
Harvesting of Saphenous Vein for Coronary Artery …161270/FULLTEXT01.pdf · Comprehensive...
55
Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1121 Harvesting of Saphenous Vein for Coronary Artery Bypass Grafting An Improved Technique that Maintains Vein Wall Integrity and Provides a High Early Patency Rate Domingos Sávio Ramos de Souza ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2002
Transcript of Harvesting of Saphenous Vein for Coronary Artery …161270/FULLTEXT01.pdf · Comprehensive...

Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1121
Harvesting of Saphenous Vein forCoronary Artery Bypass Grafting
An Improved Technique that Maintains Vein WallIntegrity and Provides a High Early Patency Rate
Domingos Sávio Ramos de Souza
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2002

Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1121
_____________________________ _____________________________
Harvesting of Saphenous Vein forCoronary Artery Bypass Grafting
An Improved Technique that Maintains Vein WallIntegrity and Provides a High Early Patency Rate
BY
DOMINGOS SÁVIO RAMOS DE SOUZA
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2002
Dissertation for the Degree of Doctor of Philosophy (Faculty of Medicine) in Thoracic Surgerypresented at Uppsala University in 2002
AbstractSouza, DR. 2002. Harvesting of Saphenous Vein for Coronary Artery Bypass Grafting. AnImproved Technique that Maintains Vein Wall Integrity and Provides a High Early PatencyRate. Acta Universitatis Upsaliensis. Comprehensive Summaries of Uppsala Dissertations fromthe Faculty of Medicine 1121. 49pp. Uppsala. ISBN 91-554-5232-9.
The primary aim of this thesis was to modify saphenous vein (SV) harvesting technique andevaluate its clinical importance. A new “no touch” (NT) technique of SV preparation wasdeveloped where the vein is harvested with a pedicle of surrounding tissue, which protects thevein from spasm therefore obviating the need for distension.
Firstly, a prospective randomised study in 156 patients who underwent coronaryartery bypass grafting was done to compare this new “no touch” technique to two others, theconventional (C) and the intermediate (I) techniques. A morphological study of the endotheliumshowed an endothelial integrity of 97% in NT vessels while about half of endothelial surface ofveins harvested by the other two techniques was devoid of endothelium. At angiographic followup, the patency for NT was 95.4%, 88.9% for grafts in group C and 86.2% for grafts in group I.A statistically significant difference in patency rate was found between the NT group and groupC (p=0.025) and the poorest result was observed in group I.
Secondly, the immunohistochemistry assessment using CD31-antibody confirmed a better-preserved endothelium for NT vessels. Putative NOS was identified by NADPH-diaphorasehistochemistry and autoradiographic localization of [3H] L-nitroarginine (NOARG) binding.NADPH staining was almost continuous on the luminal aspect and was also present in the intactadventitia of NT vessels, which was markedly reduced in conventionally harvested veins.Autoradiographic analysis of specific NOARG binding showed greater binding in the no-touchvessels, confirming the histochemistry results. All three NOS isoforms were identified in themedia of SV grafts. In NT, NOS I was abundant in adventitial nerves; NOS II was found inadventitial vasa vasorum and NOS III was associated with endothelial cells lining both the vessellumen and microvessels within the adventitia.
In conclusion, this study demonstrated that the endothelial integrity and NOS activity arebetter maintained when using the no-touch technique for vein graft harvesting. The vasorelaxantand thromboresistent activities of NO may be responsible for the reduced venospasm andimproved early patency rates observed. Furthermore, the mechanical properties provided by thecushion of surrounding tissue in grafts harvested by NT technique may contribute to theobserved high patency rate.
Key words: Saphenous vein, coronary bypass, endothelium, nitric oxide, patency rate.
Domingos R Souza, Department of Thoracic and Cardiovascular Surgery, Örebro UniversityHospital, SE-701 85 Örebro, Sweden.
Domingos Souza 2002
ISSN 0282-7476ISBN 91-554-5232-9Printed in Sweden by Uppsala University, Tryck & Medier, Uppsala 2002

“Imagination is more important than knowledge”
Albert Einstein
To Anette and my mother Julia.

iv
Papers
This thesis is based on the following papers, which will be referred to in the text by their roman
numerals:
I A New “No-touch” Preparation Technique. Souza D.
Scand J Thorac Cardiovasc Surg 1996;30:41-4.
II “No-touch” technique using saphenous vein harvested with its surrounding tissue for
coronary artery bypass grafting maintains an intact endothelium. Souza D.S., Christofferson
R.H., Bomfim V. and Filbey D.
Scand Cardiovasc J 1999;33(6):323-9.
III High early patency of saphenous vein graft for coronary artery bypass harvested with
surrounding tissue. Souza D.S.R., Bomfim V, Skoglund H, Dashwood M.R., Borowiec
J.W., Bodin L. and Filbey D.
Ann Thorac Surg 2001;71:797-800.
IV Preserved endothelial integrity and nitric oxide synthase in saphenous vein graft harvested
by a novel ”no-touch” technique. Tsui J.C.S., Souza D.S.R., Filbey D., Bomfim V. and
Dashwood M.R.
Br J Surg. 2001;88:1209-1215.
V Localization of nitric oxide synthase in saphenous vein grafts harvested with a novel ”no-
touch” technique: potential role of nitric oxide contribution to improved early graft patency
rates. Tsui J.C.S., Souza D.S.R., Filbey D. Karlsson M.G. and Dashwood M.R.
J Vasc Surg. 2002 In press.
VI Improved patency in vein grafts harvested with surrounding tissue: results of a randomized
study using three harvesting techniques. Souza D.S.R., Dashwood M.R., Tsui J.C.S., Filbey
D., Bodin L., Johansson B. and Borowiec J.
Ann Thorac Surg. Accepted for publication.
All reprints were made with kind permission from the publishers.
v
Abbreviations
ABC avidin biotinylated complex
CABG coronary artery bypass grafting
cGMP cyclic guanosine monophosphate
CI confidence interval
CX circumflex
DIAG diagonal
EDRF endothelium-derived relaxing factor
EF ejection fraction
eNOS endothelial NOS
ET-1 endothelin-1
FIH fibrointimal hyperplasia
IMA internal mammary artery
iNOS inducible NOS
LAD left anterior descending coronary artery
LIMA left internal mammary artery
NADPH nicotinamide adenine dinucleotide phosphate
nNOS neural NOS
NO nitric oxide
NOARG [3 H]-L-NG-nitroarginine
NOS nitric oxide synthase
OR odds ratio
PDA posterior descending coronary artery
PGI2 prostacyclin 2
SEM scanning electron microscopy
SMC smooth muscle cell
SV saphenous vein
TEA thrombendarterectomy
TEM transmission electron microscopy
UW University of Wisconsin
VEGF vascular endothelial graft factors

vi
Contents
Abstract ii
Papers iv
Abbreviations v
Introduction 1
Historical review of myocardial revascularization 1
Pathophysiology of vein graft failure associated with graft preparation 3
Vein wall 3
Vasoactive substances 3
Early vein graft occlusion 4
Fibrointimal hyperplasia 4
Ischemic damage 5
Altered local hemodynamics 5
Atherosclerosis 5
Vasospasm 5
Potential role of the adventitia in vein graft failure 6
Storage solution for graft preservation 7
Methods of reducing vein graft failure 8
Surgical techniques 8
Established adjuvant medical therapy 9
Emerging strategies 10
Pharmacological agents 10
Gene transfer 10
External stenting 11
Aims of the study 13
Material and methods 14
Patient selection 14
Randomisation 14
Harvesting techniques 14
Surgical aspects 15
Morphological assessment 15
Immunohistochemical assessments 16
Angiographic assessment 18
Statistical methods 19

vii
Results 21
Patient demographics 21
Morphological findings 22
Endothelial cell integrity 22
Qualitative SEM 23
Qualitative TEM 23
Immunohistochemical findings 24
Endothelium 24
Collagen 24
Autoradiographic localisation of NOS 24
NADPH-diaphorase histochemistry 25
NOS immunohistochemistry 26
Surgical data 26
Graft patency 27
Discussion 30
Patency rate 33
Surgical comments 34
General summary 36
Acknowledgements 37
References 39
Paper I 50
Paper II
Paper III
Paper IV
Paper V
Paper VI


1
Introduction
Coronary artery disease is the most important cause of morbidity and mortality in the
industrialized western world. Over one million people around the world die yearly from coronary
atherosclerosis (1). Coronary artery bypass grafting (CABG) that was developed in the 1960s
and in the 1970s, utilizing the saphenous vein graft, has dramatically changed the management
of patients with ischemic heart disease. There are three main reasons for CABG: a) to relieve
ischemic resistant to medical treatment, b) to prevent myocardial infarction and c) to increase a
productive life span (2). Although coronary bypass surgery has achieved these goals, the
degeneration of the venous graft with time is a major problem. All data indicates that the long-
term outcome of venous bypass grafts is poor and that one should strive to use alternative
methods. Virtually every synthetic and biologic alternative to arterial conduits or autologous
fresh saphenous vein has proved disappointing. Nowadays the use of arterial conduits, which
have a better long-term outcome, has become very common. Nevertheless, the saphenous vein is
still an important conduit for CABG. However, for saphenous vein grafts to remain useful as
stable and long-lasting coronary bypass conduits, the most important pathologic changes causing
graft failure, which are graft thrombosis and atherosclerosis, must be delayed or prevented.
Historical review of myocardial revascularization
The first experimental use of autologous vein grafts was reported by Goyannes, Carrell and
Guthrie (1905). Goyannes (1906) performed the first successful clinical vein autograft of
popliteal vein to bypass a popliteal aneurysm. Lexer (1907) performed the first free vein graft
using saphenous vein to restore continuity in an axillary artery following excision of a traumatic
aneurysm.
Surgical treatment for coronary artery disease began in the early 20th century. Experimental
techniques by Alexis Carrel (3) for directly anastomosing the aorta with the left anterior
descending coronary artery (LAD) failed, and indirect methods of myocardial revascularization
by Beck (4, 5) and later by Vineberg and Buller (6) increased only marginally the blood supply
to the myocardium.
In 1958 Manson Sones at The Cleveland Clinic performed the first selective coronary
angiography, which led to the application of direct myocardial revascularization (7). In 1962

2
Effler (8), was able to repair a tight narrowing of the left main trunk of the coronary artery by
using the patch graft technique developed by Senning (9). However, the mortality when applying
this technique was extremely high. In 1963 Sabiston performed a coronary bypass from the aorta
to the right coronary artery using an autologous saphenous vein (10). In 1965 Kolessov in Russia
performed the first anastomosis between LIMA and LAD (11).
In 1967 Favaloro successfully reconstructed the right coronary artery by interposing a segment
of SV and later on he started using SV graft direct from the aorta to the coronary arteries.
Afterwards, significant progress occurred when Favaloro and his group were able to perform
double bypass, emergency revascularization and even combined operation (12). Until 1970 they
had performed 1.086 CABG in 951 patients with an overall mortality of 4.2%. The promising
results from continuous observations were compiled by Sheldon et al (13, 14). The same year,
George Green started using the direct mammary coronary anastomosis. The first coronary bypass
operation in Sweden was performed in June 1970 at the Karolinska Hospital, Stockholm (15).
In the 1980s several studies published by Campeau (16, 17), Bourassa (18) and Grondin (19)
demonstrated that severe atherosclerotic deterioration of SV graft occurs between 6 and 11 years.
They proposed that aortocoronary surgery, with the use of saphenous vein grafts, should
eventually be reconsidered and suggested that modifications of harvesting techniques and
pharmacological intervention might improve the durability of aortocoronary vein grafts. At the
same time Loop (20), in a great number of patients, showed a clear advantage of using IMA over
the SV. A few years later he suggested (21) the benefit from expanded internal thoracic artery
grafting techniques by using bilateral, free and sequential anastomoses. Until 1980, only 13% of
the surgeons were using mammary grafts (22). Since the mid 80s the number of users has
increased steadily and today most surgeons employ them.
Due to the excellent results of the internal mammary artery grafts, surgeons looked for other
sources of arterial conduits. In 1987, Pym (23), Suma (24) and Attum (25) reported the first
studies on the use of the gastroepiploic artery for direct myocardial revascularization. In 1990,
Puig (26) introduced the use of inferior epigastric artery. In 1971, Carpentier introduced the
radial artery as an alternative conduit for CABG, however, the initial results were disappointing.
After the modification of the harvesting technique and with the use of peroperative calcium
channel blockers, the results were significantly improved (27, 28). Nowadays, the radial artery is
used at most cardiovascular centres around the world.

