Handovers of Patient Care: What Will It Take to Ensure...
92
Handovers of Patient Care: What Will It Take to Ensure Safe Outcomes? Take to Ensure Safe Outcomes? Vineet M. Arora, MD, MA Vineet M. Arora, MD, MA 1 Rich Frankel, PhD Rich Frankel, PhD 2 Julie K. Johnson, MSPH, PhD Julie K. Johnson, MSPH, PhD 3 Paul R. Barach, MD, MPH Paul R. Barach, MD, MPH 4 1 University of Chicago, IL, USA; University of Chicago, IL, USA; 2 Indiana University, USA; Indiana University, USA; 3 University of New South Wales, Sydney, Australia University of New South Wales, Sydney, Australia 4 University Medical Centre Utrecht, The Netherlands University Medical Centre Utrecht, The Netherlands Academy Health Academy Health Academy Health Academy Health Academy Health Academy Health June 27, 2010 June 27, 2010 Academy Health Academy Health June 27, 2010 June 27, 2010
Transcript of Handovers of Patient Care: What Will It Take to Ensure...

Handovers of Patient Care: What Will It Take to Ensure Safe Outcomes?Take to Ensure Safe Outcomes?
Vineet M. Arora, MD, MAVineet M. Arora, MD, MA11
Rich Frankel, PhDRich Frankel, PhD22
Julie K. Johnson, MSPH, PhDJulie K. Johnson, MSPH, PhD33
Paul R. Barach, MD, MPHPaul R. Barach, MD, MPH44
11University of Chicago, IL, USA; University of Chicago, IL, USA; 22Indiana University, USA;Indiana University, USA;33University of New South Wales, Sydney, AustraliaUniversity of New South Wales, Sydney, Australia
44University Medical Centre Utrecht, The NetherlandsUniversity Medical Centre Utrecht, The Netherlands
Academy HealthAcademy HealthAcademy HealthAcademy HealthAcademy HealthAcademy HealthJune 27, 2010June 27, 2010
Academy HealthAcademy HealthJune 27, 2010June 27, 2010

Session ObjectivesSession ObjectivesSession ObjectivesSession Objectives
Determine the optimal methods for Determine the optimal methods for exploring transitions/handovers of careexploring transitions/handovers of carep g /p g /
Describe international trends and research Describe international trends and research findings in transitions of patient carefindings in transitions of patient carefindings in transitions of patient carefindings in transitions of patient care
Review Educational assessment methodsReview Educational assessment methods Discuss barriers, enablers, and successful Discuss barriers, enablers, and successful
interventions for local implementationinterventions for local implementationinterventions for local implementationinterventions for local implementation

Picture of JuliePicture of JuliePicture of JuliePicture of Julie

Picture of RichPicture of RichPicture of RichPicture of Rich

IntroductionsIntroductionsIntroductionsIntroductions
Who is in the room?Who is in the room?–– How many nurses?How many nurses?How many nurses?How many nurses?–– How many physicians?How many physicians?
How many from an academic health center?How many from an academic health center?–– How many from an academic health center?How many from an academic health center?–– How many of you conduct handovers? How many of you conduct handovers?
What are your expectations for today’sWhat are your expectations for today’sWhat are your expectations for today s What are your expectations for today s session?session?

Taxonomy of Hospital Handoffsy pExtra-hospital handoffs Intra-hospital handoffs Discharge
– Home or rehab Service transfer
– Escalation or de-escalatonHome or rehab
Admission – EMS-ED or ED to floor
Escalation or de escalaton of care (in and out of ICU)
– EMS-ED or ED to floor
Inter-hospital transfer– Different specialty (med-
surgery, OR to PACU)
Shift change – Is the sender returning?
(night float with cross-cover)
Service change

Timing Is Everything for Timing Is Everything for SprintSprint Relay SuccessRelay SuccessSprintSprint--Relay SuccessRelay Success
By Sean P. FlynnBy Sean P. FlynnSpecial to The Washington PostSpecial to The Washington PostFriday, April 15, 2005; Page D16Friday, April 15, 2005; Page D16

HandHand offs and Patient Safetyoffs and Patient SafetyHandHand--offs and Patient Safetyoffs and Patient Safety Shift changes (handoffs, signShift changes (handoffs, sign--outs) represent transitions outs) represent transitions
that can impact the quality of patient care and patient that can impact the quality of patient care and patient safetysafetysafetysafety–– Some estimates put the percentage of adverse events Some estimates put the percentage of adverse events
related to shift changes as high as 80%!related to shift changes as high as 80%!related to shift changes as high as 80%! related to shift changes as high as 80%! The literature in this area has been dominated by the The literature in this area has been dominated by the
nursing professionnursing professionnursing professionnursing profession Wide variation across institutions, professional roles, Wide variation across institutions, professional roles,
shifts, and individualsshifts, and individuals,, No studies to date have tried to reduce unwanted variation No studies to date have tried to reduce unwanted variation

Role of HandRole of Hand off in Patient Careoff in Patient CareRole of HandRole of Hand--off in Patient Careoff in Patient Care Part of the “clinical microsystem” lifePart of the “clinical microsystem” life--cyclecycle Part of the clinical microsystem lifePart of the clinical microsystem life cyclecycle
–– Intern perspective: No big deal, “just part of the Intern perspective: No big deal, “just part of the k”k”work”work”
–– Nurse perspective: “We are the constant Nurse perspective: “We are the constant presence at the bedside” presence at the bedside”

Handoffs in Medicine and NursingHandoffs in Medicine and NursingHandoffs in Medicine and NursingHandoffs in Medicine and Nursing Because of the nature of the work, the limited Because of the nature of the work, the limited
time spent on each service and local variation, time spent on each service and local variation, most trainees simply “show up” on service begin most trainees simply “show up” on service begin their rotations without any formal training or their rotations without any formal training or practice practice
The result is that they quickly adopt whatever The result is that they quickly adopt whatever form of handoff is accepted on that service form of handoff is accepted on that service ppwhether it is safe and effectivewhether it is safe and effective
Perfect example of the operation of the informalPerfect example of the operation of the informal Perfect example of the operation of the informal Perfect example of the operation of the informal or hidden curriculum in medicine and nursingor hidden curriculum in medicine and nursing

Global Calls to Improve HandoffsGlobal Calls to Improve Handoffspp
The Joint Commission, 2006The Joint Commission, 2006The Joint Commission, 2006The Joint Commission, 2006 National Patient Safety Goal: a National Patient Safety Goal: a
standardized approachstandardized approach to handto hand--off off d dd dcommunications and provide an communications and provide an
opportunity for staff to ask and respond opportunity for staff to ask and respond to questions about a patient's careto questions about a patient's careto questions about a patient s care to questions about a patient s care
World Health Organization, 2006World Health Organization, 2006

Communication in HealthcareCommunication in HealthcareCommunication in HealthcareCommunication in Healthcare
–– Failures in Failures in communicationcommunicationcommunication communication are the most are the most common rootcommon rootcommon root common root cause of cause of sentinel events sentinel events reported to reported to JCAHOJCAHO
Sentinel Event Statistics. Available at: http://www.jcaho.org.

