
Harry J. M. Groen - Continuüm Oncologie J.M. Groen, Erik van der Heijden, Theo J Klinkenberg, Bonne...
51
Transcript of Harry J. M. Groen - Continuüm Oncologie J.M. Groen, Erik van der Heijden, Theo J Klinkenberg, Bonne...

Harry J. M. Groen
Longarts
Universitair Medisch Centrum Groningen
Highlights SCLC, NSCLC enMesothelioom
(potentiële) belangenverstrengeling
Voor bijeenkomst mogelijk relevante relaties met bedrijven
Eli Lilly, GSK, Merck, BMS, Roche, Genentech, Amgen, Pfizer
• Sponsoring of onderzoeksgeld• Honorarium of andere (financiële)
vergoeding• Aandeelhouder• Andere relatie, namelijk …
• CANCER-ID, IMI, KWF• UMCG
• Geen• NVALT
Disclosure
Outline
• SCLC• Radiotherapy
• bd or daily radiotherapy
• Immunotherapy for SCLC
• New drug
• NSCLC• Treuzelen bij early NSCLC
• Proton or photon in radiotherapy
• Stage III: chemoradiotherapy
• Oligometastatic NSCLC
• Immunotherapy
• Mesothelioma and thymoma 4
Small Cell Lung Cancer
• bd or daily radiotherapy
• Immunotherapy for SCLC
• New drug
5

6
7
8
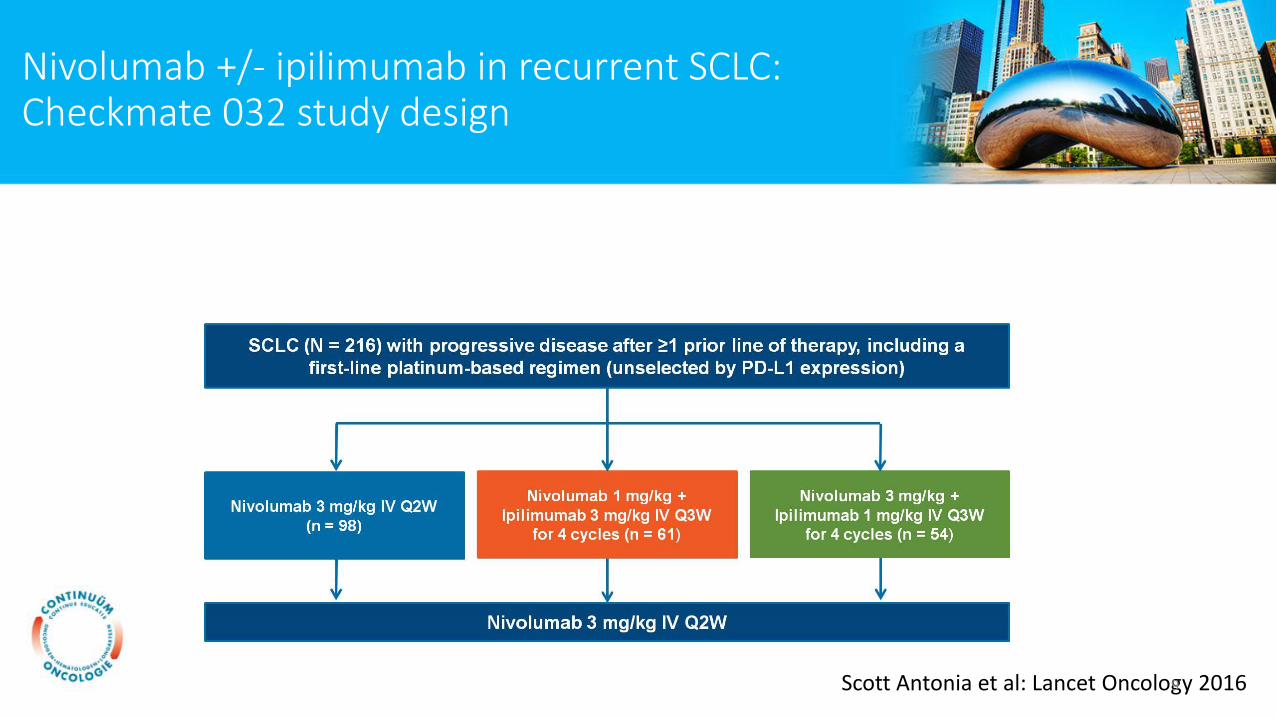
Nivolumab +/- ipilimumab in recurrent SCLC:Checkmate 032 study design
Scott Antonia et al: Lancet Oncology 20169
10
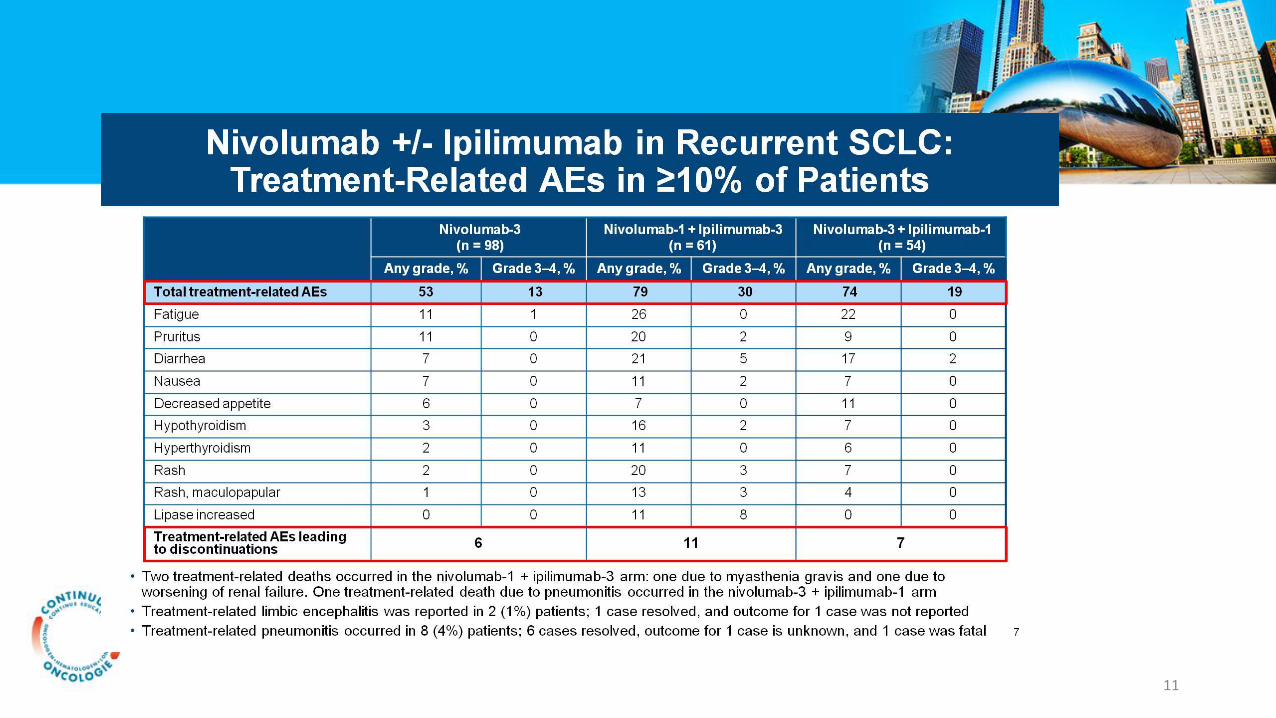
11
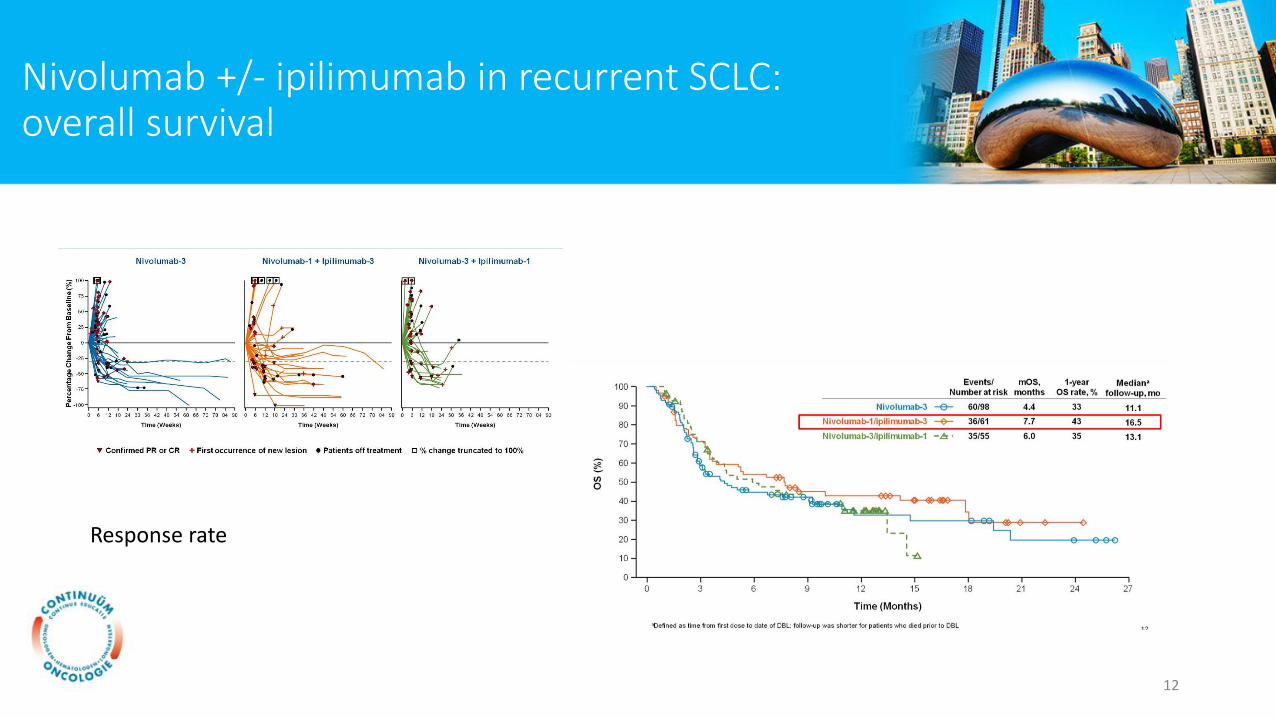
Nivolumab +/- ipilimumab in recurrent SCLC:overall survival
Response rate
12
Nivolumab +/- Ipilimumab in Recurrent SCLC: Conclusions
Presented By Scott Antonia at 2016 ASCO Annual Meeting13
Ongoing Studies With Nivolumab/Ipilimumab in SCLC
Presented By Scott Antonia at 2016 ASCO Annual Meeting14
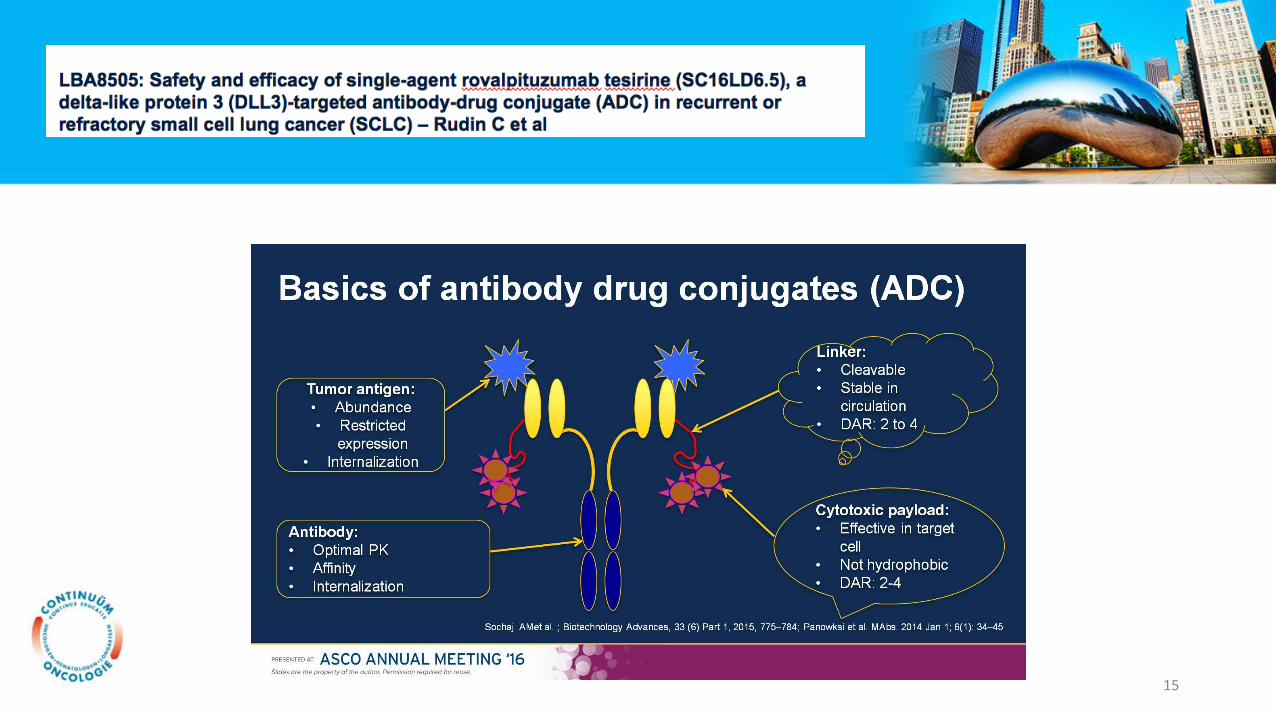