3
Despite the widespread use and superior patency of the LIMA and other arterial conduits, the
saphenous vein continues to be the most commonly used conduit for CABG. However, vein graft
failure is associated with recurrence of angina (16) and is one of the primary reasons for
reoperation. Early vein graft failure occurs in approximately 18% of saphenous vein grafts
within the first month of implantation and approximately 30% of SV grafts occlude within the
first year (29-31). At ten years, graft occlusion rates are more than 50% and the grafts that
remain patent frequently show angiographic luminal irregularity or narrowing. Thus, every effort
ought to be made to improve the patency rate of the SV grafts. Preparation of the graft is
important since there is direct evidence that surgical injury during vein preparation causes severe
intimal loss as well as biochemical and functional changes of the grafts (32).
Pathophysiology of vein graft failure associated with graft preparation
Vein wall
The wall of the vein is traditionally divided into three anatomic layers (tunica): the intima, the
media and the adventitia. The intima is the thin endothelial layer on the luminal surface of the
vessel. Beneath this lies the fenestrated basement membrane and occasional intimal cells. The
media comprises of smooth muscle cells arranged in an inner longitudinal and an outer
circumferential direction and are interlaced with collagen and elastic fibrils. The adventitia forms
the outer layer of the vein wall.
Vasoactive substances
Under normal conditions the endothelium continuously releases prostacyclin, PGI2, and the
endogenous nitrovasodilator (33) endothelium-derived relaxing factor, EDRF, which is identical
with nitric oxide (NO) (34, 35). Luminal released EDRF inhibits together with PGI2 platelet
activation, platelet adhesion and aggregation (36). Furthermore, EDRF protects the adjacent
smooth muscle from the simultaneous direct constrictor effects of humoral compounds released
from activated platelets. Endothelin-1 (ET-1) is a potent vasoconstrictor peptide produced by
vascular endothelial cells (37, 38). Veins are more sensitive to ET-1 than arteries are. Removal
of the endothelium enhances the sensitivity of smooth muscle to endothelin`s vasoconstriction
influence in veins, but does not affect smooth muscle of the arteries (39). In normal human
arteries, EDRF inhibits contractions induced by ET-1, whereas, in veins ET-1 only attenuates the
effects of EDRF and nitrovasodilators (40, 41).

4
This dominance of EDRF in the IMA has been proposed to contribute to the better patency rate
of arterial grafts as compared with SV grafts (42). Surgical preparation of the SV graft itself
results in a significant reduction in EDRF as compared with the freshly isolated vein and is
associated with marked denudation of the endothelium (43).
Early vein graft occlusion
The inevitable vascular trauma that occurs during vein harvest is thought to contribute to graft
failure. In particular, clinical evidence and data from animal studies suggest that endothelial
damage and/or dysfunction is associated with reduced graft patency. However, damage to the
tunica media and surrounding tissue of the vessel also occurs and recent observations (44, 45)
indicate that adventitial remodelling and subsequent effects on microvessels (vasa vasorum) and
vascular nerves may also be important in the pathophysiology of vein graft narrowing and
occlusion.
Morphological changes induced by harvesting and preparation are noted in all vein grafts. At
least some initial damage to the SV graft endothelium is inevitable and is aggravated by
subsequent exposure to arterial pressure (46, 47). One of the earliest findings is the insudation of
blood constituents including fibrin, erythrocytes, and neutrophils into the SV graft intima. This is
attributed to increased permeability of the endothelium and is observed consistently in all grafts
(48). In an animal study (49), the autologous vein grafts used as arterial replacement have shown
considerable damage to the endothelial cells during the process of grafting. The vessels were still
partly denuded of endothelium after four weeks. By 12 weeks and probably as early as six
weeks, a complete endothelial covering was present. Early vein graft thrombosis may be a result
of endothelial loss or damage in SV surgically prepared for coronary artery bypass grafting (50,
51). Loss of endothelium eliminates the physical and electrostatic barrier separating platelets
from subendothelial collagen, binding to which initiates platelet activation (52).
Graft failure is not only dependent on the quality of the conduit used but is also caused by poor
surgical technique and poor distal run-off of the coronary arteries (53, 54).
Fibrointimal hyperplasia
The majority of grafts that do not completely occlude exhibit some degree of fibrointimal
hyperplasia (FIH) by one month (55).

5
Ischemic damage
The etiology of the intimal and medial changes remains controversial. It has been suggested that
damage to the vasa vasorum during venous autograft distension with resultant ischemic, may be
an important mechanism promoting the subendothelial changes (56, 57). It has been
demonstrated (58) that medial fibrosis is induced whenever grafts were made ischemic by
interruption of vasa vasorum, and it is independent of intraluminal pressure. In contrast,
subjecting the grafts to arterial pressure produced intimal proliferation and fibrosis.
Altered local hemodynamics
Venous grafts within arterial systems are distended by pressures that cause increased
circumferential and radial stresses. Hydraulic distension was associated with mural thinning and
endothelial damage (59), but the implications of these findings remain unclear. Increased flow
velocity is associated with reduced development of FIH and atherosclerosis, and may thereby be
a factor of the higher long-term patency rate for IMA grafts (60). There is evidence supporting a
localized autoregulatory mechanism that senses shear stress and transduces that information into
a message to regulate luminal diameter (61). Further data suggests that this mechanism is
dependent on the presence of the endothelium that acts as the transducing element (62).
Autoregulatory malfunction may conceivably lead to excessive fibrointimal hyperplasia with
obstruction of the lumen.
Atherosclerosis
Initially vein grafts were thought to be resistant to the development of atherosclerosis (63), but
subsequent reports showed that atherosclerotic changes occur as early as three to six months
postoperatively (64, 65). The incidence of these lesions increases with time and may be as high
as 30% after three years (66). A detailed morphological study of vein grafts suggests that
virtually all SV grafts older than one year show atherosclerotic plaque formation (67). The
majority of SV grafts that occlude in the late postoperative period, i.e. five years or more after
grafting, develop a rapidly progressive form of atherosclerosis (68). There is evidence (69) that
endothelial damage stimulates migration and proliferation of smooth muscle cells into the intima,
which is a key event for development of atherosclerosis.
6
Vasospasm
Spasm may be a clinically important mechanism in the early and/or late occlusion of vein bypass
grafts (70, 71). Spasm of arterial and venous graft conduits may occur both during harvesting
and after the graft has been implanted (70). The cause of spasm of a vein during harvesting is not
well understood; there are many possible causes of vein spasm during CABG. Undoubtedly, the
most common one is surgical trauma, which can usually be minimized by a careful surgical
technique, when harvesting the artery as a pedicle rather than skeletonizing it. In the case of the
SV, the vessel is always skeletonized during harvesting and it is often subjected to surgical
trauma. Thus, unless specific pharmacologic measures are taken, the SV is always in spasm after
harvesting. In general, spasm of vascular graft conduits is best managed by prevention rather
than treatment after spasm has occurred (72).
Potential role of the adventitia in vein graft failure
The tunica adventitia is the outermost layer of blood vessels and since it gradually merges with
the loose connective tissue surrounding the vessel, this region is usually removed during
conventional harvesting of saphenous veins for use as bypass conduits. In medium sized veins,
such as the saphenous vein, the adventitia consists of longitudinally oriented bundles of smooth
muscle cells, collagen fibres and networks of elastin fibres. Fibroblasts, macrophages and
unmyelinated nerves are also found within the adventitia of medium and large sized veins.
Adventitial microvessels form the vasa vasorum, which are responsible for providing oxygen
and nutrients to the walls of large vessels. The vasa vasorum of veins penetrate much closer to
the intima than the vasa vasorum of arteries and this is particularly evident in the saphenous vein
(73). Damage to the adventitia and the structures within it may contribute significantly to vein
graft occlusion. The vasa vasorum has been shown to be associated with the long-term
development of neointimal hyperplasia in vein grafts (74), and also with tissue healing around
saphenous vein grafts (75). Damage to vasa vasorum in vein grafts may result in vessel wall
hypoxia with subsequent neointima formation, similar to the observation in arteries where
occlusion of vasa vasorum leads to neointima formation and atherosclerosis (76, 77).
The vascular nerves located within the tunica adventitia of blood vessels are disrupted during
bypass surgery. The innervation of veins differs from that of arteries. Consequently, there will be

7
major differences between the saphenous vein graft and the host artery with respect to
neurogenic factors (78). Arteries remain under a degree of vascular tone that is influenced by the
autonomic nervous system. Apart from classical compounds, such as acetylcholine,
noradrenaline and serotonin, there is an increasing list of vasoactive transmitters including NO,
which affect vasomotor tone of arteries and veins. The autonomic vascular nerves within the
adventitia penetrate the adventitia tunica media to release neurotransmitters that regulate
vasomotor tone.
Adventitial fibroblasts have also been suggested to be involved in neointimal formation and
vessel occlusion (79, 80). There is evidence for adventitial remodelling following vascular
damage, such as that caused during vein graft surgery. An increase in adventitial mass, due
mainly to the proliferation of fibroblasts has been described. More recently, it has been
suggested that fibroblasts from the adventitia are the progenitors of neointima (79). The
neointima may then progress, resulting in atherosclerotic changes in the vein wall, causing the
neointima to be called “soil for atheroma” (81).
Fig 1. Reproduced from Gutterman DD. Adventitia-dependent influences on vascular function. Am J Physiol1999;277(4 part 2):H1265-72.
Storage solution for graft preservation
Several solutions have been used as a storage medium for the preservation of SV after
harvesting. The important role of the temperature and the type of solution used for graft
preservation is well recognized (82). However, there is no ideal solution for rinsing, distending

8
and storing the saphenous vein prior to its implantation. Although, as there is yet no universal
agreement on this subject, the superiority of blood over crystalloid solutions for the preservation
of endothelial and medial SMC morphology has been suggested (54, 83). It has been
demonstrated that the preservation of endothelium was better in autologous heparinized blood
than in heparinized saline solution. However, the best preservation of the endothelium was
observed with Bretschneider`s solution compared to all other solutions tested (84). Plasma–Lyte
solution at 37°C has been recommended as a venodilating storage solution during coronary
bypass operations to optimise vein graft relaxation before implantation (85). A widespread study
showed that vessel storage in heparinized blood maintained good contractility the first 24 hours
and EDRF was effective for a period of up to 12 hours. University of Wisconsin solution (UW)
and Perfadex gave good preservation for 24 hours. Euro-Collins solution was not a suitable
solution for long-term preservation of blood vessels. Vessels stored in Krebs solution, the only
solution containing calcium, manifested no reduction in contractility throughout the 36-hour test
period. Considering the excellent results obtained with Krebs solution regarding contractility, it
was suggested that the addition of calcium to UW and Perfadex would improve their ability to
preserve smooth muscle cell function during prolonged storage (86). However, another study has
shown specific potentially detrimental effects of UW solution on the endothelium and smooth
muscle function of isolated SV (87).
Methods of reducing vein graft failure
Various methods have been attempted to reduce vein graft occlusion. Besides the established
adjuvant therapy, modifications of the surgical technique for the preparation of the SV graft and
emerging strategies are currently being used. All these methods are aimed to reduce early platelet
activation, prevent excessive neointimal proliferation and avoid lipid deposition.
Surgical techniques
Routinely, graft preparation includes dissection of the vein from its bed, ligation of side
branches, flushing and distension of the lumen to overcome spasm and to identify leaks (54, 88).
Endothelial injury results from direct mechanical trauma (53) and stretching as a result of
luminal distension (89, 90). Impaired fibrinolytic activity, caused by uncontrolled distension of
saphenous vein prior to its use as a vascular conduit, may contribute to early vein graft
thrombosis, and can be avoided by using controlled distension to <120 mmHg (91).

9
In 1977, an endothelium preserving technique without touching the vein during the anastomosis
was described (92). In 1980 it was recommended that the vein should be harvested by a ”no-
touch” technique to minimize manipulation, side branch ties should be placed away from the SV
wall, veins should be immersed in cold blood and distension above 100mmHg was to be avoided
(93). Prevention of endothelial damage in veins was demonstrated by applying pharmacologic
relaxation of the vessel that allows a gentle dilatation with low, controlled pressure (90). Based
on this principle, it was suggested that the SV preparation should incorporate subcutaneous and
perivenous infiltration with papaverine, atraumatic dissection, controlled gradual distension, and
storage of the vein in cold heparinized blood (89). The use of glyceryl trinitrate-verapamil
solution both topically and intraluminally was introduced in 1993 as a very effective and safe
combination to promote relaxation of the vein during preparation (94). Thus, various atraumatic
techniques have been described to reduce vein damage during harvesting and implantation. All
these techniques avoid high-pressure distension, but mechanical distension is still generally
required, and adventitial damage still occurs due to stripping of the perivascular tissue.
Our ”no-touch” technique consists of retaining the cushion of surrounding tissue that both
prevents venospasm, thereby obviating the need for distension, and protects the vein from direct
handling by surgical instruments even during performing the anastomoses.
Established adjuvant medical therapy
Adjuvant pharmacological interventions have been introduced in an attempt to improve graft
patency. Post-CABG, anti-platelet agents and lipid-lowering agents are the established strategies
for reducing vein graft occlusion. A multicenter study showed that Aspirin improves graft
patency at one year after bypass graft surgery, and the major benefit occurred in vein grafts
placed to smaller vessels (95). The same authors (96) found in a prospective, randomized
double–blind, placebo study that both IMA grafts and vein grafts had excellent patency rates at
one year. Aspirin did not alter this at one year, and there were no differences in patency between
IMA grafts and vein grafts when they were anastomosed to the LAD. Consistent beneficial
effects of other anti-thrombotic agents have yet to be established (97). A recent study
demonstrated that aggressive reduction of low density lipoprotein cholesterol with lovastatin
significantly reduces the rate of vein graft occlusion assessed by angiographic follow-up (98).