Global Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve HandoffsGlobal Calls to Improve Handoffs
Institute of Medicine 2008Institute of Medicine 2008 Teaching programs “should train Teaching programs “should train g p gg p g
resident in how to hand over their resident in how to hand over their patients using effective patients using effective communications”communications”
Australian Commission on Quality Australian Commission on Quality and Safety in Health Care, 2008and Safety in Health Care, 2008and Safety in Health Care, 2008and Safety in Health Care, 2008

2010 ACGME Resident Duty Hours2010 ACGME Resident Duty Hours
• July 2003– ACGME resident duty hours– Reduce sleep deprivation – Improve patient safety
BUT increase in number of hand offs– BUT increase in number of hand-offs
• June 2010- Focus on Handoff Education– Programs must ensure
– Residents are ‘competent’ in handoff communication
– Monitoring of Handoffs so they are structured, effective and safe
– 16 hours for interns16 hours for interns– 24+4 hours (transitions)-residents

Lack of National Standards for Lack of National Standards for Patient HandoffsPatient Handoffs
Only 8% of medical schools teach how to hand Only 8% of medical schools teach how to hand off patients in a formal didactic sessionoff patients in a formal didactic sessionoff patients in a formal didactic sessionoff patients in a formal didactic session. . (National survey of 125 medical schools) (National survey of 125 medical schools)
The vast majority (86%) of medical students areThe vast majority (86%) of medical students are The vast majority (86%) of medical students are The vast majority (86%) of medical students are taught by interns or residents who were likely taught by interns or residents who were likely taught by their interns or residents and so ontaught by their interns or residents and so ontaught by their interns or residents and so ontaught by their interns or residents and so on
Exemplifies the “hidden” or informal curriculum Exemplifies the “hidden” or informal curriculum i di i h t k i l d b b ii di i h t k i l d b b iin medicine where a task is learned by observing in medicine where a task is learned by observing those in charge…those in charge…
(Solet et al, 2005, Horwitz, 200

Learning Organization SengeLearning Organization SengeLearning Organization, SengeLearning Organization, Senge
Mental modelsMental models Building shared vision/EngagementBuilding shared vision/Engagement Systems thinking/Process and humanSystems thinking/Process and human Systems thinking/Process and human Systems thinking/Process and human
factorsfactors Personal mastery/Competencies and Personal mastery/Competencies and
reflectionreflection Teams/relationshipsTeams/relationships

Mental ModelsMental ModelsMental ModelsMental Models
Our personal image of the worldOur personal image of the world–– None are perfectly accurateNone are perfectly accurateNone are perfectly accurate None are perfectly accurate –– Differences in mental models explain how two Differences in mental models explain how two
people can understand the same eventpeople can understand the same eventpeople can understand the same event people can understand the same event differently differently Are generally invisible to usAre generally invisible to us until we look foruntil we look for–– Are generally invisible to us Are generally invisible to us –– until we look for until we look for themthem
1717

The LadderThe LadderThe Ladder The Ladder of Inferenceof Inference
1818

How Can We Surface Our How Can We Surface Our Mental ModelsMental Models??
W ki ith t l d l iW ki ith t l d l i Working with mental models requires Working with mental models requires surfacing, testing, and improving our internal surfacing, testing, and improving our internal i t f h th ld ki t f h th ld kpictures of how the world workspictures of how the world works
3 skills can be helpful3 skills can be helpful–– Reflection Reflection –– Use a disciplined, reflective learning Use a disciplined, reflective learning
approach approach –– for example, a Planfor example, a Plan--DoDo--StudyStudy--Act Act (PDSA) l(PDSA) l t d t di t lt d t di t l(PDSA) cycle (PDSA) cycle –– to understanding your own mental to understanding your own mental models and the implicationsmodels and the implicationsInquiryInquiry learning the questions you can ask tolearning the questions you can ask to–– Inquiry Inquiry –– learning the questions you can ask to learning the questions you can ask to help you test others’ mental modelhelp you test others’ mental model
–– AdvocacyAdvocacy –– making your thinking and reasoningmaking your thinking and reasoning
1919
Advocacy Advocacy making your thinking and reasoning making your thinking and reasoning more visible to others more visible to others

Understanding Handoffs F f C i tias a Form of Communication
“who says what to whom in what channel with what effect”channel with what effect”
Harold Dwight Lasswell

HandHand--off as a Form of Communicationoff as a Form of Communication“When you move from right to left you lose richness such asleft, you lose richness, such as physical proximity and the conscious and subconscious clues. You also lose the ability toYou also lose the ability to communicate through techniques other than words such as gestures and facial expressions. The ability f p yto change vocal inflection and timing to emphasize what you mean is also lost…Finally, the ability to answer questions in real time, are important because questions provide insight into how well the information is being understood by the listener.”
–Alistair Cockburn


Psychology of MiscommunicationPsychology of Miscommunication
Speakers systematically Speakers systematically overestimate how well their messages aretheir messages are understood by listeners
Egocentric heuristic–Senders assume that receiver has all the same knowledge that th dthey do – Worsens better you know
someoneo o
Keysar, et al. Psychol Sci. 2002; J Pers Soc Psychol. 2004; Intercultural Pragmatics. 2007

Applications of Standard Applications of Standard LanguageLanguage
“Read“Read--back”back”–– Reduces errors inReduces errors inReduces errors in Reduces errors in
lab reportinglab reporting
“Read-backs” at your neighborhood Drive Thruneighborhood Drive-Thru
29 errors detected during requested read-back of 822requested read-back of 822 lab results at Northwestern Memorial Hospital. All errors detected and corrected.
Barenfanger, Sautter, Lang, et al. Am J Clin Pathol, 2004.
detected and corrected.

A Word of Caution on A Word of Caution on TechnologyTechnology
IT solutions alone cannot substitute for a IT solutions alone cannot substitute for a “successful communication act”“successful communication act”–– Human vigilance still requiredHuman vigilance still requiredg qg q
In an emergency room, replacing a phone call for critical lab g y p g p fvalues with electronic reporting with no verbal communication resulted in 45% (1443/3228) of urgent labs to go unchecked.
Ash, Berg, Coiera. JAMIA, 2004; Kilpatrick, Holding, BMJ, 2001.

