
Headache Very common; Very common; Sensitive people; highly competitive; perfectionistic; Sensitive...
72
Headache Headache Very common; Very common; Sensitive people; highly competitive; Sensitive people; highly competitive; perfectionistic; perfectionistic; rigid control in dealing with life situatn rigid control in dealing with life situatn over respond to stress producing situations; over respond to stress producing situations; difficulty in adjusting to stress of life difficulty in adjusting to stress of life probably the most common human complaint probably the most common human complaint - - most prevalent neurologic symptom associated with any dx most prevalent neurologic symptom associated with any dx
-
Upload
oswaldo-banister -
Category
Documents
-
view
238 -
download
1
Transcript of Headache Very common; Very common; Sensitive people; highly competitive; perfectionistic; Sensitive...

HeadacheHeadache Very common;Very common;
Sensitive people; highly competitive; Sensitive people; highly competitive; perfectionistic; perfectionistic;
rigid control in dealing with life situatnrigid control in dealing with life situatn
over respond to stress producing situations;over respond to stress producing situations;
difficulty in adjusting to stress of lifedifficulty in adjusting to stress of life probably the most common human complaintprobably the most common human complaint- -
most prevalent neurologic symptom associated with any dxmost prevalent neurologic symptom associated with any dx

HeadacheHeadache
DEFINITIONDEFINITION
CLASSIFICATION AND CAUSESCLASSIFICATION AND CAUSES
PATHO PHYSIOLOGYPATHO PHYSIOLOGY
INVESTIGATIONS INVESTIGATIONS MANAGEMENT MANAGEMENT

DefinitionDefinition
Head ache / PainHead ache / Pain
cephalalgiacephalalgia

CLASSIFICATION CLASSIFICATION
Diagnosis Diagnosis good clinical managementgood clinical management Research Research epidemiologic studies epidemiologic studies clinical trialsclinical trials
IHS classification in 1988IHS classification in 1988
Revised in 2004 (ICHD-2)Revised in 2004 (ICHD-2) On-going revision..On-going revision..
44

55
The International Classification of The International Classification of Headache Disorders - IIHeadache Disorders - II
Part one: The primary headachesPart one: The primary headaches
Part two: The secondary headachesPart two: The secondary headaches
Part three: Cranial neuralgias, central Part three: Cranial neuralgias, central and primary facial pain, and other and primary facial pain, and other headachesheadaches

66
The primary The primary headachesheadaches
1.1. MigraineMigraine
2.2. Tension-type headache (TTH)Tension-type headache (TTH)
3.3. Cluster headache and other Cluster headache and other trigeminal autonomic cephalalgiastrigeminal autonomic cephalalgias
4.4. Other primary headachesOther primary headaches

77
The secondary The secondary headachesheadaches
5.5. Headache attributed to head and/or neck traumaHeadache attributed to head and/or neck trauma
6.6. Headache attributed to cranial or cervical vascular Headache attributed to cranial or cervical vascular disorderdisorder
7.7. Headache attributed to non-vascular intracranial Headache attributed to non-vascular intracranial disorderdisorder
8.8. Headache attributed to a substance or its withdrawalHeadache attributed to a substance or its withdrawal
9.9. Headache attributed to infectionHeadache attributed to infection
10.10. Headache attributed to disorder of homoeostasisHeadache attributed to disorder of homoeostasis
11.11. Headache or facial pain attributed to disorder of Headache or facial pain attributed to disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranial structuresmouth, or other facial or cranial structures
12.12. Headache attributed to psychiatric disorderHeadache attributed to psychiatric disorder

88
Cranial neuralgias, central and Cranial neuralgias, central and primary facial pain, and other primary facial pain, and other headachesheadaches
13.13.Cranial neuralgias and central Cranial neuralgias and central causes of facial paincauses of facial pain
14.14.Other headache, cranial neuralgia, Other headache, cranial neuralgia, central or primary facial paincentral or primary facial pain

99
4. Other primary 4. Other primary headachesheadaches4.1 Primary stabbing headache4.1 Primary stabbing headache4.2 Primary cough headache4.2 Primary cough headache4.3 Primary exertional headache4.3 Primary exertional headache4.4 Primary headache associated with sexual activity4.4 Primary headache associated with sexual activity
4.4.1 Preorgasmic headache4.4.1 Preorgasmic headache4.4.2 Orgasmic headache4.4.2 Orgasmic headache
4.5 Hypnic headache4.5 Hypnic headache4.6 Primary thunderclap headache4.6 Primary thunderclap headache4.7 Hemicrania continua4.7 Hemicrania continua4.8 New daily-persistent headache4.8 New daily-persistent headache

ClassificationClassification
Headache classification committee of Headache classification committee of
I.H.S. I.H.S. (International Headache society) (International Headache society)
19881988
MIGRAINE HEADACHE MIGRAINE HEADACHE
TENSION HEADACHETENSION HEADACHE
CLUSTER (M. Neuralgia) SYNDROME CLUSTER (M. Neuralgia) SYNDROME

Headache Headache ClassificationClassification H. assoc with non-haemorrhagic arterial / arteriolar disorder. H. assoc with non-haemorrhagic arterial / arteriolar disorder.
Temporal/Giant arteritis) Temporal/Giant arteritis)
H. assoc with abuse/withdrawal of substancesH. assoc with abuse/withdrawal of substances .. > 45g Aspirin; 300mg of valium monthly; Alcohol > 45g Aspirin; 300mg of valium monthly; Alcohol
H. assoc with systemic infection or focal infection outside Head H. assoc with systemic infection or focal infection outside Head
H. assoc with metabolic abnormality H. assoc with metabolic abnormality
H or facial pain from cranium; eye; ENT. H or facial pain from cranium; eye; ENT.
CRANIAL NEURALGIA & Other types of Headache. CRANIAL NEURALGIA & Other types of Headache. Post traumatic ; S.O.L; H in depression .Post traumatic ; S.O.L; H in depression . Referred pain ; Benign coital headache.Referred pain ; Benign coital headache. Cervico-genic H ;Cervico-genic H ; Traction H; Cough H.Traction H; Cough H. Post-lumbar puncture H. (starts > 48hrs; worse on standing upPost-lumbar puncture H. (starts > 48hrs; worse on standing up

