![01:202:497:81 Understanding School Violencecriminaljustice.rutgers.edu/images/syllabi/17_Fall/FALL... · 2017-05-09 · 1 01:202:497:81 Understanding School Violence [Fall 2017] Monday](https://static.fdocuments.net/doc/165x107/5f2edc6a56d81b7f180171d4/0120249781-understanding-school-vio-2017-05-09-1-0120249781-understanding.jpg)
Guidelines for Therapeutic Drug Monitoring of ... · Circuaio Joura Vol.81, April 2017 Circ J 2017;...
32
Circulation Journal Vol.81, April 2017 Circ J 2017; 81: 581 – 612 doi: 10.1253/circj.CJ-66-0138 Released online March 9, 2017 Mailing address: Scientific Committee of the Japanese Circulation Society, 18F Imperial Hotel Tower, 1-1-1 Uchisaiwai-cho, Chiyoda-ku, Tokyo 100-0011, Japan. E-mail: [email protected] This English language document is a revised digest version of Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs Clinical Use of Blood Drug Concentration Monitoring reported at the Japanese Circulation Society Joint Working Groups performed in 2015 (Website: http://www.j-circ.or.jp/guideline/pdf/JCS2015_aonuma_d.pdf). Refer to Appendix 1 for the details of members. The Japanese Circulation Society/the Japanese Society of Therapeutic Drug Monitoring Joint Guidelines (2013–2014 Joint Working Groups Report) JCS Joint Working Group: The Japanese Circulation Society (JCS), The Japanese Society of Therapeutic Drug Monitoring (JSTDM) ISSN-1346-9843 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected] Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs Clinical Use of Blood Drug Concentration Monitoring (JCS 2015) ― Digest Version ― Kazutaka Aonuma (JCS); Tsuyoshi Shiga (JSTDM); Hirotsugu Atarashi; Kosuke Doki; Hirotoshi Echizen; Nobuhisa Hagiwara; Junichi Hasegawa; Hideharu Hayashi; Kenzo Hirao; Fukiko Ichida; Takanori Ikeda; Yorinobu Maeda; Naoki Matsumoto; Toshiyuki Sakaeda; Wataru Shimizu; Mitsuru Sugawara; Kyoichi Totsuka; Yoshimasa Tsuchishita; Kazuyuki Ueno; Eiichi Watanabe; Masayuki Hashiguchi; Sumio Hirata; Hidefumi Kasai; Yoshiaki Matsumoto; Akihiko Nogami; Yukio Sekiguchi; Tokuko Shinohara; Atsushi Sugiyama; Naokata Sumitomo; Atsushi Suzuki; Naohiko Takahashi; Eiji Yukawa; Masato Homma; Minoru Horie; Hiroshi Inoue; Hiroshi Ito; Takanori Miura; Tohru Ohe; Kimikazu Shinozaki; Kazuhiko Tanaka on behalf of the Japanese Circulation Society and the Japanese Society of Therapeutic Drug Monitoring Joint Working Group Table of Contents List of CQs and HTUs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 582 I. Outline of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 1. Scope of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 2. Remarks for the Use of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 3. Selection of Clinical Questions and Grades of Recommendations∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 4. External Review∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 5. Future Plans ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 6. Conflict of Interest∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 7. Digest Version ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 II. Therapeutic Drug Monitoring (TDM) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 1. History of TDM∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 2. Pharmacokinetics Knowledge Essential to TDM∙∙∙∙∙∙∙∙∙∙∙ 584 3. Assays to Determine Drug Concentrations in Blood ∙∙∙∙∙ 586 4. Methods of Pharmacokinetic Analysis∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 586 5. Coverage With the National Health Insurance in Japan ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 586 III. Descriptions ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 587 1. Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 587 1.1 Class I Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 589 1.2 Class II Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 590 1.3 Class III Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 590 1.4 Class IV Antiarrhythmic Drugs (Bepridil) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 592 1.5 Inotropic Drugs (Digoxin) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 592 2. Antimicrobial Drugs for the Treatment of Infective Endocarditis ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 595 3. Considerations for Special Patient Populations ∙∙∙∙∙∙∙∙∙∙∙∙ 597 3.1 Patients With Renal Dysfunction or on Hemodialysis ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 597 3.2 Cirrhosis∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 598 3.3 Thyroid Dysfunction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 598 3.4 Elderly Patients ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 599 3.5 Children ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 600 3.6 Women During Pregnancy and Breastfeeding ∙∙∙∙∙∙∙ 603 4. Pharmacokinetic Profiles of Cardiovascular Drugs ∙∙∙∙∙∙∙ 604 5. Drug Interactions of Cardiovascular Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 604 References∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 606 Appendix ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 609 JCS GUIDELINES
Transcript of Guidelines for Therapeutic Drug Monitoring of ... · Circuaio Joura Vol.81, April 2017 Circ J 2017;...

Circulation Journal Vol.81, April 2017
Circ J 2017; 81: 581 – 612doi: 10.1253/circj.CJ-66-0138
Released online March 9, 2017Mailing address: Scientific Committee of the Japanese Circulation Society, 18F Imperial Hotel Tower, 1-1-1 Uchisaiwai-cho,
Chiyoda-ku, Tokyo 100-0011, Japan. E-mail: [email protected] English language document is a revised digest version of Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs
Clinical Use of Blood Drug Concentration Monitoring reported at the Japanese Circulation Society Joint Working Groups performed in 2015 (Website: http://www.j-circ.or.jp/guideline/pdf/JCS2015_aonuma_d.pdf).
Refer to Appendix 1 for the details of members.The Japanese Circulation Society/the Japanese Society of Therapeutic Drug Monitoring Joint Guidelines (2013–2014 Joint Working
Groups Report)JCS Joint Working Group: The Japanese Circulation Society (JCS), The Japanese Society of Therapeutic Drug Monitoring
(JSTDM)ISSN-1346-9843 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs Clinical Use of Blood Drug
Concentration Monitoring (JCS 2015)― Digest Version ―
Kazutaka Aonuma (JCS); Tsuyoshi Shiga (JSTDM); Hirotsugu Atarashi; Kosuke Doki; Hirotoshi Echizen; Nobuhisa Hagiwara; Junichi Hasegawa; Hideharu Hayashi;
Kenzo Hirao; Fukiko Ichida; Takanori Ikeda; Yorinobu Maeda; Naoki Matsumoto; Toshiyuki Sakaeda; Wataru Shimizu; Mitsuru Sugawara; Kyoichi Totsuka;
Yoshimasa Tsuchishita; Kazuyuki Ueno; Eiichi Watanabe; Masayuki Hashiguchi; Sumio Hirata; Hidefumi Kasai; Yoshiaki Matsumoto; Akihiko Nogami;
Yukio Sekiguchi; Tokuko Shinohara; Atsushi Sugiyama; Naokata Sumitomo; Atsushi Suzuki; Naohiko Takahashi; Eiji Yukawa; Masato Homma; Minoru Horie;
Hiroshi Inoue; Hiroshi Ito; Takanori Miura; Tohru Ohe; Kimikazu Shinozaki; Kazuhiko Tanaka on behalf of the Japanese Circulation Society and
the Japanese Society of Therapeutic Drug Monitoring Joint Working Group
Table of ContentsList of CQs and HTUs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 582I. Outline of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 1. Scope of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 2. Remarks for the Use of the Guidelines ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 3. Selection of Clinical Questions and Grades of
Recommendations∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 4. External Review ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 583 5. Future Plans ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 6. Conflict of Interest ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 7. Digest Version ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584II. Therapeutic Drug Monitoring (TDM) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 1. History of TDM ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 584 2. Pharmacokinetics Knowledge Essential to TDM ∙∙∙∙∙∙∙∙∙∙∙ 584 3. Assays to Determine Drug Concentrations in Blood ∙∙∙∙∙ 586 4. Methods of Pharmacokinetic Analysis∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 586 5. Coverage With the National Health Insurance in
Japan ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 586III. Descriptions ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 587 1. Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 587 1.1 Class I Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 589
1.2 Class II Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 590 1.3 Class III Antiarrhythmic Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 590 1.4 Class IV Antiarrhythmic Drugs (Bepridil) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 592 1.5 Inotropic Drugs (Digoxin) ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 592 2. Antimicrobial Drugs for the Treatment of Infective
Endocarditis ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 595 3. Considerations for Special Patient Populations ∙∙∙∙∙∙∙∙∙∙∙∙ 597 3.1 Patients With Renal Dysfunction or on
Hemodialysis ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 597 3.2 Cirrhosis ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 598 3.3 Thyroid Dysfunction ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 598 3.4 Elderly Patients ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 599 3.5 Children ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 600 3.6 Women During Pregnancy and Breastfeeding ∙∙∙∙∙∙∙ 603 4. Pharmacokinetic Profiles of Cardiovascular Drugs ∙∙∙∙∙∙∙ 604 5. Drug Interactions of Cardiovascular Drugs ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 604References ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 606Appendix ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ 609
JCS GUIDELINES

