HBV quantitative sAg assay: Ready for Prime time? yes · HBV quantitative sAg assay: Ready for...
34
HBV quantitative sAg assay: Ready for Prime time? yes Robert G Gish MD Professor Consultant, Stanford University Medical Director: Hepatitis B Foundation 1
Transcript of HBV quantitative sAg assay: Ready for Prime time? yes · HBV quantitative sAg assay: Ready for...

HBV quantitative sAg
assay: Ready for Prime
time?
yes
Robert G Gish MD
Professor Consultant, Stanford University
Medical Director: Hepatitis B Foundation
1

Relevant Disclosures
Consultant: Abbott, Genentech (Roche), Gilead
2
Refining Current Treatments:
Treatment Endpoints
Long-term suppression of HBV DNA
– Ideally by achievement of HBsAg seroconversion
HBeAg-positive
– Sustained HBeAg seroconversion
– If no HBeAg serconversion--> suppression of HBV DNA to low levels
HBeAg-negative
– Sustained low level HBV DNA
• On treatment if nucleosides
• Off treatment if peg-IFN
AASLD Guidelines 2009 EASL Guidelines 2012
APASL Guidelines 2012
Benefits of HBsAg Clearance
Hepatic decompensation
HCC
Survival
Levels of cccDNA
As close to cure as we can
expect to achieve in chronic
hepatitis B
Fattovich G, et al. Am J Gastro 1998; 93:896-900. Werle-Lapostolle B, et al. Gastroenterology 2004;
126(7):1750-1758. Perrillo R. Hepatology 2009; 49:1063-1065.

HBeAg-
positive
CHB
Biomarker Level PPV NPV Ref
Baseline
HBsAg 5,000
50,000
42%
77%
Piratvisuth,
HI 2011
HBeAg ≤ 31 PE
> 1300
54%
76%
Fried. Hepatology 2008
Week 12 HBsAg < 1500 55% Piratvisuth, HI 2011
Sonneveld, Hepatology
2011
No decline 97%
Vs.
82/71%
Sonneveld, Hepatology
2011
Piratvisuth, Hepatology
2011
>20,000 84% (93%) Piratvisuth, HI 2011
HBeAg < 10 53% Fried, Hepatology 2008
Week 24 HBsAg > 20,000 85% (95%, 100%)
HBeAg > 100 Fried, Hepatology 2008
HBsAg, HBeAg Levels for Prediction
of Anti-HBe Seroconversion

J Hepatology 2011;55:1121
1 IU/ml = 1-10 ng/ml HBsAg
= 2 x 108 subviral particles HBsAg
= 5 x 107 virions
What is a Significant Change?
• > 4 fold change
• > 1.0 log IU/ml

HBeAg-Positive
Chronic Hepatitis B
On-treatment HBsAg levels can predict:
PEG-IFN treatment response

Sonneveld et al. Hepatology 2013
Week HBV genotype HBsAg Rule N identified PPV response
Week 12 A (n=98) <1500 IU/mL 14 (14%) 86%
1500 - 20,000 42 (42%) 41%
>20,000 IU/mL 42 (42%) 17%
B (n=199) <1500 IU/mL 60 (30%) 42%
1500 - 20,000 101 (51%) 26%
>20,000 IU/mL 38 (19%) 8%
C (n=377) <1500 IU/mL 89 (24%) 42%
1500 - 20,000 221 (59%) 20%
>20,000 IU/mL 67 (18%) 2%
D (n=105) <1500 IU/mL 2 (2%) 0%
1500 - 20,000 28 (27%) 7%
>20,000 IU/mL 75 (71%) 4%
* Response = HBeAg loss + HBV DNA < 2,000 IU/mL
On-Treatment HBsAg Levels
Identify Good Responders*

Sonneveld et al. Hepatology 2013
Week HBV genotype HBsAg Rule N identified NPV response
Week 12 A (n=55) No decline* 13 (24%) 100%
B (n=120) >20,000 IU/mL 24 (20%) 92%
C (n=225) >20,000 IU/mL 45 (20%) 98%
D (n=54) No decline 33 (61%) 97%
Week 24 A (n=55) >20,000 IU/mL 24 (44%) 96%
B (n=122) >20,000 IU/mL 16 (13%) 100%
C (n=224) >20,000 IU/mL 27 (12%) 100%
D (n=53) >20,000 IU/mL 36 (68%) 100%
* HBsAg decline < 10%
On-Treatment HBsAg Levels
Identify Futility: Stopping Rules