Another Technology Caution: CoPaGA Syndrome
CoPaGA = Copy Paste Gone Amok
Repeated highlighting, copying and pasting text from past EHR notes into current notes;
The physician attains several goals:
1. avoiding time-consuming work of talking to patient2. building a documentation trail that portrays faux work 3. crowd-out of useful information by gluts of useless data4. zombie-like propagation of inaccuracies that persist
74% of IM residents saw cut/paste problems in signout—(unpublished)

Swiss Cheese ModelG l C fli tGoal Conflicts
and Double Binds
Incomplete Procedures
Mixed Messages
Production Pressures
Inadequate Training
Attention Distractions
Deferred Maintenance
Clumsy Technology LATENT
Triggers
Regulatory Narrowness
PressuresResponsibility
Shifting
TechnologyFAILURES
gg
The World
Accident
Modified from Reason, 1991 © 1991, James ReasonDEFENSES

Model of “Big 5” Teamworkg
Team
THE CORE
Team Leadership
Team Orientation
Mutual Performance Monitoring
Back-UpBehavior
Adaptability
Baker, Salas, King, Battles, Barach, 2006

HandHand--offs in Other offs in Other HighHigh--Risk IndustriesRisk Industries
Di t b ti f h dDi t b ti f h d ff t NASA 2ff t NASA 2 Direct observations of handDirect observations of hand--offs at NASA, 2 offs at NASA, 2 Canadian nuclear power plants, a railroad Canadian nuclear power plants, a railroad dispatch center and an ambulance dispatchdispatch center and an ambulance dispatchdispatch center, and an ambulance dispatch dispatch center, and an ambulance dispatch centercenter
STRATEGIESSTRATEGIES STRATEGIESSTRATEGIES–– Standardize Standardize -- use same order or templateuse same order or template
Update informationUpdate information–– Update information Update information –– Limit interruptions Limit interruptions –– Face to face verbal updateFace to face verbal updateFace to face verbal update Face to face verbal update with interactive questioning with interactive questioning
–– StructureStructure ReadRead--back to ensure accuracyback to ensure accuracy
Patterson, Roth, Woods, et al. Intl J Quality Health Care, 2004

Patient Handoff Video VignettesPatient Handoff Video VignettesPatient Handoff Video VignettesPatient Handoff Video Vignettes
Create a checklist for observations:Create a checklist for observations:–– Please record cultural, communication, andPlease record cultural, communication, andPlease record cultural, communication, and Please record cultural, communication, and
environmental barriers that interfere with a environmental barriers that interfere with a successful patient handsuccessful patient hand--off in the video off in the video success u pat e t a dsuccess u pat e t a d o t e deoo t e deovignettevignette

What Do You Look For?What Do You Look For?Barriers Observations/ThoughtsCultural (e.g., not prioritizing hand-offs, ( g , p g ,following proper procedures, unprofessional behavior, etc.)
Communication (e.g., vague terms, incomplete information, lack of verification, etc.)
Environmental (e.g., distractions and b l f h lobstacles interfering with completing proper
hand-off procedure)
Other
FacilitatorsWhat ent ell?What went well?

Review of Handoff VideosReview of Handoff VideosReview of Handoff VideosReview of Handoff Videos
Video #1 U of CVideo #1 U of CVideo #2 Indiana

Debriefing from the video vignettesDebriefing from the video vignettesDebriefing from the video vignettesDebriefing from the video vignettes
What did you observe?What did you observe? Barriers/Enablers?Barriers/Enablers? Barriers/Enablers?Barriers/Enablers?
–– EnvironmentEnvironmentC lt lC lt l–– CulturalCultural
–– CommunicationCommunication–– Any others?Any others?

Handoff Studies

Understanding HandUnderstanding Hand--offsoffsUnderstanding HandUnderstanding Hand--offs offs as a Processas a Processas a Processas a Process
“The first step is to draw a flow diagram. Then“The first step is to draw a flow diagram. ThenThe first step is to draw a flow diagram. Then The first step is to draw a flow diagram. Then everyone understands what his job is. If people do everyone understands what his job is. If people do
not see the process, they cannot improve it.”not see the process, they cannot improve it.”ot see t e p ocess, t ey ca ot p o e tot see t e p ocess, t ey ca ot p o e t W.E. Deming, 1993W.E. Deming, 1993

Building a Standard Handoff Protocol 2006Building a Standard Handoff Protocol 2006Building a Standard Handoff Protocol 2006Building a Standard Handoff Protocol 2006 Principles Principles
–– Protocol will be discipline Protocol will be discipline specificspecific
–– Standardization is key for both Standardization is key for both yyprocess and contentprocess and content
“Handoff Clinic” for various “Handoff Clinic” for various residency programsresidency programs–– PROCESSPROCESS
Create a process mapCreate a process map Create a process map Create a process map –– CONTENTCONTENT
Create a standard checkCreate a standard check--listlistIMPLEMENTATIONIMPLEMENTATION–– IMPLEMENTATIONIMPLEMENTATION Resident buyResident buy--inin
–– MONITORING MONITORING Identify and resolve barriersIdentify and resolve barriers

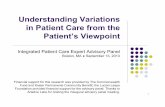
Anesthesia Resident to PACU Nurse HandAnesthesia Resident to PACU Nurse Hand--OffOff
Is patient ok to go to PACU?Patient in OR
Resident tells circulating nurse
about special needs (venilator, a-line, invasive monitors, etc.)
Resident mentally summarizes case
to prepare for documentation
Resident moves patient to PACU
Resident arrives in PACU and shouts
out to unit clerk “Where am I going/what
number bed?”
Sec’y or someone else answers with bed or slot number
Resident takes patient to
designated slotyes
Patient goes to ICU
no
Clear delineation of roles/responsibility
Are nurses waiting at slot?
Nursing hooks up monitors with
priority on oxygen and pulse ox, then
EKG and blood
Is there a greater than 30 second
delay in hook up?
Resident completes
documentation of case (fills out PACU vitals, writes note
noIs patient high risk?
(difficult airway, labile vitals, anes problem)
yes yesPACU resident
called and given special report
Resident puts monitor on patient
EKG and blood pressure, etc.
y p writes note, documents
handoff given)
yes
no
Resident identifies nurses that are taking care of
p )
no
p p
pand hooks up
oxygen, questions why no nurses
Resident mobilizes nursing team to put on monitors
taking care of patient
Resident gives report (content
checklist)
Back-up Behavior
Resident mobilizes nursing
Nurses accept patient
Nurses arrive
Resident completes and signs PACU
ordersArora, V., Johnson, J. & Barach, P. (2007).