MigraineMigraine
10% adult; > in females;10% adult; > in females; autosomal dominant + incomplete penetranceautosomal dominant + incomplete penetrance
defn: episodic disorder manifest. by H.defn: episodic disorder manifest. by H. accompanied by anorexia; N&V; photo / phonophobia.accompanied by anorexia; N&V; photo / phonophobia. lasts 4-72 hrs; < 2 ce a week. lasts 4-72 hrs; < 2 ce a week.
ATTRIBUTES TO ESTABLISH DiagnosisATTRIBUTES TO ESTABLISH Diagnosis
≥ ≥ 2 of the ff 2 of the ff .. Unilateral locationUnilateral location .. Pulsatile qualityPulsatile quality .. Moderate to severe intensityModerate to severe intensity .. exacerbation by physical activityexacerbation by physical activity
> 1 of ff must accompany > 1 of ff must accompany . N/V; Photo / phonophobia. N/V; Photo / phonophobia

Subdivisions of M.HSubdivisions of M.H(modified by OLSER & GOADSBY 1996)(modified by OLSER & GOADSBY 1996)
M with AURA 10% [CLASSIC M]M with AURA 10% [CLASSIC M]M without AURA 85% [COMMON] M without AURA 85% [COMMON] M with prolonged unilateral M with prolonged unilateral sensory/motor deficitsensory/motor deficitFamilial Hemiplegic M. 60% family hx. Familial Hemiplegic M. 60% family hx. Opthalmoplegic M. (?Post comm-artery). Opthalmoplegic M. (?Post comm-artery). BASILAR M BASILAR M [aura:vertigo;dysarthria/tinnitus/diplopia/ataxia [aura:vertigo;dysarthria/tinnitus/diplopia/ataxia M. Equivalents (acephalic M) : No Headache / M. Equivalents (acephalic M) : No Headache / No vomiting No vomiting ABDOMINAL M./episodic transient disturbance ABDOMINAL M./episodic transient disturbance CARDIAC M. responds to prophylatic treatment for CARDIAC M. responds to prophylatic treatment for
M. M.

AuraAura
Consists of well defined transient focal Consists of well defined transient focal neurologic dysfunction in clear consciousness neurologic dysfunction in clear consciousness
devs over the course of > 4 mins & lasts < devs over the course of > 4 mins & lasts < hr. hr.
Visual disorder Visual disorder see stripes/spots/lines; fortification see stripes/spots/lines; fortification
spectra/scotoma spectra/scotoma unilateral paraesthesia / numbness unilateral paraesthesia / numbness Unilateral weakness Unilateral weakness Aphasia or other speech disorder Aphasia or other speech disorder
precede /appear or recur at height of H . precede /appear or recur at height of H .

Prodromal symptomsProdromal symptoms
.. Begins insidiously Begins insidiously Lasts several hours Lasts several hours days days
characteristically involves characteristically involves
Changes in mood / behaviour ; cognitive Changes in mood / behaviour ; cognitive disturbance ; fatigue ; depression; elation; disturbance ; fatigue ; depression; elation; insomnia; somnolence ; hunger ; thirst ; oliguria ; insomnia; somnolence ; hunger ; thirst ; oliguria ; altered libido ; > urinary frequency.altered libido ; > urinary frequency.
Depression + lassitude Depression + lassitude most common most common
Feeling of well being; augmented energy and Feeling of well being; augmented energy and clarity of thought ; > appetite especially for clarity of thought ; > appetite especially for sweet.sweet.

Tension HeadacheTension Headache(Muscle Tension H)(Muscle Tension H)
HATBAND distribution;HATBAND distribution; pp ; tightness sensation of wearing tight cap, pp ; tightness sensation of wearing tight cap,
pressing;pressing; non pulsatile ; non pulsatile ; bilateral bilateral Tender spots / in neck scalp - accentuate HTender spots / in neck scalp - accentuate H
worse in the evening. worse in the evening. Not worsen with routine physical activityNot worsen with routine physical activity Not prevent sleepNot prevent sleep Does not awaken patient Does not awaken patient No nausea / vomiting No nausea / vomiting Photphobia / Sonophobia may be presentPhotphobia / Sonophobia may be present H > 2 ce/wk H > 2 ce/wk T.H. not migraine T.H. not migraine Episodic T.H. / Episodic T.H. / Chronic T.H.Chronic T.H.

Cluster HeadacheCluster Headache(Migraneous Neuralgia)(Migraneous Neuralgia)
Lasts 8-12/52; with remission of M Lasts 8-12/52; with remission of M Periodicity Periodicity lasts 45mins lasts 45mins 3 hours 3 hours Common in males; middle aged 30 – 50 yrs Common in males; middle aged 30 – 50 yrs Alcohol ProvokesAlcohol Provokes
unilateral; orbital area / supra-orbital / peri-unilateral; orbital area / supra-orbital / peri-orbital, temporal area orbital, temporal area
conjuctival injection / flushing of faceconjuctival injection / flushing of face nasal stuffiness; Rhinnorhea; nasal stuffiness; Rhinnorhea; lacrimation / tearing lacrimation / tearing Fore-head / Facial sweating; eyelid oedemaFore-head / Facial sweating; eyelid oedema ptosis + ; Miosis + (Horner’s syndrome)ptosis + ; Miosis + (Horner’s syndrome) Most patients are restless or agitated during an attack.Most patients are restless or agitated during an attack.

