HCV Treatment in the Era of DAA - Prof. Gamal Esmatgamalesmat.com/Admin/uploads/HCV...
53
Prof. Gamal Esmat Prof. Hepatology &Ex. Vice President of Cairo University, Egypt Member of WHO Strategic Committee for Viral Hepatitis www.gamalesmat.com HCV Treatment in the Era of DAA
Transcript of HCV Treatment in the Era of DAA - Prof. Gamal Esmatgamalesmat.com/Admin/uploads/HCV...

Prof. Gamal Esmat Prof. Hepatology &Ex. Vice President of Cairo University, Egypt
Member of WHO Strategic Committee for Viral Hepatitis
www.gamalesmat.com
HCV Treatment in the Era of DAA

Ribavirin
Pegylated interferons
Suppression of HCV with DAA combination
(PI + NI)
Curability of HCV without
interferon
Frequent curability of
diverse populations without IFN
Simeprevir or sofosbuvir with IFN (GT1)
HCV therapy: past, present and future
2015+ 1990 2000 2005 2010 2011 2012 2013 2014
Interferon Proof
of concept for DAA (PI)
Telaprevir and
boceprevir
Daclatasvir (Japan and
Europe)
Daclatasvir+ sofosbuvir (GT1b)
Ledipasvir + sofosbuvir
Paritaprevir/RTV/ ombitasvir +
dasabuvir ± RBV
Simeprevir + sofosbuvir
First approved IFN-free therapy: Sofosbuvir +
RBV (GT2,3)
Simeprevir + sofosbuvir (off label use in US and
EU)

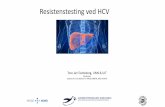
6–19 11–19 10–22
31–44 33–36
61–79
18–39 42–46
76–82 66–79
80–90 85–97
0
20
40
60
80
100
24 48 78
IFN monotherapy (weeks)
IFN + ribavirin PegIFN PegIFN + ribavirin PegIFN + ribavirin + BOC/TVR SMV or SOF + PegIFN + RBV
SOF + RBV
All genotypes Genotype 1 Genotype 2/genotype 3
Evolution of HCV treatment and SVR
rates
Davis GL, et al. N Engl J Med 1989; 321:1501–1506; Poynard T, et al. N Engl J Med 1995; 332:1457–1462; McHutchison JG, et al. N Engl J Med 1998; 339:1485–1492; Poynard T, et al. Lancet 1998; 352: 1426–1432; Zeuzem S, et al. N Engl J Med 2000;
343:1666–1672; Linsay KL, et al. Hepatology 2001; 34:395–403; Pockros PJ, et al. Am J Gastroenterol 2004; 99:1298–1305;
Manns MP, et al. Lancet 2001; 358:958–965; Fried MW, et al. N Engl J Med 2002; 347:975–982; Poordad F, et al. N Engl J Med 2011;
364:1195–1206; Jacobson IM, et al. N Engl J Med 2011; 364:2405–2416; Simeprevir prescribing information, November 2013;
Lawitz E, et al. N Engl J Med 2013; 368:1878–1887; Zeuzem S, et al. Hepatology 2013; 58(Suppl 1):733A; AbbVie press release
2014 [Accessed 25-02-14]; Gilead press release 2013 [Accessed 25-02-14]; Sulkowski MS, et al. N Engl J Med 2014; 370:211–221.
1989 2011 2013 2014/15
SV
R (
%)
DAA
comb
os
95–100

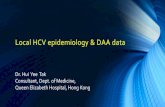
We now have highly efficacious DAAs that target
different stages in the HCV lifecycle
Lindenbach BD, Rice CM. Nature 2005;436(Suppl):933–8; Liang J, Ghany MG. N Engl J Med 2014;370:2043–7.
DAA: direct-acting antiviral agent; ER: endoplasmic reticulum; GT: genotype; IFN: interferon; LD: luminal domain; NA: nucleos(t)ide analogue;
NS: non-structural protein; SVR: sustained virological response
Receptor binding and endocytosis
Fusion and uncoating
Transport and release
(+) RNA Translation and polyprotein processing
RNA replication
Virion assembly
ER lumen
LD
LD
ER lumen
LD
NS3 protease
inhibitors
Non-NA NS5B inhibitors
NA NS5B inhibitors
NS5A inhibitors
Membranous web
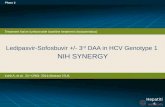
96%
SVR
Summary of New England Journal
of Medicine studies on IFN-free therapy
in GT 1 patients published in 2014
3680/
3826

