
Haemangioma of the optic disc
3
Graefe's Arch Clin Exp Ophthalmol (1990)228:332-334 Graefe's Archive for Clinical and Experimental Ophthalmology © Springer-Verlag1990 Haemangioma of the optic disc Mark Benson, Christopher Mody, Ian Rennie, and John Talbot Department of Ophthalmology, Royal Hallamshire Hospital, Sheffield$10 2JF, United Kingdom Received September 1, 1989 / Accepted November 28, 1989 Abstract. Isolated capillary haemangiomata of the optic disc are uncommon; they may be associated with the von Hippel-Lindau syndrome. Renal carcinoma occurs in almost one-third of patients with this condition, and it may go unnoticed until metastases occur. Early ne- phrectomy offers a cure. It is important, therefore, that all patients with optic disc capillary haemangiomata as well as their relatives are referred for screening for the stigmata of this disease. Introduction Isolated capillary haemangiomata of the optic disc are uncommon. When such lesions are discovered, it is im- Offprint requests to: M.T. Benson portant that the patients and their relatives be screened for other lesions found in the Von Hippel-Lindau syn- drome. We present a case that illustrates this point. Case report A 40-year-old man went to his oculist with presbyopic symptoms. A vascular lesion at the right optic disc was noted and referral to the ophthalmic clinic was made. Medical and family history were negative. The patient's visual acuity was 6/6 in each eye, without correction. The right optic disc was almost completely obscured by a large, elevated, orange-red tumour (Fig. 1). No other ocular abnormality was found in either eye. Fluorescein angiography showed some leakage from the tumour (Fig. 2). Fig. 1. A large, elevated capillary haemangioma almost completely Fig. 2. Fluorescein angiogram showing leakage of dye from the obscuring the right optic disc angioma
-
Upload
mark-benson -
Category
Documents
-
view
215 -
download
2
Transcript of Haemangioma of the optic disc
Graefe's Arch Clin Exp Ophthalmol (1990)228:332-334 Graefe's Archive for Clinical and Experimental
Ophthalmology © Springer-Verlag 1990