1818
3. Cluster headache 3. Cluster headache and other trigeminal and other trigeminal autonomic autonomic cephalalgiascephalalgias3.1 Cluster headache3.1 Cluster headache
3.2 Paroxysmal hemicrania3.2 Paroxysmal hemicrania
3.3 Short-lasting unilateral neuralgiform 3.3 Short-lasting unilateral neuralgiform headache attacks with conjunctival headache attacks with conjunctival injection and tearing (SUNCT)injection and tearing (SUNCT)
3.4 Probable trigeminal autonomic 3.4 Probable trigeminal autonomic cephalalgiacephalalgia

PathophysiologyPathophysiology
PAIN inducing structures: PAIN inducing structures: Skin, subcutaneous tissue; muscleSkin, subcutaneous tissue; muscle (pericranium / periosteum of skull(pericranium / periosteum of skull tissue of eye, ENT & nasal sinuses;tissue of eye, ENT & nasal sinuses; vesselsvessels
V - > tentorium = ant craniumV - > tentorium = ant cranium IX / X – Ear / Throat.IX / X – Ear / Throat. 11stst 3 cervical 3 cervical Post fossae Post fossae

Serotonin - 5 HTSerotonin - 5 HT
plays role centrally in pain perception & CBF regulationplays role centrally in pain perception & CBF regulation
Serotonin receptors in Serotonin receptors in 1) Cranial blood vessel (large – constrict; small – dilate). 1) Cranial blood vessel (large – constrict; small – dilate). 2) Central Neurons 2) Central Neurons
3) Dorsal raphe Nucleus and trigeminal Nuclei in brainstem - 3) Dorsal raphe Nucleus and trigeminal Nuclei in brainstem - (high concentration) (high concentration)
((Low central serotonin syndrome)Low central serotonin syndrome) < Platelet Serotonin content reflects change in central serotonergic < Platelet Serotonin content reflects change in central serotonergic
activityactivity
at onset of headache at onset of headache < 5HT and < urinary excretion of its metabolites – < 5HT and < urinary excretion of its metabolites – > 5HIAA> 5HIAA
SerotoninSerotonin
All in all All in all 14 HT receptors 1-7 14 HT receptors 1-7
Serotonin receptors Serotonin receptors 7 7
5 sub class5 sub class 1DB 1DB vascular - involved in Migraine vascular - involved in Migraine ID& ID& Neuronal Neuronal
1A: ID&; IDB; IE; IF;1A: ID&; IDB; IE; IF; 2A: 2B; 2C (HT2 – Prophylactic anti-migraine)2A: 2B; 2C (HT2 – Prophylactic anti-migraine) 5A: 5B5A: 5B Others 1 each. 3,4,6,7 Others 1 each. 3,4,6,7 (HT3 - analgesic)(HT3 - analgesic)

04/18/2304/18/23 2222
Pain Pain NeurotransmittersNeurotransmitters Sub P+ / 5HT- / NR+ Sub P+ / 5HT- / NR+ Sub-P : Sub-P :
Neurohormone/transmitter/modulatorNeurohormone/transmitter/modulator released by central process of DRG at released by central process of DRG at
the synapse in S. gelatinosa.the synapse in S. gelatinosa. VasodilatatorVasodilatator Degranulates mast cellsDegranulates mast cells Chemoattractants for leukocytesChemoattractants for leukocytes >production and release of >production and release of
inflammatory mediators inflammatory mediators (Pro-inflamatory substances)(Pro-inflamatory substances) Neurogenic inflammationNeurogenic inflammation

04/18/2304/18/23 2323
5- HT5- HT 5-HT5-HT33: inhibitory from PMP: inhibitory from PMP (Pain Modulation Pathway)descending(Pain Modulation Pathway)descending cf PTP (Pain Transmission Pathway) -cf PTP (Pain Transmission Pathway) -
ascendingascending NR – inhibitory from PMPNR – inhibitory from PMP but activates / sensitizes but activates / sensitizes
nociceptorsnociceptors Bradykinin enhances stimulatn of C-fibBradykinin enhances stimulatn of C-fib PMP inhibits S.C.P.N by PMP inhibits S.C.P.N by inhibitory transmitters from PMP inhibitory transmitters from PMP
(5HT) or excitation of inhibitory (5HT) or excitation of inhibitory enkephalinergic interneurons. enkephalinergic interneurons.

Theories of MigraineTheories of Migraine (1. Cerebrovascular)(1. Cerebrovascular)
AV shunts (opening)AV shunts (opening)
instability of vessel instability of vessel vasoconstriction/dilatationvasoconstriction/dilatation
excessive dilatation of excessive dilatation of arteries in Meningesarteries in Meninges

Theoriesof Migraine Theoriesof Migraine ( 2. Neurogenic - Cerebroparnchymal)( 2. Neurogenic - Cerebroparnchymal)
2. NEUROGENIC THEORY 2. NEUROGENIC THEORY (Moskowitz) (Cerebroparenchymal) (Moskowitz) (Cerebroparenchymal)
PRODROME:- HypothalamicPRODROME:- Hypothalamic AURA – LEAO’S spreading AURA – LEAO’S spreading
cortical depression and vascular cortical depression and vascular changeschanges
Does not ff a vascular territory - Does not ff a vascular territory - spreading oligaemia 3ml/min or spreading oligaemia 3ml/min or 2mm/min2mm/min