15
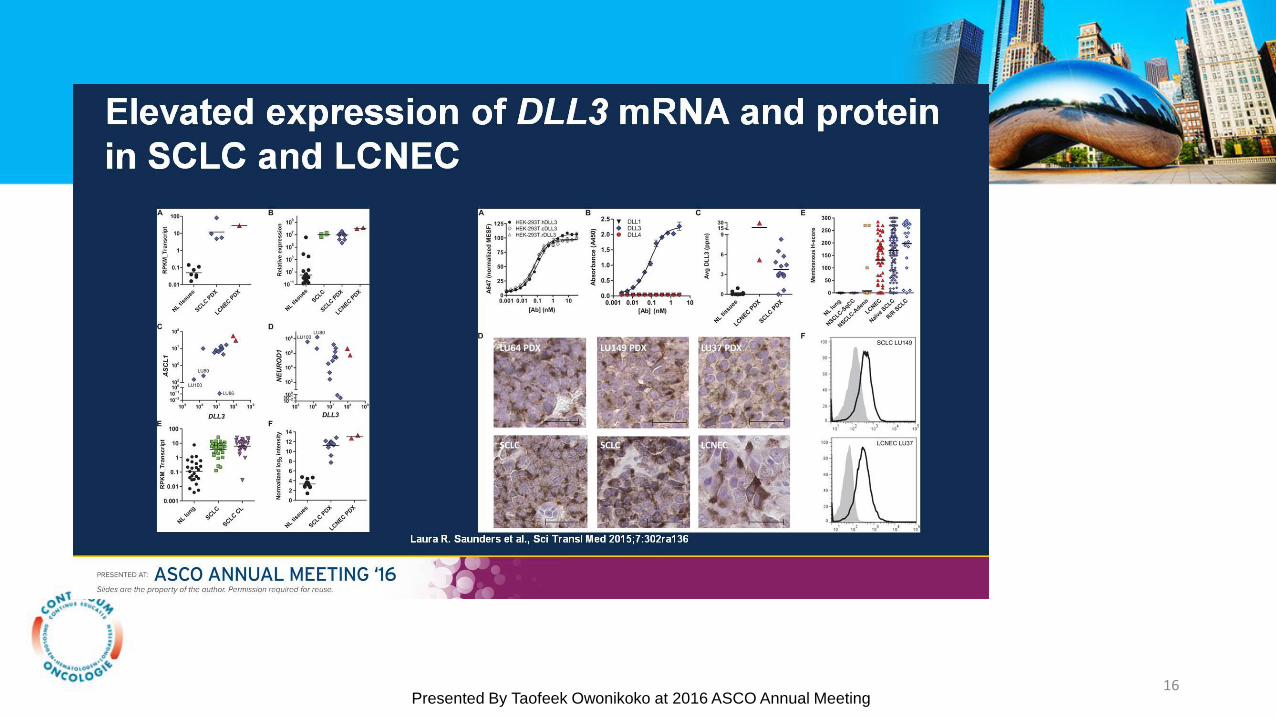
Elevated expression of DLL3 mRNA and protein in SCLC and LCNEC
Presented By Taofeek Owonikoko at 2016 ASCO Annual Meeting16
17

Best Responses per Investigator by DLL3
Presented By Taofeek Owonikoko at 2016 ASCO Annual Meeting18
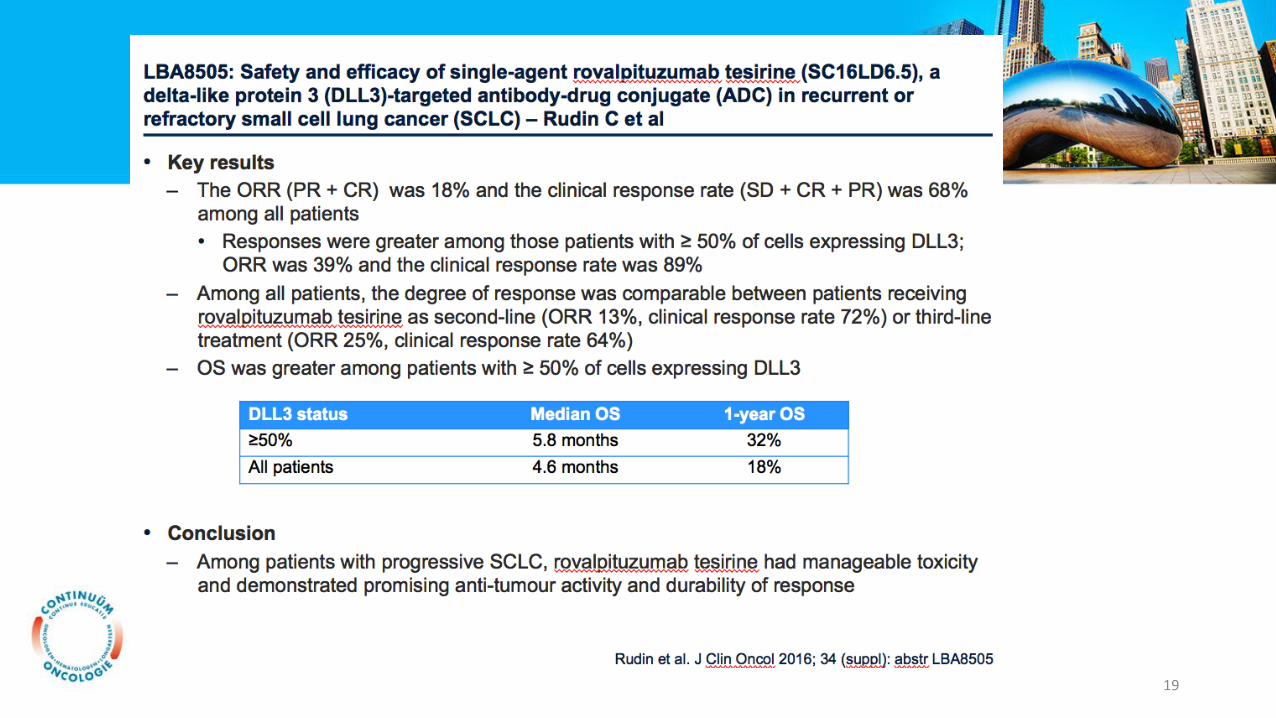
19
Non-Small Cell Lung Cancer
• Treuzelen bij early NSCLC
• Photon vs Proton radiotherapy
• Stage III: chemoradiotherapy
• Oligometastatic NSCLC
• Immunotherapy
20

Invloed van treuzelen bij NSCLC
1. Effect of time-to-treatment on survival in NSCLC (8542)
2. Impact on survival of increasing the time between diagnosis and lobectomy (8549).
21
Effect of time-to-treatment on survival in NSCLC– Anggondowati T et al
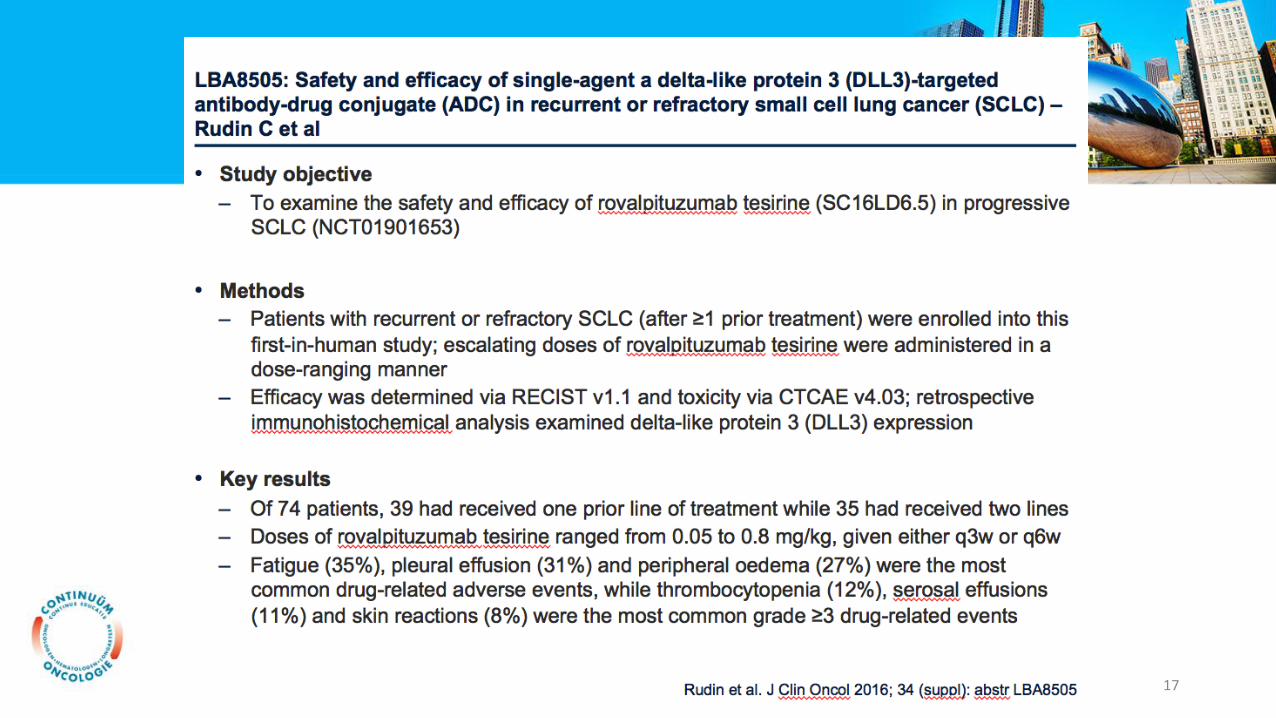
• Study objective
• To investigate the effect time-to-treatment on OS of NSCLC patients
• Methods
• Patients (n=693,554) diagnosed with NSCLC between 2003 and 2011 were identified from the National Cancer Data Base
• Time-to-treatment was defined as the interval between diagnosis and treatment initiation and categorized as: 0 days; 0.1 to 4 weeks (reference); 4.1 to 6 weeks; and >6 weeks
• Key results
• Nearly 43% of patients started treatment >4 weeks after diagnosis and 25% waited >6 weeks
• In early stage patients (I/II) who survived at least 36 months, risk of death was higher among those who waited for 4.1−6.0 weeks (HR=1.06, 95%CI 1.03−1.10), or >6 weeks (HR=1.18, 95%CI 1.15, 1.22) to start treatment, compared with those who waited 0.1−4.0 weeks