10
Emerging strategies
Pharmacological agents
There is evidence that nitric oxide (NO) synthesis is impaired at areas of vascular injury and that
the NO system is involved in graft failure (99, 100). Particularly, early vasospasm and
thrombotic occlusion may be due to reduced endothelial NO activity in vein grafts. NO is an
endothelium-derived factor synthesized by the enzyme, nitric oxide synthase (NOS), from L-
arginine. It is a potent vasodilator with other vasoprotective properties. NO prevents platelet and
leukocyte adhesion, inhibits vascular smooth muscle proliferation and migration, and
demonstrates antioxidant activity. NO donors, such as S-nitrosoglutathione have been
investigated in vein grafts and were found to cause vasodilation (101) and to inhibit platelet
deposition.
Compounds that reduce neointimal hyperplasia are also being investigated as potential
pharmacological approaches for preventing vein graft occlusion. Thapsigargin is a compound
that increases cytosolic Ca++ by its action as an irreversible inhibitor of Ca++ -ATPase.
Intracellular calcium pools are important in regulating vascular smooth muscle migration, a
prerequisite for neointimal hyperplasia. Pre-treatment with thapsigargin ex vivo reduces
neointima formation in cultured SVs (102) although the effects of exposing saphenous veins to
thapsigargin before implantation have not been studied in vivo.
Oral and intramuscular administration of rapamycin, a macrolide antibiotic with anti-mitotic
properties, has also been found to reduce neointimal formation after balloon-induced vascular
injury in porcine models (103, 104).
Whilst these approaches have been shown to reduce neointima formation in experimental
models, their clinical potential has yet to be demonstrated.
Gene transfer
Vascular gene therapy is a new area of investigation and the use of gene transfer to reduce
intimal hyperplasia and subsequent graft failure is receiving considerable attention. The use of
gene transfer is attractive since it may potentially produce long-term therapeutic benefit without
systemic side effects. Promising genes currently being evaluated include genes for NOS and
VEGF. NOS gene transfer may prevent vein graft failure by locally increasing NO synthesis in
grafts.

11
Three isoforms of NOS have been identified: endothelial NOS (eNOS), inducible NOS (iNOS)
and neuronal NOS (nNOS). Several animal studies using liposomal, adenoviral or retroviral
delivery of eNOS to injured arteries have demonstrated a reduction in intimal hyperplasia (105,
106). iNOS gene transfer also inhibits intimal hyperplasia in animal models (107), and since
iNOS produces greater levels of NO compared to eNOS, the viral load required with iNOS gene
transfer to achieve the same levels of NO should be reduced, which may be advantageous in
clinical settings.
VEGF is a potent angiogenic factor, which promotes endothelial cell regrowth following
vascular injury via a NO dependent mechanism. Early vascular gene transfer studies using
VEGF have focused on its potential in therapeutic angiogenesis in both myocardial and lower
limb ischemic (108, 109). In animal models of arterial injury, recombinant VEGF accelerated re-
endothelialization and reduced intimal hyperplasia (110).
Direct intravascular delivery of target genes to vein grafts is possible when using endovascular
techniques (111). It is unclear whether intravascular delivery of genes to the intima or
extravascular targeting of the adventitia will be more effective. For example, a recent animal
model using saphenous vein grafts interposed in femoral artery has shown that ex vivo adventitial
liposomal transfection of the eNOS gene is more effective at inducing NOS activity than
transfection of the intimal surface (112).
Whilst new developments are being made in this area, results are mainly limited to data from
animal studies and there is little information from controlled trials, and long-term effects remain
unknown.
External stenting
The stenting procedure has been introduced as a strategy to prevent late graft failure. Placement
of a non-restrictive external stent around a porcine vein graft prevents early neointima formation
and medial thickening (113, 114). The mechanisms underlying this effect are unclear and are
under investigation. Initially, it was believed that the external stent reduces the pulsatile stretch
and shear forces to which the arterialised vein graft is exposed. This would reduce the generation
of endothelium- and tissue-derived vasoactive factors with prothrombotic and proliferative
properties. Placement of an external stent also promotes angiogenesis in the adventitial region of
the graft (30) and this may improve oxygenation to otherwise hypoxic regions of the graft.

12
Effects on the levels of the adventitial vasoactive factors, such as NO, PGI2 and ET-1 may also
be potential mechanisms (99, 115, 116). There is evidence that PGI2 and cGMP are conserved at
medial/intimal regions of stented vein grafts and that adventitial formation of these compounds is
increased (99). NOS content and activity within the adventitia of stented grafts is also higher
than in unstented grafts (99).

13
Aims of the study
The aims of the present thesis were:
– to develop a ”no-touch” technique of harvesting SV for CABG, in which a cushion of
surrounding tissue is left around the vein, to prevent spasm and the deleterious effects of
contraction and distension.
– to compare the morphologic endothelial integrity of SV harvested by ”no-touch”,
conventional and intermediate techniques.
– to determine the endothelial integrity and the endothelial availability of nitric oxide
synthase (NOS) in SV harvested by the “no-touch” and conventional techniques.
– to identify and quantify the distribution in the SV graft wall of the three NOS isoforms in
veins harvested by the ”no-touch” and conventional techniques.
– to determine, by angiography, the early patency rate of SV graft harvested by ”no-touch”,
conventional and intermediate techniques.

14
Material and methods
Patient selection
Initially, 156 patients who underwent CABG at the Department of Cardiothoracic Surgery,
University Hospital, Örebro, were randomly allocated to three groups of 52 patients, according
to three techniques of harvesting the SV. The primary inclusion criteria were chosen in order to
be able to follow up the patients during a long-term period. The operations were performed from
June 1993 until April 1997 (papers I, II, III and VI).
In papers IV and V, saphenous vein samples were obtained from ten consecutive patients
undergoing CABG at the same department as mentioned above. Neither randomization nor any
exclusion criteria were used and the operations were performed between November and
December 1999.
Randomization
Patient randomization was performed by the standard method as described by Altman (117).
Briefly, the three harvesting techniques were randomly allocated a number and patient selection
was performed in numeric order after the inclusion criteria was determined and fulfilled.
Harvesting techniques
Group C - Conventional technique: The SV was exposed by a continuous longitudinal incision,
the adventitial layer was stripped and side branches were ligated with 3-0 silk. The vein was
removed from the leg immediately after dissection and was manually distended with saline at
300 mmHg for 1 min, using a syringe connected to a manometer. After distension, the vein was
stored in saline at room temperature.
Group I - Intermediate technique: The SV was dissected as in group C. Instead of manual
distension the vein was subjected to the following procedure: It was left in situ and covered by
sponges moistened with saline-papaverine solution (1mg/mL) until extracorporeal circulation
was started. The vein was then removed and stored in blood obtained from the patient’s aortic

15
cannula before cooling. Despite the use of papaverine, almost all vein grafts required gentle
mechanical distension to overcome residual spasm.
Group NT- ”No-touch” technique: The SV was also exposed using a continuous incision. All
visible side branches were ligated approximately 0.5 cm from the vein wall with 3-0 silk
ligatures. Then the vein, together with a 1 cm cushion of surrounding tissue, was isolated from
its bed (paper III, fig 1). The vein was left in situ covered with sponges moistened in saline until
extracorporeal circulation was started. The vein was then stored in blood collected from the
patient’s aortic cannula before cooling.
Surgical aspects
Cardiopulmonary bypass with moderate hypothermia (28-30°C) and cold blood intermittent
retrograde cardioplegia (4°C) was routinely used. Malleable calibrated probes were used to
measure the diameter of target coronary arteries. In all groups the distal anastomoses were
performed first. To check for leakage the proximal end of the grafts in the group NT and I were
briefly connected to the arterial cannula of the cardiopulmonary bypass. The grafts were
therefore neither flushed nor dilated with a syringe. However, in the conventional group, leakage
was checked manually using a syringe and saline. All LIMAs were anastomosed to the LAD.
The proximal anastomosis was performed after release of the aortic cross clamping. Veingraft
characteristics, such as quality and origin (distal, medial and proximal part) were taken into
consideration and recorded. The graft blood flow rate was also routinely measured by ultrasonic
transit time (Research flowmeters, Transonic Systems Inc. USA).
Morphological assessment
In paper II, the assessments consisted of scanning electron microscopy (SEM) and transmission
electron microscopy (TEM) examination of vein specimens from 10 consecutive patients from
group C, I and NT. A control specimen was taken from the distal end of the SV immediately
after removal. These control or primary specimens were neither dilated nor stored, but
immediately fixed by the same technique. Thus, it was considered that any fixation artefacts that
could have affected endothelial integrity would be present in all groups. Ten specimens were
indiscriminately chosen from group C, I and NT. Upon completion of the proximal anastomosis,
the vein segment which was not used as a graft, was flushed with heparinized saline and a 5 mm

16
segment was taken as a secondary specimen. One half was processed for SEM and the other for
TEM. The samples were collected, fixed by immersion in 2% paraformaldehyde and 2.5%
glutaraldehyde in Millonig’s buffer.
Examination for SEM of ten specimens, nine primary specimens together with a secondary
specimen, from each patient in all three groups were analysed at a magnification of x 406 (700
µm2) to observe individual endothelial cells. Four fields were sampled systematically at random
from each specimen to obtain mean value estimations. The four fields were grouped around the
specimen’s geometrical center without overlapping. Analysis was done by reading a field at a
time into an image analysis programme (Synoptocis Ltd., Cambridge, UK). Areas devoid of
endothelium were outlined on a digitizer pad. The data were given in percent (excluded area in
pixels/total area in pixels). All measurements were made by the same investigator in a blinded
fashion. Furthermore, 20 randomly sampled fields from the total of 160 were analysed twice for
agreement.
Examination for TEM of the 12 specimens (three secondary specimens from each group plus
three primary specimens) were prepared by postfixation in 1% osmium tetroxide in phosphate
buffer and embedding in Agar 100 epoxy resin (Agar, Cambridge, UK). Ultrathin sections were
analysed and contrasted with uranyl acetate and lead citrate and observed in a Hitachi H 7100
TEM at 75 kV (paper II).
Immunohistochemical assessments
In papers IV and V, each patient had the proximal part of the vein harvested with its surrounding
tissue using the ”no-touch” technique, while the distal part was stripped of the surrounding tissue
and dilated with saline at pressures of 300 mmHg for 1 min using a syringe connected to a
manometer, i.e. conventional technique. Both segments were stored in heparinized blood until
anastomosis was done. Samples of excess vein graft on completion of the proximal anastomoses
were then taken from each segment. In study V, control samples were taken from the stripped
part of the vein without distension.
A standard immunohistochemical technique with the avidin-biotinylated complex (ABC) method
was used to identify endothelial cells and collagen. Sections were fixed in acetone and
endogenous enzyme activity was inhibited with normal goat serum to block background staining.
17
The tissue was incubated in either CD31 antibody to identify endothelial cells or by a mouse
monoclonal antibody to identify collagen. Then biotinylated secondary goat antibody was
applied and finally sections were incubated with streptavidin biotinylated horseradish peroxidase
solution. 3,3’-diaminobenzidine tetrahydrochloride was used as the chromogenic substrate
solution and the sections were counterstained with Mayer’s haematoxylin and prepared for
microscopic examination (paper IV).
Quantitative assessment of endothelium using CD31 staining on vessel sections was carried out
using a Kontron Zeiss 400 imaging system (Karl Zeiss Imaging, Cambridge, UK). This was
performed on vessels from all 10 patients and three sections per vein segment were used. The
amount of positive luminal immunostaining was measured via a Polaroid CCD camera (Photonic
Science, Cambridge, UK) attached to a Nikon E800 microscope (Nikon UK, Kingston, UK) at x
40 magnification. The lumen perimeter was measured and endothelial integrity (positive CD31
staining) expressed as a percentage of the lumen length (paper IV and V).
In vitro autoradiography was used to study NOS sites using [3 H]-L-NG-nitroarginine (NOARG).
Slides were pre-incubated in Tris HCl buffer and then transferred and incubated in buffer
containing radioactive 10 nM NOARG. The degree of non-specific binding was determined by
incubating adjacent sections in the presence of an excess concentration of unlabelled L-arginine.
After incubation slides were washed and then dried in air. Sections were then post-fixed in
paraformaldehyde and were then dipped under darkroom conditions in molten nuclear emulsion
and allowed to dry overnight. Slides were then placed in racks in lightproof boxes, sealed and
stored at 4oC for 12 weeks after which the emulsion was processed following the manufacturer’s
instructions. Tissue was then stained with Mayer’s haematoxylin and eosin, microscopically
examined under dark-field and bright-field illumination and photographed where appropriate
(paper IV).
NADPH-diaphorase histochemistry was used to localize NOS on tissue sections (paper IV and
V). Slide-mounted sections were fixed in paraformaldehyde. They were then rinsed in
phosphate-buffered saline (PBS), dried in cold air and incubated with 1 mg/mL NADPH (Sigma-
Aldrich, Poole, Dorset, UK) and 0.1 mg/mL nitroblue tetrazolium (Sigma) in PBS buffer at
37oC. Negative controls were incubated in the absence of NADPH. The reaction was stopped by
removing the incubation solution and rinsing the sections in running tap water for 5 min.
Sections were then stained with 0.1% eosin for 3 min and prepared for microscopic examination.