2626
Initiating Mechanisms of Initiating Mechanisms of Headache Pain: Headache Pain: Cortical Spreading DepressionCortical Spreading Depression
Wave of intense cortical neuron activity– ↑ rCBF
Followed by neuronal suppression – ↓ rCBF
Velocity: 2–3 mm/min Underlies visual aura
rCBF = regional cerebral blood flow.
Adapted with permission from Hadjikhani N, Sanchez del-Rio M, et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc Natl Acad Sci U S A. 2001;98:4687-4692. Copyright 2001 National Academy of Sciences, U.S.A.
Pietrobon D. Neuroscientist. 2005;11:373–386; Goadsby PJ et al. N Engl J Med. 2002;346:257–270.
Time(s)
Occipital cortex

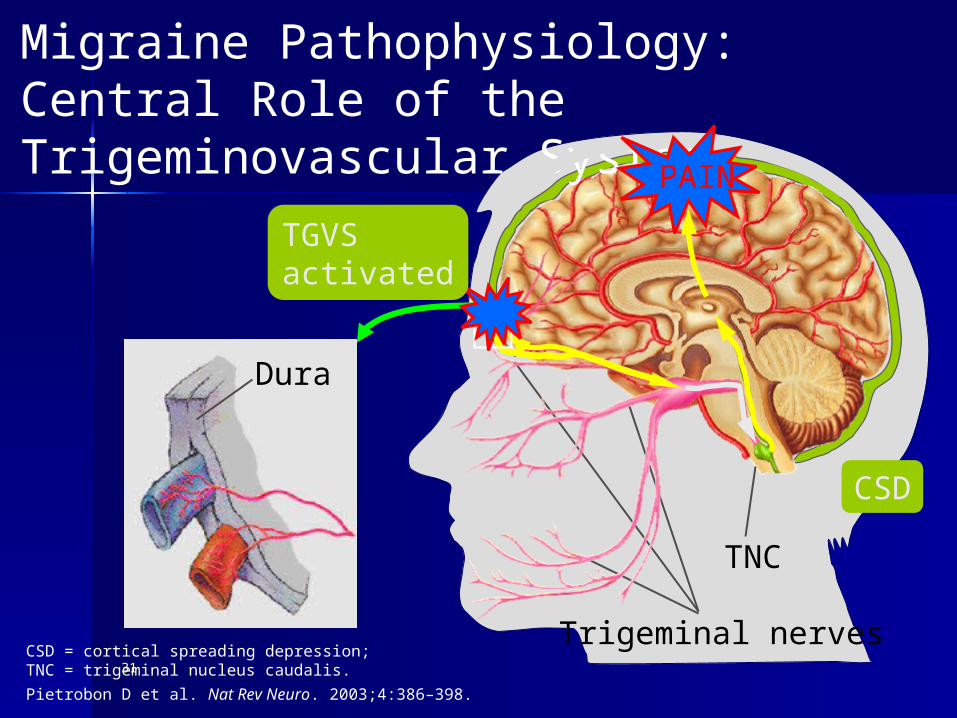
Theories of Migraine Theories of Migraine ( (3. Trigemino-vascular)3. Trigemino-vascular) Headache Headache Neurogenic inflammation Neurogenic inflammation
antidromic stimulation of Trigeminal Nucleus antidromic stimulation of Trigeminal Nucleus
Neuropeptides – substance P; Neurokinin A and Neuropeptides – substance P; Neurokinin A and Calcitonin – G- Related Protein. Calcitonin – G- Related Protein.
Nitric oxide; GlutamateNitric oxide; Glutamate M.H. AND T.H. M.H. AND T.H. Same pathogenesis Same pathogenesis
Sudden drop level of 5HT Sudden drop level of 5HT Migraine in BS. Migraine in BS. Chronic Low Level of 5HT in T.H (v. low) Chronic Low Level of 5HT in T.H (v. low) not due to muscle contraction- also fd in M.not due to muscle contraction- also fd in M.

TRIGEMINO VASCULAR TRIGEMINO VASCULAR HYPOTHESIS.HYPOTHESIS. Release of Neuropeptides (CGRP; Sub P Release of Neuropeptides (CGRP; Sub P
& Neurokinin A; NO ; Glutamate) & Neurokinin A; NO ; Glutamate) which act as neurotrammiters of which act as neurotrammiters of
Trigeminal N branches Trigeminal N branches leads to inflammatory process leads to inflammatory process (Neurogenic inflammation)(Neurogenic inflammation) plasma extravasation and plasma extravasation and
vasodilatation vasodilatation Increased permeabilityIncreased permeability IDb receptorIDb receptor Agents acting on ID (stimulator) Agents acting on ID (stimulator)
prevent release of peptides (not prevent release of peptides (not histamine)histamine)


Approach to TreatmentApproach to Treatment
> 5HT receptor agonist> 5HT receptor agonist
Non- 5HT receptor agonist Non- 5HT receptor agonist e.g Re.g Rάά - - methyl histamine (e.g methyl histamine (e.g
somatostatin)somatostatin)
Neurokinin receptor antagonistNeurokinin receptor antagonist
CGRP receptor antagonistCGRP receptor antagonist
3131
Dura
Migraine Pathophysiology: Central Role of the Trigeminovascular System
Trigeminal nerves
TNC
CSD = cortical spreading depression; TNC = trigeminal nucleus caudalis.
Pietrobon D et al. Nat Rev Neuro. 2003;4:386–398.
PAIN
CSD
TGVS activated

3232
Initiating Mechanisms Initiating Mechanisms of Migraine: Brainstem of Migraine: Brainstem DysfunctionDysfunction
Dysfunction in areas Dysfunction in areas involved in central involved in central control of nociception - control of nociception - PAGPAG
Induces migraine?Induces migraine?– Brainstem generatorBrainstem generator
Facilitates activation Facilitates activation and sensitization of and sensitization of TNC neurons?TNC neurons?– Decreased descending Decreased descending
inhibition during a inhibition during a migraine attackmigraine attackPAG = periaqueductal gray region
Adapted with permission from Pietrobon D. Nat Rev Neurosci. 2003;4:386–398.
PAG
TGVS activation
HEADACHE
Substance P