HBeAg-Negative
Chronic Hepatitis B
On-treatment HBsAg levels
can provide:
Futility Rule

Rjickborst, J Hepatology 2012 * HBV DNA < 2,000 IU/mL and normal ALT
Validation cohorts (ph III / PegBeLiver)
(n = 160, genotype D = 91)
No
N = 84 (53%)
Yes
N = 76 (48%)
< 2 logs
N = 22 (14%)
2 logs
N = 62 (39%)
< 2 logs
N = 22 (14%)
2 logs
N = 54 (34%)
37% 45% 43% 5%
HBsAg decline
Week 12
HBV DNA decline
Week 12
SVR*
STOP
Combination of HBsAg and HBV DNA
to Predict SVR in HBeAg-Negative CHB

Predicting HBeAg Seroconversion (HBV DNA compared with quantitative HBeAg)
HBeAg level at Week 24 (Paul Ehrlich units)
HBeAg seroconversion Week 72
All patients
(n=263) > 100 52% NPV 96% 4% (3/72)
HBV DNA level at Week 24 (copies/mL)
All patients (n=263)
> 9.0 log10 21% NPV 86% 14% (8/59)
Fried MW, et al. Hepatology 2008;47:428-434.
NPV = negative predictive value.

Response Guided Therapy for Peg-
Interferon in the Treatment of Hepatitis B
Week 12 and 24 are the Key
HBeAg - Positive HBeAg - Negative
Week 12 – Define Possible Non-Responders Week 12 – Define Possible Non-Responders
Week 24 – Define the Level of Treatment Response Week 24 – Define the Level of Treatment Response
High: HBsAg < 1,500 IU/ml
Mid: HBsAg 1,500 to 20,000 IU/ml
Low: HBsAg > 20,000 IU/ml
High: HBsAg decline >10%
Low: HBsAg decline < 10%
Chan, HLY et al 2011. J Hepatol;55:1121
Criteria:
1) Absence of HBsAg decline OR
2) HBsAg > 20,000 IU/ml
Criteria:
1) Absence of HBsAg decline AND
2) HBV DNA reduction < 2 log

HBsAg decline can predict HBsAg loss on
tenofovir
N=266 patients treated with tenofovir (or adefovir-tenofovir) for 2 years
N=266 overall N=16 cleared HBsAg
0 12 24 36 48 60 72 84 96
0
-25000
-50000
-75000
-100000
-125000
-150000
Weeks of study
HB
sAg
(IU
/mL)
HBsAg levels during treatment
0 12 24 36 48 60 72 84 96
Weeks of study
HBV DNA levels during treatment 0
-2
-4
-6
-8
Ch
ange
fro
m b
ase
line
in H
BV
D
NA
lo
g 10
co
pie
s/m
L)
Heathcote et al. EASL and AASLD 2009

HBsAg Serum Levels Vary in the
Different Phases of HBV Infection
Combined single-point quantification of serum
HBsAg and HBV DNA levels
– Accurate diagnosis of the inactive carrier with
immune control
HBsAg quantification is a new, reliable
diagnostic tool
– Likely to improve (in conjunction with viral load)
the management of chronic HBV infection and
disease

Summary #1
HBsAg in Natural History
HBsAg is an old marker with new applications
HBsAg clearance is the closest to cure in CHB:
functional cure
HBsAg quantification provides additional clinical
guidance:
– Helps determine phase of infection
– The increasing access to quantification assay will foster
learning about how to use it to manage both carriers and
patients more effectively
Threshold levels can be set which predict for inactive
carrier status in HBeAg-negative patients
– Levels of 500 – 1000 should be evaluated further
After S Locarnini 2014

Summary #2
HBsAg Seroclearance as an Endpoint
HBsAg seroconversion is the hallmark of successful immunological control of HBV infection
– Associated with favourable long-term clinical outcomes including a lower incidence of cirrhosis and improved survival
– Can be induced by IFN-based therapy
– Less commonly achieved in patients treated with direct antiviral therapies, i.e. nucleos(t)ide analogues
Most patients have persistently normal ALT levels
Is usually associated with improvement of liver biochemistry
Most patients have undetectable serum HBV DNA with 6-12 months
Still harbour HBV DNA in the liver (cccDNA), but transcriptionally inactive
HCC still did develop in some patients, but only in those over 50 years of age
qHBsAg provides a great NPV:
– Can HBsAg quantification provide a predictive value?
Yuen, M-F. et al 2008. Gastroenterology;135:1192-1199 After S Locarnini 2014

