopmentPartnerships
Employment-Gulf Coast Career Ctr
Areas Health Education Centers
Universities
Medical Society
VeteransAdministration
EnvironmentalHealth
Businesses
FreeClinics
Voluntary HealthAssociation
Local Government
School-based Programs
Legal – Gulf Coast Legal Foundation
Accessibility/Disability Services
National Health Service Corps
Federally QualifiedHealth Centers
Hospital
Nutrition Services
Public HealthDepartment
Foundations
Federal EntitlementPrograms
EmpowermentZones/EnterpriseCommunities
Faith-based Programs
Senior Citizens Programs
Maternal & Child Health Programs
Ryan White Programs ACCT- The AIDS coalition of Coastal TX Children's Health Insurance Program CHIP
Jesse Tree
Immunization CoalitionMainland Medical Center
Galveston County Social Services
4Cs Health Center

Better Health
for More People
for Less Cost
Better Health
for More People
for Less Cost

Models: Community Health CentersModels: Community Health Centers
• Community-owned boards• Address all barriers• 85% Poor and near-poor• 70% Minority• 41% Uninsured• 33% Medicaid

Unmet Healthcare Needs Among Uninsured PersonsUnmet Healthcare Needs Among Uninsured Persons
0
10
20
30
40
50
60
Did not get medical care
Delayed seeking care due to cost
Did not fill prescription
Sources: Kaiser Family Foundation/Commonwealth Fund, National Survey of Health Insurance
U.S. Uninsured
CHC Uninsured
Health center uninsured patients report unmet needs at half the National rates.
30 55 2416 25 12
Percent

Health Promotion TopicsHealth Promotion Topics
0
10
20
30
40
50
60
70
80
Diet Activity Smoking Alcohol Drugs SDTDs
Source: Health Center User Survey; NHIS 1995
Uninsured Adults
54 43 57 49 75 64 68 53 55 39 54 36
CHC
U.S.

Prevention – Woman Receiving MammogramsPrevention – Woman Receiving Mammograms
0 20 40 60 80
All women
<100 Poverty
100-200 Poverty
African American
Hispanic
White
Source: Health Center User Survey, NHIS and HP 2010 Contact: Bob Politzer, ScDEmail: [email protected]
62.2 %
59.7 %
61.6 %
76.7 %
58.4 %
44.5 %
40.2 %
46.7 %
49.6 %
48 %
44.5 %
63 %
2010 ObjectiveHealthy People
Health Centers Comparison Group

Significantly Lower Odds of Being Hospitalized For An Ambulatory Care Sensitive Condition
Medicaid Health Center Users . . .Medicaid Health Center Users . . .
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Source: Falik et al. ACSC Hospitalization and ER visits; 2001
Medicaid CHC Users
Medicaid Non-CHC Users
.78
1
Od
ds
Rat
io

Using Health Centers are Three Times as Likely to ReportBlood Pressure Under Control as NHIS Comparison Group
African American & Hispanic HypertensivesAfrican American & Hispanic Hypertensives
0
0.5
1
1.5
2
2.5
3
3.5
Source: NHIS & CHC User Survey, 1995 Method: Personal interviews with representative sample of health center users; comparison group from NHIS respondents w/ similar income who had at least 1 physician visit
Medicaid CHC Users
Medicaid Non-CHC Users
3.3
1
Od
ds
Rat
io

Source: C Hupke, IHI, [email protected]
7.5
8
8.5
9
9.5
10
Ap
r-99
May
-99
Jun
-99
Jul-
99
Au
g-9
9
Sep
-99
Oct
-99
No
v-99
Dec
-99
Jan
-00
Feb
-00
Mar
-00
Ap
r-00
May
-00
Jun
-00
Jul-
00
Au
g-0
0
Sep
-00
Oct
-00
No
v-00
Dec
-00
Jan
-01
Feb
-01
Mar
-01
Ap
r-01
May
-01
Jun
-01
Jul-
01
Ave
rag
eAverage HbA1c for Health Centersin (Southeast Cluster), 1999-2001
Average HbA1c for Health Centersin (Southeast Cluster), 1999-2001
Month

Sources: Uniform Data System, BPHC/HRSA 1998; Health, United States, 1998, NCHS/CDC, 1998 (1996 data).
Reducing Low Birth Weight RatesReducing Low Birth Weight Rates
All HC Infants
All U.S. Infants
African American HC Infants
African American U.S. Infants
7.1 %
7.1 %
13 %
9.9 %

BLACK/WHITE DEATH RATE BY HC PENETRATION
0
50
100
150
200
250
300
<10% 10-20% >20%

Eliminating Early Breast Cancer Detection DisparitiesEliminating Early Breast Cancer Detection Disparities
Contra Costa County, California
Percent ofBreastCancer
Detected at Stage 1
0
44
72
100
73
58
71 %70 %
77 %Asian/PI
Caucasian
Latina
African American
SolutionsSolutions
• System level change• Address barriers• Community involvement• Training – Cultural competence – Increase
minorities• Improve Quality• Replicate Models

QUALITY SOLUTIONS
• TRANSFORM PRACTICES-CHRONIC DISEASE MANAGEMENT
• INCREASE CULTURAL & LINGUISTIC SKILLS• ENHANCE PATIENT-PROVIDER
COMMUNICATION-HEALTH LITERACY• INCREASING PATIENT EDUCATION AND
SELF-CARE• MONITOR BIAS & DISCRIMINATION• INCREASE TRUST

1 2 3 6 754
5ccs
Which is a teaspoon?
/

1 2 3 6 754
5ccs
ccs. 5 8 4 4.5 5 3.7 4.3

QUALITY SOLUTIONS (CONT)
• EFFECTIVE EVIDENCE BASED INTERVENTIONS
• FOCUS MORE ON PREVENTION• INCREASE COMMUNITY INPUT• INCREASE MINORITY PROVIDERS• MAKE CARE MORE HOLISTIC (MIND,
BODY, & SPIRIT)• INTEGRATE MENTAL HEALTH
SERVICES

IOM CLOSING THE GAP REPORTS
• Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care 2002
• Speaking of Health: Assessing Health Communication Strategies for Diverse Populations 2003
• Emerging Issues in Hispanic Health 2002• The Right Thing to Do, The Smart Thing to Do:
Enhancing Diversity in Health Professions 2001• Coverage Matters: Insurance and Health- 5 Vol.• America’s Health Care Safety Net:Intact But
Endangered 2001


DIFFERENCES IN RISK FACTORS
0%
10%
20%
30%
40%
50%
60%
SMOKER INACTIVE OBESE
AAWHITE HIS/LATAIANAAPI



