3333
Low threshold to abnormal cortical activity Cortical Spreading Depression
The Primary Cause of The Primary Cause of Migraine Headache Lies in Migraine Headache Lies in the Brainthe Brain
Cortical neuronal hyperexcitability and/orbrainstem dysfunction
Activation & sensitization of the TGVS
Prolonged headache pain of migraine
Genetic predisposition in some patients
Trigger

3434
Migraine Migraine Pathophysiology:Pathophysiology:Proposed Mechanisms Proposed Mechanisms
Aura CSD
Cortical neuronal hyperexcitability
Activation and peripheral sensitization of TGVS
Neurogenicinflammation
Centralsensitization
HEADACHE
?
+
+
Genetic predisposition
Migraine initiation
Pain generation/perpetuation
Abnormal brainstem function

Cluster HeadacheCluster Headache
Hypothalamic dysfnHypothalamic dysfn Post. Hypothalamic Post. Hypothalamic Autonomic Autonomic Ant. Hypothalamic Ant. Hypothalamic biologic clock biologic clock
Hypoxaemia – Carotid body chemo receptor Hypoxaemia – Carotid body chemo receptor dysfndysfn
Periodic discharge by TVSPeriodic discharge by TVS
Changes in level of cortisol; melantonin; Changes in level of cortisol; melantonin; prolactin ; B-endorphin. prolactin ; B-endorphin.

Diagnosis - Diagnosis - InvestigationsInvestigations a clinical problem:a clinical problem:
Solved by taking a careful medical Solved by taking a careful medical history.history.
Not needNot need .. EEG / SKULL X-ray EEG / SKULL X-ray .. Isotope Brain scanIsotope Brain scan .. CATCAT
except if suspect Brain T or Surgery.except if suspect Brain T or Surgery.

Diagnosis - HistoryDiagnosis - History
psychological and environmental background.psychological and environmental background. family history, age of onset; head injury family history, age of onset; head injury
behavioural changes, environmental stress.behavioural changes, environmental stress. Time, duration .Time, duration . ChracteristicsChracteristics .. Visual/sensory somatic syndrome Visual/sensory somatic syndrome .. Location Location ? vascular malformation if ? vascular malformation if same sidesame side Throbbing/Stabbing/Steady ache Throbbing/Stabbing/Steady ache
Assoc symptoms Assoc symptoms N/V/photo/Phonophobia; N/V/photo/Phonophobia; conjuctival injection; lacrimation; flushing of conjuctival injection; lacrimation; flushing of
face.face.

History - predisposing History - predisposing factorsfactors familial; pills; menses familial; pills; menses and other ppt factors / provocative and other ppt factors / provocative Alcohol Alcohol Food Food cheese, chocolate, cheese, chocolate,
orange/tomatoesorange/tomatoes Physical & mental stressPhysical & mental stress Relaxation after stressRelaxation after stress Absence of food; Hormonal Absence of food; Hormonal
variationvariation Red wine; Bright light; insomniaRed wine; Bright light; insomnia

Treatment – mild Treatment – mild attackattackTreat underlying problemTreat underlying problem
ACUTE ATTACK (ABORTIVE)ACUTE ATTACK (ABORTIVE) Simple Measures Simple Measures Darkened roomDarkened room ANALGESICSANALGESICS ASPIRIN / PROPOXYPHENE HCLASPIRIN / PROPOXYPHENE HCL NAPROXEN/ NAPROXEN/
IBUPROFEN/PARACETAMOLIBUPROFEN/PARACETAMOL ISOMETHAPTENE (MIDRIN) ISOMETHAPTENE (MIDRIN)

Treatment – abortive / Treatment – abortive / prophylaxisprophylaxis
Acute treatmentAcute treatment HTIDb HTIDb presynaptic presynaptic
prophylactic prophylactic HT2 HT2 post synaptic post synaptic

Treatment - more Treatment - more severe attacksevere attack 1928: ERGOTAMINE – 5HT1 receptor1928: ERGOTAMINE – 5HT1 receptor Inhibit 5HT2 ; Stimulate 5HT1 Inhibit 5HT2 ; Stimulate 5HT1 .. SublingualSublingual .. OralOral .. RectalRectal .. InhalationInhalation 1-2mg taken early in attack preferably at 1-2mg taken early in attack preferably at
onset of prodromal symptoms.onset of prodromal symptoms. Repeat > 30minsRepeat > 30mins Repeated doses thereafter useless / Repeated doses thereafter useless /
harmful.harmful. Max dose 10-12mg/wk Max dose 10-12mg/wk

Ergotamine – adverse Ergotamine – adverse effectseffects vomiting - use as suppositoryvomiting - use as suppository Muscle cramps: peripheral tingling and Muscle cramps: peripheral tingling and
gangrene gangrene
C.I. C.I. Peripheral Vascular Disease. Peripheral Vascular Disease.
added caffeine (Cafegot)added caffeine (Cafegot) Raynauds PhenomenonRaynauds Phenomenon
Dihydro ergotamine -- HT1D agonistDihydro ergotamine -- HT1D agonist .. S.C./I.V/I.MS.C./I.V/I.M ..
Sumatriptan - 1991Sumatriptan - 1991
Has antiemetic effectHas antiemetic effect
Rapid absorbtionRapid absorbtion
5HTID receptor agonist5HTID receptor agonist
Orally / parenterallyOrally / parenterally

Prophylaxis Prophylaxis
.. AVOID TRIGGER FACTORSAVOID TRIGGER FACTORS Food ; stressFood ; stress .. Life style changes. Life style changes. Physical / occupation Rx Physical / occupation Rx
.. Drug treatment if > 3 Drug treatment if > 3 attacks / mthattacks / mth