Resorts to operator, pill bottles, or Google to get PCP contact infoget PCP contact info

PCP finds out via active surfing of roster, or
h i llPCP “pieces together” what happens from
il bl l b & t di
coaches patient to call PCP if they go to hospital, or home health
available labs & studies
“It’s like a detective”fax “Maybe smoke signals”

What We Learned What We Learned from Process Mappingfrom Process Mapping
Understand and attempt to reduce the variation in the Understand and attempt to reduce the variation in the handoff processhandoff processpp
Keep the focus on patient care: Define clear roles and Keep the focus on patient care: Define clear roles and backback--up behaviorup behavior
HandHand--off = Transfer of information + professional off = Transfer of information + professional responsibilityresponsibility
Need to ensure “closedNeed to ensure “closed--loop” handloop” hand--off communication off communication Maps were important tools because they enabled Maps were important tools because they enabled
visualization and logical synchronization of the transfers visualization and logical synchronization of the transfers

Communication Failures During the Hand-off of Patients g
Adverse Events/Near Misses due to Poor Sign-out in Preceding Shiftn Preceding Shift
Category (n)
Sub-category (n)
Representative Incident (n=25)*(n) (n)
Content Omissions
Medications or Therapies (11)
There was a patient who had their heparin drip turned off and it was not mentioned to me that
(22) it was turned off.
Tests or Consults (10)
There was a consult that was pending that was not listed and then ID [infectious disease] and ( ) [ ]pulmonary called with recommendations and there was no note that these recommendations were coming or what I should do with them.
Active Medical Problems (9)
There was a patient that had hematuria and it was not indicated on the sign-out. They had ordered CBI [continuous bladder irrigation] and o de ed C [co t uous b adde gat o ] a dI had no idea.
Arora, et al. 2005

Testing Communication Theories:P di i I S dPediatric Intern Study
Th t i t t i f i f ti NOT The most important piece of information was NOT communicated 60% of the time – despite the sender believing it had beenp g
Did not agree on the rationale provided for 60% of items– At times contradictory (i.e. pt going home vs. pt needed to stay)
Some things more likely to be remembered…Some things more likely to be remembered…– To do items (65%) & If/then items (69%) more likely to be
remembered than knowledge items (35%), p=0.003
However, the peer assessment of handoff quality was high in spite of abovep
Chang V, et al. Pediatrics 2010

Is it a Problem with Listening?
Category Definition ExamplesDisplays of understanding
Things that make me THINK you’re listening
Nodding, eye contact, body language, positioningg g g , p g
Processing information
Things that let me KNOW you’re
Read-back, Note Taking Askinginformation KNOW you re
listening Taking, Asking Questions
Interruptions & Distractions
Things that prevent you from listening to me
Interrupting sender, checking phone, side conversations eating,listening to me conversations eating, gathering belongings

Is the Problem The Sign outs?g
When comparing meds on sign-out to i h l 1/3 dipatient charts, nearly 1/3 discrepant
– 80% contained at least 1 med omission; 40% one commission40% one commission
Omissions more common; BUT ;commissions more serious– Anticoagulants, iv antibiotics, pain
medications like narcotics, hypoglycemics (insulin etc.)
Over half had the potential to cause significant harm to patients
Arora, et al, JGIM. 2007
p g pMajority persisted after first day - mechanism failure to update

One possible One possible framework forframework for
ANTICipateANTICipateframework for framework for written signout written signout
Administrative Data □ Patient name, age, gender □ Medical record number □ Room number
1. Routine data 1. Routine data in case of in case of
□ Room number □ Admission date □ Primary inpatient medical team, primary care physician □ Family contact information
New Information (Clinical Update)emergencyemergency2. Focus on new 2. Focus on new
New Information (Clinical Update)□ Chief complaint, brief HPI, and diagnosis (or differential diagnosis) □ Updated list of medications with doses, updated allergies □ Updated, brief assessment by system/problem, with dates □ Current “baseline” status (e.g., mental status, cardiopulmonary, vital signs,
or recent or recent informationinformation3 Wh t t3 Wh t t
especially if abnormal but stable)□ Recent procedures and significant events
Tasks (What needs to be done) □ Specific, using “if-then” statements
3. What to 3. What to anticipate and anticipate and what to dowhat to do
□ Prepare cross-coverage (e.g., patient consent for blood transfusion) □ Warn of incoming information (e.g., study results, consultant recommendations
and what action, if any, needs to be taken that night
Illness what to dowhat to do□ Is the patient sick?
Contingency Planning / Code Status □ What may go wrong and what to do about it □ What has or hasn’t worked before (e g responds to 40mg IV furosemide)□ What has or hasn t worked before (e.g., responds to 40mg IV furosemide)□ Difficult family or psychosocial situations □ Code status, especially recent changes or family discussions
Vidyarthi, et al 2005

Is the h kli tchecklist
the holythe holy grail?grail?

Caution for ‘checklists’Caution for checklists Check the box mentality Check the box mentality
– Complete the form but don’t improve careCh kb f “I t t d th PCP” Checkbox for “I contacted the PCP”
Forms don’t fill out themselves– Training and frontline buy-in
One size fits all doesn’t always work y– Customization often needed (i.e. SBAR)
Sustaining behavior change difficult Sustaining behavior change difficult– Audits to ensure continued use
E f tli t ff t t i– Engage frontline staff to customize

Case of SBAR
Originated in Navy Originated in Navy to communicate critical situationscritical situations
Adapted for nurse t h i ito physician communication
Became most commonly described handoff mneumonic

Misuse of SBARMisuse of SBAR
U i “SBAR” b Using “SBAR” as a verb– “I’m SBARing”
Failing to customize and specify the precise elements in each categoryprecise elements in each category– Likely that situation for a L&D unit differs
from a geriatrics unitfrom a geriatrics unit Assumption that using SBAR checklist will
result in comprehensive informationresult in comprehensive information transfer

Improving Handoffs for NursingImproving Handoffs for NursingImproving Handoffs for NursingImproving Handoffs for Nursing Behaviors Attitudes and Perceived Risks:Behaviors Attitudes and Perceived Risks: Behaviors, Attitudes, and Perceived Risks: Behaviors, Attitudes, and Perceived Risks:
Communication of Patient Care Information Across Communication of Patient Care Information Across Shifts in Critical Care Settings Shifts in Critical Care Settings
At three different sites: At three different sites: –– The PICU, PACU, and an adult patient wardThe PICU, PACU, and an adult patient ward
Two different perspectives:Two different perspectives:–– Ethnographic observations on nurses’ and residents’ Ethnographic observations on nurses’ and residents’
behaviors and methods of communicationbehaviors and methods of communicationbehaviors and methods of communicationbehaviors and methods of communication–– Structured interviews with nurse managers, attending Structured interviews with nurse managers, attending
physicians, nurses, residents, fellows, and hospital physicians, nurses, residents, fellows, and hospital p y pp y padministrators on detailed attitudes and perceptions of risk administrators on detailed attitudes and perceptions of risk with regard to handoffswith regard to handoffs
Sharit J, Thevenin, D, Barach P, Human Factors 2005; Sharit, et al. Risk Aanlysis, 2008.