• A survival benefit of shorter time-to-treatment was not found in patients who survived <12 months and stage IV patients
• Conclusion
• Survival benefit can be gained by expediting treatment for early stage NSCLC
• Future research is needed to identify patients’ characteristics that could predict the tolerable time-to-treatment for individual patients
Anggondowati et al. J Clin Oncol 2016; 34 (suppl): abstr 854222
Optimal timing of lobectomy for clinical stage IA NSCLC– Yang C-F et al
• Study objective
• To investigate the impact on survival of increasing the time between diagnosis and lobectomy with clinical stage IA NSCLC
• Methods
• Retrospective analysis of 16,861 patients who underwent lobectomy as primary therapy for clinical stage IA NSCLC identified from the National Cancer Data Base (2006 to 2011)
• ‘Early’ surgery was defined as within 1−36 days of diagnosis; ‘late’ surgery was ≥37 days
• Key results
• Patient with increased surgical waiting time were more likely to be older, black, have more comorbidities, uninsured, lower income and lower education status
• A delay in surgery was associated with worse 5-year OS (59.9% with late surgery vs. 65.5% with early; p<0.001)
• In a multivariable analysis, delaying surgery beyond 37 days led to an increased risk of death with a HR of 1.11
• Conclusion
• Shorter time to surgery among patients with early stage NSCLC is associated with improved survival
• If possible, surgical resection should be performed at least within five weeks of diagnosis
Yang et al. J Clin Oncol 2016; 34 (suppl): abstr 854923