Circulation Journal Vol.81, April 2017
582 AONUMA K et al.
List of CQs and HTUs
1. Antiarrhythmic DrugsCQ1 Is blood drug concentration monitoring effective for patients with arrhythmia receiving antiarrhythmic drugs? ..........................................................................587CQ2 Does blood drug concentration monitoring of anti-arrhythmic drugs help reduce ADRs in patients with arrhyth-mia who are receiving antiarrhythmic drugs? ..............588CQ3 Can we shorten the time to achieve an optimal dos-age regimen by blood drug concentration monitoring of antiarrhythmic drugs in patients with arrhythmia?......588HTU1 When should blood samples be taken to monitor blood concentrations of antiarrhythmic drugs? ...........588HTU2 Is it possible to predict the peak and trough con-centrations of a drug on the basis of the timing of blood sampling and the blood drug concentration? ...............588HTU3 When should drug concentrations be moni-tored? ..................................................................... 588
1.1 Class I Antiarrhythmic DrugsHTU4 Please summarize the toxic (ADRs) concentration range of each class I antiarrhythmic drug. .................589HTU5 What are typical drug concentration-dependent ADRs to antiarrhythmic drugs? ..................................589HTU6 What are the clinical implications of the active metabolites of drugs subject to TDM? .........................589
1.2 Class II Antiarrhythmic DrugsCQ4 Is blood drug concentration monitoring beneficial for patients receiving beta-blockers for the treatment of arrhythmia? .................................................................590
1.3 Class III Antiarrhythmic DrugsCQ5 Is blood drug concentration monitoring beneficial for patients receiving amiodarone for the treatment of arrhythmia? .................................................................590CQ6 Does blood drug concentration monitoring help decrease the incidence of extracardiac ADRs in patients receiving amiodarone for the treatment of arrhyth-mia? .............................................................................590HTU7 When should blood samples for blood drug con-centration monitoring of amiodarone be obtained?.....590HTU8 Is blood drug concentration monitoring necessary for patients who receive amiodarone by continuous intravenous infusion? ..................................................591HTU9 Is the measurement of blood desethylamiodarone concentration useful as an index of efficacy and safety of amiodarone? ................................................................591CQ7 Is TDM effective in ensuring optimal antiarrhythmic treatment with sotalol? ................................................591HTU10 When should blood samples be taken to perform blood drug concentration monitoring of sotalol? ........591
1.4 Class IV Antiarrhythmic Drugs (Bepridil)CQ8 Is blood drug concentration monitoring effective for patients with arrhythmia receiving bepridil? ..........592HTU11 When should blood samples be taken to perform blood drug concentration monitoring of bepridil? .......592
1.5 Inotropic Drugs (Digoxin)CQ9 Is blood drug concentration monitoring effective for patients with arrhythmia receiving digoxin? ..........592CQ10 Is blood drug concentration monitoring effective
for patients with heart failure receiving digoxin? .........592HTU12 When should blood samples be taken to monitor blood concentrations of digoxin? .................................593HTU13 How frequently should blood samples be taken when blood drug concentration monitoring is conducted during long-term digoxin therapy? ..............................593HTU14 What is the target blood concentration of digoxin? .......................................................................594HTU15 Can we use digoxin concentrations during blood drug concentration monitoring of methyldigoxin? ......594HTU16 Should physicians consider the possible effects of endogenous digoxin-like immunoreactive substances or drugs that have a chemical structure similar to digoxin on blood digoxin concentration monitoring? ...................595HTU17 Does digitalis intoxication occur in relation to blood digoxin concentration? ......................................595
2. Antimicrobial Drugs for the Treatment of Infective Endocarditis
CQ11 Does TDM of vancomycin help ensure effective treatment of infective endocarditis? .............................595CQ12 Does TDM of aminoglycosides help ensure effec-tive treatment of infective endocarditis? ......................596HTU18 When should blood samples be taken to monitor blood concentrations of vancomycin? .........................596HTU19 When should blood samples for TDM of amino-glycosides be obtained? ................................................596HTU20 When should blood samples be taken to monitor blood concentrations of teicoplanin? ...........................596
3. Considerations for Special Patient Populations3.1 Patients With Renal Dysfunction or on HemodialysisHTU21 How should blood drug concentration monitoring of antiarrhythmic drugs be conducted for patients with renal dysfunction or those on hemodialysis? ...............597HTU22 How should blood drug concentration monitoring of digoxin be conducted for patients with renal dysfunction or those on hemodialysis? ............................................597HTU23 How should TDM of vancomycin be conducted for patients with renal dysfunction or those on hemodialysis who are complicated with infective endocarditis? ........598
3.2 CirrhosisHTU24 How should blood drug concentration monitoring of antiarrhythmic drugs be conducted for patients with cirrhosis? ......................................................................598
3.3 Thyroid DysfunctionHTU25 How should blood concentration monitoring of digoxin be conducted for patients with thyroid dysfunc-tion? .............................................................................598
3.4 Elderly PatientsHTU26 How should blood drug concentration monitor-ing of antiarrhythmic drugs be conducted for elderly patients? .......................................................................599HTU27 How should blood drug concentration monitoring of pilsicainide be conducted for elderly patients? .........599HTU28 How should blood drug concentration monitoring of digoxin be conducted for elderly patients?...............600

Circulation Journal Vol.81, April 2017
583JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
3.5 ChildrenHTU29 When antiarrhythmic drugs are administered to children, can physicians target blood drug concentrations similar to those for adults? ...........................................600HTU30 When digoxin is administered to children, can physicians target blood drug concentrations similar to those for adults?...........................................................601HTU31 When glycopeptides or aminoglycosides are
administered to children with infective endocarditis, can physicians target blood drug concentrations similar to those for adults? ....................................................................601
3.6 Women During Pregnancy and BreastfeedingCQ13 What are indications and precautions for the use of antiarrhythmic drugs in women during pregnancy and breastfeeding? ..............................................................603
I. Outline of the Guidelines
1. Scope of the Guidelines
The principle of pharmacotherapy is maximizing the therapeutic effect while minimizing adverse reactions. Therapeutic drug monitoring (TDM) is a strategy to individualize drug treatment through monitoring various factors that affect the efficacy and adverse effects of drugs. Antiarrhythmic drugs have long been investigated for their pharmacokinetic behaviors in the body and efficacy, and are used in the clinical setting on the basis of TDM findings. However, blood concentrations of antiarrhythmic drugs should be interpreted according to not only expertise in pharmacokinetics, pharmacodynamics, and drug interac-tions, but also patient adherence to medication. The National Health Insurance in Japan covers the clinical use of blood drug concentration monitoring for many antiar-rhythmic drugs and digoxin, but many practitioners do not use it well because the role and definition of TDM have not been established fully. Accordingly, the Japanese Circulation Society (JCS) and the Japanese Society of Therapeutic Drug Monitoring (JSTDM) decided to jointly create the Guidelines for Therapeutic Drug Monitoring of Cardio-vascular Drugs in order to ensure safe and effective phar-macotherapy for the treatment of cardiovascular diseases using appropriate TDM of blood drug concentrations.
Recently, TDM is increasingly being expected to play a role as a safety index especially in the pharmacotherapy of cardiovascular diseases. The present guidelines are prepared for physicians who prescribe drugs for the treatment of cardiovascular diseases, and pharmacists, nurses, and clinical laboratory technologists who work with them.
The present guidelines describe how to conduct TDM appropriately (e.g., appropriate timing of blood sampling as the elapsed time from the last dose and that from the initiation of treatment) in the clinical setting and interpret blood drug concentrations, as well as limitations of TDM. Cardiovascular drugs described in the present guidelines are those of which TDM is commercially available and covered by the National Health Insurance in Japan.