Improving Handoffs for NursingImproving Handoffs for Nursing Examples of Poor SignExamples of Poor Sign--outs (PICU Nurses)outs (PICU Nurses)
–– Omission in communicationOmission in communication OGN fails to communicate to ICN that patient is going to OGN fails to communicate to ICN that patient is going to
have a MRI that morninghave a MRI that morninghave a MRI that morninghave a MRI that morning ICN does not follow through to ensure MRI is obtainedICN does not follow through to ensure MRI is obtained Patient's treatment delayed due to poor scheduling with no Patient's treatment delayed due to poor scheduling with no y p gy p g
back up system beyond the handback up system beyond the hand--off requestoff request
–– Ambiguity in communicationAmbiguity in communication OGN indicates “I had some trouble with this port” OGN indicates “I had some trouble with this port” ICN assumes, based on the nature of the communication, ICN assumes, based on the nature of the communication,
that the port was still flushingthat the port was still flushingthat the port was still flushingthat the port was still flushing–– “After hooking everything up it didn’t work and I needed to get “After hooking everything up it didn’t work and I needed to get
meds in”meds in”“I should have asked more questions”“I should have asked more questions”–– “I should have asked more questions”“I should have asked more questions”
Sharit, McCane, Thevenin, Barach. Risk Analysis. 2008.

Influence Diagram on Nurses during Influence Diagram on Nurses during Patient HandoversPatient HandoversPatient HandoversPatient Handovers
Sharit, McCane, Thevenin, Barach. Risk Analysis. 2008.

Preliminary HypothesisPreliminary Hypothesis——Care vs. Cure?Care vs. Cure?
Nurses and physicians’ mental models of Nurses and physicians’ mental models of care differ; as a result they see patients andcare differ; as a result they see patients andcare differ; as a result, they see patients and care differ; as a result, they see patients and the handover of responsibilities differently.the handover of responsibilities differently.
These differences may lead to These differences may lead to communication breakdowns e.g., physicians communication breakdowns e.g., physicians may find nurses may find nurses to be overly detailed to be overly detailed in in giving information that may not seem giving information that may not seem g g yg g ypertinent, and nurses may see physicians as pertinent, and nurses may see physicians as focusing on diagnosis and treatment, missingfocusing on diagnosis and treatment, missingfocusing on diagnosis and treatment, missing focusing on diagnosis and treatment, missing the patient and the care processes.the patient and the care processes.

Quotes From Opportunistic Interviews With Quotes From Opportunistic Interviews With ResidentsResidents
“Yeah, it’s like the only way I can make it “Yeah, it’s like the only way I can make it manageable for my handovers is to tell manageable for my handovers is to tell g yg ythe incoming resident which patient is the incoming resident which patient is going to need what during the next 8going to need what during the next 8--1212going to need what during the next 8going to need what during the next 8 12 12 hours.” hours.” “ h h h“ h h h “I just try to give him or her the most “I just try to give him or her the most pertinent information about what has pertinent information about what has pphappened during the last shift and what t happened during the last shift and what t watch out for during the upcoming shift.”watch out for during the upcoming shift.”watch out for during the upcoming shift.watch out for during the upcoming shift.

Quotes From Opportunistic Interviews With Quotes From Opportunistic Interviews With NursesNurses
“I try to go through each patient with the “I try to go through each patient with the incoming nurse so that they can get a incoming nurse so that they can get a complete picture of what’s going on.”complete picture of what’s going on.”
“It’s important for me during shift change to“It’s important for me during shift change to It s important for me during shift change to It s important for me during shift change to provide as much information as possible so provide as much information as possible so that the person taking over the care canthat the person taking over the care canthat the person taking over the care can that the person taking over the care can judge how she will be spending her time.” judge how she will be spending her time.” “I b li i t ki th ti t f ll i f“I b li i t ki th ti t f ll i f “I believe in taking the time to fully inform “I believe in taking the time to fully inform the person replacing me about the status of the person replacing me about the status of the patients on the service.”the patients on the service.”

Preliminary Findings From A VA Study of Preliminary Findings From A VA Study of Physician and Nurse Handoffs Physician and Nurse Handoffs
Physician handoffs tend to be donePhysician handoffs tend to be done by exclusionby exclusion Physician handoffs tend to be done Physician handoffs tend to be done by exclusionby exclusion. . As a rule residents report only pertinent positives As a rule residents report only pertinent positives about patients who the incoming resident willabout patients who the incoming resident willabout patients who the incoming resident will about patients who the incoming resident will need to pay special attention to.need to pay special attention to.
Nursing handoffs tent to be muchNursing handoffs tent to be much more detailedmore detailed Nursing handoffs tent to be much Nursing handoffs tent to be much more detailed, more detailed, information rich information rich and include details on the care and include details on the care and needs of each patient regardless of theirand needs of each patient regardless of theirand needs of each patient regardless of their and needs of each patient regardless of their clinical statusclinical status
It is possible that these styles represent differentIt is possible that these styles represent different It is possible that these styles represent different It is possible that these styles represent different mental models held by nurses and physicians mental models held by nurses and physicians about patients and what is required to manageabout patients and what is required to manageabout patients and what is required to manage about patients and what is required to manage and maintain their care over time. and maintain their care over time.

Improving Patient Hospital to Community Handover Processes in EuropeHandover Processes in Europe
http://handover.eu/

Hospital to Community TransitionHospital to Community TransitionHospital to Community TransitionHospital to Community Transition

EUEU 7 G7 G HANDOVERHANDOVEREUEU--7 Grant 7 Grant -- HANDOVERHANDOVER 3 year, $5 million project to study handovers in 3 year, $5 million project to study handovers in
6 countries, awarded in October 20086 countries, awarded in October 2008 The first time the EU has funded a project on The first time the EU has funded a project on
transitions of care transitions of care A key driver was growing recognition of adverse A key driver was growing recognition of adverse
care caused by informal, non standardizedcare caused by informal, non standardizedcare caused by informal, non standardized care caused by informal, non standardized handovers and the movement of patients across handovers and the movement of patients across countriescountriescountriescountries