Randomized phase III study of adjuvant chemotherapy with or without low-molecular weight heparin in completely resected non-small cell lung cancer patients: The NVALT-8 study
Harry J.M. Groen, Erik van der Heijden, Theo J Klinkenberg, Bonne Biesma, Joachim Aerts, Ad Verhagen, Corinne Kloosterziel, Hans J.M. Smit, Franz Schramel, Vincent van
der Noort, Harm van Tinteren, Egbert F. Smit, Anne-Marie C. Dingemans for the NVALT Study Group
The Netherlands
Trialnr: NTR1250
24
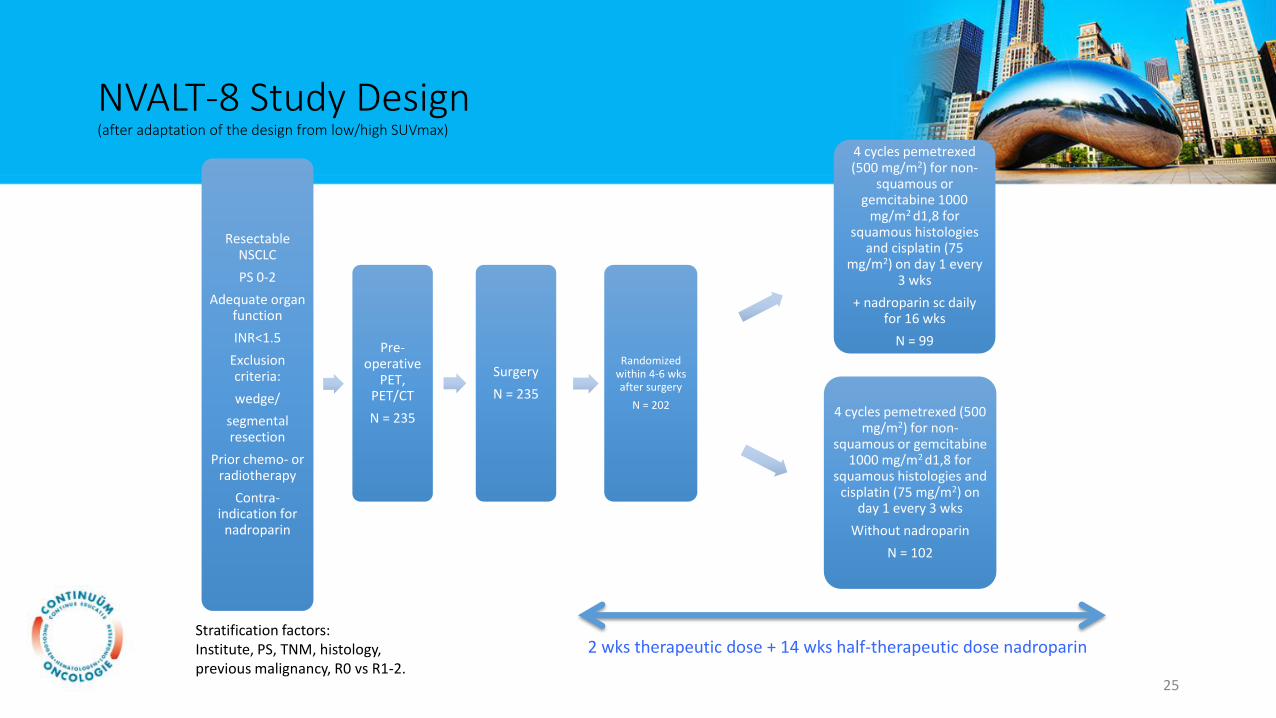
NVALT-8 Study Design(after adaptation of the design from low/high SUVmax)
ResectableNSCLC
PS 0-2
Adequate organ function
INR<1.5
Exclusion criteria:
wedge/
segmental resection
Prior chemo- or radiotherapy
Contra-indication for
nadroparin
Pre-operative
PET, PET/CT
N = 235
Surgery
N = 235
Randomized within 4-6 wksafter surgery
N = 202
4 cycles pemetrexed(500 mg/m2) for non-
squamous or gemcitabine 1000
mg/m2 d1,8 for squamous histologies
and cisplatin (75 mg/m2) on day 1 every
3 wks
+ nadroparin sc daily for 16 wks
N = 99
4 cycles pemetrexed (500 mg/m2) for non-
squamous or gemcitabine 1000 mg/m2 d1,8 for
squamous histologies and cisplatin (75 mg/m2) on
day 1 every 3 wks
Without nadroparin
N = 102
2 wks therapeutic dose + 14 wks half-therapeutic dose nadroparinStratification factors:Institute, PS, TNM, histology,previous malignancy, R0 vs R1-2.
25
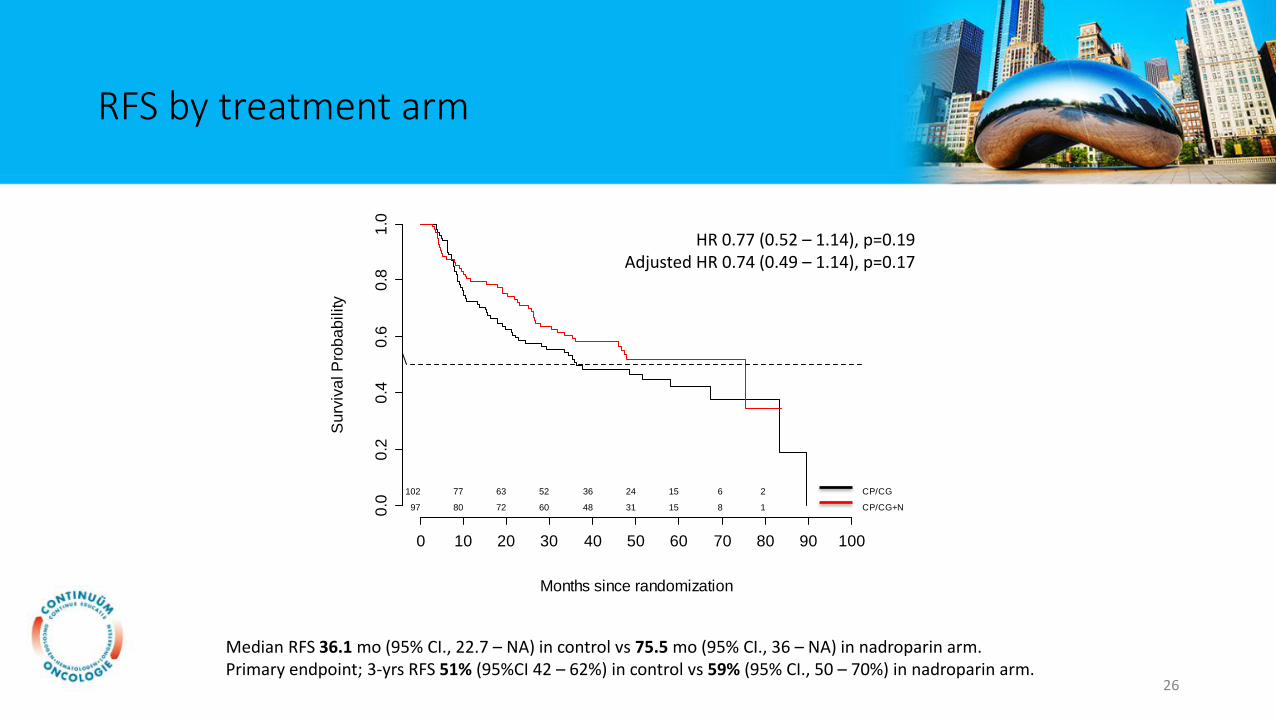
RFS by treatment arm
Median RFS 36.1 mo (95% CI., 22.7 – NA) in control vs 75.5 mo (95% CI., 36 – NA) in nadroparin arm.Primary endpoint; 3-yrs RFS 51% (95%CI 42 – 62%) in control vs 59% (95% CI., 50 – 70%) in nadroparin arm.