2. Remarks for the Use of the Guidelines
The present guidelines reflect the National Health Insurance in Japan at the time of writing. Reactions to a drug are not defined only by pharmacokinetics of the drug. Pharmaco-therapy should be assessed comprehensively based on the patient’s clinical characteristics, pathological conditions, and underlying diseases, among other factors. If a physician uses TDM or interprets its findings in a way inconsistent with the present guidelines considering the circumstances unique to the patient, the physician’s discretion should be
prioritized over the guidelines. The present guidelines do not provide any basis for any legal action.
3. Selection of Clinical Questions and Grades of Recommendations
The practice guidelines were prepared according to the procedures proposed by the Medical Information Network Distribution Service (MINDS). Guideline Writing Groups of the JCS and the JSTDM specified Clinical Questions (CQs) on cardiovascular drugs. For each CQ, relevant literature published from 1960 to 2013 were searched and identified via queries of the MEDLINE, EMBASE, and JAMAS, and were used as evidence. The JCS Guideline Writing Group specified questions on the use of TDM where evidence is limited to list them as How To Use (HTU) questions, and the JSTDM Guideline Writing Group prepared answers to HTU questions with a certain level of consensus.
Answers to CQs are indicated with their respective levels of evidence and grades of recommendations.
- Levels of EvidenceLevel I: Systematic review or meta-analysis of random-
ized controlled trialsLevel II: One or more randomized controlled trialsLevel III: Non-randomized controlled trialsLevel IVa: Cohort studyLevel IVb: Case-control study or cross-sectional studyLevel V: Case reports or case seriesLevel VI: Expert committee’s or expert’s opinions not
based on patient data
- Grades of RecommendationsGrade A: Strongly recommended and supported by
strong evidenceGrade B: Recommended with moderately strong support-
ing evidenceGrade C1: Recommended despite no strong supporting
evidenceGrade C2: Not recommended because of the absence of
strong supporting evidence.Grade D: Not recommended as evidence indicates that
the treatment is ineffective or even harmful.
4. External Review
Four members each of the JCS and the JSTDM joined as external reviewers to review draft guidelines.

Circulation Journal Vol.81, April 2017
584 AONUMA K et al.
5. Future Plans
The Japanese version of the present guidelines will be published by the JCS as a printed material, and will also become available on the websites of the JCS and the JSTDM. A digest of the guidelines will be prepared in Japanese and in English, and the English version will be published in an English journal of the JCS. The guidelines will also become available on the MINDS website.
6. Conflict of Interest
During the preparation of the present guidelines, guideline
writing group meetings were held. All expenses for the meetings, including transportation costs, were covered by the JCS and the JSTDM. Members of the writing groups provided conflict of interest statements, which were maintained by the relevant society.
7. Digest Version
The present digest version was prepared for use in the clinical setting. In order to simplify the contents, some information in the unabridged version was excluded or modified. The reader is encouraged to refer to the unabridged version to understand the guidelines fully.
II. Therapeutic Drug Monitoring (TDM)
1. History of TDM
Drugs that show substantial inter-individual variability in response, and those with a narrow therapeutic range, i.e., a small difference between toxic and therapeutic doses, cannot be used at a fixed dose. In order to ensure safer and more effective treatment with these drugs, healthcare professionals needed quantitative methods to quantita-tively assess the pharmacokinetics of such drugs and predict drug response in individual patients. As this approach was expected to help physicians create optimal drug treatment strategies for individual patients, researchers tried to develop new approaches to maintain blood drug concentrations in a therapeutic range.
In the 1960 s, microassay methods to measure small amounts of drugs in blood were developed, and the results of studies on the relationship between blood concentrations of antiepileptic drugs such as phenytoin and lithium carbonate and pharmacological effects were reported, which led to the development of clinical pharmacology as a new academic field. In the 1960 s and early 1970 s, researchers started to promote a concept of clinical pharmacokinetics, and practitioners began to design drug treatment strategies using blood drug concentrations in the clinical setting in the 1970s. The original meaning of thera-peutic drug monitoring (TDM) is to administer drugs in an optimal way for each patient through monitoring various factors that affect drug efficacy and adverse drug reactions (ADRs). As physicians have used blood drug concentra-tions to ensure optimal drug therapy, TDM is often con-sidered an approach to optimize pharmacotherapy by monitoring drug concentrations in blood.
In Japan, TDM based on drug concentrations in blood was introduced in the early 1970 s, and TDM has been widely used in the clinical setting since the 1970 s and 1980 s. As the importance of TDM in medical treatment is fully accepted, TDM for various types of drugs is now covered by the National Health Insurance under a category of “specific therapeutic drug monitoring fees.” With the advancement in molecular biology, the roles of various proteins and genes have been clarified, which has enabled detailed analysis of the pharamcokineticsof drugs. Nowadays physicians are able to design an optimal treatment strategy for each patient with TDM considering detailed information of these proteins and genes. The era of tailor-made drug
therapies has come.
2. Pharmacokinetics Knowledge Essential to TDM
TDM and basic principles of pharmacokinetics (PK) can be used to evaluate or predict the effect of a drug in reference to concentration (C) of the drug in the vicinity of target molecules located in the target organ or tissues. This method is particularly useful for patients whose patho-logical condition affects PK of a drug of interest.
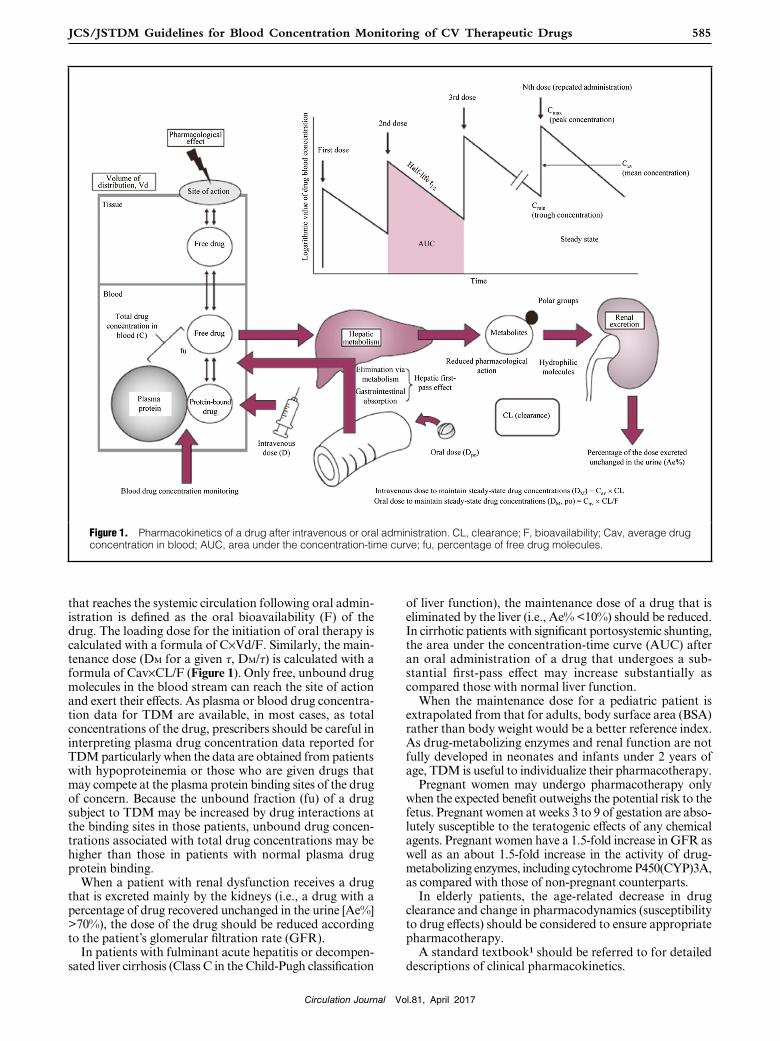
When a drug is given, the drug concentration (C) in the blood reaches its peak level, and then decreases as a function of time and systemic clearance (CL; expressed with a unit of L/hr or other units) of the drug. When the drug is given as a single intravenous injection, it reaches its peak concen-tration in the blood (Cmax) almost immediately. When the drug is given as a single intravenous dose to achieve the target drug concentration as the Cmax, the required dose may be calculated as the product of the volume of distribu-tion (Vd) of the drug and the target concentration (C) (i.e., DL=C×Vd). This dose may be used as the first dose (i.e., loading dose, DL) for continuous infusion or repeated intravenous injections. When the drug is infused continu-ously to maintain a stable therapeutic plasma drug concen-tration, the required dose, i.e., the maintenance dose (DM), is calculated as the product of the C and CL (DM=C×CL). When the drug is administered with repeated intravenous injections at DM with an interval τ (tau), DM is calculated as the product of average plasma drug concentration dur-ing the dosing interval (Cav) and CL (DM/τ=Cav×CL) (Figure 1).