Summary #3
HBsAg in Response Guided Therapy
On-treatment monitoring of HBsAg with or without
HBV DNA offers the prospect of response-guided,
individualized therapy in patients with CHB
– PEG-IFN
• On-treatment HBsAg decline is associated with sustained
immune control
– NAs
• HBsAg monitoring may help identify patients who are able to
stop treatment
HBsAg monitoring has the potential to guide
patient management in the future
After S Locarnini 2014

Start TDF during follow-up if prespecified safety criteria met
Study GS-US-174-0149 Design
Randomized, controlled, open-label study (N=740)
– Stratified by screening HBeAg status and HBV genotype
Inclusion criteria
– HBeAg+ and HBV DNA ≥20,000 IU/mL; HBeAg- and HBV DNA ≥2,000 IU/mL
– ALT >54 and ≤400 U/L (men); ALT >36 and ≤300 U/L (women)
– No bridging fibrosis or cirrhosis on liver biopsy or by transient elastography
0 48 120 72
TDF + PEG
TDF+PEG → TDF
24
n=186
n=184
n=185
n=185 PEG
16
TDF
Week
Primary endpoint: HBsAg loss
H Chan, EASL 2015

Results: HBsAg Loss Over Time (Week 72) P
atie
nts
w
ith
HB
sA
g L
oss,
Kapla
n-M
eie
r E
stim
ate
(%
)
0.10
0.09
0.08
0.07
0.06
0.05
0.04
0.03
0.02
0.01
0.00
48 weeks
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
Week
0.15
0.14
0.13
0.12
0.11
72 weeks
TDF + PEG 16 wk →TDF 32 wk
TDF + PEG 48 wk 9.1%
0%
2.8%
2.8%
p=0.003
p<0.001
p=NS
p=NS PEG 48 wk
TDF 120 wk
7 patients had HBsAg seroreversion on or after Week 48 (4 [TDF + PEG 48 wk],
3 [TDF + PEG 16 wk →TDF 32 wk])
– 5/7 had ≤1 week of therapy after HBsAg loss H Chan, EASL 2015

On-Treatment Predictors of HBsAg Loss at
Week 72
Univariate
p-value
Multivariate
p-value
Hazard
Ratio*
HBsAg decrease >1 log10 IU/mL
by Week 12 <0.001 <0.001 17.8
HBsAg <100 IU/mL at Week 12 <0.001
HBsAg <1000 IU/mL at Week 12 <0.001
HBsAb >10 mIU/mL at Week 12 0.138 0.003 9.97
HBV DNA <15 IU/mL at Week 12 0.014 0.070 15.68
ALT >400 U/L (males) or >300 U/L
(females) during first 12 weeks <0.001 0.031 2.85
*Multivariate
H Chan, EASL 2015

Stopping TDF After Long-Term Virologic
Suppression in HBeAg-Negative CHB
36
FINITE CHB
Randomized
N=45
Withdrew consent
n=3
Week 48
TDF-Restart
n=3
Week 48
TDF-Stop
n=18
Week 48
TDF-Continue
n=21
TDF-Stop
n=21
TDF-Continue
n=21
86% of TDF-Stop subjects did not restart TDF by Week 48
Berg, EASL, 2015, O119

37
* TDF-Restart
-1 1 3 5
HBsAg (log10 reduction)
-1 1 3 5
HBsAg (log10 reduction)
TDF-Stop (n=21) TDF-Continue (n=20)
*
*
*
HBsAg Log10 Reduction: Median 0.283 Mean 0.773 HBsAg loss n=2
HBsAg Log10 Reduction: Median 0.088 Mean 0.109 HBsAg loss n=0
Week 48 HBsAg log10 Reduction (Individual Patients)
FINITE CHB
Stopping TDF was associated with a more profound decline in HBsAg levels compared to continuous TDF
HBsAg loss
HBsAg loss
Berg, EASL, 2015, O119