Non-Nucs
NS5A inhibitors ‘…asvirs’
Sofosbuvir Ledipasvir
Sofosbuvir Daclatasvir
Sofosbuvir Simeprevir
Protease inhibitors ‘…previrs’
Polymerase inhibitors ‘…buvirs’
Nucleos(t)ide
Paritaprevir/r Ombitasvir +/-Dasabuvir
Sofosbuvir + RBV
IFN-free regimens available in 2016
EASL Recommendations 2015, DOI: http://dx.doi.org/10.1016/j.jhep.2015.03.025. Accessed April 2015.
Grazoprevir Elbasvir

Currently approved IFN-free treatment choices
in the International label for patients with HCV GT-4
DCV + SOF1,2
SOF/LDV (FDC)3
SOF2 + Riba
AASLD
x
Duration (weeks)
EASL WHO
x x
SIM + SOF1,2 x
SOF/PEG/RBV x
PARr/OMB
*Consideration should be given to potentially extending treatment duration, up to 24 weeks, especially for those subgroups with one or more factors historically associated with lower response rates to IFN-based therapies. 1. Daklinza (Daclatasvir) SmPC, Bristol-Myers Squibb Pharmaceutical Limited, October 2014. 2. Sovaldi (Sofosbuvir) SmPC, Gilead Sciences Ltd, March 2015. 3. Harvoni (LDV/SOF FDC) SmPC, Gilead Sciences Ltd, November 2014.
Graz/Elba x x

Guidelines of the National Treatment Program in Egypt
• Easy to treat group: • Treatment naïve • Total serum bilirubin ≤ 1.2 mg/dl. • Serum albumin ≥ 3.5 g/dl. • INR≤ 1.2. • Platelet count≥ 150.000/mm3.
• Easy to treat group are eligible to be treated by any of the following regimens for 12 weeks:
• Sofosbuvir + daclatasvir • Sofosbuvir + simeprevir • Sofosbuvir + ledipasvir • Paritaprevir-r/ombitasvir +ribavirin

Guidelines of the National Treatment Program in Egypt
• Not easy to treat group: • Peg-IFN treatment experienced • Total serum bilirubin ≥1.2 mg/dl. • Serum albumin ≤3.5 g/dl. • INR≥1.2. • Platelet count <150.000/mm3.
• These patients are eligible to be treated by any of the following regimens for 12 weeks:
• Sofosbuvir +daclatasvir +ribavirin • Sofosbuvir + simeprevir • Sofosbuvir + ledipasvir +ribavirin • Paritaprevir-r/Ombitasvir +ribavirin
• *The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability.
• *Neither paritaprevir-r/ombitasvir or sofosbuvir-simeprevir is given to patients with Child B or C cirrhosis.

Guidelines of the National Treatment Program in Egypt
Patients with advanced liver disease(Child B)
• Treatment only in one of several assigned specialized centers.
• One of the following regimens is used for 12 weeks :
• Sofosbuvir + Daclatasvir + Ribavirin
• Sofosbuvir + Ledipasvir + Ribavirin
• The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability
• Treatment of patients with post organ transplantation:
• Treatment will be with Sofosbuvir + Daclatasvir or Sofosbuvir + Ledipasvir for 24 weeks

Unique Patient Populations Decompensated Cirrhosis
Genotype Recommended Rating
1 and 4
DCV + SOF + RBV** x 12 weeks
OR
SOF/LDV + RBV** x 12 weeks
Class II, Level A
Class IIb, Level C
2 and 3
DCV + SOF + RBV** x 12 weeks
OR
SOF + RBV x up to 48 weeks
Class II, Level A
Class IIb, Level B
RBV intolerant/ineligible
1 and 4 DCV + SOF x 24 weeks Class IIb, Level C
Prior SOF-based regimen failure
1 and 4 SOF/LDV + RBV** x 24 weeks Class IIb, Level C
* Decompensated cirrhosis (moderate or severe hepatic impairment; CTP class B or C) who may or may not be candidates for liver transplantation,
including those with hepatocellular carcinoma
**initial RBV dose of 600 mg, increased as tolerated
PEG: Pegylated interferon, RBV: Ribavirin, SMV: Simeprevir, SOF: Sofosbuvir, LDV: Ledipasvir, DCV: Daclatasvir, PrOD: Paritaprevir + Ritonavir + Ombitasvir, + Dasabuvir
AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015. AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015.