The time required for a drug to reach drug concentration that is half of any original concentrations is defined as half-life (t1/2). A drug having a short t1/2 needs to be administered with a shorter dosing interval than that having a longer t1/2 in order to maintain therapeutic drug concentrations throughout the dosing interval, because plasma drug concentrations decline rapidly and reach those that no longer elicit clinically appreciable drug effects.
When a drug is administered orally, the fraction of the dose absorbed from the gastrointestinal tract and the first-pass metabolism in the liver (i.e., first-pass effect) should be considered. The proportion of the administered dose
Circulation Journal Vol.81, April 2017
585JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
that reaches the systemic circulation following oral admin-istration is defined as the oral bioavailability (F) of the drug. The loading dose for the initiation of oral therapy is calculated with a formula of C×Vd/F. Similarly, the main-tenance dose (DM for a given τ, DM/τ) is calculated with a formula of Cav×CL/F (Figure 1). Only free, unbound drug molecules in the blood stream can reach the site of action and exert their effects. As plasma or blood drug concentra-tion data for TDM are available, in most cases, as total concentrations of the drug, prescribers should be careful in interpreting plasma drug concentration data reported for TDM particularly when the data are obtained from patients with hypoproteinemia or those who are given drugs that may compete at the plasma protein binding sites of the drug of concern. Because the unbound fraction (fu) of a drug subject to TDM may be increased by drug interactions at the binding sites in those patients, unbound drug concen-trations associated with total drug concentrations may be higher than those in patients with normal plasma drug protein binding.
When a patient with renal dysfunction receives a drug that is excreted mainly by the kidneys (i.e., a drug with a percentage of drug recovered unchanged in the urine [Ae%] >70%), the dose of the drug should be reduced according to the patient’s glomerular filtration rate (GFR).
In patients with fulminant acute hepatitis or decompen-sated liver cirrhosis (Class C in the Child-Pugh classification
of liver function), the maintenance dose of a drug that is eliminated by the liver (i.e., Ae% <10%) should be reduced. In cirrhotic patients with significant portosystemic shunting, the area under the concentration-time curve (AUC) after an oral administration of a drug that undergoes a sub-stantial first-pass effect may increase substantially as compared those with normal liver function.
When the maintenance dose for a pediatric patient is extrapolated from that for adults, body surface area (BSA) rather than body weight would be a better reference index. As drug-metabolizing enzymes and renal function are not fully developed in neonates and infants under 2 years of age, TDM is useful to individualize their pharmacotherapy.
Pregnant women may undergo pharmacotherapy only when the expected benefit outweighs the potential risk to the fetus. Pregnant women at weeks 3 to 9 of gestation are abso-lutely susceptible to the teratogenic effects of any chemical agents. Pregnant women have a 1.5-fold increase in GFR as well as an about 1.5-fold increase in the activity of drug-metabolizing enzymes, including cytochrome P450(CYP)3A, as compared with those of non-pregnant counterparts.
In elderly patients, the age-related decrease in drug clearance and change in pharmacodynamics (susceptibility to drug effects) should be considered to ensure appropriate pharmacotherapy.
A standard textbook1 should be referred to for detailed descriptions of clinical pharmacokinetics.
Figure 1. Pharmacokinetics of a drug after intravenous or oral administration. CL, clearance; F, bioavailability; Cav, average drug concentration in blood; AUC, area under the concentration-time curve; fu, percentage of free drug molecules.

Circulation Journal Vol.81, April 2017
586 AONUMA K et al.
3. Assays to Determine Drug Concentrations in Blood
Table 1 summarizes commonly used assays to determine drug concentrations in blood. Assays to determine drug concentrations in blood are classified largely into immuno-assays, separation analyses, and other methods. Immuno-assays use antibodies to detect the presence of the target molecule. Immunoassays are widely used as simple and rapid analytical methods, and many immunoassay kits are commercially available. Recently, general-purpose auto-mated clinical analyzers are often used to determine drug concentrations in blood. Blood concentrations of cardio-vascular drugs are typically determined with enzyme multiplied immunoassay techniques (EMIT) and affinity column mediated immunoassays (ACMIA). However, physicians should be aware that substances in the body, metabolites of the target drug, and other drugs used concomitantly with the target drug may affect the results of these assays or interact with detection antibodies. As assays for antiarrhythmic drugs are often commercially unavailable even for drugs of which TDM is covered by the NHI, separation analyses should be used for these drugs. High performance liquid chromatography (HPLC), a separation analysis, is highly specific and is used to deter-mine blood concentrations of many drugs, but it needs complex procedures including pretreatment. Liquid chro-matography-mass analysis (LC/MS/MS) is a technique combining HPLC and mass spectrometry (MS) to ensure a high degree of analytical accuracy. Many commercial laboratories use HPLC and LC/MS/MS.
4. Methods of Pharmacokinetic Analysis
In order to simulate changes over time in blood concentra-tions of a drug in a patient, pharmacokinetic parameters, such as the clearance, volume of distribution, and absorp-
tion rate constant of the drug, of the patient are required. It should be known that pharmacokinetic parameters described in package inserts for ethical drugs and published literature are average values obtained from study subjects. For example, clearance differs substantially by age, body size, or renal/hepatic function, which leads to individual differences in drug concentrations in blood (Figure 2). Accordingly, in order to predict drug concentrations in blood in a patient, pharmacokinetic parameters of the patient have to be calculated. When the results of a popu-lation pharmacokinetics (PPK) analysis are available for the target drug, pharmacokinetic parameters for the patient may be calculated using PPK parameters and the blood concentration of the drug in the patient at one or more time points. Pharmacokinetic parameters in the patient may be calculated using the Bayes analysis, and may be used to simulate the pharmacokinetics of the drug in the patient.
However, the Bayes analysis cannot always calculate the patient’s individual pharmacokinetic parameters accurately. The accuracy in estimating the patient’s pharmacokinetic parameters depends on when blood samples are obtained. A blood sample obtained at the time of the trough concen-tration of the drug can accurately estimate the clearance value in the patient.
However, a blood sample obtained when the drug concentration is reaching its peak may not lead to accurate estimation of the clearance because the drug concentration at such time point is influenced by the volume of dis-tribution. The Bayes analysis can be used to estimate pharmacokinetic parameters that can explain the drug concentrations in the patient, but the estimated parameters should be used only to predict drug concentrations in the patient and design the patient’s dosage regimen.
5. Coverage With the National Health Insurance in Japan
For almost all drugs described in the present guidelines, analysis of blood concentrations is covered by the National Health Insurance (NHI) in Japan under a category of “specific therapeutic drug monitoring fees”. The criteria
Table 1. How to Determine Drug Concentrations in Blood
1. Immunoassays
1) Radioimmunoassays (RIAs)
2) Non-radioactive immunoassays
Enzyme-linked immunosorbent assay (EIA)
Fluorescence polarization immunoassay (FPIA)
Homogeneous enzyme immunoassay (EMIT)
Competitive fluorescent microsphere immunoassay (CFIA)
Chemiluminescence immunoassay (CLIA)
Heterogeneous enzyme-linked immunosorbent assay (ELISA)
Immunochromatography
Latex immunoagglutination inhibition method (PENTINIA)
2. Separation analyses
1) Gas chromatography (GC)
2) High-performance liquid chromatography (HPLC)
3. Other methods
1) Atomic absorption spectrometry
2) Flame photometry
3) Electrode technique
4) Chromogenic technique
Figure 2. Individual differences in drug concentrations in blood. Patients with lower clearance have slower elimination rates, and those with higher clearance have faster elimination rates. Patients with smaller volumes of distribution have higher peak drug concentrations.

Circulation Journal Vol.81, April 2017
587JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
for the coverage are as follows: (MHLW Ordinance No. 76 issued in 2012, and Notification No. 0305-1 of the Medical Economics Division, the Health Insurance Bureau, MHLW dated March 5, 2012).