18
NOS isoforms were studied using rabbit polyclonal anti-NOS antibodies to localize NOS I, NOS
II and NOS III (paper V). Here, an ABC alkaline phosphatase method was used. Briefly, primary
antibodies to NOS I, NOS II and NOS III were added and, after rinsing in PBS, biotinylated
universal secondary antibody was added followed by incubation in avidin and biotinylated
alkaline phosphatase H solution. After rinsing sections in water, alkaline phosphatase activity
was revealed by alkaline phosphatase substrate. Sections were counterstained with Mayer’s
haematoxylin, prepared for microscopic examination, visualised and photographed.
NADPH-diaphorase staining of whole sections representing total tissue NOS was quantified to
assess the relative amount of NOS present in the different vein segments. Quantification was
performed using a Zeiss KS400 image analysis system. Here, haematoxylin-stained transverse
vein sections were captured at x100 magnification using a ProgRes 3012 camera attached to a
Zeiss Axioplan microscope. Three sections of each SV segment (conventional, control and ”no-
touch”) were analysed from all ten patients. All observations were carried out in a blinded
fashion. Data from each segment were presented as mean ± SEM % staining of total tissue area
relative to the ”no-touch” sections from the same vein (paper V).
Angiographic assessment
Selective graft angiographies were made according to Judkins technique (118). Low osmolarity
Vispaque contrast medium (Nycomed Amersham AB, Stockholm) was used. Both the SV graft
and LIMA were visualised in 2 projections. The angiographic assessment was performed in a
blinded way by one radiologist. Angiography was assessed as graft patency and degree of
localised and/or diffuse changes. Occlusion was identified by visualization of a remaining stump
by selective injection or by lack of opacification after a 50 mL bolus injection of dye in the
ascending aorta.

19
Statistical methods
In paper II, the Kruskal-Wallis non-parametric analysis of variance was used, with posterior tests
for comparisons between treatment groups and the control group as described by Siegel and
Castellan (119).
In paper III, the difference in frequency of occluded and non-occluded grafts was analyzed with
chi-square tests in the case of univariate analysis and logistic regression models when two or
more explanatory variables were considered. The actual calculations were performed with the
statistical programs StatXact and LogXact (Cytel Software Corporation, Cambridge, MA. USA)
which are especially designed for analysis of small samples.
In paper IV, the results are presented as median (range). Statistical analysis was performed with
a two-tailed Wilcoxon signed rank test.
In paper V, analysis of variance and Bonferroni adjustment multiple comparison tests were
performed with GraphPad Prism version 3.02 for Windows.
In paper VI, patency of graft was analyzed with logistic regression models. The main
explanatory factor was the three different harvesting techniques: conventional, intermediate and
”no-touch”. Additional explanatory factors were examined individually and those showing a
significant relation to the outcome and also having an uneven distribution across the three
harvesting techniques were selected and used in the final model. Calculations were performed
with consideration of the fact that there was more than one graft per patient. The p-values and
confidence intervals shown are in this way corrected for problems with correlated observations
and confounding factors.
The outcome parameter of interest in the logistic regression model is the odds ratio (OR). An OR
of 1.0 indicates no effect in the analyzed category compared with the chosen reference category.
OR above 1.0 indicates increased chance for patency, OR below 1.0 less chance. As occlusion is
a relatively rare event the OR approximates the relative risk well in this study. Before reaching
the final model we examined the possibility that the chosen explanatory factors had significant
interactions, in particular with the main predictor variable, the harvesting technique. In the final
model we also calculated the goodness-of-fit of the model to the observed data by using the
likelihood ratio criterion. Basic references for our modelling approach are Rogers (120) and
Cnaan, Laird & Slasor (121).
For all analyses, statistical significance was inferred at p <0.05.

20
Results
Patient demographics
Patients included in paper I, II, III and VI are from the same initial population, and patients’
demographics can be seen in table 1. No major differences in patient characteristics were
observed between the groups. Patients who were on lipid-lowering drugs on admission or had
serum cholesterol concentration above the normal range (2.6 – 5.0 µmol/L) were considered to
have hyperlipidemia. Hypertension was defined as a diastolic blood pressure above 90 mmHg
and/or systolic blood pressure above 140 mmHg. The left ventricular function was determined
by the ejection fraction (EF).
Table 1. Patient characteristics.
Operational technique
Patient characteristic Conventional Intermediate “No-touch”
Number of patients, n 46 41 45
Female/Male 6/40 8/33 7/38
Age at surgery, Mean (range) 58 (45 – 70) 60 (41 – 71) 58 (43 – 67)
Preoperative infarct, n (%) 29 (63%) 16 (39%) 25 (56%)
Preoperative ejection fraction (EF) Mean (range) 63 (41 – 81) 67 (39 – 87) 67 (40 – 86)
Hyperlipidemia, n (%) Preoperative 18 months after surgery
29 (63%)22 (48%)
19 (46%)20 (49%)
29 (64%)27 (60%)
Smoker, n (%) Preoperative 18 months after surgery
9 (20%)9 (20%)
4 (10%)1 (2%)
9 (20%)6 (13%)
The anti-platelet drug, Aspirin, was started on the day after the operation with a dose of 160
mg/day. At the time of the angiographic examination, 42 patients in group C were receiving 160
mg/day, three had 75 mg/day and one was not on antiplatelet drug therapy. In group I, 35
patients were taking 160 mg/day, four had 75 mg/day and two were not on drug therapy. In
group NT, 35 patients were receiving 160 mg/day; seven patients 75 mg/day and three were not
taking any anti-platelet drug.

21
In papers IV and V the mean age of the ten patients was 66 (range 57-81) years. Two were
females. Three were smokers. There was one insulin-dependent diabetic and one non-insulin
dependent diabetic. All ten patients were on Aspirin, nine were on β-blockers and anti-
hypertensives and eight were on lipid-lowering medication.
Morphological findings
Paper I was designed to describe in detail the new ”no-touch” SV harvesting technique. It also
gave the preliminary results of the morphologic investigation of the endothelial integrity by
using SEM, which indicated that preservation of endothelial integrity was better with the new
”no-touch” technique, fig 2 and 3.
Fig. 2. SEM from “no-touch” graft. Theendothelium is intact, and the endothelial cells(E) exhibit prominent cell borders (arrows)and microvilli, indicating a preservedmetabolic activity at the moment of fixation.
Fig. 3. SEM from conventional harvestingtechnique. The summoned effect of mechanical,chemical and thermal trauma duringpreparation is observed as the loss ofendothelial cell (E) integrity.
Endothelial cell integrity
The morphological data of quantitative SEM are shown in paper II, fig 2. Secondary specimens
in group NT had an endothelial cell integrity similar to that of their primary specimens. In
contrast, roughly half of the luminal surface of secondary specimens from group C was devoid of
endothelium. The secondary specimens in group I exhibited endothelial cell integrity between
the secondary specimens of group C and NT. A significant difference between groups was
found. The posterior tests between the control specimens and each of the three treatment groups
resulted in the following p-values, control versus conventional p<0.01, control versus
intermediate p<0.05 and control versus “no-touch“ p>0.50.

22
Qualitative SEM
In primary specimens from all three groups, the endothelium was essentially intact with
prominent nuclear bulges and microvilli. The picture was similar in secondary specimens from
group NT. In preparations from the conventional procedure, patchy areas of endothelial
denudation were frequently found, usually with adherent and activated platelets, which
confirmed the preliminary findings of paper I. The secondary specimens from group I, exhibited
less extensive endothelial cell damage than the secondary specimens from group C. In five
specimens, the section surface had hit venous vasa vasorum in the graft wall that was continuous
with the graft lumen (paper II, fig 4).
Qualitative TEM
In all three procedures, areas in which the endothelium was well fixed could be found, with
intact mitochondria and parallel membranes in the granular endoplasmic reticulum (paper II, fig
6a). In the primary specimens from all three groups and the secondary specimen from group NT,
the endothelium was continuous and attached to the basal membrane. In the secondary specimen
from group C, discontinuous endothelium was frequently observed with detached endothelial
cells separated from the basal membrane (paper II, fig 6b). Again, secondary specimens from
group I represented a morphological intermediate between the other two groups.
Immunohistochemical findings
Endothelium
The CD31 immunostaining, identifying endothelial cells, shown in paper IV and V, confirmed
that the endothelial cell integrity of “no-touch” grafts was well preserved, whereas in
conventionally harvested veins it was reduced. Apart from a reduction in the luminal
endothelium of veins prepared using the conventional technique, immunostaining of the
endothelial cells of the vasa vasorum within the adventitia was also decreased compared to
abundant staining in segments of ”no-touch” saphenous vein (paper IV, fig 3).
Collagen
Collagen immunostaining showed the intact adventitia surrounding vessels harvested using the
”no-touch” technique and revealed microvessels within this area. This was absent in segments of
SV prepared with the conventional technique (paper IV, fig. 2).
23
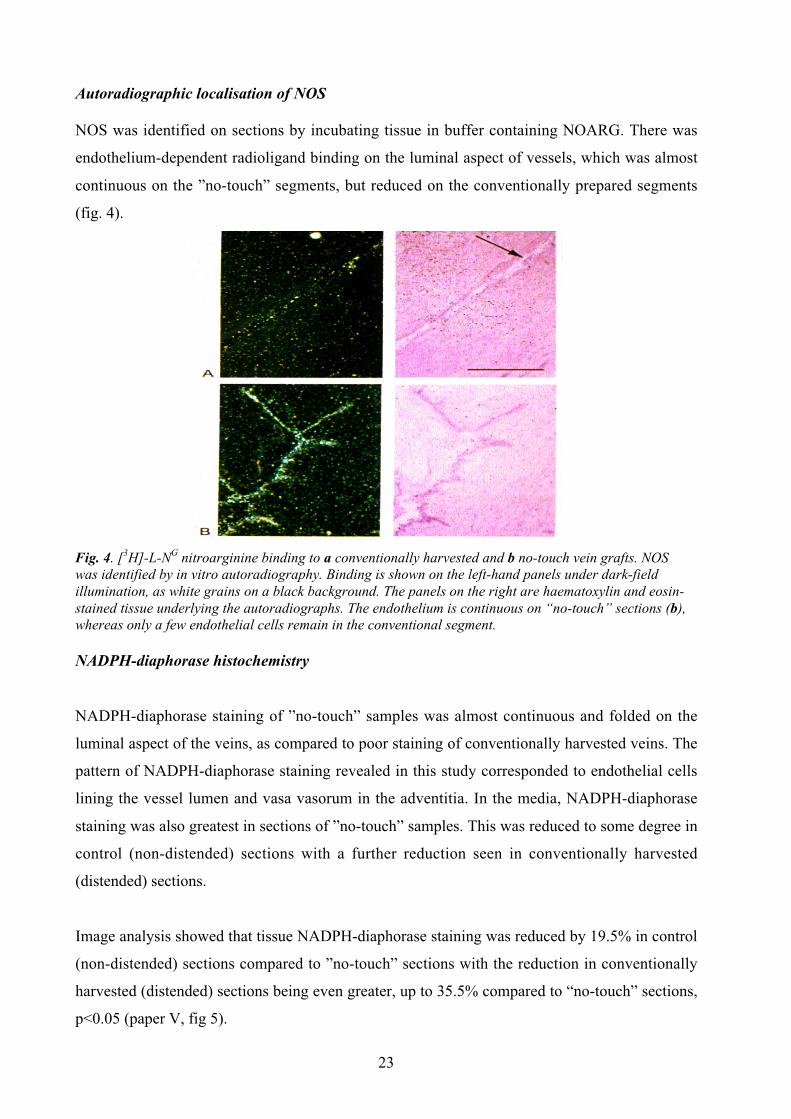
Autoradiographic localisation of NOS
NOS was identified on sections by incubating tissue in buffer containing NOARG. There was
endothelium-dependent radioligand binding on the luminal aspect of vessels, which was almost
continuous on the ”no-touch” segments, but reduced on the conventionally prepared segments
(fig. 4).
Fig. 4. [3H]-L-NG nitroarginine binding to a conventionally harvested and b no-touch vein grafts. NOSwas identified by in vitro autoradiography. Binding is shown on the left-hand panels under dark-fieldillumination, as white grains on a black background. The panels on the right are haematoxylin and eosin-stained tissue underlying the autoradiographs. The endothelium is continuous on “no-touch” sections (b),whereas only a few endothelial cells remain in the conventional segment.
NADPH-diaphorase histochemistry
NADPH-diaphorase staining of ”no-touch” samples was almost continuous and folded on the
luminal aspect of the veins, as compared to poor staining of conventionally harvested veins. The
pattern of NADPH-diaphorase staining revealed in this study corresponded to endothelial cells
lining the vessel lumen and vasa vasorum in the adventitia. In the media, NADPH-diaphorase
staining was also greatest in sections of ”no-touch” samples. This was reduced to some degree in
control (non-distended) sections with a further reduction seen in conventionally harvested
(distended) sections.
Image analysis showed that tissue NADPH-diaphorase staining was reduced by 19.5% in control
(non-distended) sections compared to ”no-touch” sections with the reduction in conventionally
harvested (distended) sections being even greater, up to 35.5% compared to “no-touch” sections,
p<0.05 (paper V, fig 5).