HR 0.77 (0.52 – 1.14), p=0.19Adjusted HR 0.74 (0.49 – 1.14), p=0.17
Months since randomization
0 10 20 30 40 50 60 70 80 90 100
Su
rviv
al P
rob
ab
ility
0.0
0.2
0.4
0.6
0.8
1.0
102 77 63 52 36 24 15 6 2 CP/CG
97 80 72 60 48 31 15 8 1 CP/CG+N
26

RFS stratified for SUVmax risk groups
Stratitified for SUVmax-based risk groups:HR 0.69 (95% CI., 0.46 - 1.05, p = 0.09)
Months since randomization
0 10 20 30 40 50 60 70 80 90 100
Su
rviv
al P
rob
ab
ility
0.0
0.2
0.4
0.6
0.8
1.0
75 55 48 41 29 20 15 6 2 CP/CG High
19 16 11 7 4 2 CP/CG Low
57 45 42 39 33 25 13 7 1 CP/CG+N High
34 30 25 19 14 6 2 1 CP/CG+N Low
27
Conclusions
• Adjuvant nadroparin in patients with resected NSCLC added to adjuvant chemotherapy does not improve RFS.
• SUVmax does not predict for recurrence-free survival in resectable NSCLC.
28
29
30
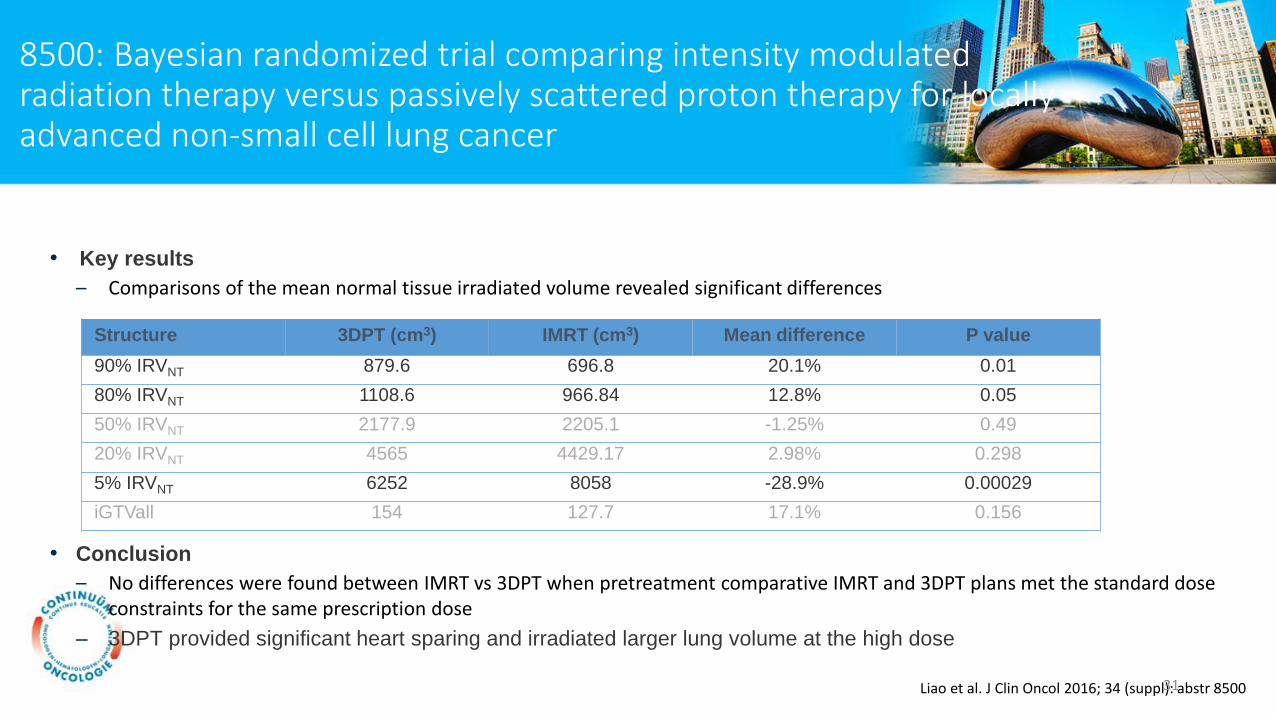
• Key results
– Comparisons of the mean normal tissue irradiated volume revealed significant differences
• Conclusion
– No differences were found between IMRT vs 3DPT when pretreatment comparative IMRT and 3DPT plans met the standard dose constraints for the same prescription dose
– 3DPT provided significant heart sparing and irradiated larger lung volume at the high dose
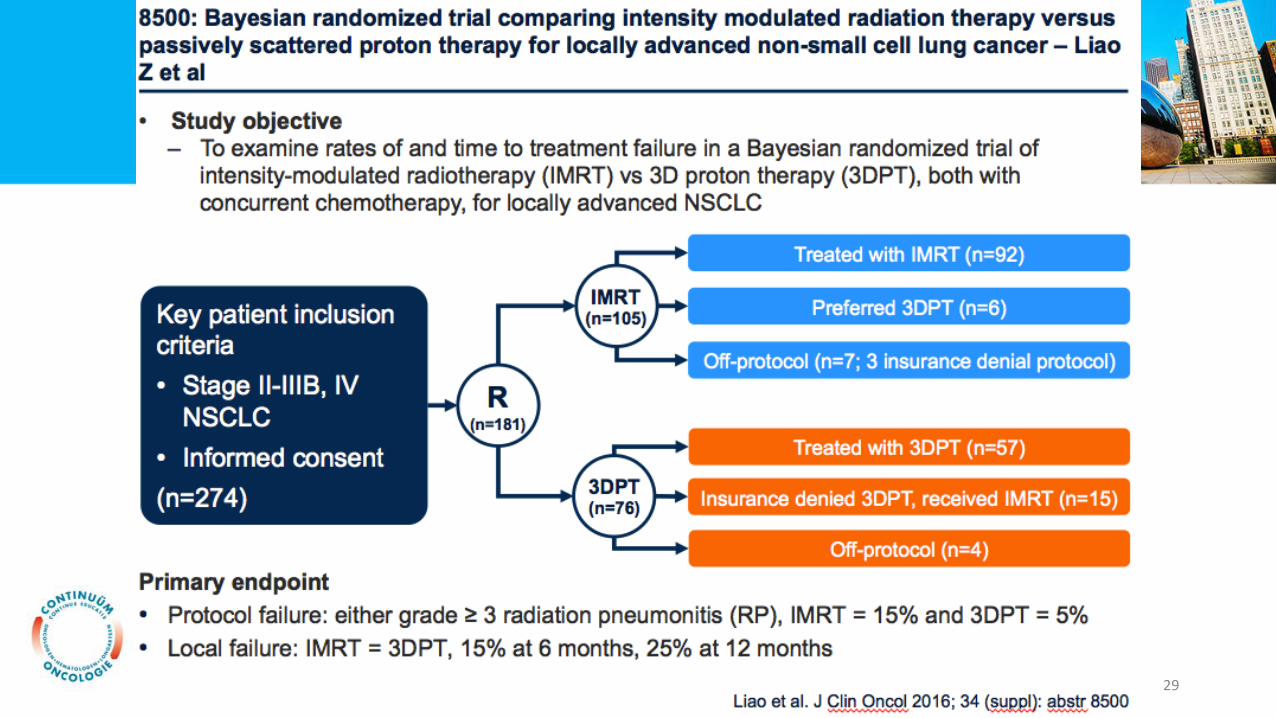
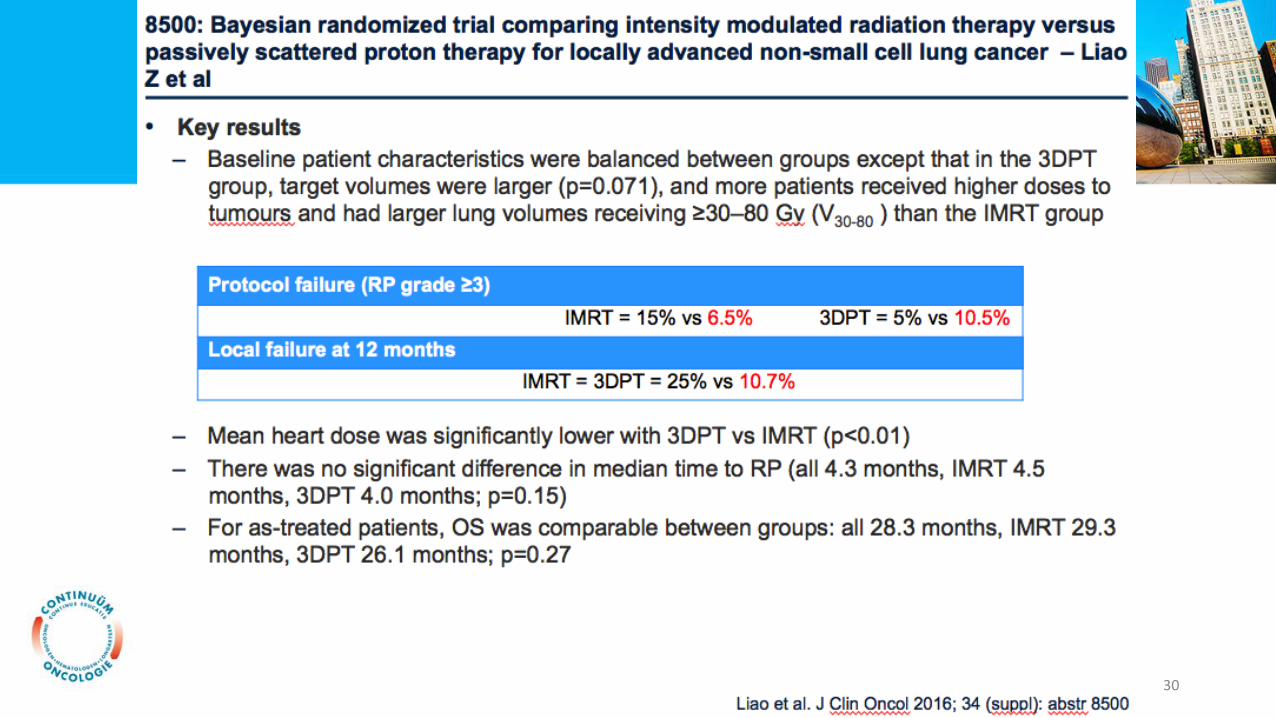
