Haemodynamics in PAH: Long Term Outcomes and Importance in … · 2015-07-07 · Haemodynamics in...
55
Haemodynamics in PAH: Long Term Outcomes and Importance in Guiding PAH–Specific Therapy Dr. Peter Steele Director of Cardiology Royal Adelaide Hospital South Australia
Transcript of Haemodynamics in PAH: Long Term Outcomes and Importance in … · 2015-07-07 · Haemodynamics in...

Haemodynamics in PAH:
Long Term Outcomes and
Importance in Guiding
PAH–Specific Therapy
Dr. Peter Steele
Director of Cardiology
Royal Adelaide Hospital
South Australia




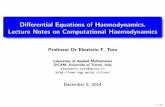
Schematic Progression of PAH
Time
PAP
PVR
CO
Pre-symptomatic/
Compensated
Symptomatic/
Decompensating
Symptom Threshold
Right Heart
Dysfunction
Declining/
Decompensated
CO=PAP
PVR
Galiè N, Rubin LJ. J Am Coll Cardiol 2004;43(12 Suppl S):1S. Rich S. Progress Cardiovasc Diseases 1988;31(3):205-38.
Humbert MD et al. N Engl J Med 2004;351:1425-36. D’Alonzo GE et al. Ann Intern Med 1991;115:343-49.

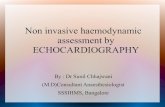
ΔP ( pressure )
Q ( output )=
MPA – PCWPPVR
CO=
MPA – PCWPPVRI
CI*=
*CI = adjusted for BSA
(Dyn. sec cm -5) = 1 Wood unit x 80
R (resistance)
Ohm’s Law (hydrodynamic form)

Haemodynamics in PAH
– Cardiac Catheter
• PA, RA, wedge pressures
• Shunts
• Oxygen saturations
• Cardiac output
• PVR calculation
• Left heart disease
• Pulmonary angiography
• Vasodilator challenge

Haemodynamics in PAH
– Importance
• Definition of PAH (mPAP>25mmHg,with a
normal wedge pressure <15mmHg)
• Diagnosis (exclusions, cardiac catheter)
• Prognosis
• Assessment/selection of treatment

Primary Pulmonary Hypertension:
Natural History and the Importance
of Thrombosis
VALENTIN FUSTER, M.D., *PETER M. STEELE, M.B.B.S. (Hons), F.R.A.C.P.
WILLIAM D. EDWARDS, M.D., BERNARD J. GERSH, M.B., CH.B, D. PHIL.,
MICHAEL D. MCGOON M.D., and ROBERT L. FRYE, M.D.
Circulation 70, No.4, 580–587, 1984.
Fuster V et al. Circulation 1984;70(4):580-7.

Mean Range
Pulmonary arterial pressure (mm Hg)
Peak 98 53 – 208
Mean 64 36 – 120
Pulmonary index, (l/min/m2 ) 2.2 0.7 – 5.0
Total pulmonary resistance (Um2) 33 11 – 95
Right ventricular end-diastolic
pressure (mmHg) 13 2 – 30
Right ventricular work index
(kg/min/m2) 1.6 0.4 – 5.8
Systemic arterial oxygen saturation (%) 91 42 – 99
Pulmonary arterial oxygen saturation (%) 60 20 – 80
Haemodynamic features at
diagnosis
Fuster V et al. Circulation 1984;70(4):580-7.

Data were obtained at entry into study from the 115 patients who survived diagnostic heart catheterisation
Factor p value
Pulmonary arterial oxygen saturation < .00001*
Systemic arterial oxygen saturation <.00001
Total pulmonary resistance <.00001
Right ventricular end-diastolic pressure .004
Pulmonary artery pressure, mean .006
Pulmonary index .009
Anticoagulant therapy .02*
Cardiomegaly .03
Age .2
Right ventricular work index .3
Sex .9
Univariate Analysis of
Prognostic Factors
Fuster V et al. Circulation 1984;70(4):580-7.

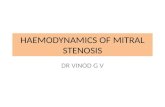
Percent
surviving
100
90
80
70
60
50
40
30
20
10
1
(62)
(24)
(7)
109876543210
Years
Observed survival to 10 years of patients
with primary pulmonary hypertension
Fuster V et al. Circulation 1984;70(4):580-7.