Immuno-Virologique
1Hôpital Saint Joseph, Marseilles, France,2INSERM UMR-S1136 Saint Antoine Paris,3
1Hôpital Saint Joseph, Marseilles, France,2INSERM UMR-S1136 Saint Antoine Paris,3
Titre document / Le 15 - 09 - 2013
38
EASL 2015 / April 22-26 - Vienna
HBsAg clearance after addition of 48 weeks of PEGIFN in HBeAg negative CHB patients on NUC therapy with undetectable HBV DNA for at least one year : Final results from ANRS-HB06 PEGAN study : a multicenter randomized controlled phase III trial.
Marc Bourlière1, Pascaline Rabiega2, Nathalie Ganne-Carrie3, Lawrence Serfaty4, Patrick Marcellin5, Noëlle Pouget2, Dominique Guyader6, Christophe Hezode7, Magali Picon8, Xavier Causse9, Vincent Leroy10, Jean Pierre Bronowicki11, Ghassan Riachi12, Isabelle Rosa13, Pierre Attali14, Jean Michel Molina15, Yannick Bacq16, Albert Tran17, Jean Didier Grangé18, Fabien Zoulim19, Hélène Fontaine20, Inga Bertucci21, Magali Bouvier-Alias22, Fabrice Carrat 2, Yves Benhamou 23 and the ANRS HB06 PEGAN Study Group.
1Hôpital Saint Joseph, Marseille, France,2INSERM UMR-S1136 Saint Antoine Paris,3Hôpital Jean Verdier, Bondy, 4 Hôpital Saint Antoine, Paris,5 Hôpital Beaujon , Clichy, 6Hôpital Pontchaillou, Rennes,7Hôpital Henri Mondor, Créteil, 8Centre Hospitalier du Pays d’Aix, Aix en provence, 9 Hôpital de la Source, Orléans, 10CHU Grenoble, 11Hôpital de Brabois, Nancy, 12Hôpital Charles Nicolle, Rouen, 13 CHIC Créteil , 14Hôpital Bicêtre, Le Kremlin Bicêtre, 15Hôpital Saint Louis Paris, 16Hôpital Trousseau, Tours, 17Hôpital de L’Archet, Nice, 18Hôpital Tenon, Paris, 19Hôpital Hotel Dieu Lyon, 20Hôpital Cochin, Paris, 21Inserm-ANRS, 22INSERM U635, 23Hôpital La Pitié Salpétrière, Paris.

Study Design
40
N=185 CHB patients
HBeAg negative
N=185 CHB patients
HBeAg negative
N=92 N=92 N=90* N=90*
W-6 W0 W48 W96 W144§
N=93 N=93
ran
do
miz
atio
n
* 1 patient withdrew consent and 1 patient excluded for major deviation inclusion criteria as pre-specified. § Visits W144 are ongoing.
Pti
mar
y e
nd
po
int PEGIFN α2a 180 µg/Wk
NUC treatment
Randomized, controlled, open-label study (N=185). Stratified by HBsAg titer (<2.25 log IU/ml or ≥2.25log IU/ml)
Key inclusion criteria HBeAg negative Undetectable HBV DNA with NUC for at least 1 year Stable NUC regimens for at least 3 months (no Telbivudine) No decompensated cirrhosis
Patients in the PEGIFN group were monitored monthly during the first 48 weeks, then every 3 months.
Treatment discontinuation was allowed if HBsAg loss was sustained for 24 weeks.
N=93 N=93
Bourliere EASL 2015

Efficacy : HBsAg loss and HBs seroconversion
45
All patients included, N (%) NUCs Alone PEGIFN + NUCs
P-Value
Randomization stratification Log10(IU/ml) < 2.25 ≥2.25 Total < 2.25 ≥2.25 Total
N=15 N=78 N=93 N=14 N=76 N=90
W48 Loss of HBsAg 0 (0) 0 (0) 0 (0) 3 (22) 4 (5) 7 (8) 0.0057
HBs seroconversion 0 (0) 0 (0) 0 (0) 2 (14) 2 (3) 4 (4) 0.0384
W96 Loss of HBsAg 2 (13) 1 (1) 3 (3) 4 (29) 3 (4) 7 (8) 0.1521
HBs seroconversion 0 (0) 1 (1) 1 (1) 3 (21) 3 (4) 6 (7) 0.0465
Patients Per Protocol, N(%)
NUCs Alone PEGIFN + NUCs
P-Value N=15 N=78 N=93 N=12 N=73 N=85
W48 Loss of HBsAg 0 (0) 0 (0) 0 (0) 3 (25) 4 (6) 7 (8) 0.0038
HBs seroconversion 0 (0) 0 (0) 0 (0) 2 (17) 2 (3) 4 (5) 0.0296
W96 Loss of HBsAg 2 (13) 1 (1) 3 (3) 4 (33) 3 (4) 7 (8) 0.1038
HBs seroconversion 0 (0) 1 (1) 1 (1) 3 (25) 3 (4) 6 (7) 0.0341
Patients Per Protocol full dose of PEGIFN, N (%)
NUCs Alone PEGIFN + NUCs
P-Value N=15 N=78 N=93 N=10 N=55 N=65
W48 Loss of HBsAg 0 (0) 0 (0) 0 (0) 3 (30) 4 (7) 7 (11) 0.0011
HBs seroconversion 0 (0) 0 (0) 0 (0) 2 (20) 2 (4) 4 (6) 0.0145
W96 Loss of HBsAg 2 (13) 1 (1) 3 (3) 4 (40) 3 (5) 7 (11) 0.0415
HBs seroconversion 0 (0) 1 (1) 1 (1) 3 (30) 3 (5) 6 (9) 0.0131
Bourliere EASL 2015