Prophylaxis Prophylaxis 5HT2 receptors 5HT2 receptors antagonistantagonist PROMETHAZINE 25mgPROMETHAZINE 25mg
B- BLOCKERS B- BLOCKERS PROPRANOLOL 20mg bd – 80mg tds; PROPRANOLOL 20mg bd – 80mg tds; ATENOLOL; NADOLOL; TIMOLOLATENOLOL; NADOLOL; TIMOLOL
TRICYCLIC ANTIDEPRESSANTSTRICYCLIC ANTIDEPRESSANTS . . Amitryptilline Amitryptilline . . Low dose: > 1/12 for effectLow dose: > 1/12 for effect
.. Nortriptyline; b-BlockersNortriptyline; b-Blockers
Prevents reuptake – 5HT1 Prevents reuptake – 5HT1 Blocks 5HT2 Blocks 5HT2

ProphylaxisProphylaxis
PIZOTIFEN (SANDO MIGRAINE) 0.5 -2mg t.d.s. – PIZOTIFEN (SANDO MIGRAINE) 0.5 -2mg t.d.s. – 5HT 2 receptor blockade5HT 2 receptor blockade
CLONIDINE 25 ug bd – 50ug tdsCLONIDINE 25 ug bd – 50ug tds Site of action Site of action uncertain - ? central vasomotor uncertain - ? central vasomotor
blockade or direct action on vessel wall blockade or direct action on vessel wall
CALCIUM – CHANNEL BLOCKERSCALCIUM – CHANNEL BLOCKERS Prevent Ca influx induced by 5HT.Prevent Ca influx induced by 5HT. VerapamilVerapamil NifedipineNifedipine DiltiazemDiltiazem Flunarizine Flunarizine

Prophylaxis – Prophylaxis – serotonin antagonistsserotonin antagonists
CyproheptadineCyproheptadine
MAO Inhibitor (phenelzine) 15mg MAO Inhibitor (phenelzine) 15mg tdstds
AspirinAspirin
Methysergide Methysergide 1mg/d1mg/d 2mg/d 2mg/d (Retro peritoneal fibrosis)(Retro peritoneal fibrosis)

Other treatmentOther treatment
short course steroid short course steroid
Neuroleptics Neuroleptics
Occipital Nerve block Occipital Nerve block

Fig 1Fig 1
Midbrain / brain stemMidbrain / brain stem
forebrain forebrain
Low 5HT Low 5HT Excitatory Excitatory
Excess 5HT – inhibitory at synapseExcess 5HT – inhibitory at synapse

Treatment – Tension HTreatment – Tension H
Same Treatment Same Treatment
No place for No place for Anxiolytic Anxiolytic muscle relaxant muscle relaxant

Treatment - CLUSTER HTreatment - CLUSTER Habortive abortive
.. O2 - 100%O2 - 100% .. ERGOTAMINEERGOTAMINE .. DihydroergotamineDihydroergotamine .. SumatriptanSumatriptan .. CorticosteroidsCorticosteroids .. Local anaestheticLocal anaesthetic .. 4% xylocaine -4% xylocaine - instil in instil in
NostrilNostril .. Sphenopalatine ganglian blockSphenopalatine ganglian block

Treatment – Cluster HTreatment – Cluster HprophylaxisprophylaxisCa 2+ channel blocker - Ca 2+ channel blocker - VerapamiVerapami
Lithium carbonateLithium carbonate
MethysergideMethysergide
Steroids - Predinsolone 40 – 80mg/dSteroids - Predinsolone 40 – 80mg/d

NEWER TREATMENT – NEWER TREATMENT – Cluster HCluster H
Valproate Valproate
Nerve blockersNerve blockers
Light treatmentLight treatment
expose patient to light change expose patient to light change
circadian rhythm circadian rhythm

PrognosisPrognosis
Good Good except if symptomatic migraine except if symptomatic migraine due todue to cerebrovascular malformationcerebrovascular malformation Cererovascular angioma.Cererovascular angioma. Cerebrovascular aneurysmCerebrovascular aneurysm

5555
1. Migraine1. Migraine
1.1 Migraine without aura1.1 Migraine without aura1.2 Migraine with aura1.2 Migraine with aura1.3 Childhood periodic syndromes 1.3 Childhood periodic syndromes
that are that are commonly precursors of migrainecommonly precursors of migraine1.4 Retinal migraine1.4 Retinal migraine1.5 Complications of migraine1.5 Complications of migraine1.6 Probable migraine1.6 Probable migraine

5656
1.1 Migraine without 1.1 Migraine without auraaura A recurrent headache disorder A recurrent headache disorder
manifesting in attacks lasting 4-72 manifesting in attacks lasting 4-72 hours.hours.
Typical characteristics of the headache Typical characteristics of the headache are unilateral location, pulsating are unilateral location, pulsating quality, moderate or severe intensity, quality, moderate or severe intensity, aggravation by routine physical aggravation by routine physical activity and association with nausea activity and association with nausea and/or photophobia and phonophobia.and/or photophobia and phonophobia.

5757
IHS Diagnostic Criteria IHS Diagnostic Criteria for Migraine without for Migraine without auraauraA. At least 5 attacks fulfilling criteria B through DA. At least 5 attacks fulfilling criteria B through DB. Headache attacks lasting 4-72 hrs (untreated or B. Headache attacks lasting 4-72 hrs (untreated or
unsuccessfully treated)unsuccessfully treated)C. Headache has at least two of the following characteristics:C. Headache has at least two of the following characteristics:
1. Unilateral location1. Unilateral location2. Pulsating quality2. Pulsating quality3. Moderate or severe pain intensity3. Moderate or severe pain intensity4. Aggravation by or causing avoidance of routine physical activity 4. Aggravation by or causing avoidance of routine physical activity ((eg, eg, climbing stairs)climbing stairs)
D. During headache at least 1 of the following:D. During headache at least 1 of the following:1. Nausea and/or vomiting1. Nausea and/or vomiting2. Photophobia and phonophobia2. Photophobia and phonophobia
E. Not attributed to another disorderE. Not attributed to another disorder

5858
1.2 Migraine with aura1.2 Migraine with aura
A recurrent disorder manifesting in A recurrent disorder manifesting in attacks of reversible focal neurological attacks of reversible focal neurological symptoms that usually develop symptoms that usually develop gradually over 5-20 minutes and last gradually over 5-20 minutes and last for less than 60 minutes.for less than 60 minutes.
Headache with the features of Headache with the features of migraine without aura usually follows migraine without aura usually follows the aura symptoms. the aura symptoms.
Headache may be absent.Headache may be absent.