8500: Bayesian randomized trial comparing intensity modulated radiation therapy versus passively scattered proton therapy for locally advanced non-small cell lung cancer
Liao et al. J Clin Oncol 2016; 34 (suppl): abstr 8500
Structure 3DPT (cm3) IMRT (cm3) Mean difference P value
90% IRVNT 879.6 696.8 20.1% 0.01
80% IRVNT 1108.6 966.84 12.8% 0.05
50% IRVNT 2177.9 2205.1 -1.25% 0.49
20% IRVNT 4565 4429.17 2.98% 0.298
5% IRVNT 6252 8058 -28.9% 0.00029
iGTVall 154 127.7 17.1% 0.156
31
32
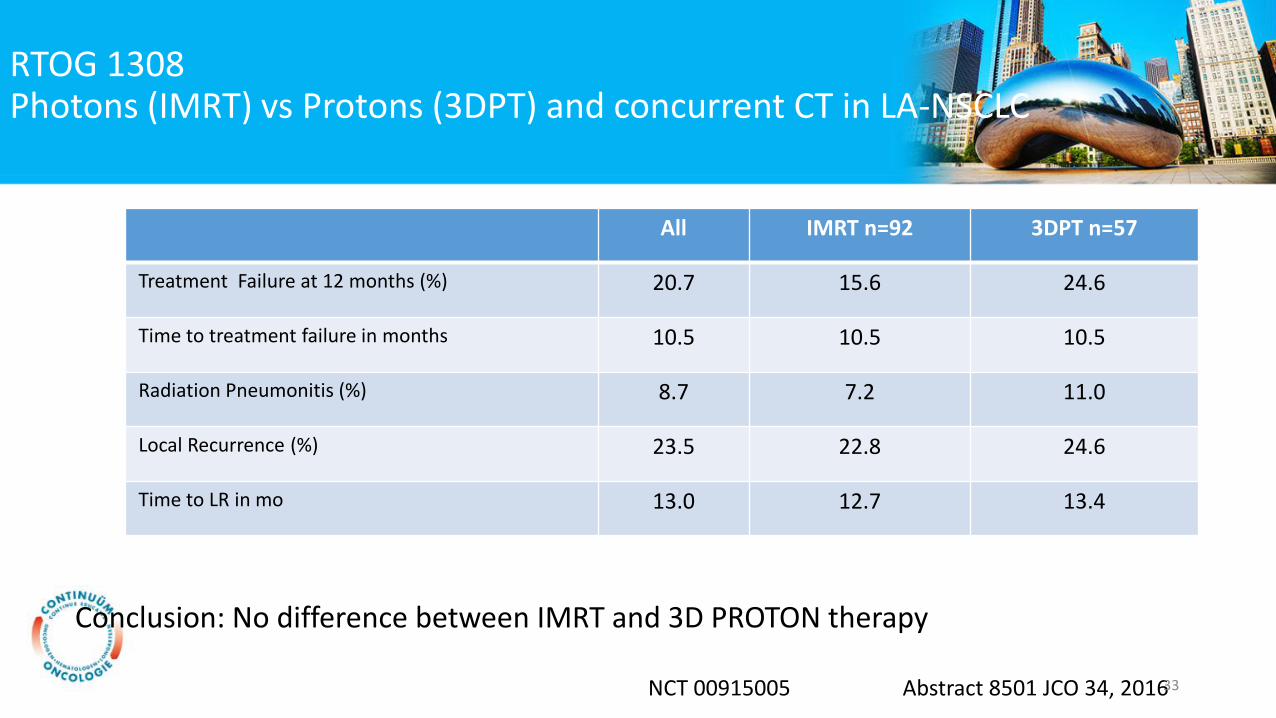
RTOG 1308 Photons (IMRT) vs Protons (3DPT) and concurrent CT in LA-NSCLC
All IMRT n=92 3DPT n=57
Treatment Failure at 12 months (%) 20.7 15.6 24.6
Time to treatment failure in months 10.5 10.5 10.5
Radiation Pneumonitis (%) 8.7 7.2 11.0
Local Recurrence (%) 23.5 22.8 24.6
Time to LR in mo 13.0 12.7 13.4
Abstract 8501 JCO 34, 2016
Conclusion: No difference between IMRT and 3D PROTON therapy
NCT 00915005 33
RTOG 1308Photons (IMRT) vs Protons (3DPT) and concurrent CT in LA-NSCLC
• Target volumes larger and dosis higher to tumors and lung tissue in 3DPT group.
• TF rate was much better than anticipated: 20.7% instead of 40% at 12 months
• First generation proton therapy technique “3D PT” (using passive scattering) versus optimal photon therapy.
• Currently: Intensity Modulated Proton Therapy (IMPT) available with better conformity.