24
NOS immunohistochemistry
Positive NOS III immunostaining was identified on the luminal aspect of vessels, that was
almost continuous on ”no-touch” and control sections, but reduced and patchy on conventional
sections (paper V). All three isoforms were identified in the media, contributing to the positive
NADPH-diaphorase staining. In the intact adventitia of ”no-touch” vessels, abundant NOS III
positive staining was associated with microvessels, and this coincided with positive CD31
staining. These microvessels also stained positive for NOS II. NOS I immunostaining was
associated with adventitial perivascular nerves.
Surgical data
Paper III and VI. The mean duration of cardiopulmonary bypass and aortic cross clamp time was
121 minutes (range 59-187) and 64 (range 34-95) minutes respectively for group C; 126 (range
90-180) and 69 (range 41-117) respectively in group I; 139 (range 88-195) and 72 (range 41-
113) respectively in group NT. The majority of patients in all groups received three vein grafts
and a mammary artery. A total of 127 vein grafts and 41 LIMA grafts were inserted in group C.
In group I, a total of 116 vein grafts and 35 LIMA grafts were used and in group NT, a total of
124 vein grafts and 42 LIMA grafts were implanted. There were 107 single grafts, 16 double
sequential grafts and four triple sequential grafts in group C. In group I, 100 single grafts 14
double sequential grafts and two triple sequential grafts were used and in group NT we had 109
single grafts and 15 double sequential grafts. LIMA grafts were considered not suitable in five
patients in group C, five in group I and three in group NT. It was necessary to perform
thrombendarterectomy (TEA) in two posterior descending coronary artery (PDA) in group C,
one PDA in group I, but no TEA was necessary in any coronary artery in group NT.
No operative mortality occurred in the three groups. Peroperative myocardial infarction occurred
in two patients in group C. There was one reoperation to control postoperative bleeding
performed in one patient in group NT, where the source of the bleeding was from the LIMA bed.
Only minor wound complications were seen in a few cases in all the three groups. Two of 46
patients (4.3%) in group C, Three of 41 patients (7.3%) in group I and five of 45 (11.1%) in
group NT developed superficial infection or cellulitis. We had no major complication that
required subsequent surgical intervention
25
Graft patency
One hundred and thirty-two patients, 46 patients from group C, 41 from group I and 45 from
group NT underwent an angiographic follow-up. The time to angiography was 17.2 (SD ±4.4)
range 9-31 months for group C, 16.0 (SD ±2.6) range 11-25 months for group I and 16.3 (SD
±2.7) range 11 – 28 months for group NT. The remaining 24 patients declined further
angiographic assessment.
The results of the NT group were first reported in paper III. The patency rate was 118/124
(95.4%) for vein grafts and 39/42 (93.3%) for LIMA. In this study there were two surgical
factors that affected the outcome of the vein graft. The occlusion was statistically significant
when related to the size of the coronary artery (p=0.03) and to the quality of SV before
harvesting (p=0.02). However, other surgical factors such as the quality of the recipient target
arteries, the graft length and the graft flow rate did not play an important role in the graft
occlusion. When we compared the flow rate to the size of the coronary arteries we found a trend
toward graft occlusion (24%) for those grafts anastomosed to small coronary arteries (1 mm)
with a flow rate of ≤20 mL/min. However, all grafts that were anastomosed to 1 mm arteries and
had a flow rate of more than 20 mL/min or those that had a flow rate of ≤20 mL/min but were
anastomosed to arteries of ≥1.5 mm were patent (paper III, table 1). No association between vein
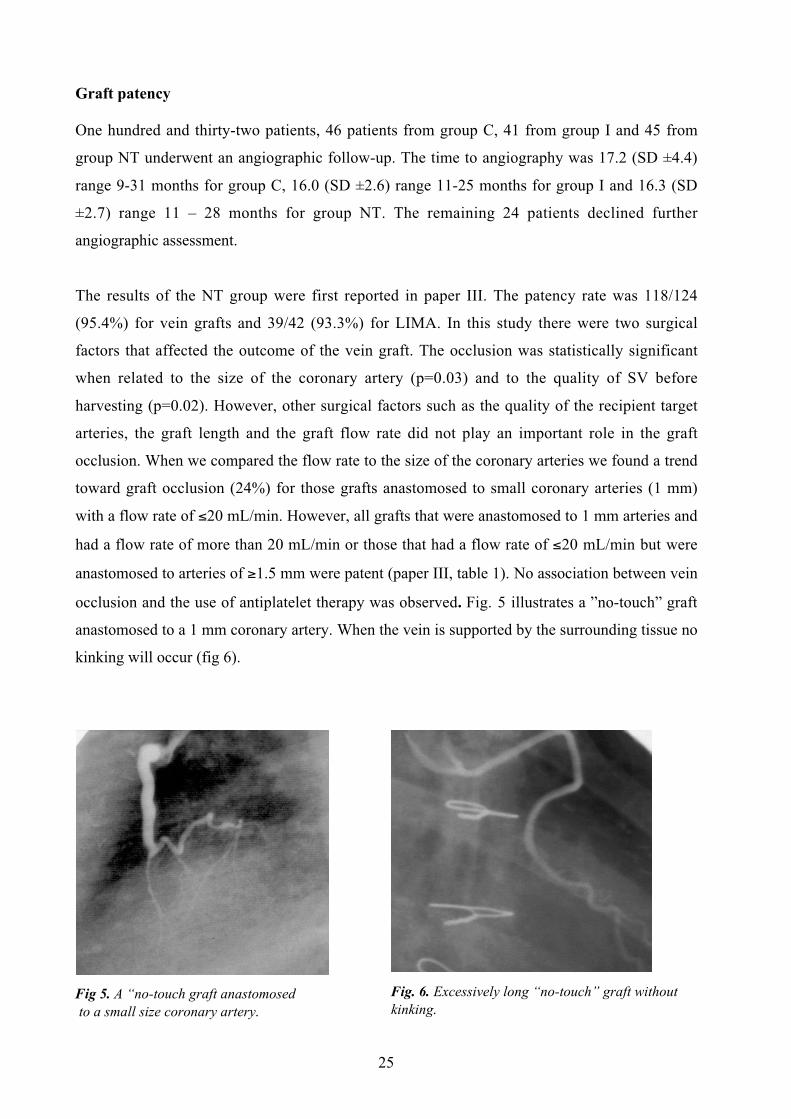
occlusion and the use of antiplatelet therapy was observed. Fig. 5 illustrates a ”no-touch” graft
anastomosed to a 1 mm coronary artery. When the vein is supported by the surrounding tissue no
kinking will occur (fig 6).
Fig 5. A “no-touch graft anastomosed to a small size coronary artery.
Fig. 6. Excessively long “no-touch” graft withoutkinking.

26
Paper VI shows the final angiographic results performed in 132 patients from all three groups.
The patency for NT was 118/124 (95.4%), for grafts in group C was 113/127 (88.9%) and for
grafts in group I was 100/116 (86.2%). The patency for LIMA was 108/118 (91.5%).
Low flow associated with small size coronary artery increased the occlusion rate in all groups
and by itself had a greater effect on the occlusion rate for grafts in group I. The quality of target
coronary artery did not influence the patency in any group, and both grafts which were
anastomosed to PDA after TEA in group C were open but the graft in group I was not. The
occlusion rate for veins of poor quality prior to implantation was 4/10 (44.4%) in group C, 6/19
(31.6%) in group I and 3/29 (10.3%) in group NT.
All sequential grafts in the NT and I groups were open whilst in group C two sequential grafts
were totally occluded and two others were partially occluded. Thus, 47/51 (92.2%) of all
sequential grafts were completely open.
A logistic regression analysis of the most important factors that affected the graft outcome, i.e.
the patency rate are shown in paper VI, table 3. A statistically significant difference in patency
rate was found between the NT group and group C (p=0.025) and the poorest result was
observed in group I. The odds ratio (OR) for ”no-touch” in comparison with group C was 3.9
with a 95% confidence interval (CI) of 1.2 to 12.6. The analysis showed high OR for increasing
coronary artery diameter (OR 4.7 for diameter ≥2.0 mm compared with 1.0 mm) and increased
flow (OR 4.9 for flow ≥41 ml/min compared with ≤20 ml/min). Poor vein quality gave a low
odds ratio (OR 0.2). Odds ratios of 0.2 were observed for central and proximal parts compared
with distal parts of the vein. All these parameters were based on multivariate adjustment and
were statistically significant.
No association between vein occlusion and classical clinical factors which are reported to
influence the graft patency such as age, preoperative infarctions, cholesterol level, smoking
habits or hypertension was observed in any group.

27
Discussion
For many reasons both the SV and the LIMA will continue to be the most important conduits in
CABG. The high incidence of vein graft occlusion is a major and unsolved problem in
myocardial revascularization. Improvement of SV graft patency rate is therefore a big challenge
in the field of cardiovascular surgery. The widespread use of complete arterial grafting with
LIMA and other arterial conduits cannot yet be justified on scientific grounds, as there are few
late survival data and no controlled studies (122, 123).
This is the first study to show that the surrounding tissue of the SV contributes to a high early
patency rate of SV grafts compared to SV graft prepared with conventional technique.
Different structural and functional properties between arteries and veins are probably the
explaination for the better results of the arterial grafts (124). Nevertheless, the trauma to the SV
wall that occurs during its harvesting for CABG may also contribute to the poor results of
venous grafts. At the time of implantation, endothelial damage is almost absent in internal
mammary artery (IMA) grafts. In contrast, the endothelium of harvested human saphenous vein
shows greater thrombogenic defects with exposed collagenous fibrils (125). It was shown (126)
that although the smooth muscle proliferation was similar in undamaged saphenous vein and
IMA, muscle proliferation was significantly greater in damaged veins. This implies that the
greater intimal proliferation seen in saphenous vein grafts may arise not from intrinsic
differences in arterial and venous smooth muscle cells but from a greater susceptibility to injury.
In an animal model, free internal mammary artery that was stripped from its surrounding tissue,
showed a higher incidence of thrombosis, intimal thickening, and medial injury than the pedicled
grafts did (127).
Many strategies have been used both to prevent vein occlusion and to improve the short- and
long-term patency rate. Apart from established adjuvant medical therapy, new pharmacological
agents, gene therapy, and also mechanical devices are presently undergoing evaluation. Many of
these strategies have shown to be promising in experimental vein bypass models, but a few have
successfully been transferred into clinical practice. In addition, an important point is the
continuing improvement of surgical techniques to prevent vein wall damage during harvesting
and implantation.

28
Harvesting the saphenous vein together with a pedicle of surrounding tissue protects the vein
from spasm, thereby obviating the need for vein distension. The cushion of surrounding tissue
allows for careful handling of the vein, from harvesting to implantation. Our results suggest that
this technique could be an additional strategy to improve vein graft patency. Papers I and II show
that this new ”no-touch” technique results in excellent maintenance of endothelial cell integrity,
as measured by SEM. However, with the other two techniques there was extensive damage to the
endothelial layer. TEM permitted analysis of both endothelial integrity and the morphology at
the subcellular level. The ”no-touch” technique provided a more gentle approach to the handling
of SV, which was confirmed by a continuous layer of endothelial cells showing better attachment
to the basal membrane in comparison with the other two techniques.
We could demonstrate that the adventitia and the cushion of surrounding tissue, that remains
intact after harvesting by the ”no-touch” technique, has high collagen content. This may act as a
buffer against the pulsatile stress that the graft is exposed to, and it works in a similar manner as
an external stent (paper IV). There is evidence, that even in the absence of intraluminal blood
flow, the vasa vasorum maintained endothelial integrity, and that the endothelium is very
sensitive to the loss of the vasa vasorum (56). Thus, the endothelial surface of an arterialized
vein bypass is probably nourished by both the luminal blood and through the vasa vasorum blood
supply. In paper II, we found that the vasa vasorum drains into the lumen, so it is possible that
arterial blood from the lumen to some extent perfuses retrogradely through the vasa vasorum,
thereby decreasing ischemic damage.
NADPH-diaphorase staining and NOARG binding, as indicators of putative activity, suggest that
NOS availability is also preserved on the luminal endothelium of grafts harvested by the ”no-
touch” technique. Veins harvested by this technique may maintain their nitric oxide-producing
capacity in vivo, which could reduce the incidence of vein occlusion by promoting
vasodilatation, reducing platelet aggregation and preventing thrombus formation. Apart from
being located on the luminal endothelium, NOS was also found in microvascular endothelium
within the adventitia.
The alterations in NOS distribution of SV harvested by the ”no-touch” technique was
demonstrated and compared to that of veins harvested with the conventional technique. In
addition to the preservation of NOS associated with luminal endothelial cells, NOS in the media
and adventitia of ”no-touch” vessels was also preserved. In the adventitia, NOS sources were

29
identified, and they were associated with microvessels and perivascular nerves. NOS levels were
not only reduced by removal of the surrounding tissue from the SV but also by distension, which
suggests that both of these measures contribute to the reduction in NOS levels seen in
conventionally harvested vessels. Distension appears to have a greater effect on luminal
endothelial and medial NOS, whilst removal of perivascular tissue eliminates important
adventitial NOS sources. This preservation of NOS sources suggests that NO availability, which
is usually reduced by conventional surgical preparation (43), may be improved by using the ”no-
touch” technique, and that the NO pathway contributes to the improved results of SV harvested
by this new technique.
During surgery and in the immediate postoperative period, venospasm is often encountered and
NO donors have been shown to reduce venospasm via their vasodilator action (128).
Preservation of adequate endogenous NO may provide protection against venospasm; no
significant venospasm occurs intraoperatively when using the ”no-touch” technique. This
precludes the need for distension and resultant vascular damage. The protective mechanism
against venospasm may be maintained during the early postoperative period, and counteract any
effects of endogenous vasoconstrictors to which the vein graft is highly sensitive (129-131).
All three NOS isoforms were identified in the media of SV grafts, where NO production would
modulate vessel tone. NOS I, II and III expression in vascular smooth muscle has been
previously reported (132-135), and has been thought to be particularly important following
vascular injury where NOS III-derived NO may be reduced due to endothelial cell injury. In ”no-
touch” vessels, NOS I was abundant in adventitial nerves; NOS II was found in adventitial vasa
vasorum; NOS III was associated with endothelial cells lining both in the vessel lumen and in the
microvessels within the adventitia. The potentially beneficial involvement of all three isoforms
of NOS supports data from studies showing that all isoforms are vasculoprotective. NOS I,
produced by perivascular nerves has been shown to modulate vascular tone of cerebral arteries
(136), and may play a similar role in the saphenous vein, causing vasodilation. NOS III reduces
intimal hyperplasia in NOS III-knockout mice (137) and NOS III-transgenic mice studies (138).
Similar studies, using the carotid artery ligation model in NOS II-knockout mice, have described
suppressed constrictive remodelling by this isoform (137). The presence of these isoforms in
”no-touch” vessels may reduce both intermediate and late occlusions via attenuation of intimal
hyperplasia and constrictive vascular remodelling.