HANDOVER ParticipantsHANDOVER ParticipantsHANDOVER ParticipantsHANDOVER ParticipantsTh N th l dTh N th l d The NetherlandsThe Netherlands–– University Medical Centre UtrechtUniversity Medical Centre Utrecht–– Centre for Learning Sciences and Technologies (OUNL)Centre for Learning Sciences and Technologies (OUNL)Centre for Learning Sciences and Technologies (OUNL)Centre for Learning Sciences and Technologies (OUNL)–– Radboud University Medical CentreRadboud University Medical Centre
Avedis Donabedian Institute, Autonomous University of Avedis Donabedian Institute, Autonomous University of l S il S iBarcelona, SpainBarcelona, Spain
University of Birmingham, United KingdomUniversity of Birmingham, United KingdomAzienda Sanitaria Firenze ItalyAzienda Sanitaria Firenze Italy Azienda Sanitaria Firenze, ItalyAzienda Sanitaria Firenze, Italy
Karolinska Institute, SwedenKarolinska Institute, Sweden National Centre for Quality Assessment in HealthcareNational Centre for Quality Assessment in Healthcare National Centre for Quality Assessment in Healthcare, National Centre for Quality Assessment in Healthcare,
PolandPoland

Many Actors InvolvedMany Actors InvolvedFamily
Many Actors InvolvedMany Actors InvolvedFamily
PhysiciansSocial insurance office
Pharmacy
Means of assistanceMedical Service
Nurses
Medical Assistants
Pharmacy
Means of assistanceDietitian
Economic & Adm.Physiotherapist
Speech Welfare officer
Home-help i
therapistEMS
service

How are we learning about How are we learning about gghandovers in each setting?handovers in each setting?
Process analysis Process analysis Structured InterviewsStructured Interviews--MD’s, RN’s, MD’s, RN’s,
Patients, FamiliesPatients, Familiesat e ts, a esat e ts, a es Focus GroupsFocus Groups Artifact AnalysisArtifact Analysis Bayseian and Cost benefit analysis ofBayseian and Cost benefit analysis of Bayseian and Cost benefit analysis of Bayseian and Cost benefit analysis of
interventionsinterventions


PreliminaryPreliminary ResultsResultsArtifacts Patient Interviews Hospital staff
InterviewsPrimary care physician
1. From primary care
Hospital has access to primary care files in the same geographical area under the
Access to information could avoid duplication of tests: ”If they communicated [between primary
”We receive the referral information from primary care, the system is good ”
Doctor was not informed about discharge of the patient, he realized when the patient came for a follow up
to hospitalgeographical area under the same provider network.
communicated [between primary care and hospital] they didn’t have to repeat the analysis”
system is good. when the patient came for a follow up.
Barriers: Little information if patient comes on own initiative (without referral note)
Patient is admitted to various hospitals, depending on the availability of beds
Evolution of the patient is not sufficiently detailed (e.g. edema and medication)
Hospital doctors may overrule primary care doctors judgements.To speak to another health professionalreferral note) availability of beds.
Consequently, hospitals may or may not have access to information from previous episodes.
and medication)Information is missing, the system does not allow entering it.Details on current medications not sufficient.Access to records depends on geographical area
To speak to another health professional personally is very difficult.
geographical area.
Facilitators: Hospital has information on previous episodes in the same hospital and from other hospitals and primary care centre in the same purchaser network
Patient always brings previous records to hospital visits (emergency and planned admissions).
Important to hand relevant documents in paper to patients, so that they are available when needed (irrespective of access to system)
Electronic record facilitates work substantially.Direct contact with ER to coordinate specialist visit; possible because of personal contactssame purchaser network. system) personal contacts.
2. From hospital to home/primar
Hospital prepares medical and nursing discharge report, files are stored in common platform (PDF)
”...this is why they have the computers: it is very easy to pass information from one to another, b t th d ’t d it d th I
”What is clear to us is that the patient has to take the discharge note when he leaves the h it l ”
”Access to the shared medical record is the best method to check the evolution of a patient”.
home/primary care
(PDF). but they don’t do it .. and then I shouldn’t have to carry these papers back and forth...”
hospital.”
Barriers: Medical report is only for physician (patient as postman)
Hospital staff lost the full medical history that the patient brought
Not possible to access records of other providers that are not using
Does not receive information automatically about the hospital stay
from previous admissions to other hospitals.Hospital should inform primary care about ER admissions
the SAP system.Primary care doctors overrule medication.
and discharge.Within working hours there is little time to make phone calls between visits.Not knowing whom to contact. Medical record does not detail specific nursing needs.
Facilitators: Detailled medical and nursing discharge report.Patient is programmed to have a specialist follow up.
Patient hands over discharge record from hospital to the primary care physician
Discharge note inclues all details about evolution, exams, and treatment. The patient has to take it to primary care.
Hospital discharge notes are brought by patient, but also accessible in the IT system (in this primary care centre).

Bayseian Analysis

Evaluating Policy and Service Interventions: A Framework to Guide g ySelection and Interpretation of Study End Points Lilford R, et al. BMJ, 2010, in press

Ch llCh llChallengesChallenges
Different health care delivery modelsDifferent health care delivery models Different health care financing modelsDifferent health care financing models Different health care financing modelsDifferent health care financing models Different administrative challenges related to governanceDifferent administrative challenges related to governance

Training, Monitoring, Training, Monitoring, g, g,g, g,and Evaluationand Evaluation
How can you train newcomers inHow can you train newcomers inHow can you train newcomers in How can you train newcomers in handover communication?handover communication?

Interviews: SignInterviews: Sign--out training out training and evaluationand evaluation
No formal mechanisms are in place either for No formal mechanisms are in place either for instruction on how to perform signinstruction on how to perform sign--outs, or for outs, or for
l ti th il ti th i t ft fevaluating the signevaluating the sign--outs of nursesouts of nurses Senior nurses, >15 years on job, 25Senior nurses, >15 years on job, 25--45 min 45 min
t t d i t it t d i t istructured interviewsstructured interviews–– Nurse Manager (NM)#1: “Nurses are so individualized and Nurse Manager (NM)#1: “Nurses are so individualized and
patients are so individualizedpatients are so individualized it would be difficult (but notit would be difficult (but notpatients are so individualizedpatients are so individualized——it would be difficult (but not it would be difficult (but not impossible) to standardize the process”impossible) to standardize the process”
–– NM#2: “You buddy up with a senior nurse for a finite NM#2: “You buddy up with a senior nurse for a finite y py pperiod and learn from that nurse what should be period and learn from that nurse what should be communicated to the next shift”communicated to the next shift”
Sharit, McCane, Thevenin, Barach. Risk Analysis. 2008.