52
Univariate analysis
All patients included
N=7/90
Patients Per Protocol
N=7/85
Patients Per protocol full dose of PEGIFN N=7/65
OR IC 95% P-value OR IC 95% P-value OR IC 95% P-value
HBeAg at diagnosis (- vs +) 2.77 0.37 18.27 0.3865 2.80 0.37 18.62 0.3814 2.74 0.35 18.99 0.4137
HBsAg at randomization by decreasing unit (log10)
3.43 1.09 12.47 0.0339 3.60 1.11 13.64 0.0300 4.00 1.17 16.41 0.0240
Fibrosis (F3-F4 vs F0-F2) 2.49 0.39 18.25 0.4319 2.30 0.36 16.86 0.4971 2.92 0.44 22.20 0.3368
Previous PEGIFN treatment (yes vs no) 2.33 0.37 17,00 0.4804 2.23 0.35 16.31 0.5190 2.32 0.36 17.37 0.4998
Related to HBs seroconversion
Age, sex, origin, IL-28B profil, duration of undetectable HBV DNA from first undetectability and from latest undetectability were tested and were not significant.
Univariate analysis
All patients included
N=6/90
Patients Per Protocol
N=6/85
Patients Per protocol full dose of PEGIFN N=6/65
OR IC 95% P-value OR IC 95% P-value OR IC 95% P-value
HBeAg at diagnosis (- vs +) 3.74 0.46 30.64 0.2594 3.78 0.46 31.22 0.2555 3.71 0.44 31.77 0.2774
HBsAg at randomization by decreasing unit (log10)
3.50 1.02 14.29 0.0465 3.68 1.04 15.59 0.0419 4.03 1.09 18.22 0.0349
Fibrosis (F3-F4 vs F0-F2) 1.81 0.23 14.42 0.7611 1.67 0.21 13.33 0.8374 2.08 0.25 17.51 0.6498
Previous PEGIFN treatment (yes vs no) 3.55 0.48 41.37 0.2838 3.40 0.46 39.73 0.3096 3.54 0.47 42.28 0.2947
Related to HBsAg loss
Baseline predictive factors at W96 in PEGIFN group
Bourliere EASL 2015

W96 HBsAg loss according to HBsAg titer at inclusion
53
All patients included NUCs Alone
N=93 Trend test
PEGIFN + NUCs N=90
Trend test
HBsAg titer at W0 (log10 IU/ml), N <2 2/12
0.0038 2/8
0.0245 2-3 1/22 3/26 ≥3 0/59 2/56
Patients Per Protocol NUCs Alone
N=93 Trend test
PEGIFN + NUCs N=85
Trend test
<2 2/12 0.0038
2/7 0.0200 2-3 1/22 3/25
≥3 0/59 2/53
Patients Per Protocol full dose of PEGIFN
NUCs Alone N=93
Trend test
PEGIFN + NUCs N=65
Trend test
<2 2/12 0.0038
2/6 0.0150 2-3 1/22 3/16
≥3 0/59 2/43
HBsAg loss is associated with low baseline HBsAg titer.
HBsAg titer (log10IU/ml) NUCs Alone
N=93
PEGIFN+NUCs
N=65
< 2 log10 IU/ml 16% 33%
< 3 log10 IU/ml 8% 23%
> 3 log10 IU/ml 0% 4%
Bourliere EASL 2015

Conclusions of ANRS HB06 PEGAN
Addition of a 48 weeks of PEGIFN α2a to NUCs therapy in HBeAg negative CHB patients with undetectable HBV DNA for at least one year, results in higher rates of HBsAg loss and HBs seroconversion.
Low baseline qHBsAg levels increase HBsAg loss and HBs seroconversion at week 96.
However, acceptability of such regimen in patients treated with NUCs is poor and discontinuation due to adverse events occurred in 20% of the patients.
Therefore, this combination should be proposed in a selected HBeAg negative CHB patients population.
56 Bourliere EASL 2015