30
Patency rate
The early patency rate of saphenous veins harvested with its surrounding tissue is very high
(95.4%), even in saphenous vein grafts that demonstrated low blood flow. Such a high patency
rate has not been demonstrated when using other harvesting techniques. We investigated whether
a cushion of surrounding tissue might improve venous graft patency rate by comparing early
angiographic results between the ”no-touch” and two other techniques. There was a significant
improvement of vein graft patency using this new ”no-touch” technique over the other
techniques (p=0.02).
When the vein is stripped from its surrounding tissue, the accurate adjustment of the length of
the graft is an important technical aspect, as kinking will certainly occur if the graft is too long.
Many techniques have been applied for dealing with aortocoronary graft length to prevent kinks
and twists in the graft (139). The preservation of the surrounding tissue when using the NT
technique protects the vein graft, and prevents such complications to occur.
Because endothelial injury is inevitable when the SV is handled by the conventional harvesting
technique, the use of antithrombotic therapy should also be started preoperatively with a dose of
325 mg /day of Aspirin (140). In the present study we started to use Aspirin the day after the
operation at a low dose of 160 mg/day. At the time of the angiographic assessment, some
patients were on a dose of only 75 mg/day, and a few patients were not using Aspirin at all. On
the basis of our results, pharmacological inhibition of platelet function has not been found to be
of major importance in preventing vein graft occlusion, if the SV endothelium remains intact
during harvesting and implantation.
The intermediate group was devised to demonstrate the importance of the surrounding tissue to
vein grafts, since after dissection, the handling of the SV vein was identical to that of the ”no-
touch” group, except that the vein in the intermediate group was stripped. Removal of
surrounding tissue generally resulted in pronounced spasm, and mechanical distension was
required despite local application of papaverine. In contrast, grafts retaining a pedicle of
surrounding tissue required neither pharmacological relaxation nor mechanical distension.
The ”no-touch” group provides both the best endothelial protection and the highest patency rate.
However, an unexpected finding was that veins harvested conventionally showed a higher
patency rate than the intermediate technique, despite our previous observation that the

31
endothelial lining is better protected in the intermediate group than it is in the conventional group
(141). This suggests that it is not only the endothelial layer that plays an important role in
protecting the grafts from occlusion, but also that the adventitial layer makes a significant
contribution to improved graft patency.
In paper III, the quality of the vein before its harvesting was an important factor in determining
the fate of the graft (p<0.002). This is in agreement with another study (142), which shows that
many of the changes are present prior to grafting and may be important in graft failure. The
incidence of occlusion rate was also statistically significant (p<0.03) when taking into account
the size of the coronary artery. Other registered surgical and clinical factors did not contributed
to vessel occlusion.
In paper VI, in agreement with another study (143), the graft flow rate and diameter of the lumen
of the target coronary arteries are important factors in predicting the outcome of the grafts,
irrespective of the method of vein harvesting used. We corroborate a previous study, which
reported an improved patency rate for sequential grafts (144). Poor vein quality had an important
effect on the occlusion rate for all groups. Thus, when analysing all groups together, not only the
size of coronary arteries and the quality of the vein before implantation, but also the graft flow
rate, the segment of the vein and the technique of harvesting the SV were important factors in
determining the outcome of the grafts. In agreement with a recently published article (145),
traditional cardiovascular risk factors for arteriosclerosis did not seem to predict the early fate of
SV grafts. However, it is likely that atherosclerotic changes will become more evident at long-
term follow-up.
Surgical comments
The “no-touch” technique can be used in most patients, but in our experience it is more difficult
to accomplish in obese patients, or if the vein is situated superficially. So far, we have not
experienced problems regarding reoperation for bleeding from unligated side branches. The
likelihood to miss an unligated side branch is greater in the vein segment from the thigh than
from the calf region. Therefore we use, in most cases, the proximal vein to the right coronary
artery branches, as it is easier to deal with bleeding side branches if the graft is placed in front of,
or on the right side of the heart. With regards to damage to the saphenous nerve a double blind
study was performed in 22 patients of which 8 had veins harvested by the conventional

32
technique. The sensory impairment around the wound was found in both groups but it was more
pronounced in patients from the ”no-touch” harvesting technique. However, none of the patients
complained about neurological disturbances that affected their quality of life.
No major wound complication occurred and we attribute this to our exclusion criteria and the
meticulous surgical technique used. However, it is expected that wound complications are more
likely to occur in patients who have their veins harvested by the ”no-touch” technique; therefore
we recommend some approaches to avoid serious complications. Firstly, it is imperative to apply
a surgical technique as presented in paper I, and not perform it on patients at risk, in particular
those with peripheral vascular disease. Secondly, we suggest whenever possible, to perform a
preoperative SV mapping using ultrasonographic imaging the day before surgery, whereby the
course of the vein in the leg can be marked on the overlying skin. This will allow us to make the
incision exactly above the vein, avoiding a long flap of subcutaneous tissue, which might be a
major cause of wound complication. Also excessive use of electrocautery is an important cause
of postoperative complications. The operation time is somewhat longer using the ”no-touch”
technique than the other two techniques. Inasmuch as the success of bypass grafting procedures
is critically related to the quality of the conduit, the extra time and effort required are warranted.
In conclusion, the technique of harvesting the SV has a great influence on the fate of the venous
graft. This thesis is based on a novel harvesting technique of SV preparation for CABG, whereby
the vein is protected by its cushion of surrounding tissue. The adventitial layer and the structures
contained within the cushion of surrounding tissue possess both mechanical and functional
properties that protect the vein from spasm and ischemia. The endothelial integrity was better
maintained using the ”no-touch” technique. NOS activity was preserved on the endothelium, and
from both neuronal and adventitial microvessel sources, suggesting that NO availability is
retained by these grafts. The vasorelaxant and thromboresistent activities of NO may be
responsible for the reduced venospasm, and the observed improved early patency rates. In
contrast, removal of surrounding tissue results in spasm and mechanical distension is often
required, even when vasodilators are used during harvesting. This compromises endothelial,
medial and adventitial integrity, and influences the short-term and also probably the long-term
success of venous graft in CABG. In addition, the surrounding tissue supports excessively long
vein grafts and prevents kinking. Whilst short-term results are encouraging when using the ”no-
touch” technique, long-term results remain to be established.
33
General summary
The findings in the present series of studies can be summarized as follows:
– Retaining a cushion of surrounding tissue has provided a better conduit for SV graft by
protecting the vein from spasm and obviating the need for distension.
– The endothelial integrity was much better preserved in veins harvested by the ”no-touch”
technique than in veins harvested by the other two techniques.
– Both the endothelial integrity and the availability of NOS in SV graft were higher in
veins harvested by the ”no-touch” technique than in veins harvested by the conventional
technique.
– All NOS isoforms, as well as their distribution throughout the vein wall, were present and
better preserved in SV graft harvested by the ”no-touch” technique.
– The early patency rate assessed by angiography was found to be higher in veins harvested
by the "no-touch" technique than the other two techniques, and the difference was
statistically significant.

34
Acknowledgements
I wish to express my sincere gratitude to a large number of people, who with their help, support
and encouragement during my introduction into the field of research, have made this thesis
possible. I would particularly like to thank:
Derek Filbey, co-supervisor, and incredible friend. For the privilege and the pleasure of working
with you during my research experience. You were in the front position, you were always
available, you let me share your great experience in research, and you gave me strong support.
Your generosity is larger than yourself, and I cannot be grateful enough. I am also grateful to
your wife, who let me spend so much time with you, working with my thesis. Gun-Britt, thank
you, and thank you for your delicious cakes!
Vollmer Bomfim, co-supervisor, co-author and friend. For introducing me into the field of
cardiothoracic surgery, and for inviting me to work with you in Sweden. You gave me
inspiration and excellent conditions to perform my research. You also provided me your great
experience as a surgeon and researcher.
Jan Borowiec, head-supervisor from Uppsala University. Ever since you became involved with
my thesis, you have been a great support. Your help, experience in research and your knowledge
in this field of work made it possible for me to continue and finish what I had started.
Michael Dashwood, co-author, and “amigo”. Luckily I met you at a scientific meeting just at the
right time. Your scientific contributions to my work gave substance and depth and have been of
crucial importance. You introduced me into the field of nitric oxide and intoxicated me with your
knowledge. Janice Tsui, co-author and friend. You inspired me in my work and without your
expertise the results would be far poorer.
My co-authors, Rolf Christofferson, Lennart Bodin, Helge Skoglund, Mats G. Karlsson and
Benny Johansson for all the fruitful discussions and practical help.
Asgrimur Ragnarsson for the angiographic analyses and the nurses at the Radiology Department,
who spent hours with my patients during the angiographies.

35
Birger Wandt, my colleague, for your knowledge, your encouragement, good advice and
“forcing” me to go on when times seemed difficult.
Jane Strand, Laila Örtensjö, Eva Norgren-Holst and Ulla-Britt Lindqvist for helping me to take
care of the patients, for helping me to administrate all data, and to Margaretha Sandin, for your
secretarial skills.
The Staff of the operating theatres, particularly the assisting nurses, for your incredible patience
and hard work, for your accuracy with the surgical protocols and for your cheerful
temperaments. Also, my gratitude to the doctors and nurses at the Department of
Anaesthesiology for your contributions.
My colleagues at the Department of Cardiothoracic Surgery for your patience while assisting me
at surgery, all the way from harvesting to implantation of the “fat vein”.
My family, my deceased father José Martins and especially my mother Julia for their support
throughout my life. Also, my daugther Letícia.
Most of all I want to thank my family: my beloved, Anette, for your support and love, for all
your efforts at work and at home that has made this possible. To our children, Johanna, Josef
and Filip, who patiently have seen all this work taking place. Thank you, I love you all.
The expert help from the staff at the Medical Library, a special thanks to Margareta Gawell for
her database searches and compilations.
Lars-Göran Jansson at the Department of Medical Photography, for providing me with your
excellent work every time I needed.
Last but not least, I want to thank both Örebro University Hospital’s Medical Research
Committee and Mälarsjukhus in Eskilstuna for their support by supplying grants to cover some
of this work.
36
References
1. Eisenberg MS. The problem of sudden cardiac death. In: Eisenberg MS, Hallstrom AP,
editors. Sudden Cardiac Death in the Community. New York: Praeger, 1984:2.
2. Rahimtoola SH. Coronary bypass surgery - a perspective. In: Rahimtoola SH, Brest AN,
editors. Coronary Bypas Surgery. Philadelphia: F A Davis, 1977:11.
3. Carrel A. On the experimental surgery of the thoracic aorta and the heart. Ann Surg
1910;52:83-95.
4. Beck CS. The development of a new blood supply to the heart by operation. Ann Surg
1935;102:801-13.
5. Beck CS, Leighninger DS. Operations for coronary artery disease. JAMA 1954;156:1226-
33.
6. Vineberg A, Buller W. Technical factors which favor mammary-coronary anastomosis
with report of forty-five cases of human coronary artery disease thus treated. J Thorac
Surg 1955;30:411-35.
7. Sones Jr FM, Shirey EK. Cine coronary arteriography. Mod Concepts Cardiovasc Dis
1962;31:735-8.
8. Effler DB, Groves LK, Sones Jr FM, Shirey EK. Endarterectomy in the treatment of
coronary artery disease. J Thorac Cardiovasc Surg 1964;47:98-108.
9. Senning A. Strip grafting in coronary arteries. Report of a case. J Thorac Cardiovasc Surg
1961;41:542-9.
10. Sabiston DCJ. Direct surgical management of congenital and acquired lesions of the
coronary circulation. Prog Cardiovasc Dis 1963;6:299-316.
11. Kolessov VI. Mammary artery-coronary artery anastomosis as method of treatment for
angina pectoris. J Thorac Cardiovasc Surg 1967;54:535-44.
12. Favaloro RG. Surgical treatment of coronary arteriosclerosis. Baltimore: Williams &
Wilkins, 1970.
13. Sheldon WC, Sones FJ, Shirey EK, Fergusson DJ, Favaloro RG, Effler DB. Reconstructive
coronary artery surgery: postoperative assessment. Circulation 1969;39:I61-6.
14. Sheldon WC, Favaloro RG, Sones FMJ, Effler DB. Reconstructive coronary artery
surgery. Venous autograft technique. JAMA 1970;213:78-82.
15. Ekestrom S. Aorto-koronar bypasskirurgi 1970--77 vid toraxkirurgiska kliniken, KS.
Lakartidningen 1978;75:4479-81.
16. Campeau L, Enjalbert M, Lesperance J, Vaislic C, Grondin CM, Bourassa MG.
Atherosclerosis and late closure of aortocoronary saphenous vein grafts: sequential