Patient SimulatorsPatient Simulators

Immersive Learning Immersive Learning d ld land Simulationand Simulation
Long history of successful use of standardized Long history of successful use of standardized patients to teach medical students patients to teach medical students (Harden, et al, (Harden, et al, 1975)1975)
–– Communication and clinical skillsCommunication and clinical skills Observed Structured Clinical Exam OSCE (USMLE clinical skills)Observed Structured Clinical Exam OSCE (USMLE clinical skills)Observed Structured Clinical Exam OSCE (USMLE clinical skills) Observed Structured Clinical Exam OSCE (USMLE clinical skills)
Recent innovative adaptations of “OSCE” t t h t diti l bj t“OSCE” to teach non-traditional subjects
–Quality improvement/PBLI (Varkey, et al, 2008)–Objective Structured TEACHING Exercise (OSTE) (Stone, et al, 2003)Objective Structured TEACHING Exercise (OSTE) (Stone, et al, 2003)–Teach patient safety competencies using simulation (Barach P, Mayer D., 2005)

OSHE (Objective Simulated OSHE (Objective Simulated HandHand--off Experience)off Experience)
10 minutes to review mock patient H&P Based on actual patientp
Mrs. H is a 68y/o Caucasian female with a history of COPD, HTN and DM2 presenting via the ED c/o SOB x 3 days
H&P including routine data for sign-outf d i i h di ti reason for admission, home medications,
code status, PCP and contact information for f ilfamily
Farnan, et al. JGIM 2009

CEXCEXCEXCEX 5 minute “interval patient 5 minute “interval patient
events” videoevents” video Contains important clinical Contains important clinical
updates to trigger anticipatory updates to trigger anticipatory p gg p yp gg p yguidance & toguidance & to--do itemsdo items–– FollowFollow--up on labsup on labs
“Remember to tell your cross“Remember to tell your cross-- Remember to tell your crossRemember to tell your crosscover to take a peek at the cover to take a peek at the potassium on the 10PM BMP”potassium on the 10PM BMP”
–– Oxygen requirementOxygen requirementOxygen requirementOxygen requirement “Dr., the patient is looking “Dr., the patient is looking
more tachypneic and is more tachypneic and is hypotensive”hypotensive”
–– Family meetingFamily meeting

HandHand--off CEXoff CEXHandHand off CEXoff CEX Based on “MiniBased on “Mini-- CEX” CEX”
instrument widely used ininstrument widely used ininstrument widely used in instrument widely used in internal medicine internal medicine (Norcini, et al, 2003)(Norcini, et al, 2003)
Domains assessed:Domains assessed:–– Organization/EfficiencyOrganization/EfficiencyOrganization/EfficiencyOrganization/Efficiency–– Communication skillsCommunication skills–– Clinical judgmentClinical judgment–– ProfessionalismProfessionalism
99 point scalepoint scale 99--point scale point scale
Adapted to nursing andAdapted to nursing and Adapted to nursing and Adapted to nursing and Hospitalists Hospitalists

Peer EvaluationsPeer EvaluationsPeer EvaluationsPeer EvaluationsCompetencyCompetency based peer evaluation of handoffsbased peer evaluation of handoffs CompetencyCompetency--based peer evaluation of handoffsbased peer evaluation of handoffs
Administered to interns through New Innovations at Administered to interns through New Innovations at end of inpatient general medicine monthend of inpatient general medicine monthend of inpatient general medicine monthend of inpatient general medicine month
Anonymously evaluate coAnonymously evaluate co--interns oninterns on
•Delivering signout (updated written sign-out)R i i i t (li t i b h i •Receiving signout (listening behavior, cross-
cover, documentation of overnight events.)

Handoffs are a Two Way StreetHandoffs are a Two Way Street
B d d Best understood as a dialogue – an interaction that fosters
common ground, h dempathy, and equity to
transfer necessary informationinformation
Sender must paint a pictureSender must paint a picturereceiver must see it, understand it, act on it, and, ultimately communicate it to someone else
Gibson CS, et al. Ann Emerg Med 2009
ultimately, communicate it to someone else

What Can Senders Do?What Can Senders Do?Think about the “R”eceiver (4Rs) Think about the “R”eceiver (4Rs)
Relevant items that will be Remembered Relevant items that will be Remembered– Focus on sickest patients first – Daily progress (today’s baseline, updated events)
Di ti T D It d If/th it– Direction To Do Items and If/then items
Directions with Rationale Directions with Rationale – avoid ambiguity “check CBC” without giving a reason why
and what to do with results
Check for receiver understanding– Encourage questions and read-backEncourage questions and read back– Overcome egocentric heuristic (think about receiver)

What Can Receivers Do?What Can Receivers Do?
A ti l li t Actively listen– stay focused, limit interruptions, taking notes can
enhance memoryenhance memory Ask questions
to ensure you understand directions– to ensure you understand directions – the handoff is your learning opportunity
Use a system Use a system – to keep track of to do items that require your action
Readback Readback – directions to ensure you are on the same page

ConclusionsConclusionsConclusionsConclusions

Elements of Effective Hand OffsElements of Effective Hand OffsElements of Effective Hand OffsElements of Effective Hand Offs
Efficient/effective communicationEfficient/effective communicationA ti i t M tA ti i t M tAnticipatory ManagementAnticipatory ManagementContinuity of care (technical andContinuity of care (technical andContinuity of care (technical and Continuity of care (technical and from the patient’s perspective)from the patient’s perspective)from the patient s perspective)from the patient s perspective)Interprofessional collaboration/ Interprofessional collaboration/ p /p /
teamworkteamwork

Risk Stratifying Care TransitionsRisk Stratifying Care TransitionsI th ti t h i ll i ?1. Is the patient physically moving?
2. Is the patient critical or unstable?
3. Is the hand-off temporary or p ypermanent?
4. Is this the first time the receiver4. Is this the first time the receiver is hearing about a patient?
If yes to any question, inherent increase in safety risk

The TeamSTEPPS FrameworkThe TeamSTEPPS FrameworkThe TeamSTEPPS FrameworkThe TeamSTEPPS Framework
KnowledgeKnowledge–– Shared Mental ModelShared Mental Model
AttitudesAttitudes–– Mutual TrustMutual Trust–– Team OrientationTeam Orientation
PerformancePerformance–– AdaptabilityAdaptability
AccuracyAccuracy–– AccuracyAccuracy–– ProductivityProductivity–– EfficiencyEfficiency–– SafetySafetyyy
Baker D, Salas E, Battles J, King H, Barach P, 2005, 2006, 2008