In subgroup analysis of pts in the advanced cirrhosis cohort, those who
were Child-Pugh class C (n = 16) or had albumin < 2.8 g/dL (n = 18)
had SVR12 rates of 56%
ALLY-1: SVR12 by HCV Genotype
76
97 100 90
80 83 91
100 100
0
20
40
60
80
100
SV
R12, %
1a 1b 2 3 4 6
Genotype
1a 1b 2 3 4 6
Advanced cirrhosis cohort N = 60
Post-transplant cohort N = 53
Child-Pugh Class
11/12
92
A B C
30/ 32
94
9/ 16
56

87 87 8689 89 90
0
20
40
60
80
100
Overall ChildPughB ChildPughC
LDV/SOF+RBV12weeks LDV/SOF+RBV24weeks
SV
R 1
2 (
%)
45/52 42/47 26/30 24/27 19/22 18/20
3 relapses
1 death
1 relapses 2 deaths
1 relapses 1 death 1 LFU
1 relapses 1 death
6 patients were transplanted and excluded from analysis
3 patients did not reach SVR12
108 patients randomized 12 vs 24 weeks
Rbv: escalating dose staring at 600 mg/day
Deaths (n=3), D/S for AE (n=3), OLT (n=4)
Flam et al., AASLD 2014
SOLAR1: LDV-SOF in Decompensated Cirrhosis

AASLD 2015
Patients with HCV who have decompensated cirrhosis (moderate or severe hepatic impairment; Child Turcotte Pugh [CTP] class B or C) should be referred to a medical practitioner who is highly experienced in the management of advanced liver disease and HCV treatment (ideally in a liver transplant center).

SOLAR-1: Change in MELD Score From BL
to FU Wk 4 in Decompensated Cirrhosis
n = 5
n = 5
n = 2
n = 3
(-8)
(+10)
CTP B CTP C 12 wks (n = 30)* 24 wks (n = 29)* 12 wks (n = 23)* 24 wks (n = 26)*
*Missing FU-4: n = 2 CTP B 12 wks; n = 4 CTP B 24 wks; n = 2 CTP C 12 wks; n = 7 CTP C 24 wks. Each bar represents 1 pt.
Flamm SL, et al. AASLD 2014. Abstract 239. Reproduced with permission.
4
2
0
-2
-4
-6
4
2
0
-2
-4
-6
Ch
ange
in M
ELD
Sco
re

Guidelines of the National Treatment Program in Egypt
Patients with chronic kidney disease (CKD):
• In patients having a serum creatinine exceeding the upper normal level, eGFR is calculated, and, accordingly,
• Patients with CKD stage I-II (eGFR> 30 ml/min) are treated by the usual treatment regimens.
• Patients with CKD stage III-V (eGFR≤ 30 ml/min) are treated by Paritaprevir-r/Ombitasvir+ribavirin, provided the following are fulfilled
• Patients have compensated liver (Child A cirrhosis or no cirrhosis) • Hb level is at least 10 g/dL • The patient has no associated uncontrolled co-morbidity (Cardiac, neuro-
psychic,..) • A nephrologist consultation is done. A report determining the treatment
eligibility and necessity, and the exact ribavirin recommended dose (and time of administration in relation to dialysis).
• In case of dialysis, the patient should be aware of the high risk of re-infection by signing a consent form.

Renal Impairment
PEG: Pegylated interferon, RBV: Ribavirin, SMV: Simeprevir, SOF: Sofosbuvir, LDV: Ledipasvir, PTV: Paritaprevir, OBV: Ombitasvir, DSV: Dasabuvir;
Renal
Impairment
eGFR/
CrCl
(ml/mi
n) SOF LDV DCV OBV PTV SMV
Mild 50-80 Standard Standard Standard Standard Standard Standard
Moderate 30-50 Standard Standard Standard Standard Standard Standard
Severe <30 Limited
data
available
Data not
available
Limited
data
available
Standard Standard Standard
ESRD/HD Limited
data
available
Data not
available
Limited
data
available
Limited
data
available
Limited
data
available
Limited
data
available
Abbreviations: CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; HD, hemodialysis.
Unique Patient Populations
AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015.