37
angiographic studies at 2 weeks, 1 year, 5 to 7 years, and 10 to 12 years after surgery.
Circulation 1983;68:1-7.
17. Campeau L, Enjalbert M, Lesperance J, Bourassa MG, Kwiterovich PJ, Wacholder S, et al.
The relation of risk factors to the development of atherosclerosis in saphenous-vein bypass
grafts and the progression of disease in the native circulation. A study 10 years after
aortocoronary bypass surgery. N Engl J Med 1984;311:1329-32.
18. Bourassa MG, Enjalbert M, Campeau L, Lesperance J. Progression of atherosclerosis in
coronary arteries and bypass grafts: ten years later. Am J Cardiol 1984;53:102C-107C.
19. Grondin CM, Campeau L, Lesperance J, Enjalbert M, Bourassa MG. Comparison of late
changes in internal ammary artery and saphenous vein grafts in two consecutive series of
patients 10 years after operation. Circulation 1984;70:208-12.
20. Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, et al.
Influence of the internal-mammary-artery graft on 10-year survival and other cardiac
events. N Engl J Med 1986;314:1-6.
21. Loop FD, Lytle BW, Cosgrove DM. New arteries for old. Circulation 1989;79:I40-5.
22. Miller DW, Ivey TD, Bailey WW, Johnson DD, Hessel WA. The practice of coronary
bypass surgery in 1980. J Thorac Cardiovasc Surg 1981;81:423-7.
23. Pym J, Brown PM, Charrette EJ, Parker JO, West RO. Gastroepiploic-coronary
anastomosis. A viable alternative bypass graft. J Thorac Cardiovasc Surg 1987;94:256-9.
24. Suma H, Fukumoto H, Takeuchi A. Coronary artery bypass grafting by utilizing in situ
right gastroepiploic artery: basic study and clinical application. Ann Thorac Surg
1987;44:394-7.
25. Attum AA. The use of gastroepiploic artery for coronary artery bypass graft: another
alternative. Tex Heart Inst J 1987;14:289-92.
26. Puig LB, Ciongolli W, Cividanes GV, Dontos A, Kopel L, Bittencourt D, et al. Inferior
epigastric artery as a free graft for myocardial revascularization. J Thorac Cardiovasc Surg
1990;99:251-5.
27. Acar C, Jebara VA, Portoghese M, Fontaliran F, Dervanian P, Chachques JC, et al.
Comparative anatomy and histology of the radial artery and the internal thoracic artery.
Implication for coronary artery bypass. Surg Radiol Anat 1991;13:283-8.
28. Acar C, Jebara VA, Portoghese M, Beyssen B, Pagny JY, Grare P, et al. Revival of the
radial artery for coronary artery bypass grafting. Ann Thorac Surg 1992;54:652-9.
29. Izzat M, West R, Bryan A, Angelini GD. Coronary artery bypass surgery: current practice
in the United Kingdom. Br Heart J 1994;71:382-5.

38
30. Mehta D, Izzat MB, Bryan AJ, Angelini GD. Towards the prevention of vein graft failure.
Int J Cardiol 1997;62 Suppl 1:S55-63.
31. Schroeder TV. The TASC supplement - international recommendations for management of
peripheral artery disease. Eur J Vasc Surg 2000;19:563.
32. Mills NL, Everson CT. Vein graft failure. Curr Opin Cardiol 1995;10:562-8.
33. Griffith TM. Studies of endothelium-derived relaxant factors (EDRF), its nature and mode
of action. Eur Heart J 1985;6:37-49.
34. Palmer RMJ, Ferrige AJ, Moncada S. Nitric oxide release accounts for the biological
activity of endothelium-derived relaxing factor. Nature 1987;327:524-6.
35. Furchgott RF. Endothelium-derived relaxing factor: discovery, early studies, and
identification as nitric oxide. Biosci Rep 1999;19:235-51.
36. Radomski MW, Palmer RMJ, Moncada S. Comparative pharmacology of endothelium-
derived relaxing factor, nitric oxide and prostacyclin in platelets. Br J Pharmacol
1987;92:181-7.
37. Clozel M, Fischli W. Human cultured endothelial cells do secrete endothelin-1. J
Cardiovasc Pharmacol 1989;13 Suppl 5:S229-31.
38. Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, et al. A novel
potent vasoconstrictor peptide produced by vascular endothelial cells. Nature
1988;332:411-5.
39. Miller VM, Komori K, Burnett JCJ, Vanhoutte PM. Differential sensitivity to endothelin in
canine arteries and veins. Am J Physiol 1989;257:H1127-31.
40. Luscher TF, Diederich D, Siebenmann R, Lehmann K, Stulz P, von Segesser L, et al.
Difference between endothelium-dependent relaxation in arterial and in venous coronary
bypass grafts. N Engl J Med 1988;319:462-7.
41. Yang ZH, Diederich D, Schneider K, Siebenmann R, Stulz P, von Segesser L, et al.
Endothelium-derived relaxing factor and protection against contractions induced by
histamine and serotonin in the human internal mammary artery and in the saphenous vein.
Circulation 1989;80:1041-8.
42. Luscher TF, Yang Z, Tschudi M, von Segesser L, Stulz P, Boulanger C, et al. Interaction
between endothelin-1 and endothelium-derived relaxing factor in human arteries and veins.
Circ Res 1990;66:1088-94.
43. Angelini GD, Christie MI, Bryan AJ, Lewis MJ. Surgical preparation impairs release of
endothelium-derived relaxing factor from human saphenous vein. Ann Thorac Surg
1989;48:417-20.

39
44. Barker SG, Tilling LC, Miller GC, Beesley JE, Fleetwood G, Stavri GT, et al. The
adventitia and atherogenesis: removal initiates intimal proliferation in the rabbit which
regresses on generation of a 'neoadventitia'. Atherosclerosis 1994;105:131-44.
45. Gutterman DD. Adventitia-dependent influences on vascular function. Am J Physiol
1999;277:H1265-72.
46. Brook WH. A historical review of the histology of patent autogenous vein grafts and vein
patches. J Cardiovasc Surg (Torino) 1975;16:43-52.
47. Svendsen E, Dalen H, Moland J, Engedal H. A quantitative study of endothelial cell injury
in aorto-coronary vein grafts. J Cardiovasc Surg (Torino) 1986;27:65-71.
48. Vlodaver Z, Edwards JE. Pathologic changes in aortic-coronary arterial saphenous vein
grafts. Circulation 1971;44:719-28.
49. Wyatt AP, Taylor GW. Vein grafts: changes in the endothelium of autogenous free vein
grafts used as arterial replacements. Br J Surg 1966;53:943-7.
50. Dilley RJ, McGeachie JK, Prendergast FJ. A review of the histologic changes in vein-to-
artery grafts, with particular reference to intimal hyperplasia. Arch Surg 1988;123:691-6.
51. Unni KK, Kottke BA, Titus JL, Frye RL, Wallace RB, Brown AL. Pathologic changes in
aortocoronary saphenous vein grafts. Am J Cardiol 1974;34:526-32.
52. Baumgartner HR, Muggli R, Tschopp TB, Turitto VT. Platelet adhesion, release and
aggregation in flowing blood: effects of surface properties and platelet function. Thromb
Haemost 1976;35:124-38.
53. Catinella FP, Cunningham JNJ, Srungaram RK, Baumann FG, Nathan IM, Glassman EA,
et al. The factors influencing early patency of coronary artery bypass vein grafts:
correlation of angiographic and ultrastructural findings. J Thorac Cardiovasc Surg
1982;83:686-700.
54. Gundry SR, Jones M, Ishihara T, Ferrans VJ. Optimal preparation techniques for human
saphenous vein grafts. Surgery 1980;88:785-94.
55. Angelini GD. Time-course of medial and intimal thickening in pig venous arterial grafts:
relationship to endothelial injury and cholesterol accumulation. J Thorac Cardiovasc Surg
1992;103:1093-103.
56. Corson JD, Leather RP, Naraynsingh V, Karmody AM, Shah DM. Relationship between
vasa vasorum and blood flow to vein bypass endothelial morphology. Arch Surg
1985;120:386-8.
57. Spray TL, Roberts WC. Changes in saphenous veins used as aortocoronary bypass grafts.
Am Heart J 1977;94:500-16.

40
58. Brody WR, Kosek JC, Angell WW. Changes in vein grafts following aorto-coronary
bypass induced by pressure and ischemia. J Thorac Cardiovasc Surg 1972;64:847-53.
59. Kennedy JH, Lever MJ, Addis BJ, Paneth M. Changes in vein interstitium following
distension for aortocoronary bypass. J Cardiovasc Surg (Torino) 1989;30:992-5.
60. Fujiwara T, Kajiya F, Kanazawa S. Comparison of blood-flow velocity waveforms in
different coronary artery bypass grafts. Sequential saphenous veins grafts and internal
mammary artery grafts. Circulation 1988;78:1210-7.
61. Zwolak RM, Adams MC, Clowes AW. Kinetics of vein graft hyperplasia: association with
tangential stress. J Vasc Surg 1987;5:126-36.
62. Langille BL, O'Donnell F. Reductions in arterial diameter produced by chronic decreases
in blood flow are endothelium-dependent. Science 1986;231:405-7.
63. Manderson JA, Campbell GR. Venous response to endothelial denudation. Pathology
1986;18:77-87.
64. Barboriak JJ, Pintar K, Korns ME. Atherosclerosis in aortocoronary vein grafts. Lancet
1974;2:621-4.
65. Grondin CM. Graft disease in patients with coronary bypass grafting. Why does it start?
Where do we stop? J Thorac Cardiovasc Surg 1986;92:323-9.
66. Fuchs JC, Mitchener JS3, Hagen PO. Postoperative changes in autologous vein grafts. Ann
Surg 1978;188:1-15.
67. Kalan JM, Roberts WC. Morphologic findings in saphenous veins used as coronary arterial
bypass conduits for longer than 1 year: necropsy analysis of 53 patients, 123 saphenous
veins, and 1865 five-millimeter segments of veins. Am Heart J 1990;119:1164-84.
68. Ratliff NB, Myles JL. Rapidly progressive atherosclerosis in aortocoronary saphenous vein
grafts. Possible immune-mediated disease. Arch Pathol Lab Med 1989;113:772-6.
69. Ross R. Atherosclerosis and the arterial smooth muscle cell: Proliferation of smooth
muscle is a key event in the genesis of the lesions of atherosclerosis. Science
1973;180:1332-9.
70. Mann JM, McIntosh CL, Roberts WC. Spasm of saphenous vein used as conduits for
aortocoronary bypass grafting. Am J Cardiol 1987;59:1000-2.
71. Victor MF, Kimbiris D, Iskandrian AS, Mintz GS, Bemis CE, Procacci PM, et al. Spasm of
a saphenous vein bypass graft. A possible mechanism for occlusion of the venous graft.
Chest 1981;80:413-5.
72. Rosenfeldt FL, He G-W, Buxton BF, Angus JA. Pharmocology of coronary artery bypass
grafts. Ann Thorac Surg 1999;67:878-88.

41
73. Wheater PR, Burkitt HG, Daniels VG. Functional histology. A text and colour atlas.
London: Churchill Livingstone, 1987.
74. McGeachie JK, Meagher S, Prendergast FJ. Vein-to-artery grafts: the long-term
development of neo-intimal hyperplasia and its relationship to vasa vasorum and
sympathetic innervation. Aust N Z J Surg 1989;59:59-65.
75. O'Brien Jr JE, Shi Y, Fard A, Bauer T, Zalewski A, Mannion JD. Wound healing around
and within saphenous vein bypass grafts. J Thorac Cardiovasc Surg 1997;114:38-45.
76. Barker SG, Talbert A, Cottam S, Baskerville PA, Martin JF. Arterial intimal hyperplasia after
occlusion of the adventitial vasa vasorum in the pig. Arterioscler Thromb 1993;13:70-7.
77. Martin JF, Booth RF, Moncada S. Arterial wall hypoxia following thrombosis of the vasa
vasorum is an initial lesion in atherosclerosis. Eur J Clin Invest 1991;21:355-9.
78. Dashwood MR, Angelini GD, Mehta D, Jeremy JY, Meunter K, Kirchengast M. Effect of
angioplasty and grafting on porcine vascular nerves: a potential neurotropic role for
endothelin-1. J Anat 1998;192:435-7.
79. Shi Y, O'Brien JE, Fard A, Mannion JD, Wang D, Zalewski A. Adventitial myofibroblasts
contribute to neointimal formation in injured porcine coronary arteries. Circulation
1996;94:1655-64.
80. Shi Y, Pieniek M, Fard A, O'Brien J, Mannion JD, Zalewski A. Adventitial remodeling
after coronary arterial injury. Circulation 1996;93:340-8.
81. Schwartz SM, DeBlois D, O'Brien ER. The intima. Soil for atherosclerosis and restenosis.
Circ Res 1995;77:445-65.
82. Karnsz M, Christman EW, Derrick JR. Use of cold cardioplegic solution for vein graft
distension and preservation: A light and scanning electron microscopic study. Ann Thorac
Surg 1981;32:68-74.
83. Sottiurai VS, Stanley JC, Fry WJ. Ultrastructure of human and transplanted canine veins:
effects of different preparation media. Surgery 1983;93:28-38.
84. Schaeffer U, Tanner B, Strohschneider T, Stadtmuller A, Hannekum A. Damage to arterial
and venous endothelial cells in bypass grafts induced by several solutions used in bypass
surgery. Thorac Cardiovasc Surg 1997;45:168-71.
85. Sanchez AM, Wooldridge TA, Boerboom LE, Olinger GN, Almassi GH, Rusch NJ.
Comparison of saphenous vein graft relaxation between Plasma-Lyte solution and normal
saline solution. J Thorac Cardiovasc Surg 1994;107:1445-53.
86. Ingemansson R, Sjoberg T, Massa G, Steen S. Long-term preservation of vascular
endothelium and smooth muscle. Ann Thorac Surg 1995;59:1177-81.

