Understanding Gynecology in TCM Zhangqinhua Gynecology of Shuguang hospital.
Upload
college-of-medicine-sulaymaniyahCategory
view
825download
0description

Dr. Maryam Bakir

Defined as clinical or biochemical evidence of androgen excess, hirsutism which is the most frequent manifestation of androgen excess in woman is defined as excessive growth of terminal hair in male like pattern i.e. (midline hair, mustache, beard, intermammary and inner thigh).
Two condition should be differentiated from hirsutism :
- Hypertrichosis is the term reserved for androgen-independent growth of hair that is in non-sexual area such as trunk and extremities. This condition may be due to genetic factor, anorexia nervosa, thyroid dysfunction or drugs like phenytoin or minoxidil.
- virilization characterize by coarsening of voice ,decrease breast size, loss of female contour, increased muscle mass, and enlargement of clitoris.

INCIDENCE: 2-10%
Pathophysiology: either due to excessive androgen production or increased end organ sensitivity.

1.PCOS most common.2.Idiopathic 2nd most common in which there is
normal androgen level and regular ovulation by unknown mechanism although it may be due to increased 5-alfa reductase activity in skin.
3.Adrenal tumor like adenoma or androgen secreting Leydig-Sertoli cell tumor these characterized by rapid progressive course. Treatment is by removal of tumor.
4.Other causes like late-onset 21-Hydroxylase deficiency, Cushing syndrome and Acromegaly.

Is the most common cause of hyperandrogenaemia.
PCOS is a heterogeneous collection of signs and symptoms that gathered together form a spectrum of a disorder, sometime mild and sometime severe.
Incidence: is about 5-10% of reproductive age group. Historically is first described at 1921 by Achard
and Thies and it has been called (Diabetes of bearded women), then subsequently described by Stien and Leventhal in 1935.

There is a considerable heterogeneity and complexity in pathogenesis of PCOS, but the two main contributory factors are
Genetic which is mostly polygenic because no single gene mutation has been found and this suggested by familial clustering of disease and that about half of 1st degree relative of PCOS have hyperandrogenaemia with or without anovulation which might suggest autosomal dominant mode.
Environmental like obesity or nutritional factors.

• Increase ovarian stromal theca cell lead to increase androgen production.• Increased LH secretion due to disordered -ve feedback mechanism.• Hyperinsulinaemia due to insulin resistance which potentiates the action of LH and increase androgen.

Criteria (important) ESHRE/ASRM 2004 consensus meeting was
agreed that presence of 2 out of three of the following criteria is required:
Oligo-and/or anovulation. Hyperandrogenism (clinical and/or
biochemical). Polycystic appearance of ovary this is defined
as an ovary with 12 or more follicles measuring 2-9 mm in diameter and increased ovarian volume more than 10 cm3 on TVU (normal range is up to 8cm3).
20-30% of women have polycystic appearance without clinical features

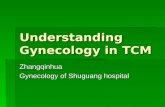
Polycystic Ovaries
Cystic Follicles
Uterus
Tube
Anatomic Features of the Polycystic
Ovary

Menstrual disturbance (50% oligo., 20% amenorrhea, 30% normal).
Obesity (BMI is measured by weight in kg/height in m2).

Hirsutism, acne, alopecia not virilization.


Other skin changes like acanthisis negricans.

Laboratory finding: High LH and normal or low FSH resulting in
raised LH/FSH ratio. High androgens and low sex hormone
binding globulin (SHBG). Increased estrogens. Increased prolactin.
Health consequence of PCOS: Diabetes mellitus. Endometrial carcinoma. Breast cancer. Dyslipidaemia. Hypertension and cardiovascular.

More or less depend on complain of patient and is not required in all.
Reduction of weight might correct majority of derangement.
1. Menstrual irregularity because they are hyper estrogenic they have no risk of osteoporosis but they have risk of endometrial hyperplasia so with drawal bleeding is important. Regulation best achieved by either low dose COCP or progesterone like medroxyprogesteron acetate(provera) or dydrogesteron (duphaston). If there is prolonged amenorrhea endometrial biopsyis indicated. Insulin-sensitizer might reduce risk of endometrial cancer by enhancing ovulation.

2. Obesity: to keep carbohydrate content down and to avoid fatty food. Anti obesity drugs may be helpful. Metformin does not reduce weight.
3. Anovulation: which is a primary cause of infertility is best treated by - Clomiphine citrate: this is first line therapy given in dose of 50 mg/day starting from 3rd day of cycle for 5 days following spontaneous or artificial cycle. If no response it increased by 50 mg in subsequent cycle.
- Metformin: up to 1500mg/day might lead to spontaneous ovulation.
- Gonadotrophins: for resistance cases other alternative are surgical treatment.

4. Hirsutism: the most challengeable, medical treatment should stop further of hirsuitism and decrease rate of hair growth
- COPC is commonly used mechanism of action is due to suppression of LH secretion (effect of progesterone), increasing hepatic SHBG, and decreasing circulating androgens (effect of estrogen).
- Dianette used as first line treatment which contains ethinylestradiol 30 microgram and cyproterone acetate 2mg. liver function may be affected and there is risk of thromboembolism so moniter LFT.

- Spironolacton is a weak potassium sparing diuretic is given in daily doses of 25-100 mg. side effects are irregular vaginal bleeding, fatigue, and polyuria. Diane and spironolacton require COCP cover.
- Flutamide is originally used for ca prostate, significant reduction is observed over 8 month in doses of up to 250 mg. the main adverse effect are sever hepatitis so not used widely.
- Ketoconazole and finastride are not used widely.
- Metformin, troglitazon might reduce hair gtowth.
SURGICAL TREATMENT of PCOS: - wedge resection of ovary, no longer used. - laproscopic ovarian drilling LOD.

THANKS