Guidelines of the National Treatment Program in Egypt
• Patients who failed previous Sofosbuvir containing regimen
• Treatment will be with Sofosbuvir + Daclatasvir + Ribavirin
Or Sofosbuvir + ledipasvir +ribavirin
• for 24 weeks.
• The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability

ATU / AMM project 2014 - 07/12/15 (patients treated with AAD)
18
Cohorte ANRS CO22 HEPATHER
4 978 patients treated with DAA (patients treated in therapeutic trials excluded)
• Combinaisons thérapeutiques
Combination Effective Patients 12 weeks after the DAA initiation
W12 or EOT
Patients 24 weeks after the DAA initiation
SVR12 or EOT
SOF + RBV 463 453 427
SOF + PegIFN + RBV 270 270 268
SOF + DCV 1 487 1 438 1 412
SOF + DCV + RBV 495 472 446
SOF + SMV 793 788 780
SOF + SMV + RBV 88 85 82
SOF + LDV 958 837 711
SOF + LDV + RBV 410 376 319
OBV + PTV+ RTV 123 84 56
OBV + PTV+ RTV + RBV 82 70 55

Figure 8: Real-world experience from the TRIO Network: Patient distribution and SVR rates with all-oral DAA regimens

Figure 9: SVR12 rates by regimen in the TRIO network

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

TREATMENT Of ACUTE HCV

Course of acute, resolving HCV Course of acute HCV evolving into chronicity


Table 2: SOF/LDV vs. SOF + SIM for Acute Hepatitis C: Results

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

Bourlière M, et al. AASLD 2014. Abstract 82. Reproduced with permission.
SVR12 Rates With LDV/SOF ± RBV by Platelet Count, Cirrhosis Level
• SVR12 rates lower among pts determined to have cirrhosis using FibroTest + APRI (89%) and among pts with a platelet count < 75,000 cells/mm3 (84%)
80 90 100
Total Treatment
Naive
Treatment
Experienced
Overall SVR12 96% 98% 95%
Platelets
(x 103/µL)
< 75 84% 90% 82%
≥ 75 to < 100 99% 100% 98%
≥ 100 to < 125 95% 98% 93%
≥ 125 98% 98% 98%
FibroScan
(kPa)
> 12.5 to ≤ 20 99% 100% 99%
> 20 96% 100% 95%
SVR12 (%)
80 90 100
80 90 100

Figure 7: HCV-TARGET: Multivariable Logistic Model for SVR with LDV/SOF

Table 4: TRIO results: predictors of HCV treatment response

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

Figure 30: ASTRAL study program

Figure 32: ASTRAL-1: SVR12 by HCV Genotype

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

Sofosbuvir + ledipasvir FDC:
LONESTAR SVR24 rates
RAV: resistance-associated variant Lawitz E, et al. Lancet 2014;383:515–23
S282T mutation (NS5B inhibitor RAV) and multiple NS5A RAVs were detected in the patient who relapsed after 8 weeks’ SOF/LDV; retreatment was successful with 24 weeks’ SOF/LDV
100
80
60
40
20
0
Pati
en
ts (
%)
–
8
+
8
–
12
+
12
RBV
Duration
(weeks)
Treatment naïve (no cirrhosis) PI failures (50% cirrhosis)
19/20 21/21 18/19 21/21
–
12
18/19
1 relapse 1 lost to
follow up
after SVR8
1 relapse

table 3: Baseline characteristics from the TRIO network

Figure 3a+b: Effectiveness of 8 or 12 week LDV/SOF in GT1, treatment-naïve, non-cirrhotic HCV patients

• LB-23 Complete cure after three weeks of all-oral triple-direct acting antiviral (DAA) regimens in non-cirrhotic chronic hepatitis C genotype 1b Chinese subjects (SODAPI STUDY) George K. Lau3, 5, Yves Benhamou4, Guofeng Chen5, Jin Li6, Qing Shao5, Dong Ji5, Fan Li5, Bing Li5, Jialiang Liu5, Jinlin Hou7, Jian Sun7, Cheng Wang3, 7, Jing Chen3, Vanessa Wu3, April Wong3, Lei Po, Chris Wong8, Stella Tsui Ying Tsang8, Wang Yudong3, Ruian Ke9, Alan S. Perelson9, Raymond F. Schinazi1, 2 1Emory University, 2Veterans Affairs Medical Center, 3Humanity & Health Medical Centre, 4Hôpital Pitié-Salpêtrière, 5302 Hospital, 6302 Hospital, 7Nanfang Hospital, Southern Medical University, 8Hong Kong Molecular Pathology Diagnostic Centre, 9Los Alamos National Laboratory

