headache
26
Hot Topics-Headaches
description
- PowerPoint PPT Presentation
Transcript of headache

Hot Topics - Headaches

Introduction
Problematic 40% UK popMigraine occurs in 12-15% UK popEstimated 187,000 attacks daily75% report disability at least sometimes90,000 absenteeisms work / school dailyLost work / impaired effectiveness £1.5 bill. per year

Headache classification - Primary
1. Migraine, including:1.1 Migraine without aura1.2 Migraine with aura 2. Tension-type headache, including: 2.1 Episodic tension-type headache2.2 Chronic tension-type headache 3. Cluster headache4. Miscellaneous headaches unassociated with
structural lesion

Headache classification - Secondary
5. Headache associated with head trauma, including:5.1 Acute post-traumatic headache
5.2 Chronic post-traumatic headache
6. Headache associated with vascular disorders, including:6.3 Subarachnoid haemorrhage
7. Headache associated with non-vascular intracranial disorders, including:
7.1.1 Benign intracranial hypertension
7.3 Intracranial infection
7.6 Intracranial neoplasm

Headache classification - Secondary
8. Headache associated with substances or their withdrawal, including:
8.1.4 Acute alcohol induced headache
8.2.1 Chronic ergotamine induced headache
8.2.2 Chronic analgesics abuse headache
8.3.1 Alcohol withdrawal headache (hangover)
9. Headache associated with non-cephalic infection 10. Headache associated with metabolic disorder

Headache classification - Secondary
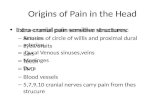
11. Headache or facial pain associated with disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cranial structures, including:
11.2.1 Cervical spine
11.3.1 Acute glaucoma
11.5.1 Acute sinus headache
12. Cranial neuralgias, nerve trunk pain and deafferentation pain, including:
12.1.4.1 Herpes zoster
12.2 Trigeminal neuralgia
13. Headache not classifiable

Pathophysiology of PainRelease of vasoactive substances (e.g., substance P) from trigeminal nerve fibers induces a sterile inflammatory reaction around the blood vessels at the base of the brain and in the blood vessels of the dura and pia.This "neurogenic inflammation" may be accompanied by
vasodilation. Specific abortive agents for migraine such as sumatriptan (Imigran) and ergotamine can reverse this neurogenic inflammation. This effect is probably mediated by interaction with specific serotonin receptors (5-HT1D).Stimulation of inhibitory (5-HT1) serotonin receptors is thought to turn off neurogenic inflammation, whereas activation of the excitatory (5-HT2) serotonin receptors can lead to migraine. Many medications used for migraine prophylaxis work by blocking 5-HT2 receptors.

Diagnosing Headache
History, history, history (Diary)SiteOnsetCharacterRadiationAssociated symptomsTimingExacerbating and relievingSeverityState of health between attacks

Examination
Blood pressureBrief but comprehensive neurological examinationOptic fundiHead and neck ROMInvestigations rarely contribute if Hx and Ex suggest no underlying cause

Important Headaches
MigraineTension-type headacheCluster headache
Medication overuse headache

Causes headaches not to be missed!
Intra-cranial tumoursMeningitisSubarachnoid haemorrhageTemporal arteritisPrimary angle closure glaucomaIdiopathic intracranial hypertensionSubacute carbon monoxide poisoning

Migraine
Moderate or severe pain, which may be unilateral or throbbing Lasts hours to 2-3 days Aggravated by routine activity Associated with nausea and sometimes vomiting Accompanied by photophobia and phonophobia Attacks occur between once a week and once a year (median one per month) One third always have an aura or less commonly a reversible focal neurological disturbance

Migraine
Typical visual aura spreads across the visual field (1-9 left) over about 30 minutes.
Patients can draw their visual aura (above)
Representation of a scintillating scotoma is pathognomonic of migraine

IHS migraine diagnostic criteria (without aura)
An idiopathic, recurring headache disorder with:
A At least 5 attacks fulfilling B-D
B Headache attacks lasting 4-72 hours
C Headache having at least two of the following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe intensity
4. Aggravation by routine physical activity

IHS migraine diagnostic criteria (without aura)
D During headache at least one of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E At least one of the following:
1. History and examination do not suggest any condition to which the headache may be secondary
2. History and/or examination do suggest such a condition, but investigation has excluded it
3. Such a condition exists, but migraine did not begin in temporal relation to it

Migraine
Six elements of good management of migraine in primary care
Correct and timely diagnosisExplanation and appropriate reassurance High but realistic objectives, agreed by doctor and patientIdentification of predisposing or trigger factors and how to avoid themIntervention (drug or non-drug, or both)Referral when these measures fail

Migraine - Acute Rx
‘Stepped care’Simple oral analgesia (soluble form)Prokinetic anti-emeticDiclofenac and domperidone PRTriptians

A proposal for the rational use of triptans*
Use Dose regimenAppropriate for first use of a triptan Sumatriptan 50 mg, zolmitriptan
2.5mg,
When greater efficacy is needed Sumatriptan 100 mg, orsumatriptan 20 mg nasal sprayor zolmitriptan 5 mg orally
In reserve (pending routine clinical experience) Eletriptan 40 - 80 mg orally
When a rapid response is important above all Sumatriptan 6 mg S/C
When vomiting precludes oral therapy Sumatriptan 6 mg S/C
When side effects are troublesome with Naratriptan 2.5mg
other triptans
When relapse is a particular problem Ergotamine 1-2mg rectally

Migraine - Prophylaxis Rx
Use (4-6months) when symptom control with best acute Rx is inadequateß - Blockers (atenolol 50-200 mg (unlicensed indication) or propranolol (long acting) 80-320 mg dailySodium valproate 0.6-2.5 g daily (unlicensed indication)Pizotifen 1.5 mg daily Amitriptyline 50-150 mg at night (unlicensed indication) Mefanamic acid, oestrogen transdermal or COC in menstrually
related migraine

Tension-type Headache
Attack-like episodes (usually 2-3 hours)Variable frequency‘Pressure’ tightness or band likeLacks specific featureRarely disabling‘Chronic’ sub-type >15 days per monthMay be stress related or assoc. with stuctural
cervical or cranial musculoskeletal abnormality

Tension-type Headache
Address underlying factors (remember depression)Regular exerciseReassurance and OTC preparations
(avoid codeine preps)Consider physiotherapyAmitriptyline (4-6 months)

Cluster headache
Affects 1:1000 men and 1:6000 womenMajority >20yrs and many are smokersEpisodic bouts (6-12weeks) once a year or every 2 years around the same timeStrictly unilateral around the eye,once or more daily, commonly at nightPatient agitated and often beats headEye red and watery and nose runs / blocked, +/- ptosisChronic form has a continuous milder background headacheUsually persist more than 30 years

Cluster headache
May go undiagnosed for yearsSpecialist referralAlcohol is a triggerAcute Rx with sumatriptan or oxygen; analgesics have no place!Prophylaxis options will depend on correct diagnosisVerapamilPrednisoloneLithium carbonateErgotamine

Medication overuse headache
Daily or near daily headache affects ~5% pop and chronic overuse of headache preparations account ~50% of theseWomen : men 5:1Common and probable key-factor is pre-emptive useDoesn’t develop if taken for another indicationConfirmed only when symptoms improve after medication is withdrawnHeadache often ‘oppressive’ and worse on awakeningIncreased with physical exertionAssoc. naus and vom rare

Medication overuse headache
Prevention and educationWithdrawal suspected drugsInitial worsening of effectsUsually improves within 2 weeks50-75% revert to original headache typeRelapse rate 40% within 5 yearsMost require extended support

Questions?