Conclusion: No difference between IMRT and 3D PROTON therapy
34
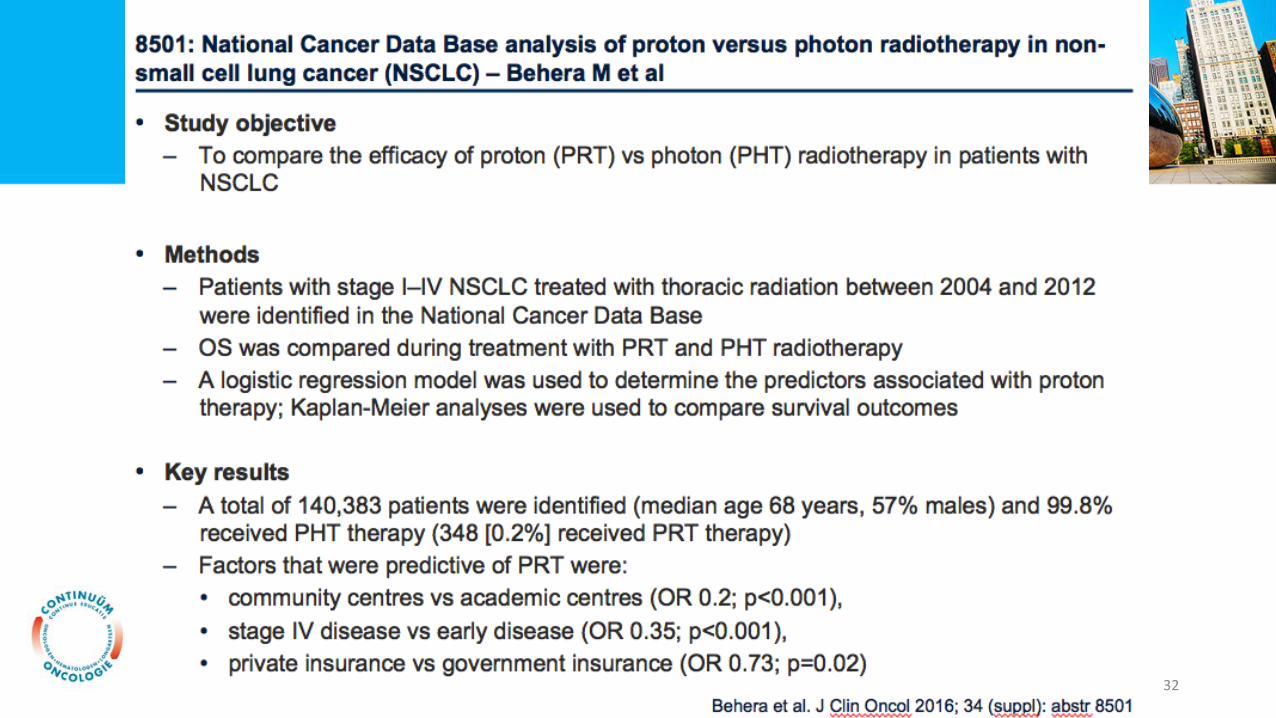
8501: National Cancer Data Base analysis of proton versus photon radiotherapy in non-small cell lung cancer (NSCLC) – Behera M et al
• Key results
• Multivariate analysis revealed that PHT was associated with an increased risk of death relative to PRT (HR 1.46; p<0.001)
• Comparing PHT and PRT in a propensity-matched analysis, 5-year OS was 14% and 23%; median survival was 13.5 vs 18.4 months; p<0.02
• For patients with stage II/III disease, PHT was associated with an increased risk of death relative to PRT (multivariate HR 1.35; p<0.003)
• Comparing PHT and PRT in patients with stage II/II, 5-year OS was 15% and 22%; median survival was 13.4 vs 17.4 months; log-rank p<0.02
• Conclusion
• In this retrospective database analysis thoracic radiation with protons is associated with better survival rates in stage II/III NSCLC patients
• An active phase III randomized trial (NRG Oncology 1308) is underway to evaluate if chemotherapy and PRT for stage III NSCLC patients improves survival over chemotherapy and PHT
Behera et al. J Clin Oncol 2016; 34 (suppl): abstr 850135

8508: A pooled analysis of concurrent chemoradiotherapy (CCRT)for patients with stage III NSCLC who participatedin US cooperative group trials: Comparing the outcomes of elderly to younger patients
• Study objective
• To analyse the outcomes of CCRT in elderly patients with stage III NSCLC compared with younger patients
• Methods
• Analysis of 3,070 stage IIIA/B patients from 15 clinical trials in the US Cooperative Group
• Compared OS, PFS and AEs for patients aged ≥70 years (n=733) and <70 years (n=2,337)
• Key results
• OS was significantly worse in elderly patients (HR 1.18 [95%CI 1.08, 1.29]; p=0.0006)
• PFS did not differ by age (HR 1.05 [95%CI 0.96, 1.15]; p=0.41)
• There was a higher rate of grade ≥3 AEs in elderly compared with younger patients (OR 1.23 [95%CI 0.97, 1.56])
• Grade 5 AEs were more common in elderly patients (7.6% vs. 3.8% in younger patients; p<0.05) but treatment-related deaths were not different
• Conclusion
• Elderly patients showed significantly worse OS and similar PFS to younger patients
• Grade 3 and 5 AEs were more frequent in elderly patients but rate of death attributed to treatment was similar
Stinchcombe et al. J Clin Oncol 2016; 34 (suppl): abstr 850836
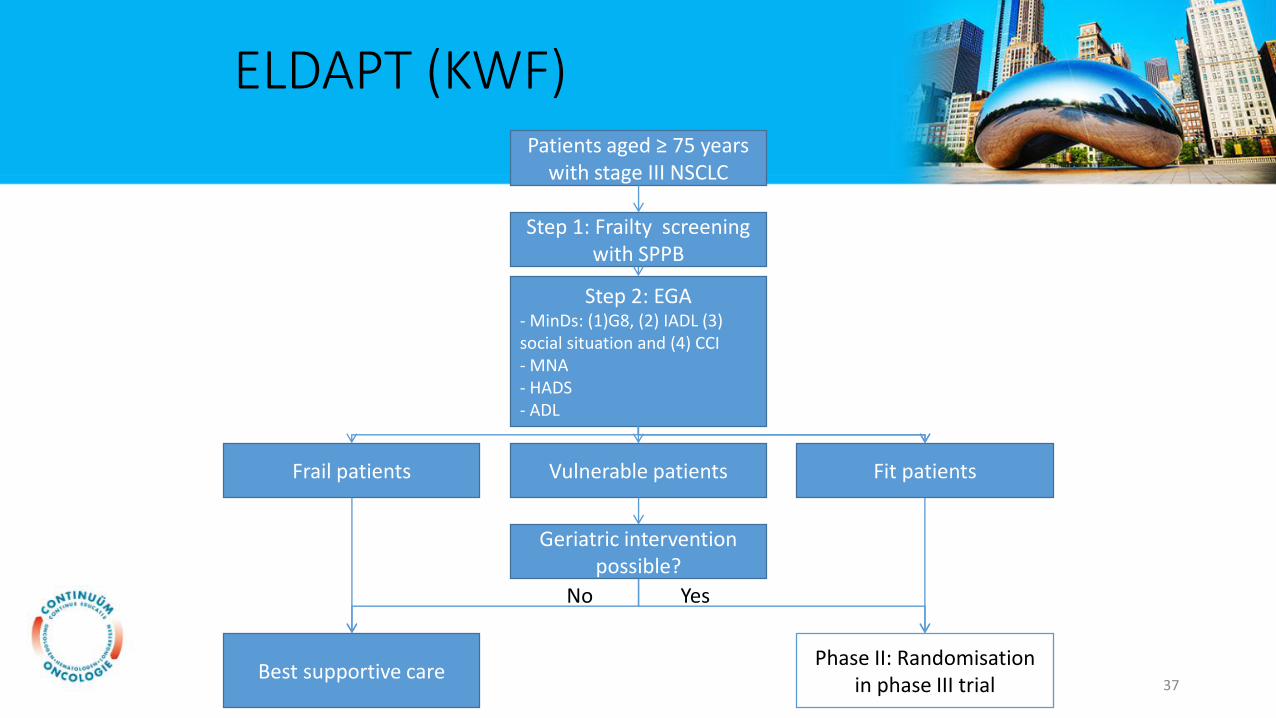
ELDAPT (KWF)
Phase II: Randomisation in phase III trial
Step 1: Frailty screening with SPPB
Best supportive care
Fit patientsFrail patients
Step 2: EGA- MinDs: (1)G8, (2) IADL (3) social situation and (4) CCI- MNA- HADS - ADL
Patients aged ≥ 75 years with stage III NSCLC
Geriatric intervention possible?