5959
1.2 Migraine with aura1.2 Migraine with aura
1.2.1 Typical aura with migraine 1.2.1 Typical aura with migraine headacheheadache
1.2.2 Typical aura with non-migraine 1.2.2 Typical aura with non-migraine headacheheadache
1.2.3 Typical aura without headache1.2.3 Typical aura without headache
1.2.4 Familial hemiplegic migraine1.2.4 Familial hemiplegic migraine
1.2.5 Sporadic hemiplegic migraine1.2.5 Sporadic hemiplegic migraine
1.2.6 Basilar-type migraine1.2.6 Basilar-type migraine

6060
IHS Diagnostic Criteria IHS Diagnostic Criteria for Migraine with aurafor Migraine with auraA. At least 2 attacks fulfilling criteria B through DA. At least 2 attacks fulfilling criteria B through DB. Aura consisting of at least one of the following but no motor weakness:B. Aura consisting of at least one of the following but no motor weakness: 1. fully reversible visual symptoms including positive features (1. fully reversible visual symptoms including positive features (eg, eg, flickering lights, flickering lights,
spots or lines) and/or negative features (spots or lines) and/or negative features (ie,ie,loss of vision)loss of vision) 2. fully reversible sensory symptoms including positive features (2. fully reversible sensory symptoms including positive features (ie,ie, pins and needles) pins and needles)
and/or negative features (and/or negative features (ie, ie, numbness)numbness) 3. fully reversible dysphasic speech disturbance3. fully reversible dysphasic speech disturbanceC. At least two of the following:C. At least two of the following: 1. homonymous visual symptoms and/or unilateral sensory symptoms1. homonymous visual symptoms and/or unilateral sensory symptoms 2. at least one aura symptom develops gradually over ≥5 minutes and/or different 2. at least one aura symptom develops gradually over ≥5 minutes and/or different
aura symptoms occur in succession over ≥5 minutesaura symptoms occur in succession over ≥5 minutes 3. each symptom lasts ≥5 and ≤60 minutes3. each symptom lasts ≥5 and ≤60 minutesD. Headache fulfilling criteria B-D for Migraine without aura begins during the D. Headache fulfilling criteria B-D for Migraine without aura begins during the
aura or follows aura within 60 minutes aura or follows aura within 60 minutes E. Not attributable to another disorder E. Not attributable to another disorder

6161
2. Tension-type 2. Tension-type headache (TTH)headache (TTH)
2.1 Infrequent episodic TTH2.1 Infrequent episodic TTH
2.2 Frequent episodic TTH2.2 Frequent episodic TTH
2.3 Chronic TTH2.3 Chronic TTH
2.4 Probable TTH2.4 Probable TTH

6262
2.1 Infrequent 2.1 Infrequent episodic TTHepisodic TTH Infrequent episodes of headache Infrequent episodes of headache
lasting minutes to days. lasting minutes to days. The pain is typically bilateral, pressing The pain is typically bilateral, pressing
or tightening in quality and of mild to or tightening in quality and of mild to moderate intensity, and does not moderate intensity, and does not worsen with routine physical activity. worsen with routine physical activity.
There is no nausea but photophobia or There is no nausea but photophobia or phonophobia may be present.phonophobia may be present.

6363
IHS Diagnostic Criteria IHS Diagnostic Criteria for Infrequent Episodic for Infrequent Episodic TTHTTHA.A. At least 10 episodes occurring on <1 day per month on average (<12 days At least 10 episodes occurring on <1 day per month on average (<12 days
per year) and per year) and fulfilling criteria B through Dfulfilling criteria B through D
B. Headache lasting from 30 mins to 7 daysB. Headache lasting from 30 mins to 7 daysC. Headache has at least two of the following characteristics:C. Headache has at least two of the following characteristics:
1. bilateral location1. bilateral location2. pressing/tightening (non-pulsating) quality2. pressing/tightening (non-pulsating) quality3. mild or moderate intensity3. mild or moderate intensity4. not aggravated by routine physical activity such as walking or climbing 4. not aggravated by routine physical activity such as walking or climbing stairsstairs
D. Both of the following:D. Both of the following:1. no nausea or vomiting (anorexia may occur)1. no nausea or vomiting (anorexia may occur)2. no more than one of photophobia or phonophobia2. no more than one of photophobia or phonophobia
E. Not attributed to another disorderE. Not attributed to another disorder

6464
2.2 Frequent episodic 2.2 Frequent episodic TTHTTH Frequent episodes of headache lasting Frequent episodes of headache lasting
minutes to days. minutes to days. The pain is typically bilateral, pressing The pain is typically bilateral, pressing
or tightening in quality and of mild to or tightening in quality and of mild to moderate intensity, and does not moderate intensity, and does not worsen with routine physical activity. worsen with routine physical activity.
There is no nausea but photophobia or There is no nausea but photophobia or phonophobia may be present.phonophobia may be present.