- When a drug concentration measurement is conducted one or more times a month to ensure accurate manage-ment of the treatment with the drug, the physician may claim reimbursement for the fee for only one measurement per month. The NHI price for specific therapeutic drug monitoring is 470 points. (In the first month of the claim for specific therapeutic drug monitoring, an additional NHI price of 280 points will be added.)
- The specific therapeutic drug monitoring fees include fees for the determination of blood concentration of the relevant drug, those for sampling blood for the determi-nation, and management of the dosage regimen according to the analytical results.
- When determinations and scheduled treatment manage-ment that are covered under the “specific therapeutic drug monitoring fees” are conducted for a patient more than once in a month, the fees for only one session are covered by the NHI. The claim for the fee should be made when the first session is conducted.
- Drug concentrations in blood and outline of treatment
strategies should be described in the medical record.- The specific therapeutic drug monitoring fees may be
applied for patients who use antiarrhythmic drugs regu-larly, and inpatients who use aminoglycoside antibiotics for at least a few days.
- Patients with heart disease who are receiving digitalis preparations*1
- Patients with arrhythmia who are receiving antiarrhythmic drugs regularly.
- Antiarrhythmic drugs that may be claimed under a category of specific therapeutic drug monitoring fees are procainamide, N-acetylprocainamide, disopyramide, quinidine, aprindine, lidocaine, pilsicainide hydrochloride, propafenone, mexiletine, flecainide, cibenzoline succinate, pirmenol, amiodarone, sotalol hydrochloride, and bepridil hydrochloride.
- For inpatients who receive antimicrobial agents such as aminoglycosides*2 and glycopeptides for at least a few days, the fees for one session per month of determination of blood concentrations and dose adjustment based on the results are covered by the NHI.
- Glycopeptides to be covered under the specific therapeutic drug monitoring fees are vancomycin and teicoplanin.
*1Digoxin*2Amikacin, arbekacin, gentamicin, and tobramycin
III. Descriptions
1. Antiarrhythmic Drugs
CQ1 Is blood drug concentration monitoring effective for patients with arrhythmia receiving antiarrhythmic drugs?
Answer:Confirming the range of blood drug concentrations appro-priate for each patient helps physicians prescribe the drug at an optimal dose and thereby avoid adverse drug reac-tions (ADRs). Blood drug concentration monitoring is especially beneficial in confirming the patient’s adherence to medication, reconsidering the dose when the current treatment is ineffective (diagnosing undertreatment), avoiding the occurrence of drug concentration-dependent ADRs, confirming and managing pharmacokinetic drug interactions, and assessing treatment efficacy when the patient’s condition changes or when a new pharmaceutical form of a regularly used drug is used.
Level of evidence: VGrade of recommendation: C1
Commentary:Blood drug concentration monitoring of antiarrhythmic drugs is beneficial in ensuring the safety of antiarrhythmic therapy.2 However, it is unclear whether blood drug concentration monitoring of antiarrhythmic drugs may improve the clinical outcome of patients with arrhythmia.
Drug effects are affected by a variety of factors such as age, gender, genetic differences, environmental factors, meals, life styles, underlying diseases, and drug interactions (Figure 3).3 Blood concentrations of renally excreted drugs, i.e., drugs extensively excreted unchanted in the urine, are prone to be affected easily by changes in renal function. Drugs excreted by the kidneys include pilsicainide, sotalol,
digoxin, and cibenzoline. On the other hand, blood con-centrations of drugs eliminated by hepatic metabolism are affected by individual differences in the activity of drug-metabolizing enzymes. All drugs are metabolized in different ways. When different drugs are used concomitantly, a drug may reduce or enhance the activity of a particular drug-metabolizing enzyme, which are correspondingly referred to enzyme inhibition or induction, resulting in drug interactions (Table 2).
Figure 3. Individual differences in drug reactions and factors affecting them. (Adapted from Boobis AR, et al. Cardiovascular pharmacogenetics. Springer-Verlag 2003; 39 – 77,3 with mod-ifications and with permission from Springer.)

Circulation Journal Vol.81, April 2017
588 AONUMA K et al.
CQ2 Does blood drug concentration monitoring of antiar-rhythmic drugs help reduce ADRs in patients with arrhythmia who are receiving antiarrhythmic drugs?
Answer:It is unclear whether the occurrence of ADRs, including those by proarrhythmic effects of antiarrhythmic drugs, may be reduced by blood drug concentration monitoring of antiarrhythmic drugs. However, it is useful in terms of safety as ADRs occur more commonly when blood concentrations of antiarrhythmic drugs exceed their therapeutic ranges.
Level of evidence: IVbGrade of recommendation: C1
Commentary:Drug concentration-dependent ADRs may be prevented by blood drug concentration monitoring. It has been reported that the incidence of digitalis intoxication decreases by selecting the dose of digoxin based on blood digoxin concentrations.4,5 As class I antiarrhythmic drugs and amiodarone cause ADRs more commonly at higher concentrations in blood,6 monitoring drug concentrations helps prevent ADRs.
CQ3 Can we shorten the time to achieve an optimal dosage regimen by blood drug concentration monitoring of antiar-rhythmic drugs in patients with arrhythmia?
Answer:Adjusting the dose of an antiarrhythmic drug based on blood concentrations of the drug may help maintain the drug concentrations within the therapeutic range, but the effects of antiarrhythmic drugs cannot be evaluated based only on their blood concentrations. It is thus unclear whether blood drug concentration monitoring can shorten the time to achieve an optimal dosage regimen.
Level of evidence: VIGrade of recommendation: C2
Commentary:The effects of antiarrhythmic drugs cannot be predicted based only on their blood concentrations.7 The dosage regimen of antiarrhythmic drugs should be determined comprehensively according to the patient’s signs and symptoms, Electrocardiogram (ECG) findings, and results of exercise testing, among other findings indicating the
response of the drugs. The dose should not be set only to achieve the therapeutic range.
HTU1 When should blood samples be taken to monitor blood concentrations of antiarrhythmic drugs?
HTU2 Is it possible to predict the peak and trough concen-trations of a drug on the basis of the timing of blood sampling and the blood drug concentration?
Answer:In general, blood samples should be obtained after the drug concentration reached a steady state. For the purpose of confirming the efficacy and ADRs of a drug, a blood sample should be obtained at trough (just before the next administration). For drugs that cause ADRs when the drug concentration reaches a peak, a blood sample may also be obtained around the time of peak concentration.
When the population pharmacokinetic (PPK) analysis can be used to simulate the pharmacokinetic profile of a drug in a patient, the concentration-time curve in the patient may be estimated using blood concentration data at a single time point, but its accuracy is limited.
Commentary:A steady state is defined as an equilibrium between the amount of drug administered and the amount of drug eliminated per day, which results in stable drug concen-trations. The time to reach a steady state depends on the length of half-life.
As described in the section “II.4. Methods of Pharmaco-kinetic Analysis” (Page 586), the trough drug concentra-tion is prone to be affected by the clearance of the drug. As clearance is an important pharmacokinetic parameter used to determine a dosage regimen to achieve an optimal steady-state drug concentration, trough blood samples should be obtained to ensure more accurate estimation.
The section “II.4. Methods of Pharmacokinetic Analysis” also describes that the data from a trough blood sample can be used to estimate the peak drug concentration or vice versa when PPK parameters and concentration data at a single time point are available. However, it should be known that the accuracy of estimating the drug concentration at a time point different from the sampling time point (e.g., estimating peak drug concentration using data obtained from a trough sample) is not high.
HTU3 When should drug concentrations be monitored?
Table 2. Cytochrome P450 (CYP) Involving the Metabolism of Commonly-Used Antiarrhythmic Drugs: Major Substrates, Inhibitors and Inducers
Names Substrates Inhibitors Inducers
CYP1A2 Propranolol, mexiletine Mexiletine, fluvoxamine Smoking
CYP2C9 S-warfarin Amiodarone Rifampicin, phenytoin, phenobarbital, carbamazepine
CYP2D6 Aprindine, flecainide, mexiletine, lidocaine, propafenone, bepridil, propranolol, metoprolol, carvedilol
Amiodarone, quinidine, propafenone, paroxetine, cimetidine, duloxetine
CYP3A4 Dihydropyridine calcium channel blockers, amiodarone, quinidine, disopyramide, lidocaine, bepridil, diltiazem, verapamil
Amiodarone, diltiazem, erythromycin, clarithromycin, azoles antifungal drugs, cimetidine, grapefruit juice
Rifampicin, phenytoin, phenobarbital, carbamazepine
Antiarrhythmic drugs are typed in red.