Vulnerable patients
YesNo
37
Prevalence, clinical risk factors and outcomes of patients with lung cancer presenting with brain metastases – Waqar S et al
• Study objective
• To determine the frequency of brain metastases in patients diagnosed with NSCLC and clinical risk factors associated with their presence
• Methods
• Patients (n=457,481) with NSCLC diagnosed between 2010 and 2012 with brain metastasis data available were identified from the National Cancer Data Base
• Odds ratios (ORs) for presence of brain metastasis were calculated for individual pre-specified covariates of interest using logistic regression analysis
• Key results
• Brain metastases were observed in 10.4% of patients with NSCLC
• On multivariate analysis the following variables were significantly associated with presence of brain metastasis: age; adenocarcinoma histology; tumor size; tumor grade and node positive disease
• The incidence of brain metastasis ranged from 0.6% in patients with only 1 risk factor to as high as 22% in patients with all 5 risk factors
• Conclusion
• The risk of brain metastases at presentation of NSCLC may be calculated based on 5 clinical variables
• If validated, this model may be used to guide the staging work-up for patients with newly diagnosed NSCLC without symptoms suggesting brain metastases
Waqar et al. J Clin Oncol 2016; 34 (suppl): abstr 207538
39
40

41
42
43
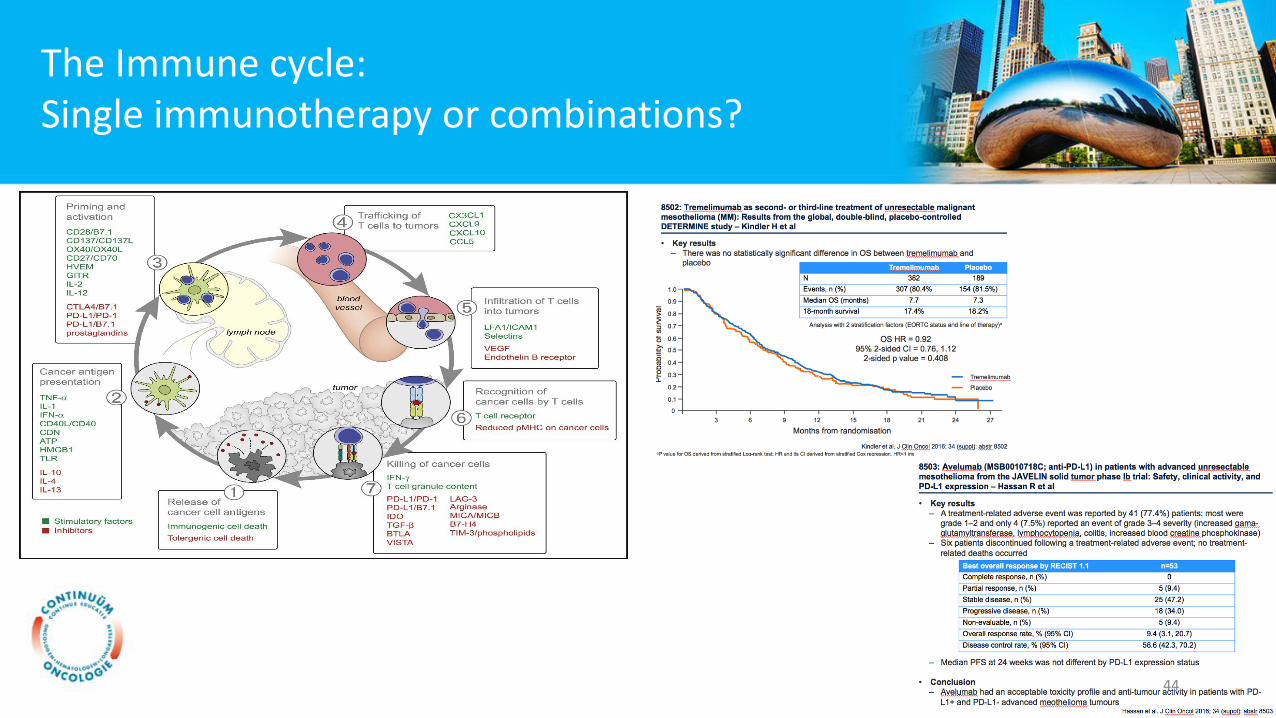
The Immune cycle:Single immunotherapy or combinations?
Immunity 2013 39, 1-10DOI: (10.1016/j.immuni.2013.07.012) Chen & Mellman, Immunity 201344
Conclusie
• Radiotherapie blijft standaard bij SCLC
• Protonen en fotonen: technische verbeteringen moeten de beloftevan protonen waarmaken.
• Niet meer treuzelen in het zorgpad longkanker.
• Combineren van immunotherapie is de volgende stap in de behandeling van longkanker: verbetering van overleving en meertoxiciteit.
45
• Ga nu naar: www.pollev.com/benecke en
beantwoord de eerste vraag
• U krijgt 30 seconden per vraag om te antwoorden.
Vragen
Vraag 1
Op welke locatie bent u?
A. Amsterdam
B. Rotterdam
C. Zwolle
D. Eindhoven
47
Vraag 2
Hoe bent u vandaag gekomen?
A. Auto
B. Openbaar vervoer
C. Fiets
D. Lopend
48
Vraag 3
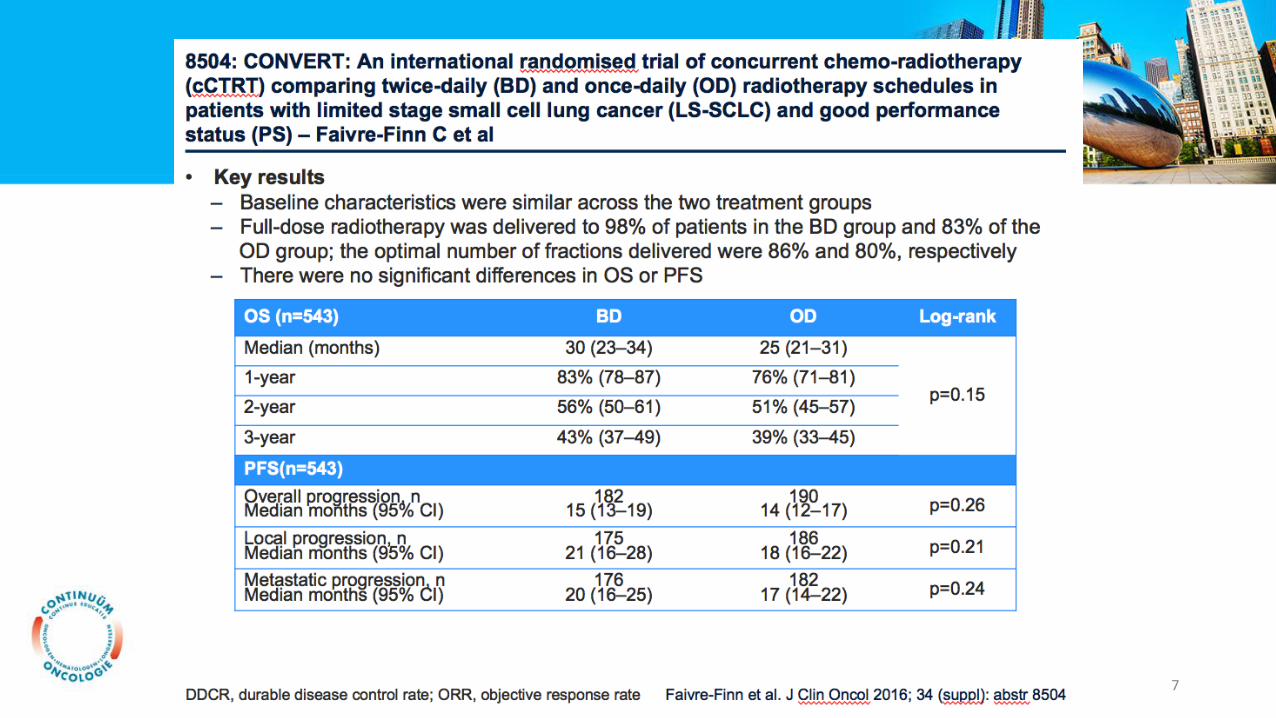
De CONVERT studie is een gerandomiseerde studie van gelijktijdigechemoradiotherapie waarbij twee maal daags (totaal 45 Gy) versus eenmaaldaags radiotherapie (60 Gy) wordt gegeven bij LD-SCLC met een goede PS.
a. eenmaal daags is beter dan de lage bestralingsdosis
b. de lage bestralingsdosis geeft dezelfde uitkomst als de hogebestralingsdosis
c. de lage bestralingsdosis geeft minder toxiciteit en werkt minder goed
d. Alle bovenstaande beweringen zijn fout
49
Vraag 4
Kleincellig longcarcinoom is een toonbeeld van hoge PD-L1 expressie, omdat deze tumoren goed op behandeling reageren.
a. Waar
b. Niet waar
50
Vraag 5
De bijwerkingen van immunotherapie worden door de wetenschappelijke vereniging van longartsen schromelijkoverdreven. Chemotherapie heeft immers meer bijwerkingen. Dat er drie op de 61 patiënten immuno-gerelateerde doden bijnivo + ipi zijn gevallen doet er niet toe.
a. Waar
b. Niet waar
51


