Haemangioma of the optic disc Mark Benson, Christopher Mody, Ian Rennie, and John Talbot
Department of Ophthalmology, Royal Hallamshire Hospital, Sheffield $10 2JF, United Kingdom
Received September 1, 1989 / Accepted November 28, 1989
Abstract. Isolated capillary haemangiomata of the optic disc are uncommon; they may be associated with the von Hippel-Lindau syndrome. Renal carcinoma occurs in almost one-third of patients with this condition, and it may go unnoticed until metastases occur. Early ne- phrectomy offers a cure. It is important, therefore, that all patients with optic disc capillary haemangiomata as well as their relatives are referred for screening for the stigmata of this disease.
Introduction
Isolated capillary haemangiomata of the optic disc are uncommon. When such lesions are discovered, it is im-
Offprint requests to: M.T. Benson
portant that the patients and their relatives be screened for other lesions found in the Von Hippel-Lindau syn- drome. We present a case that illustrates this point.
Case report
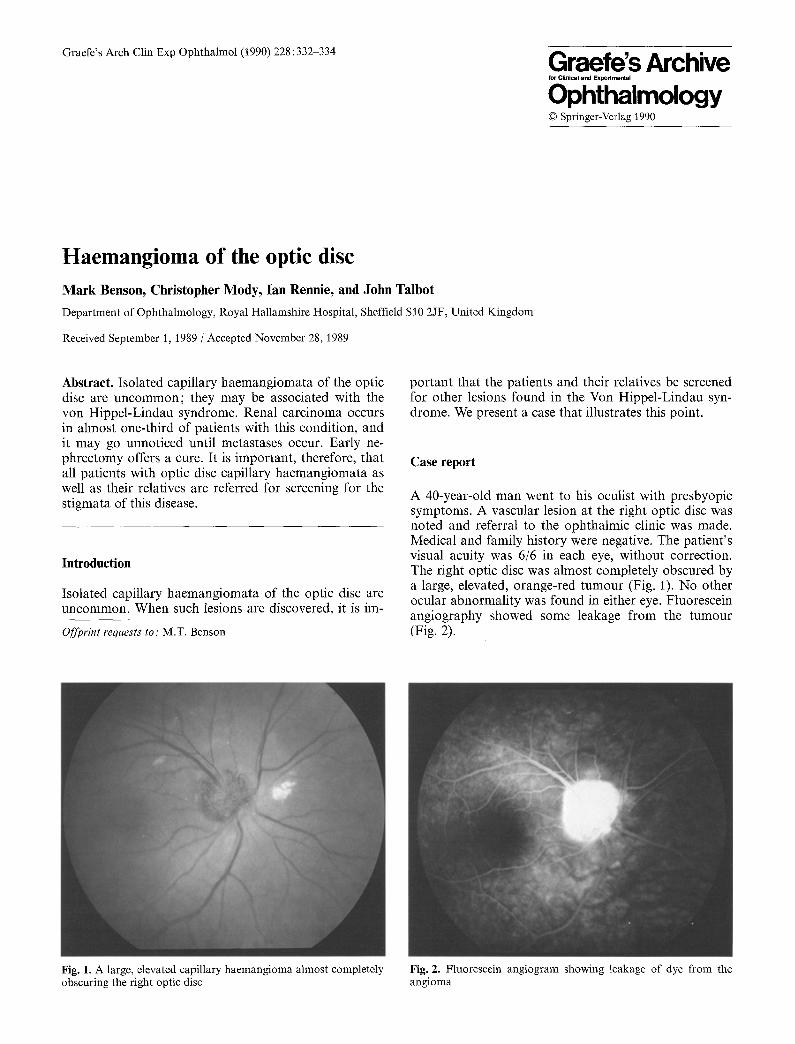
A 40-year-old man went to his oculist with presbyopic symptoms. A vascular lesion at the right optic disc was noted and referral to the ophthalmic clinic was made. Medical and family history were negative. The patient's visual acuity was 6/6 in each eye, without correction. The right optic disc was almost completely obscured by a large, elevated, orange-red tumour (Fig. 1). No other ocular abnormality was found in either eye. Fluorescein angiography showed some leakage from the tumour (Fig. 2).
Fig. 1. A large, elevated capillary haemangioma almost completely Fig. 2. Fluorescein angiogram showing leakage of dye from the obscuring the right optic disc angioma
333
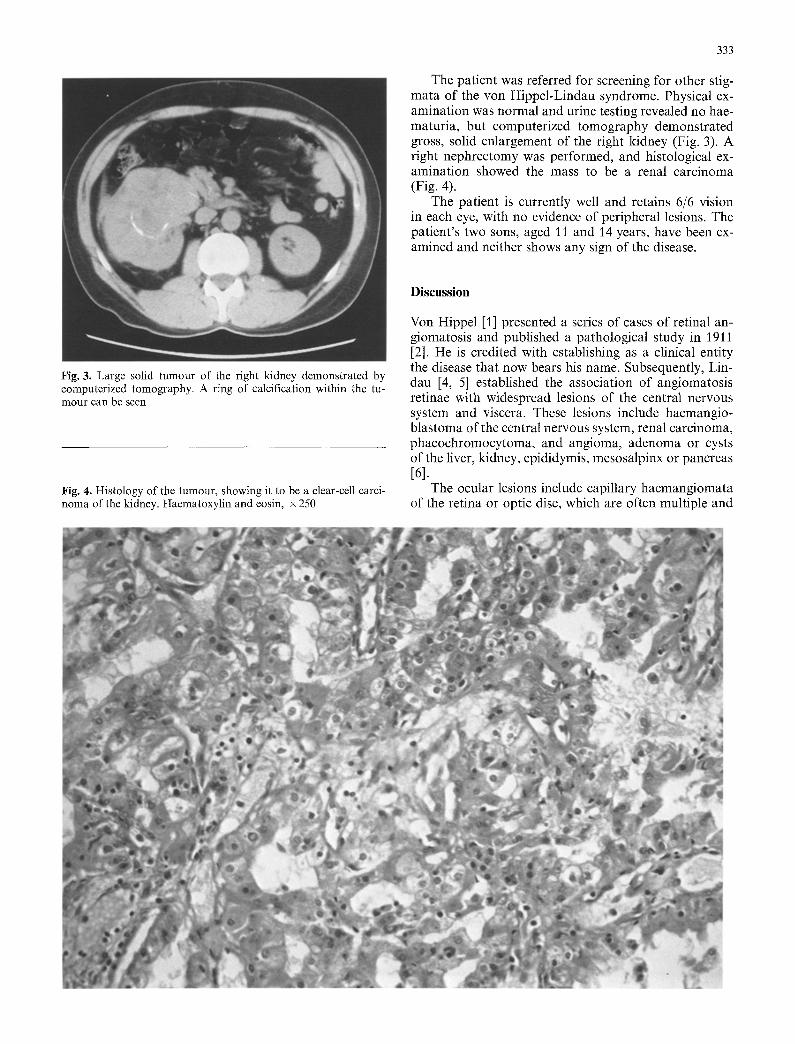
The patient was referred for screening for other stig- mata of the von Hippel-Lindau syndrome. Physical ex- amination was normal and urine testing revealed no hae- maturia, but computerized tomography demonstrated gross, solid enlargement of the right kidney (Fig. 3). A right nephrectomy was performed, and histological ex- amination showed the mass to be a renal carcinoma (Fig. 4).