Results of the NIH registry
D`Alonzo et al Ann Int Medicine 1991

Validation of the
prognostic Equation
Sandoval et al 1994, Circulation

Haemodynamic prognostic indicators
iPAH
McLaughlin et al CHEST 2004

Haemodynamic prognostic
indicators
McLaughlin et al CHEST 2004

Haemodynamics in PAH
– Clinical Relevance
• Advanced disease – death predicted by RV failure (low CO, high RAP, poor RV)
• RV function assessment difficult (MRI better)
• CO/PAWP measurement errors (TR etc.)
• PA pressure alone not accurate
• RA pressure load dependent
• PVR (includes CO) most important indicator of disease status

Drug Study No. of pts D 6 MWD at
3-4 mths
P value
Bosentan BREATHE 1
NEJM 2002
213 + 44 < 0.001
Ambrisentan Galie et al,
JACC 2005
64 + 36* < 0.001
Sitaxsentan STRIDE 1,
AJRCCM 2004
178 + 34 < 0.01
Prostacyclin
(IV)
Meta-Analysis,
Cochrane, 2005
196 + 90 < 0.0002
Iloprost
(Inhaled)
AIR,
NEJM, 2002
203 + 36 0.004
Treprostinil
(SC)
Simmoneau,
AJRCCM, 2002
470 + 16 0.006
Beraprost ALPHABET,
JACC, 2002
130 + 25 0.036
Sildenafil SUPER-1,
NEJM, 2005
278 + 45-50 < 0.001
(* vs baseline, all other trials vs placebo)

ΔP ( pressure )
Q ( output )=
MPA – PCWPPVR
CO=
MPA – PCWPPVRI
CI*=
*CI = adjusted for BSA
(Dyn. sec cm -5) = 1 Wood unit x 80
R (resistance)
Ohm’s Law (hydrodynamic form)

Iloprost

Air Study
Olschewski, H et al, 2002

Olschewski, H et al, 2002

Sildenafil

Super 1
Galie et al NEJM 2005

Haemodynamic response
12 weeks therapy
Galie et al NEJM 2005

Epoprostenol

Barst et al, NEJM 1996

Haemodynamic response at 12 weeks therapy
Barst et al, NEJM 1996

Bosentan

Bosentan Baseline Haemodynamics
Channick et al, 2001 LANCET

Bosentan Haemodynamic response to
treatment after 12 weeks
Channick et al, 2001 LANCET

Bosentan in WHO FC II patients
EARLY Baseline characteristics
Placebo (n=92) Tracleer (n=93)
Mean time from diagnosis,
years
3.7 2.9
Aetiology, n (%)
PPH
CHD
SSc
Other
58 (63%)
16 (17.4%)
5 (5.4%)
13 (14.2%)
54 (58.1%)
16 (17.2%)
9 (9.7%)
14 (15%)
Mean 6MWD, m ± SD 430.9 ± 91.9 442.5 ± 82.9
Mean PVR, dyn.sec.cm5 ±
SD
802 ± 365 851 ± 535
Galie et al ESC, 2007

Haemodynamics
Change from baseline to month 6 v’s placebo
• mPAP treatment effect - 5.7mmHg
p =<.0001
• TPR treatment effect - 207 (dyn.sec/cm5)
p =<.0001
• Cardiac Index treatment effect 0.24 L/ mn/m2
p = 0.0249
• SVO2 treatment effect 4.8% increase
p = 0.0020
Galie et al ESC, 2007

Drug Treatment effect
Cardiac
index
PVR mRAP
Bosentan
SItaxentan (100mg)
1.0 L/Min/m2
0.3 L/Min/m2
415 dyn
270 dyn
-6.2 mmHg
-1 mmHg
Prostacyclin (IV) 0.5 L/Min/m2 400 dyn -2.3 mmHg
Sildenafil
20mg
80mg
0.23 L/Min/m2
0.39 L/Min/m2
171 dyn
310 dyn
-1.1 mmHg
-1.3 mmHg
Iloprost
Pre inhalation
Post inhalation
0.12 L/Min/m2
0.37 L/Min/m2
105 dyn
335 dyn
+1.9 mmHg
+0.6 mmHg

How do these haemodynamic
changes translate into long
term outcomes?