Handover Skills as Part of Training Handover Skills as Part of Training Teams and the MicrosystemTeams and the Microsystem
Handovers are essential link and skill of effective clinical Handovers are essential link and skill of effective clinical microsystemsmicrosystems
Team based handoff training has higher chance of Team based handoff training has higher chance of sustainabilitysustainabilityH ldi li i l b f th i tH ldi li i l b f th i t Holding clinical members of the microsystem Holding clinical members of the microsystem accountable for their behaviorsaccountable for their behaviors
Salas E, Baker D, King H, Battles J. Barach P. On Teams, Organizations and Safety.Salas E, Baker D, King H, Battles J. Barach P. On Teams, Organizations and Safety. Joint Joint Commission Journal on Quality and SafetyCommission Journal on Quality and Safety 20062006;32:109;32:109--112.112.
Barach P Johnson J Team Based Learning in MicrosystemsBarach P Johnson J Team Based Learning in Microsystems An Organizational Framework forAn Organizational Framework for Barach P, Johnson J. Team Based Learning in MicrosystemsBarach P, Johnson J. Team Based Learning in Microsystems--An Organizational Framework for An Organizational Framework for Success. Success. Technology, Instruction, Cognition and Learning, 2006;3:307Technology, Instruction, Cognition and Learning, 2006;3:307--321.321.
Johnson J, Barach P. Handovers of Patient Care: What Will it Take to Ensure Quality and Safety Johnson J, Barach P. Handovers of Patient Care: What Will it Take to Ensure Quality and Safety During Times of Transition? During Times of Transition? Medical Journal of AustraliaMedical Journal of Australia 2009; 190(11): S1102009; 190(11): S110--S112.S112.

What isWhat is GeneralizableGeneralizable??What is What is GeneralizableGeneralizable??
The Model:The Model:–– A process and content driven improvementA process and content driven improvementA process and content driven improvement A process and content driven improvement
strategystrategy
The Approach to Implementation andThe Approach to Implementation and The Approach to Implementation and The Approach to Implementation and MonitoringMonitoring–– Collaborative format, team driven Collaborative format, team driven
improvement, coupled with researchimprovement, coupled with research

Challenges/OpportunitiesChallenges/OpportunitiesChallenges/OpportunitiesChallenges/Opportunities
Addressing organizational, cultural, Addressing organizational, cultural, professional barriers professional barriers pp
Sustainability Sustainability C ti l l l d hiC ti l l l d hi Creating local leadershipCreating local leadership
Training, Monitoring, and EvaluationTraining, Monitoring, and EvaluationTraining, Monitoring, and EvaluationTraining, Monitoring, and Evaluation Can we prove that our interventions make Can we prove that our interventions make
a diffe encea diffe encea differencea difference

Lessons LearnedLessons Learnedesso s ea edesso s ea ed
Handovers are an integral to the daily clinical workHandovers are an integral to the daily clinical work–– Improvement must be driven by those doing the handoversImprovement must be driven by those doing the handovers
There’s the research, but then there’s the improvement There’s the research, but then there’s the improvement –– Improving handovers were a vehicle for teaching improvement Improving handovers were a vehicle for teaching improvement
skillsskillsskillsskills–– The best way to learn about improvement is by trying to The best way to learn about improvement is by trying to
improveimprove
There are cultural differences, There are cultural differences, but at some level we have the but at some level we have the
d d thd d thsame needs and the same same needs and the same problems problems –– Local solutions may varyLocal solutions may varyLocal solutions may varyLocal solutions may vary

Challenges/OpportunitiesChallenges/Opportunitiesg / ppg / pp
SustainabilitySustainabilityyy–– What happens when you are What happens when you are
“done” with the project? “done” with the project? p jp j–– How do you sustain the How do you sustain the
improvement?improvement? Identify local championsIdentify local champions Build around microsystemBuild around microsystem
BuildBuild in process monitoring andin process monitoring and BuildBuild--in process monitoring and in process monitoring and evaluation from the beginningevaluation from the beginning
Connect to present clinical and Connect to present clinical and pporganizational processesorganizational processes
Arora, VM; Johnson, J. “Spreading and Sustaining Use of Standardized Handoff Protocols for Residency Training ” In: Implementing and Sustaining Improvements inArora, VM; Johnson, J. “Spreading and Sustaining Use of Standardized Handoff Protocols for Residency Training ” In: Implementing and Sustaining Improvements inProtocols for Residency Training. In: Implementing and Sustaining Improvements in Health Care. USA: Joint Commission Publishing. 2009. pp 88-97.
Johnson J, Barach, Medical J of Austraralia, 2009.
Protocols for Residency Training. In: Implementing and Sustaining Improvements in Health Care. USA: Joint Commission Publishing. 2009. pp 88-97.
Johnson J, Barach, Medical J of Austraralia, 2009.

Challenges/OpportunitiesChallenges/OpportunitiesChallenges/OpportunitiesChallenges/Opportunities
Local leadershipLocal leadership–– All change is localAll change is localAll change is localAll change is local–– The research team can’t improve the process The research team can’t improve the process
that is being studiedthat is being studied ---- this has to bethis has to bethat is being studied that is being studied this has to be this has to be accomplished by those at the front linesaccomplished by those at the front linesLocal champions are necessary to lead andLocal champions are necessary to lead and–– Local champions are necessary to lead and Local champions are necessary to lead and manage the improvement piece manage the improvement piece Ch i d t b t d (th ’tCh i d t b t d (th ’t–– Champions need to be nurtured (they won’t Champions need to be nurtured (they won’t necessarily know what to do)necessarily know what to do)

Does the training make a difference on patient care?
Entin, Lei Barach P. Surgical Innovation 2006;13:170-179.

Future workFuture work
We are still in the early stages of work on We are still in the early stages of work on handoffshandoffs
Continue researchContinue research–– Identify “vulnerable gaps” across the continuum of Identify “vulnerable gaps” across the continuum of
care, e.g., admission, care during hospitalization, care, e.g., admission, care during hospitalization, discharge planning, transition to ambulatory care, discharge planning, transition to ambulatory care, physician patient relationship/communication in physician patient relationship/communication in ambulatory visitsambulatory visitsambulatory visits ambulatory visits
–– Human factors and ergonomic issues that impede Human factors and ergonomic issues that impede hand offshand offshand offshand offs
We might have very difficult time proving We might have very difficult time proving h h dh h dthat interventions have sustained impact that interventions have sustained impact

Two Brains Steve Martin VideoTwo Brains Steve Martin VideoTwo Brains Steve Martin VideoTwo Brains Steve Martin Video

Questions or Ideas?Questions or Ideas?QQ
Contact Us:Contact Us: Vineet AroraVineet Arora [email protected]@uchicago.edu Paul BarachPaul Barach [email protected]@umcutrecht.nl Rich FrankelRich Frankel [email protected]@iupui.edu Julie JohnsonJulie Johnson [email protected]@unsw.edu.au
For copies of our Papers and/or Tools in this talk, contact usFor copies of our Papers and/or Tools in this talk, contact us