Circulation Journal Vol.81, April 2017
589JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
Answer:The purpose of determining drug concentrations in blood is to determine the optimal dose, dosing interval, and method of administration to maximize the efficacy and prevent ADRs in individual patients. Determination of drug concentrations in blood is considered effective and meaningful in the following cases:
1) Situations where the selected dose should be determined as appropriate or not:
a. when treatment at an apparently adequate dose is not effective (diagnosing undertreatment)
b. when a good dose-response relationship is not seen2) Situations where poor adherence to treatment is sus-
pected3) Situations where drug poisoning and/or ADRs are
suspected a. when the cause of drug poisoning symptoms due to
overdosing must be specified in a patient receiving multiple drugs
b. when it is difficult to specify the cause of symptoms to be drug intoxication, ADRs, or disease condition
4) Situations where blood drug concentrations fluctuate substantially despite no changes in dosage regimen
a. when biological or disease-related changes in phar-macokinetics are suspected
b. when drug interactions are suspected5) When the pharmaceutical form or dosage regimen of a
drug is changed
▋1.1 Class I Antiarrhythmic DrugsHTU4 Please summarize the toxic (ADRs) concentration range of each class I antiarrhythmic drug.
Answer:As the blood concentration range that causes drug-related toxicity (ADRs) differs substantially by the type of ADR of concern, it is difficult to summarize it.
Commentary:Several clinical reports have described the blood concen-tration range at which class I antiarrhythmic drugs caused toxicity or ADRs, but the blood concentration range differs by type of toxicity signs/symptoms or ADRs. The level of evidence is not high in some of these reports. As electrolyte levels and genetic factors may affect the occurrence of abnormal ECG findings and/or proarrhythmic effects of these drugs, the blood drug concentration is not a single factor that determines the occurrence of these effects. However, the occurrence of extracardiac ADRs to antiar-rhythmic drugs are considered to be related to drug concentrations in tissues, and some studies have investigated the relationship between the occurrence of extracardiac ADRs and blood drug concentrations. For example, the incidence of hypoglycemia (fasting blood glucose level of <70 mg/mL) due to cibenzoline is low when its trough serum concentration is ≤400 ng/mL.8,9
HTU5 What are typical drug concentration-dependent ADRs to antiarrhythmic drugs?
Answer:As ADRs develop more commonly at higher blood drug concentrations, but the occurrence of abnormal ECG
findings as well as a proarrhythmic effect and negative inotropic effect of antiarrhythmic drugs cannot be predicted only with blood drug concentrations. Extracardiac ADRs are relatively related to blood drug concentrations.
Commentary:ADRs to antiarrhythmic drugs are classified roughly into cardiac effects and extracardiac effects. Cardiac ADRs include abnormal ECG findings, proarrhythmic effects, and negative inotropic effects, and are not necessarily related to drug concentrations in blood. As electrolyte levels and genetic mutations also affect the occurrence of cardiac ADRs, the risk of cardiac ADRs cannot be predicted only with blood concentrations of antiarrhythmic drugs. On the other hand, the occurrence of extracardiac ADRs is relatively more related to blood drug concentrations. Studies have investigated the relationship between the occurrence of extracardiac ADRs to antiarrhythmic drugs such as aprindine, cibenzoline, and disopyramide and blood drug concentration. For example, the incidence of central nervous ADRs to aprindine increased in relation to serum aprindine concentration: The incidence was very low at 0.75–1 μg/mL, and few ADRs developed at <0.75 μg/mL.10
HTU6 What are the clinical implications of the active metabolites of drugs subject to TDM?
Answer:Drugs mainly eliminated via metabolism may produce pharmacologically active metabolites. In these drugs, the parent drug and its active metabolites contribute to their therapeutic and adverse effects. Cautions should be exer-cised for drugs of which active metabolites are eliminated mainly via the kidneys (e.g., NAPA for procainamide), because blood concentrations of their active metabolites may be elevated to an extent that drug efficacy and ADRs are largely attributable to the active metabolite, rather than the parent drug.
Commentary:Procainamide is a classic antiarrhythmic drug. Approxi-mately 20% of procainamide administered to humans is metabolized into N-acetylprocainamide (NAPA) by N-acet-yltransferase (NAT). NAPA has antiarrhythmic effects. As NAT has genetic polymorphisms, the activity of NAT differs between individuals. As NAPA is eliminated mainly via the kidneys, NAPA concentrations may increase to a level higher than procainamide concentrations in plasma in patients with high NAT activity and renal dysfunction. Determination of NAPA concentrations in plasma would benefit patients who have ADRs despite low plasma pro-cainamide concentrations. The therapeutic range of pro-cainamide is considered 4 to 10 μg/mL, and that of NAPA, 7 to 15 μg/mL. There was an opinion that the therapeutic range should be considered to be 5 to 30 μg/mL as the sum of procainamide and NAPA concentrations.11 In addition, an active metabolite of propafenone, 5-OH-propafenone, exerts an antiarrhythmic effect that is almost identical to that of the parent drug, but its beta-blocking effect is weaker than that of propafenone. It remains unclear whether plasma 5-OH-propafenone concentrations are to be moni-tored with propafenone in the routine TDM.11a

Circulation Journal Vol.81, April 2017
590 AONUMA K et al.
▋1.2 Class II Antiarrhythmic DrugsCQ4 Is blood drug concentration monitoring beneficial for patients receiving beta-blockers for the treatment of arrhythmia?
Answer:It is difficult to predict the antiarrhythmic effect of beta-blockers based on blood drug concentrations. ECG moni-toring is useful in the evaluation of the antiarrhythmic effect of beta-blockers. There is no evidence indicating that blood drug concentration monitoring is superior to ECG monitoring.
Level of evidence: VIGrade of recommendation: C2
Commentary:Sympathetic stimulation of cardiac conduction system cells and cardiac myocytes is mediated mainly through beta-1 receptors, and appears most clearly as an increase in heart rate. In patients with sinus node dysfunction (excluding those complicated with conduction disturbance), the presence or absence of increased automaticity of the lower conduc-tion system or ordinary cardiac muscle such as increased frequency of junctional or ventricular rhythms is a useful indicator.
The antiarrhythmic effect of beta-blockers is dose-dependent. However, some patients may respond well to low doses of beta-blockers, while others may experience ADRs without any beneficial effects. There is no accumu-lated evidence to indicate the clinical benefits of blood drug monitoring as a predictor of efficacy of beta-blockers in the treatment of arrhythmia.
Drug monitoring assays are commercially available only for propranolol. Propranolol is lipid-soluble, has a high protein binding rate, and is eliminated rapidly through hepatic metabolism by CYP1A2 and CYP2D6. Its bioavail-ability is as low as about 30%.12,13 Propranolol is comprised of two enantiomers that have a complex metabolism and differ substantially in pharmacokinetic profiles.14,15 As propranolol is a non-selective beta-blocker that inhibits not only beta-1 receptors on cardiac myocytes but also beta-2 receptors on vascular and bronchial smooth muscle cells, it may cause ADRs related to peripheral vasocon-striction (e.g., blood flow disorder in patients with arterio-sclerosis obliterans) or exacerbation of bronchial asthma (e.g., bronchospasm). Bisoprolol, one of the most widely used beta 1-selective blockers, has a bioavailability of about 80%. As blood bisoprolol concentration is dose-related, it is not meaningful to determine blood bisoprolol concentra-tions as an index of efficacy.
No convincing evidence has been obtained for the significance of blood drug concentration monitoring as a measure to prevent ADRs to bisoprolol. Bradycardia may be detected by ECG or pulse monitoring, and cardiac inhibition may be detected by the appearance of symptoms of heart failure, chest X-ray, plasma brain natriuretic peptide (BNP) levels, or echocardiography. The dose of landiolol, a beta-blocker with a short half-life, may be appropriately adjusted according to clinical variables such as heart rate and blood pressure.
▋1.3 Class III Antiarrhythmic DrugsCQ5 Is blood drug concentration monitoring beneficial for patients receiving amiodarone for the treatment of arrhythmia?