Variable HR IC 95% p
HBV DNA negative 2.37 1.34 – 4.19 0.03
HBsAg <1000 IU/ml 49.4 6.76 – 361.02 <0.001
Multivariate analysis:Factors associated with HBsAg clearance
HBV DNA
Positive
Cu
mu
lati
ve
p
rob
ab
ilit
y
Cu
mu
lati
ve
p
rob
ab
ilit
y
Negative
≥ 1000 IU/ml
< 1000 IU/ml
HBs Ag
González-Diéguez EASL 2015
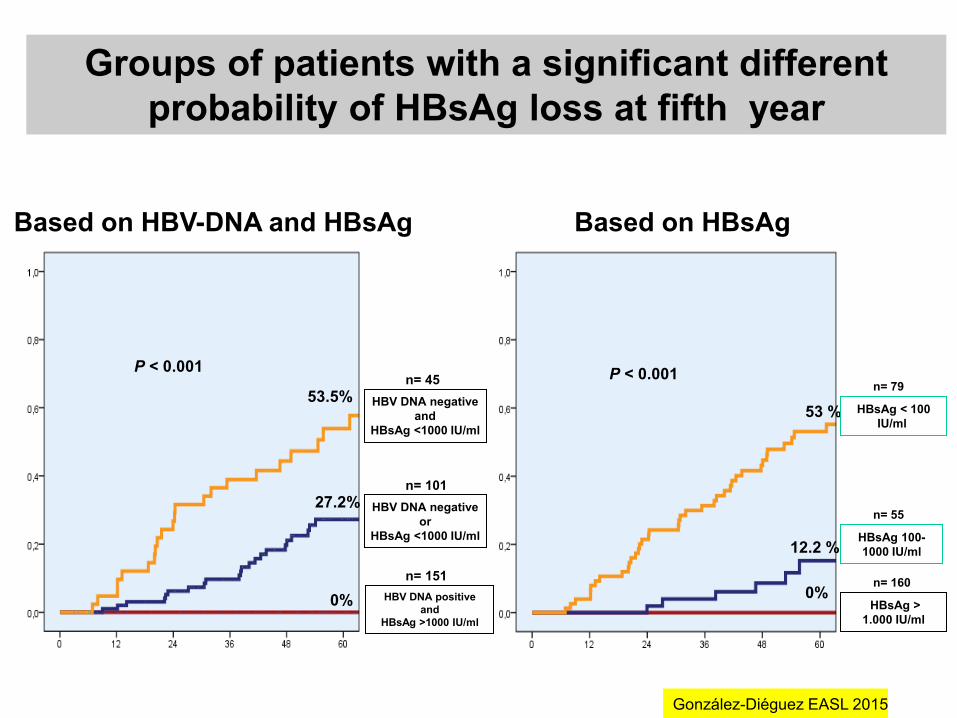
Groups of patients with a significant different
probability of HBsAg loss at fifth year
Based on HBsAg
n= 151
HBV DNA positive
and
HBsAg >1000 IU/mll
HBV DNA negative
and
HBsAg <1000 IU/mll
HBV DNA negative
or
HBsAg <1000 IU/mll
n= 101
n= 45 P < 0.001
53.5%
27.2%
0%
Based on HBV-DNA and HBsAg
53 %
12.2 %
0% n= 160
HBsAg >
1.000 IU/ml
HBsAg < 100
IU/mll
HBsAg 100-
1000 IU/ml
n= 55
n= 79 P < 0.001
González-Diéguez EASL 2015

77 Liiu EASL 2015

Conclusions part II
Discovery of HBsAg has revolutionized the diagnosis and
management of HBV infection
A highly sensitive HBsAg test that is able to detect most surface
region mutant is important to avoid false negative results
HBsAg quantification – Combined with viral load, improve the
management of chronic HBV infection
Serum HBsAg quantification can provide additional information on the
transcriptional activity and amount of cccDNA inside the liver
Low HBsAg level can identify inactive carriers and predict lower risk
of HCC
On-treatment HBsAg quantification can predict response to peg-
interferon
Monitoring of serum HBsAg level can potentially time the cessation of
oral antiviral therapy
Over 3 Million qHBsAg assays are used worldwide each
year = Prime time is here !

Thank you to my sAg Gurus
Henry Chan
Harry Janssen
Steve Locarnini
Pietro Lampertico
Seng-Gee Lim and the post-
EASL Singapore Viral
Hepatitis Meeting
79