Iloprost
Optizs et al Eur Heart Journ, 2005

Inhaled Iloprost
– Long term efficacy
Opitz et al, Eur Heart J, 2005 Sep;26(18):1895-902
** Bosentan
McLaughlin et al, Eur Resp J, 2005
Event-free survival (freedom from death, transplantation, switch to
Intravenous therapy, or additional oral therapy)
Cu
mu
lati
ve
eve
nt-
fre
e s
urv
iva
l (%
)

SUPER 2 Study
277 149No. at risk:
(Data on file. Pfizer Inc, New York, NY.)
88%
All patients up titrated
to 80mgs TID

Bosentan observed and predicted
survivalKaplan-Meier survival estimates with 99% CI
0 6 12 18 24 30 36 months
169 Patients at risk167 163 153 113 23 16
0102030405060708090
100
Event Rate / year (exponential): 5.5%% o
f event-
fre
e p
atients
Predicted (NIH 2)
Observed 1
2 D’Alonzo et al, Ann Intern Med 1991; 115:343
1 Mc Laughlin et al, Eur Resp J 2005; 25:244-249
96%
69%
92%

Only RCT to show improvements in
Survival – IV Epoprostenol
Barst et al, NEJM, 1996

Matched cohort
Sitbon, THORAX 2005

Drug Treatment effect
Cardiac
index
PVR mRAP
Bosentan
SItaxentan (100mg)
1.0 L/Min/m2
0.3 L/Min/m2
415 dyn
270 dyn
-6.2 mmHg
-1 mmHg
Prostacyclin (IV) 0.5 L/Min/m2 400 dyn -2.3 mmHg
Sildenafil
20mg
80mg
0.23 L/Min/m2
0.39 L/Min/m2
171 dyn
310 dyn
-1.1 mmHg
-1.3 mmHg
Iloprost
Pre inhalation
Post inhalation
0.12 L/Min/m2
0.37 L/Min/m2
105 dyn
335 dyn
+1.9 mmHg
+0.6 mmHg

Haemodynamics in PAH
– Summary
• Haemodynamic data predicts survival
(CO, RAP, PAP, PVR)
• Clinical correlation critical
• PVR best indicator of disease status
• Cardiac catheter essential
• Drugs with greater PVR reduction appear
to produce better long term clinical
outcomes


Sitaxentan

Sitaxentan treatment effect – 100mg OD
• PVR - 270 dyns
• CI +0.3 l/min

What about Time to Clinical
Worsening?
Does this paint a picture of
Morbidity and Mortality in PAH?

BREATHE-1: Time to clinical worsening
in WHO FC III and IV PAH patients
Bosentan
125/250 mg bid
Rubin LJ, et al. N Eng J Med 2002; 346:896-903.
Eve
nt-
fre
e (
%)
Time (weeks)
0 4 8 12 16 20 24 28
p < 0.01
50
75
100
Placebo
p < 0.004
0
144
69
142
68
31
10
141
63
138
62
103
48
25
7
13
3
Patients at riskBosentanPlacebo

Galiè N, et al. N Engl J Med 2005; 353:2148-57.
Sildenafil: SUPER-1Time to clinical worsening
Placebo
(n = 70)
Sildenafil
20 mg
(n = 69)
Sildenafil
40 mg
(n = 67)
Sildenafil
80 mg
(n = 71)
Proportion worsened (%) 10 4 3 7
(95% CI) (3.17) (0.9) (0.7) (1.13)
Incidence of clinical
worsening events
Death 1 (1) 1 (1) 0 (0) 2† (3)
Lung transplantation 0 (0) 0 (0) 0 (0) 0 (0)
Hospitalisation due to PH 7 (10) 2 (3) 2 (3) 2 (3)
Initiation of prostacyclin 1 (1) 0 (0) 0 (0) 0 (0)
Initiation of bosentan 0 (0) 0 (0) 1 (2) 2 (3)
†1 patient died during the 1st week whilst receiving sildenafil 40 mg