The patient is currently well and retains 6/6 vision in each eye, with no evidence of peripheral lesions. The patient's two sons, aged 11 and 14 years, have been ex- amined and neither shows any sign of the disease.
Fig. 3. Large solid tumour of the right kidney demonstrated by computerized tomography. A ring of calcification within the tu- mour can be seen
Fig. 4. Histology of the tumour, showing it to be a clear-cell carci- noma of the kidney. Haematoxylin and eosin, x 250
Discussion
Von Hippel [1] presented a series of cases of retinal an- giomatosis and published a pathological study in 1911 [2]. He is credited with establishing as a clinical entity the disease that now bears his name. Subsequently, Lin- dau [4, 5] established the association of angiomatosis retinae with widespread lesions of the central nervous system and viscera. These lesions include haemangio- blastoma of the central nervous system, renal carcinoma, phaeochromocytoma, and angioma, adenoma or cysts of the liver, kidney, epididymis, mesosalpinx or pancreas [61.
The ocular lesions include capillary haemangiomata of the retina or optic disc, which are often multiple and

334
bilateral. These lesions occur in 50%-60% of patients with Von Hippel-Lindau disease, and they are generally the earliest manifestation of this condition [3, 6]. They are located in the capillary bed, between an arteriole and a venule that become grossly dilated. The haeman- giomata may occur de novo in retina previously ob- served to be normal by ophthalmoscopy and angiogra- phy. Visual loss may occur f rom exudation, retinal de- tachment or haemorrhage. Cerebellar haemangioblasto- ma is the most common cause of initial symptoms in this disease. It occurs in 36%-60% of patients, with a mean age at diagnosis of 31 years, and it causes the greatest morbidi ty and mortali ty [3, 6].
Renal carcinoma occurs in 28% of patients, with a mean age at diagnosis of 41 years [3, 6], and is the last of the major manifestations to appear. It differs f rom sporadic renal carcinoma in that the mean age at diagnosis is lower and it has only a slight male pre- dominance (sporadic renal carcinoma is 3 times more common in males, and the mean age at diagnosis lies around 50-60 years). It is of interest that the gene for von Hippel-Lindau disease, which is an autosomal domi- nant condition with incomplete penetrance, maps to chromosome 3p, which is the region associated with spo- radic renal carcinoma [8].
Isolated retinal capillary haemangiomata at the optic disc are uncommon [7], but they may be associated with the von Hippel-Lindau syndrome. Whereas intracranial
haemangioblas toma is likely to manifest itself, renal car- cinoma, which is common in this syndrome, may go unnoticed until metastases occur [3]. Early nephrectomy offers a cure. This case emphasizes the importance of routine fundal examination as well as referral of patients with isolated capillary haemangiomata of the optic disc for screening.
References
1. Hippel E von (1904) Uber eine sehr seltene Erkrankung der Netzhaut: klinische Beobachtungen. Arch Ophthalmol 59:83- 106
2. Hippel E von (1911) Die anatomische Grundlage der von mir beschriebenen sehr seltenen Erkrankung der Netzhaut. Arch Ophthalmol 79:350-377
3. Horton WA, Wong V, Eldridge R (1976) Von Hippel-Lindau disease. Arch Intern Med 136:769-777
4. Lindau A (1926) Studien fiber Kleinhirncysten. Bau, Pathoge- nese und Beziehungen zur Angiomatosis retinae. Acta Pathol Microbiol Scand [Suppl] 1 : 1-128
5. Lindau A (1927) Zur Frage der Angiomatosis retinae und ihrer Hirnkomplikationen. Acta Ophthalmol 4:193-226
6. Melmon KL, Rosen SW (1964) Lindau's disease: review of the literature and study of a large kindred. Am J Med 36:595-617
7. Schindler RF, Sarin LK, MacDonald PR (1975) Hemangiomas of the optic disc. Can J Ophthalmol 10:305-318
8. Seizinger BR, Rouleau GA, Ozelius LJ et al. (1988) Von Hippel- Lindau disease maps to the region of chromosome 3 associated with renal cell carcinoma. Nature 332:268-269


