42
87. Anastasiou N, Allen S, Paniagua R, Chester A, Yacoub M. Altered endothelial and smooth
muscle cell reactivity caused by University of Wisconsin preservation solution in human
saphenous vein. J Vasc Surg 1997;25:713-21.
88. Hofer H, Mihatsch MJ, Guggenheim R, Amsler B, Hasse J, Graedel E. Morphologic
studies in saphenous vein grafts for aorto-coronary bypass surgery. Part I: Morphology of
the Graft using ordinary surgical preparation techniques. Thorac Cardiovasc Surg
1981;29:32-7.
89. Adcock OT, Adcock GLD, Wheeler JR, Gregory RT, Snyder SO, Gayle RG. Optimal
techniques for harvesting and preparation of reversed autogenous vein grafts for use as
arterial substitutes: A review. Surgery 1984;96:886-94.
90. Haudenschild CC, Gould KE, Quist WC, LoGerfo FW. Protection of endothelium in vessel
segments excised for grafting. Circulation 1981;64:101-7.
91. Underwood MJ. Effect of locally applied tissue-type plasminogen activator on venous
fibrinolytic activity: in vitro and in vivo investigations. Cardiovasc Res 1993;27:2270-3.
92. Gottlob R. The preservation of the venous endothelium by "dissection without touching"
and by an atraumatic technique of vascular anastomosis. The importance for arterial and
venous surgery. Minerva Chir 1977;32:693-700.
93. Gundry SR. Intraoperative trauma to human saphenous veins: scanning electron
microscopic comparison of preparation techniques. Ann Thorac Surg 1980;30:40-7.
94. He GW, Rosenfeldt FL, Angus JA. Pharmacological relaxation of the saphenous vein
during harvesting for coronary artery bypass grafting. Ann Thorac Surg 1993;55:1210-7.
95. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, et al. Saphenous vein
graft patency 1 year after coronary artery bypass surgery and effects of antiplatelet therapy:
results of a veterans administration cooperative study. Circulation 1989;80:1190-7.
96. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, et al. Internal
mammary artery and saphenous vein graft patency. Effects of aspirin. Circulation
1990;82:237-42.
97. Stein PD. Antithrombotic therapy in patients with saphenous vein and internal mammary
artery bypass grafts. Chest 1995;108:424S-30S.
98. The effect of aggressive lowering of low-density lipoprotein cholesterol levels and low-
dose anticoagulation on obstructive changes in saphenous-vein coronary-artery bypass
grafts. The Post Coronary Artery Bypass Graft Trial Investigators. N Engl J Med
1997;336:153-62.
43
99. Jeremy JY, Dashwood MR, Mehta D, Izzat MB, Shukla N, Angelini GD. Nitric oxide,
prostacyclin and cyclic nucleotide formation in externally stented porcine vein grafts.
Atherosclerosis 1998;141:297-305.
100. Tsui JCS, Souza DR, Filbey D, Bomfim V, Dashwood MR. Preserved endothelial integrity
and nitric oxide synthase in saphenous vein graft harvested by a "no-touch" technique. Br J
Surg 2001;88:1209-15.
101. Sogo N, Campanella C, Webb DJ, Megson IL. S-nitrosothiols cause prolonged, nitric
oxide-mediated relaxation in human saphenous vein and internal mammary artery:
therapeutic potential in bypass surgery. Br J Pharmacol 2000;131:1236-44.
102. George SJ, Johnson JL, Angelini GD, Jeremy JY. Short-term exposure to thapsigargin
inhibits neointima formation in human saphenous vein. Arterioscler Thromb Vasc Biol
1997;17:2500-6.
103. Burke SE, Lubbers NL, Chen YW, Hsieh GC, Mollison KW, Luly JR, et al. Neointimal
formation after balloon-induced vascular injury in Yucatan minipigs is reduced by oral
rapamycin. J Cardiovasc Pharmacol 1999;33:829-35.
104. Gallo R, Padurean A, Jayaraman T, Marx S, Roque M, Adelman S, et al. Inhibition of
intimal thickening after balloon angioplasty in porcine coronary arteries by targeting
regulators of the cell cycle. Circulation 1999;99:2164-70.
105. Chen L, Daum G, Forough R, Clowes M, Walter U, Clowes AW. Overexpression of
human endothelial nitric oxide synthase in rat vascular smooth muscle cells and in balloon-
injured carotid artery. Circ Res 1998;82:862-70.
106. Janssens S, Flaherty D, Nong Z, Varenne O, van Pelt N, Haustermans C, et al. Human
endothelial nitric oxide synthase gene transfer inhibits vascular smooth muscle cell
proliferation and neointima formation after balloon injury in rats. Circulation
1998;97:1274-81.
107. Shears LL2n, Kibbe MR, Murdock AD, Billiar TR, Lizonova A, Kovesdi I, et al. Efficient
inhibition of intimal hyperplasia by adenovirus-mediated inducible nitric oxide synthase
gene transfer to rats and pigs in vivo. J Am Coll Surg 1998;187:295-306.
108. Hariawala MD, Horowitz JR, Esakof D, Sheriff DD, Walter DH, Keyt B, et al. VEGF
improves myocardial blood flow but produces EDRF-mediated hypotension in porcine
hearts. J Surg Res 1996;63:77-82.
109. Takeshita S, Zheng LP, Brogi E, Kearney M, Pu LQ, Bunting S, et al. Therapeutic
angiogenesis. A single intraarterial bolus of vascular endothelial growth factor augments
revascularization in a rabbit ischemic hind limb model. J Clin Invest 1994;93:662-70.

44
110. Van Belle E, Maillard L, Tio F, OIsner JM. Accelerated endothelialization by local
delivery of recombinant human vascular endothelial growth factor reduces in-stent intimal
formation. Biochem Biophys Res Commun 1997;235:311-6.
111. Yla-Herttuala S, Martin JF. Cardiovascular gene therapy. Lancet 2000;355:213-22.
112. Kalra M, Jost CJ, Severson SR, Miller VM. Adventitial versus intimal liposome-mediated
ex vivo transfection of canine saphenous vein grafts with endothelial nitric oxide synthase
gene. J Vasc Surg 2000;32:1190-200.
113. Mehta D, George SJ, Jeremy JY, Basher Izzat M, Southgate KM, Bryan AJ, et al. External
stenting reduces long-term medial and neointimal thickening and platelet derived growth
factor expression in a pig model of arteriovenous bypass grafting. Nature Medicine
1998;4:235-9.
114. Violaris AG, Newby AC, Angelini GD. Effects of external stenting on wall thickening in
arteriovenous bypass grafts. Ann Thorac Surg 1993;55:667-71.
115. Jeremy JY, Dashwood MR, Timm M, Izzat MB, Mehta D, Bryan AJ, et al. Nitric oxide
synthase and adenylyl and guanylyl cyclase activity in porcine interposition vein grafts.
Ann Thorac Surg 1997;63:470-6.
116. Dashwood MR, Mehta D, Izzat MB. Distribution of endothelin-1 (ET) receptors (ETA and
ETB) and immunoreactive ET-1 in porcine saphenous vein-carotid artery interposition
grafts. Atherosclerosis 1998;137:233-42.
117. Altman DG, Bland JM. How to randomise. BMJ 1999;319:703-4.
118. Judkins MP. Selective coronary arteriography. Part I: A percutaneous transfemoral technic.
Radiology 1967;89:815-24.
119. Siegal S, Castellan NJ. Non-parametric statistics for the behavioral sciences. London:
McGraw-Hill, 1988.
120. Rogers WH. Stata Technical Bulletin, Stata Corp, College Station Tx, 1993.
121. Cnaan A, Laird NM, Slasor P. Using the general linear mixed model to analyse repeated
measures and longitudinal data. Stat Med 1997;16:2349-80.
122. Cooper GJ, Underwood MJ, Deverall PB. Arterial and venous conduits for coronary artery
bypass. A current review. Eur J Cardiothorac Surg 1996;10:129-40.
123. Reardon MJ, Conklin LD, Reardon PR, Baldwin JC. Coronary artery bypass conduits:
review of current status. J Cardiovasc Surg (Torino) 1997;38:201-9.
124. Cox JL, Chaisson DA, Gotlieb AI. Stranger in a strange land: the pathogenesis of
saphenous vein graft stenosis with emphasis on structural and functional differences
between veins and arteries. Prog Cardiovasc Dis 1991;34:45-68.

45
125. Lehmann KH, von Segesser L, Muller-Glauser W, Siebenmann R, Schneider K, Luscher
TF, et al. Internal-mammary coronary artery grafts: is their superiority also due to a
basically intact endothelium? Thorac Cardiovasc Surg 1989;37:187-9.
126. Holt CM, Francis SE, Newby AC, Rogers S, Gadsdon PA, Taylor T, et al. Comparison of
response to injury in organ culture of human saphenous vein and internal mammary artery.
Ann Thorac Surg 1993;55:1522-8.
127. Daly RC, McCarthy PM, Orszulak TA, Schaff HV, Edwards WD. Histologic comparison
of experimental coronary artery bypass grafts. Similarity of in situ and free internal
mammary artery grafts. J Thorac Cardiovasc Surg 1988;96:19-29.
128. Roubos N, Rosenfeldt FL, Richards SM, Conyers RAJ, Davis BB. Improved preservation
of saphenous vein grafts by the use of glyceryl-trinitrate-verapamil solution during
harvesting. Circulation 1995;92:31-6.
129. Costello KB, Stewart DJ, Baffour R. Endothelin is a potent constrictor of human vessels
used in coronary revascularization surgery. Eur J Pharmacol 1990;186:311-4.
130. Cracowski JL, Stanke-Labesque F, Sessa C, Hunt M, Chavanon O, Devillier P, et al.
Functional comparison of the human isolated femoral artery, internal mammary artery,
gastroepiploic artery, and saphenous vein. Can J Physiol Pharmacol 1999;77:770-6.
131. O'Neil GS, Chester AH, Schyns CJ, Tadjkarimi S, Borland JA, Yacoub MH. Effect of
surgical preparation and arterialization on vasomotion of human saphenous vein. J Thorac
Cardiovasc Surg 1994;107:699-706.
132. Binko J, Meachem S, Majewski H. Endothelium removal induces iNOS in rat aorta in
organ culture, leading to tissue damage. Am J Physiol 1999;276:E125-34.
133. Boulanger CM, Heymes C, Benessiano J, Geske RS, Levy BI, Vanhoutte PM. Neuronal
nitric oxide synthase is expressed in rat vascular smooth muscle cells: activation by
angiotensin II in hypertension. Circ Res 1998;83:1271-8.
134. Comini L, Bachetti T, Gaia G, Pasini E, Agnoletti L, Pepi P, et al. Aorta and skeletal
muscle NO synthase expression in experimental heart failure. J Mol Cell Cardiol
1996;28:2241-8.
135. Papadaki M, Tilton RG, Eskin SG, McIntire LV. Nitric oxide production by cultured
human aortic smooth muscle cells: stimulation by fluid flow. Am J Physiol
1998;274:H616-26.
136. Gonzalez C, Barroso C, Martin C, Gulbenkian S, Estrada C. Neuronal nitric oxide synthase
activation by vasoactive intestinal peptide in bovine cerebral arteries. J Cereb Blood Flow
Metab 1997;17:977-84.

46
137. Yogo K, Shimokawa H, Funakoshi H, Kandabashi T, Miyata K, Okamoto S, et al.
Different vasculoprotective roles of NO synthase isoforms in vascular lesion formation in
mice. Arterioscler Thromb Vasc Biol 2000;20:96-100.
138. Kawashima S, Yamashita T, Ozaki M, Ohashi Y, Azumi H, Inoue N, et al. Endothelial NO
synthase overexpression inhibits lesion formation in mouse model of vascular remodeling.
Arterioscler Thromb Vasc Biol 2001;21:201-7.
139. Durrani A, Sim EKW, Grignani RT. Accurate length adjustment of aortocoronary
saphenous vein bypass grafts. Ann Thorac Surg 1998;66:966-7.
140. Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, et al. Saphenous vein
graft patency 1 year after coronary artery bypass surgery and effects of antiplatelet therapy.
Results of a Veterans Administration Cooperative Study. Circulation 1989;80:1190-7.
141. Souza DSR, Christofersson RHB, Bomfim V, Filbey D. "No-touch" technique by using
saphenous vein harvested with its surrounding tissue for coronary artery bypass grafting
maintains an intact endothelium. Scand J Thorac Cardiovasc Surg 1999;33:323-9.
142. Milroy CM, Scott DJ, Beard JD, Horrocks M, Bradfield JW. Histological appearances of
the long saphenous vein. J Pathol 1989;159:311-6.
143. Björk VO, Ekeström S, Henze A, Ivert T, Landou C. Early and late patency of
artocoronary vein grafts. Scand J Thorac Cardiovasc Surg 1981;15:11-21.
144. Vural KM, Sener E, Tasdemir O. Long-term patency of sequential and individual
saphenous vein coronary bypass grafts. Eur J Cardiothorac Surg 2001;19:140-4.
145. Korpilahti K, Engblom E, Syvänne M, Hämäläinen H, Puukka P, Vänttinen E, et al.
Angiographic changes in saphenous vein grafts and atherosclerosis risk factors. Scand J
Thorac Cardiovasc Surg 1998;32:343-51.


