Answer:Blood amiodarone concentrations is not useful in predicting its antiarrhythmic effect, but is helpful in assessing the efficacy and safety of treatment when the pharmaceutical form or dosage of a drug is changed, and adherence to medication. Within the same patient, there may be a correlation between the antiarrhythmic effect and blood concentration of amiodarone.
Level of evidence: VGrade of recommendation: C1
Commentary:There are no data indicating a correlation between the antiarrhythmic effect and blood concentration of amioda-rone. According to a report from the United States in the 1980s, amiodarone should be present at a concentration of at least 1 to 2 μg/mL in blood to exert its pharmacological action.16 However, the use of low-dose oral preparations of amiodarone has increased over time in Europe and the United States, and physicians are targeting lower concen-trations to treat patients. When new signs, symptoms, or abnormal laboratory findings develop at the occurrence or recurrence of arrhythmia, when a dosage regimen or pharmaceutical form is changed (e.g., from intravenous drug to oral drug or vice versa, or from a brand-name drug to its generic version or vice versa), or when the patient’s adherence to treatment is needed to be confirmed, data on blood drug concentrations will help design an optimal treatment plan.
CQ6 Does blood drug concentration monitoring help decrease the incidence of extracardiac ADRs in patients receiving amiodarone for the treatment of arrhythmia?
Answer:It is unclear whether blood drug concentration monitoring can help decrease the incidence of extracardiac ADRs to amiodarone. However, TDM may be useful in predicting the risk of drug concentration-dependent ADRs (those in the nervous system, gastrointestinal system, or lungs) or prevent the occurrence of them.
Level of evidence: VGrade of recommendation: C1
Commentary:It has been reported that neurological or gastrointestinal ADRs to amiodarone often develop at blood drug concen-trations of ≥2.5 to 4 μg/mL.17–19 Pulmonary toxicity of amiodarone has been suggested to be associated with long-term treatment at high doses or high blood amiodarone concentrations.16 A study in Japanese patients has reported that the risk of pulmonary toxicity is high in patients with a plasma desethylamiodarone concentration of ≥0.6 μg/mL.20
HTU7 When should blood samples for blood drug concen-tration monitoring of amiodarone be obtained?

Circulation Journal Vol.81, April 2017
591JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
Answer:In the early phase of oral amiodarone therapy, it is desirable to obtain a trough sample for blood drug concentration monitoring. However, for outpatients who receive the drug for a long period of time, blood samples may be obtained at any time points.
Commentary:In the early phase of oral amiodarone therapy, blood amiodarone concentration changes over time after admin-istration. A trough blood sample should be obtained. In patients receiving amiodarone for a long period of time, blood amiodarone concentration does not vary substantially after administration. Blood samples from such patients may be obtained at any time in relation to administration.
HTU8 Is blood drug concentration monitoring necessary for patients who receive amiodarone by continuous intravenous infusion?
Answer:Blood drug concentration monitoring is not necessarily required for patients who receive amiodarone by continuous intravenous infusion. However, when intravenous amioda-rone is replaced by oral amiodarone, blood amiodarone concentrations may be monitored for some patients.
Commentary:When a drug is administered intravenously, the drug is directly distributed into the systemic circulation, and the blood drug concentration is related to the dose adminis-tered. Immediately after the initiation of continuous intra-venous infusion, amiodarone in the circulating blood is distributed into extravascular tissues especially fat tissues. It takes about 12 hours to stabilize blood amiodarone concentrations.21 Intravenous amiodarone therapy is used in acute-phase treatment, and the dose should be adjusted according to the effects observed. When the intravenous amiodarone therapy is switched to an oral amiodarone therapy, blood amiodarone concentrations may be changed due to the decrease in bioavailability or changes in dose.21 In order maintain the antiarrhythmic effect of amiodarone, blood concentration monitoring may help adjust the oral dose to maintain the drug concentration within the thera-peutic range for the patient.
HTU9 Is the measurement of blood desethylamiodarone concentration useful as an index of efficacy and safety of amiodarone?
Answer:As desethylamiodarone is an active metabolite of amioda-rone, the measurement of blood desethylamiodarone concentration may be useful as an index of efficacy and safety of amiodarone therapy as in the case of that of amiodarone.
Commentary:Desethylamiodarone, an active metabolite of amiodarone, has a pharmacological action similar to that of amioda-rone22 and a half-life slightly longer than that of amioda-rone.16 As desethylamiodarone may affect the clinical efficacy of amiodarone therapy, pharmacokinetic analysis of desethylamiodarone may help assess the efficacy of amiodarone therapy. Experimental findings have indicated
that desethylamiodarone is more pulmonary toxic than amiodarone.23 A study has also reported a relationship between the occurrence of pulmonary toxicity and blood desethylamiodarone concentration.20
CQ7 Is TDM effective in ensuring optimal antiarrhythmic treatment with sotalol?
Answer:It is considered difficult to estimate the antiarrhythmic effect of sotalol based on blood drug concentrations. As sotalol has beta-blocking action and potassium channel-blocking action, ECG-based heart rate can be used as an indicator of efficacy, and QT interval as an indicator of the risk of ADRs. No evidence has indicated that TDM is more useful than these indicators.
Level of evidence: VIGrade of recommendation: C2
Commentary:Sotalol acts as a beta-blocker and a class III antiarrhythmic drug (potassium channel blocker). Sotalol exerts its potas-sium channel-blocking effect in relation to dose and blood drug concentration, while it exerts its beta-blocking effect even at low doses or low drug concentrations in blood.25 There is little evidence indicating that the efficacy of sotalol can be expected with blood sotalol concentrations. Many clinicians think that the effective dose differs substantially among patients in the clinical setting (see “III.1.2 Class II Antiarrhythmic Drugs”, page 590).
ECG monitoring is useful because the efficacy of sotalol as a beta-blocking drug can be assessed based on heart rate (see “III.1.2 Class II Antiarrhythmic Drugs”), and the efficacy as a class III antiarrhythmic drug based on QT interval. Only a small number of reports have described the relationship between blood sotalol concentration and its antiarrhythmic effect. In a study of 17 patients with chronic stable ventricular premature complexes, an antiarrhythmic response to sotalol (70 to 100% reduction in VPCs) was observed at a wide range of plasma concentrations (0.34 to 3.44 μg/mL), and significant QTc prolongation was observed at ≥2.55 μg/mL.25 However, the therapeutic dose range for the treatment of ventricular tachycardia or fibrillation, or atrial fibrillation (not covered by NHI in Japan) has not been established.
No superiority of TDM over ECG monitoring has been demonstrated in terms of clinical assessment of patients receiving sotalol for the treatment of arrhythmia. Sotalol is a racemic mixture of d- and l-sotalol, and these isomers differ in their pharmacological effects and pharmacokinetic profiles. The benefit of TDM of d-sotalol, a pure potassium channel-blocking agent, should be assessed in the future.26
HTU10 When should blood samples be taken to perform blood drug concentration monitoring of sotalol?
Answer:Sotalol reaches its peak concentration at about 3 hours after oral administration, and is eliminated at a half-life of 7 to 11 hours. Usually sotalol is administered orally twice a day.27 As sotalol has a low protein-binding rate, a small volume of distribution, and a high renal excretion rate, it has a simple pharmacokinetic profile. Trough blood samples should be obtained for blood drug concentration monitoring

Circulation Journal Vol.81, April 2017
592 AONUMA K et al.
of sotalol, but blood samples obtained in the elimination phase may provide useful data when the interval between dosing and sampling is considered.
▋1.4 Class IV Antiarrhythmic Drugs (Bepridil)CQ8 Is blood drug concentration monitoring effective for patients with arrhythmia receiving bepridil?
Answer:Increased blood bepridil concentrations are associated with increased risk of polymorphic ventricular tachycardia (torsades de pointes) with QT prolongation. Blood bepridil concentration is not useful in predicting its antiarrhythmic effect, but is useful in assessing whether the changed dose is effective or not and whether the patient takes the drug as directed (adherence to medication). Within the same patient, there may be a correlation between the antiarrhythmic effect and blood concentration of bepridil.