RG-101 Targeting miR-122 for HCV
• Hepatitis C virus (HCV) uniquely requires the liver-specific microRNA-122 for replication
• Enrollment is complete in an ongoing Phase II study evaluating the combination of RG-101 with multiple approved DAAs. Treatment-naïve patients chronically infected with genotypes 1 or 4 were randomized to one of three treatment arms (n=78).
• Patients receive a single subcutaneous injection of 2 mg/kg of RG-101, followed by 28 days of once/daily DAAs Harvoni®, Olysio®, or Daklinza®, followed by an additional subcutaneous injection of 2 mg/kg of RG-101 on Day 29

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

DAA Treatment Failure
• Relapse or Reinfection.
• RAV (RAS) testing.
• Sofo +Rib+ change from protease to NS5A inh.
or vice versa.
• 24 weeks

AGENDA
• Acute HCV
• Predictors of response
• G3
• Shorten duration of therapy
• Retreatment.
• Future HCV management in Egypt

National Survey (DHS) 2015 (1 -59 years)
2015(1-59 Y) HCV Ab 6.3%
HCV PCR 4.4%

Percentage of women and men with an active hepatitis C infection by age, Egypt 2015
0.9 1.5 1.9
3.2
5.3
7.3
10.4
16.1
17.6
0.6
3.1
4.7
7.1 6.9
10.8
12.4
23.7
27.8
0
5
10
15
20
25
30
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59
women
men

Trends in Percentage of population age 15-59 testing positive HCV Ab, Egypt
1996-2008-2015
22.9 20.1
25.8
14.2 11.8
16.6
10 9
12
total Women Men
Chart Title
1996 2008 2015

HCV in EGYPT from Control to Eradication
To decrease HCV prevalence to< 2 % in Egypt
in 10 years(Mathematical modeling)
Effective treatment SVR > 90%
Annual treatment of 250.000 to 300.000 patients
Prioritize treatment early and to most frequent injectors

Our aim to maintain a disease control (by reaching international prevalence disease rates with 2% infection rate compared with the current 8% infection rate). To reach for disease eradication (disease rate <1%)

Control of HCV in Egypt Overcoming the Barriers
Decrease incidence Ideal drug Mass treatment

Decrease incidence
• Blood safety.
• Avoid unneeded injection.
• Auto destructive syringes.
• Infection control.
• Media awareness.
• Case detection and treatment by Ideal drug

Screening for HCV in Egypt (Targeted)
1)- Families of HCV patients.
- Healthcare providers and students admitted to medical sector in universities
- Patients attending intervention procedures.
2)-Students admitted to the universities.
- Any one asking for a service in a medical facility.
- Before ID or driving license.
3)Everyone

Mass Treatment Curing exceed of 350,000 yearly cases is vital challenge requiring a radical change of treatment regulations Explains as follows: - Patients should be cured by almost "side-effects free" - Curing all the patients, regardless of their age or fibrosis score. - Decrease number of patient visits to only 3 visits - In 2016, we will reach 100 free of charges medical center plus reach 50 health insurance medical centers.

Chronology of Treatment Protocols Implemented by the National Program
Date Implmented Protocol Inclusion criteria
2007-2014 PegIFN-RBV F1-F3 patients
October 2014-May 2015 Sofosbuvir-PegIFN-RBV F3,F4 IFN tolerant
Sofosbuvir-RBV F3,F4 IFN intolerant up to Child B 8 (down to 7)
May 2015-November 2015 Sofosbuvir-PegIFN-RBV F0-F4, normal synthetic function
Sofosbuvir-Simeprevir F0-F4, impaired synthetic function up to Child A6
November 2015 IFN-free regimen. Two DAAs ± RBV
F0-F4, impaired synthetic function up to B7. Higher Child in special centers

World Hepatitis Day in Egypt 28July 2015
• Egypt was chosen to host World Hepatitis Day 2015 as the country has demonstrated a high level of commitment by tackling hepatitis comprehensively in their plan of action for prevention, care and treatment.
• The Ministry of Health has set up 32 specialized centres and introduced a new hepatitis C drug last year, which is the first highly-effective and approved direct-acting antiviral drug for the nationwide treatment of hepatitis C infection. This medication is safer than previous medications and has been shown to cure more than 90% of those completing treatment, in combination with other drugs. In a global first, the drug has been made available to Egyptian patients for US$ 900, which is 1% of its international price. So far, 128 000 people have started the new treatment.

THANK YOU please visit
www.gamalesmat.com
You can see this presentation and more