6565
IHS Diagnostic Criteria IHS Diagnostic Criteria for frequent Episodic for frequent Episodic TTHTTHA.A. At least 10 episodes occurring on ≥1 but <15 days per month for at least 3 At least 10 episodes occurring on ≥1 but <15 days per month for at least 3
months (≥12 months (≥12 and <180 days per year) and fulfilling criteria B through Dand <180 days per year) and fulfilling criteria B through D
B. Headache lasting from 30 mins to 7 daysB. Headache lasting from 30 mins to 7 daysC. Headache has at least two of the following characteristics:C. Headache has at least two of the following characteristics:
1. bilateral location1. bilateral location2. pressing/tightening (non-pulsating) quality2. pressing/tightening (non-pulsating) quality3. mild or moderate intensity3. mild or moderate intensity4. not aggravated by routine physical activity such as walking or climbing 4. not aggravated by routine physical activity such as walking or climbing stairsstairs
D. Both of the following:D. Both of the following:1. no nausea or vomiting (anorexia may occur)1. no nausea or vomiting (anorexia may occur)2. no more than one of photophobia or phonophobia2. no more than one of photophobia or phonophobia
E. Not attributed to another disorderE. Not attributed to another disorder

6666
2.3 Chronic TTH2.3 Chronic TTH
A disorder evolving from episodic tension-A disorder evolving from episodic tension-type headache, with daily or very type headache, with daily or very frequent episodes of headache lasting frequent episodes of headache lasting minutes to days. minutes to days.
The pain is typically bilateral, pressing or The pain is typically bilateral, pressing or tightening in quality and of mild to tightening in quality and of mild to moderate intensity, and it does not moderate intensity, and it does not worsen with routine physical activity. worsen with routine physical activity.
There may be mild nausea, photophobia There may be mild nausea, photophobia or phonophobia.or phonophobia.

6767
IHS Diagnostic Criteria IHS Diagnostic Criteria for chronic TTHfor chronic TTHA.A. Headache occurring on ≥15 days per month on average for >3 Headache occurring on ≥15 days per month on average for >3
months (≥180 days per year) and fulfilling criteria B through Dmonths (≥180 days per year) and fulfilling criteria B through DB.B. Headache lasts hours or may be continuousHeadache lasts hours or may be continuousC.C. Headache has at least two of the following characteristics:Headache has at least two of the following characteristics:
1. bilateral location1. bilateral location2. pressing/tightening (non-pulsating) quality2. pressing/tightening (non-pulsating) quality3. mild or moderate intensity3. mild or moderate intensity4. not aggravated by routine physical activity such as walking or 4. not aggravated by routine physical activity such as walking or climbing stairsclimbing stairs
D.D. Both of the following:Both of the following:1. no more than one of photophobia, phonophobia or mild nausea1. no more than one of photophobia, phonophobia or mild nausea2. neither moderate or severe nausea nor vomiting2. neither moderate or severe nausea nor vomiting
E.E. Not attributed to another disorderNot attributed to another disorder

6868
3.1 Cluster headache3.1 Cluster headache
This is a disorder with attacks of severe, strictly This is a disorder with attacks of severe, strictly unilateral pain which is orbital, supraorbital, unilateral pain which is orbital, supraorbital, temporal or in any combination of these sites, temporal or in any combination of these sites, lasting 15-180 minutes and occurring from lasting 15-180 minutes and occurring from once every other day to 8 times a day. once every other day to 8 times a day.
The attacks are associated with one or more of The attacks are associated with one or more of the following, all of which are ipsilateral: the following, all of which are ipsilateral: conjunctival injection, lacrimation, nasal conjunctival injection, lacrimation, nasal congestion, rhinorrhoea, forehead and facial congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis, eyelid oedema. sweating, miosis, ptosis, eyelid oedema.
Most patients are restless or agitated during an Most patients are restless or agitated during an attack.attack.

6969
3.1 Cluster headache3.1 Cluster headache
3.1.1 Episodic cluster headache3.1.1 Episodic cluster headache
3.1.2 Chronic cluster headache3.1.2 Chronic cluster headache

7070
IHS Diagnostic Criteria IHS Diagnostic Criteria for Cluster Headachefor Cluster HeadacheA.A. At least 5 attacks fulfilling criteria B through DAt least 5 attacks fulfilling criteria B through DB.B. Severe or very severe unilateral orbital, supraorbital and/or Severe or very severe unilateral orbital, supraorbital and/or
temporal pain lasting 15-180 mins if untreatedtemporal pain lasting 15-180 mins if untreatedC.C. Headache is accompanied by at least one of the following:Headache is accompanied by at least one of the following:
1. ipsilateral conjunctival injection and/or lacrimation1. ipsilateral conjunctival injection and/or lacrimation2. ipsilateral nasal congestion and/or rhinorrhoea2. ipsilateral nasal congestion and/or rhinorrhoea3. ipsilateral eyelid oedema3. ipsilateral eyelid oedema4. ipsilateral forehead and facial swelling4. ipsilateral forehead and facial swelling5. ipsilateral miosis and/or ptosis5. ipsilateral miosis and/or ptosis6. a sense of restlessness or agitation6. a sense of restlessness or agitation
D.D. Attacks have a frequency from one every other day to 8 per dayAttacks have a frequency from one every other day to 8 per dayE.E. Not attributed to another disorderNot attributed to another disorder

7171
3.1.1 Episodic cluster 3.1.1 Episodic cluster headacheheadache Cluster headache attacks occurring Cluster headache attacks occurring
in periods lasting 7 days to 1 year in periods lasting 7 days to 1 year separated by pain-free periods separated by pain-free periods lasting 1 month or longerlasting 1 month or longer

7272
3.1.2 Chronic cluster 3.1.2 Chronic cluster headacheheadache Cluster headache attacks occurring Cluster headache attacks occurring
for more than 1 year without for more than 1 year without remission or with remissions lasting remission or with remissions lasting less than 1 month.less than 1 month.


