BOSENTAN SITAXENTAN AMBRISENTAN SILDENAFIL
Study 351 BREATHE-1 EARLY STRIDE-1 STRIDE-2 ARIES-1 ARIES-2 SUPER-1
6-MWD, m+76,
p = 0.021
+44,
p < 0.001
+19.1
NS
100/300mg:
+35/+33,
p < 0.01
50 mg: NS
100 mg:
+31.4,
p = 0.03
5mg:
+30.6,
p = 0.0084
10mg: +51.4
p = 0.0001
2.5mg:
+32.3,
p = 0.0219
5mg: +59.4
p = 0.0002
20/40/80 mg:
+45/+46/+50
p < 0.001
WHO class p = 0.0039 p = 0.0407
p-value
not
quoted
p < 0.02
50 mg: NS
100 mg:
p <0.04
NS NS p ≤ 0.003
PVR,
dyn·s·cm-5 -415,
p ≤ 0.001
23%,
p < 0.0001
100/300mg:
-221/-194,
p < 0.001
20/40 mg:
-122/-143,
p = 0.01
80 mg:
-261,
p < 0.001
TTCW p = 0.033 p = 0.002 p = 0.0114 NS NS NS
2.5 mg:
p = 0.0048
5 mg:
p = 0.0076
NS
Clinical endpoints:
Summary table

Sitaxentan base line
haemodynamics
Barst et al, AJRCCM 2003

EARLY: Time to clinical worsening in
WHO FC II PAH patients
Patients are censored at the end of the study
100
80
60
40
20
00 4 8 12 16 20 2824 32
92 90 89 86 84 83 1877 9
93 92 87 85 84 83 2780 15
Weeks from treatment start
Patients
witho
ut
the e
vent
(%)
Patients at risk
Placebo
Bosentan
p = 0.0114; log rank
Hazard ratio = 0.227
(95% CL: 0.065, 0.798)
Galiè N, et al. Presented at ESC 2007.
Time to clinical worsening in WHO FC II PAH patients

Sitaxentan: STRIDE programmeTime to clinical worsening
Parametera
STRIDE-1 STRIDE-2
Placebo
(n = 60)
100 mg sitaxentan
(n = 55)
300 mg sitaxentan
(n = 63)
Placebo
(n = 62)
50 mg sitaxentan
(n = 62)
100 mg sitaxentan
(n = 61)
Time to clinical worsening
Delay in time to clinical worsening p = NS p = NS p = 0.27 p = 0.08
No. of clinical worsening events, n
(%)3 (5) 0 (0) 1 (2) 10 (16) 6 (10) 4 (7)
Hospitalisation for PAH 4 (6) 1 (2) 1 (2)
Death Not quoted 0 (0) Not quoted 0 (0) 0 (0) 0 (0)
Transplantation Not quoted 0 (0) Not quoted 0 (0) 0 (0) 0 (0)
Initiation of new chronic PAH
therapyNot quoted 0 (0) Not quoted 4 (6) 4 (6) 3 (5)
Atrial septostomy Not quoted 0 (0) Not quoted 0 (0) 0 (0) 0 (0)
WHO FC deterioration and ≥ 15%
decrease in 6-MWD2 (3) 1 (2) 0 (0)
aAll p-values derived from comparisons with placebo unless otherwise stated
Barst RJ, et al. Am J Respir Crit Care Med 2004; 169:441-7.
Barst RJ, et al. J Am Coll Cardiol 2006; 47:2049-56.

Time to clinical worsening* in RCTs
Trial Agent p-value
Study 351 Bosentan p <0.051
BREATHE-1 Bosentan p <0.052
SUPER-1 Sildenafil NS3
STRIDE-1 Sitaxentan NS4
STRIDE-2 Sitaxentan NS5
ARIES-1 Ambrisentan NS6
ARIES-2 Ambrisentan p <0.057
EARLY Bosentan p <0.058
1.Channick RN, et al. Lancet 2001. 2.Rubin LJ, et al. NEJM 2002. 3.Galiè N, et al. NEJM 2005.
4.Barst RJ, et al. AJRCCM 2004. 5.Barst RJ, et al. JACC 2006. 6.Oudiz R, et al. Chest Meeting Abstracts
2006. 7.Olschewski H, et al. ATS 2006. 8.Galiè N, et al. Presented at ESC 2007.
*Combined end point of death, lung transplantation, hospitalisation for pulmonary hypertension, lack of clinical improvement or worsening leading to discontinuation, need for epoprostenol therapy, or atrial septostomy

Study 351: Time to clinical worsening in
WHO FC III PAH patients
Eve
nt-
fre
e (
%)
Time (weeks)
0 4 8 12 16 20 24 28100
50
75
100
0
Bosentan
Placebo
21
11
21
11
7
1
21
10
21
8
12
4
6
1
2
1
p < 0.05
Channick RN, et al. Lancet 2001; 358:1119-23.