Level of evidence: VGrade of recommendation: C1
Commentary:Bepridil undergoes a complex metabolism, has a bioavail-ability of about 60%, and is metabolized in the liver by CYP2D6 and CYP3A4 with a half-life after repeated doses of about 80 hours.28,29 Bepridil increases the risk of polymorphic ventricular tachycardia (torsades de pointes), and a relationship between increased bepridil concentration and QT prolongation has been documented.30–34 The therapeutic range of bepridil is 250 to 800 ng/mL, and the risk of QT prolongation increases at plasma bepridil concentrations of >800 ng/mL.33 The clearance of bepridil is low in low-body-weight individuals and elderly indi-viduals.35,36 Monitoring blood bepridil concentrations is significant in order to assess the safety of treatment.
HTU11 When should blood samples be taken to perform blood drug concentration monitoring of bepridil?
Answer:Basically, blood samples should be obtained at steady state. As it takes about 3 weeks to reach steady-state concentra-tions, a trough blood sample should be taken at around 3 weeks after the initiation of bepridil therapy. However, as bepridil has a nonlinear pharmacokinetic profile, it may take a longer time to reach steady-state concentrations in some patients. Blood bepridil concentrations should be determined even before the steady state is attained when the drug is administered to high-risk patients or when ADRs to bepridil are suspected.
Commentary:Only a small amount of unchanged bepridil is excreted via the kidney. Bepridil is eliminated from the body mainly by hepatic metabolism by CYP2D6 and CYP3A4. Metabolism of bepridil differs substantially among individuals. Bepridil is metabolized slowly, and saturation of CYP2D6 occurs during the process of metabolism, which produces a nonlinear pharmacokinetic profile. As bepridil has an extremely large volume of distribution, and it takes a long period of time for bepridil to diffuse from blood into tissues, careful consideration should be taken to determine when blood samples should be taken.37 When bepridil is admin-
istered repeatedly, it takes 3 weeks to reach steady-state concentrations, but it may take more time in some cases. Blood bepridil concentrations should therefore be evaluated at more than one time point in patients receiving the drug for a long period of time. Blood samples should be taken immediately before the next dose when the drug concentra-tion is at trough, but blood samples may be obtained at other time points. The target therapeutic range is 250 to 800 ng/mL.30,32,33 Blood bepridil concentrations should be determined for patients with a high risk of ADRs and those suspected to have ADRs, even when the steady state has not been achieved. In such cases, blood samples may be obtained at any time points.
▋1.5 Inotropic Drugs (Digoxin)CQ9 Is blood drug concentration monitoring effective for patients with arrhythmia receiving digoxin?
Answer:Blood drug concentration monitoring is useful as it may decrease the occurrence of digitalis intoxication. Data on the time of dosing and that of blood sampling are important to interpret blood digoxin concentrations appropriately. Blood samples should be taken at an appropriate timing.
Level of evidence: IVbGrade of recommendation: B
Commentary:Digitalis intoxication is a common problem in digoxin therapy (Table 3).38,39 It has been reported that high blood digoxin concentrations are a risk factor for digitalis intox-ication.39–41 Reports have indicated that the occurrence of digitalis intoxication during digoxin therapy can be decreased by adjusting the dose based on blood digoxin concentra-tions.4,5,42–44 Since digoxin has a high renal excretion rate, blood digoxin concentrations increase as renal dysfunction. When the effect of treatment is insufficient, data on blood digoxin concentrations may provide useful information on whether the dose should be increased or not, and whether the patient is taking the drug as directed (adherence to medication).
Blood samples for TDM should be taken at an appro-priate timing. When blood samples are taken at an inap-propriate condition such as conducting TDM without a clear purpose, and obtaining a blood sample before reaching a steady state, or within 6 hours after dosing, no TDM assessment can be conducted even if blood concentrations are outside the therapeutic range.45–47
CQ10 Is blood drug concentration monitoring effective for patients with heart failure receiving digoxin?
Answer:Blood drug concentration monitoring is useful as it may decrease the occurrence of ADRs to digoxin. Data on the time of dosing and that of blood sampling are important to interpret blood digoxin concentrations appropriately. Blood samples should be taken at an appropriate timing.
Level of evidence: IVbGrade of recommendation: B

Circulation Journal Vol.81, April 2017
593JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
Commentary:Digoxin causes ADRs in relation to its serum concentration. It has been reported that serum digoxin concentrations may be used as a predictor of digitalis intoxication.40,41 In a post-hoc analysis of the randomized, double-blinded, placebo-controlled Digitalis Investigation Group (DIG) trial48 that was conducted before beta-blocker therapy for heart failure was established in patients with chronic heart failure who had a left ventricular ejection fraction (LVEF) of ≤45% and were in sinus rhythm, an association of serum digoxin concentration and all-cause mortality rate was shown in men. Lower serum digoxin concentrations (0.5 to 0.8 ng/mL) were significantly associated with decreased all-cause mortality rates, and higher concentrations (≥1.2 ng/mL) were significantly associated with increased all-cause mortality rates as compared with patients receiving placebo.49 As digoxin is currently used to alleviate symp-toms and reduce hospitalization due to heart failure rather than to improve their life expectancy, serum digoxin concentration should be maintained low in order to avoid ADRs as much as possible.50 TDM of blood digoxin concentration is considered useful to ensure the safety of treatment.
HTU12 When should blood samples be taken to monitor blood concentrations of digoxin?
Answer:A trough blood sample at 12 to 24 hours after dosing should be obtained from the patient at steady state. When it is difficult to obtain a trough blood sample, it is preferable to obtain a blood sample in the elimination phase, that is at ≥6 hours after dosing. Data from blood samples taken at <6 hours after dosing cannot be interpreted fully, and can only help assess the risk of drug concentration-related ADRs and the patient’s adherence to treatment.
Commentary:It takes a long period of time to achieve equilibrium between blood and tissue digoxin concentrations. When administered orally, digoxin is not fully distributed in the heart until 6 to 8 hours after the last dose, and digoxin concentrations in blood do not represent those in myocar-dium during early hours after dosing. Accordingly, a blood sample should be taken immediately before the next dose to determine a trough concentration. If it difficult to obtain a trough blood sample in the clinical setting, a blood sample should be taken 6 to 8 hours after the last dose (Figure 4).51 As for the timing in terms of the number of days after the initiation of digoxin therapy or the modification of digoxin dose, a blood sample for TDM should be obtained at least 7 days after the initiation or dose modification in patients with intact renal function when blood digoxin concentra-tions have achieved steady state. For patients with renal dysfunction, a blood sample for TDM should be obtained after at least four half-lives (Figure 5).44,51–55 When drug concentration-related ADRs or excessive effects of digoxin are suspected, a blood sample should be taken without delay to determine digoxin concentration.
HTU13 How frequently should blood samples be taken when blood drug concentration monitoring is conducted during long-term digoxin therapy?
Answer:No clear recommendations have been proposed on the frequency or interval of blood drug concentration moni-toring for patients, especially ambulatory patients, who are receiving digoxin for a long period of time. Blood samples may be taken at any time when a change in efficacy, ADRs, or drug interactions are suspected, or when the patient’s condition has changed. It is not necessary to determine digoxin concentrations in patients who respond well to treatment, have a stable condition, and have no change in their treatment regimens. However, annual drug concen-tration monitoring may be acceptable.
Commentary:Blood drug concentration monitoring for patients receiving digoxin is known to reduce the risk of ADRs to digoxin,4,5 but there is no evidence indicating that routine digoxin concentration monitoring helps increase the efficacy of
Table 3. Manifestations of Digitalis Intoxication
1. Cardiac disturbances (cardiotoxicity)
Arrhythmias due to increased automaticity, or due to delayed afterdepolarization
Extrasystoles
Accelerated junctional rhythm
Unifocal or multifocal ventricular bigeminy
Ventricular tachycardia
Bidirectional ventricular tachycardia
Arrhythmias due to decreased conduction velocity and effective refractory period
Asystole
Sinoatrial block
First or second degree (wenckebach) atrioventricular block, advanced or complete heart block
Acceleration of conduction via accessory pathway in WPW syndrome
Multifocal or paroxysmal atrial tachycardia with block
Idioventricular rhythm, atrioventricular dissociation
2. Gastrointestinal symptoms
Anorexia
Nausea
Vomiting
Diarrhea
Abdominal pain
Intestinal ischemia/infarction
3. Central nervous system symptoms
Visual disturbance (blurred vision, yellow vision)
Headache
Weakness
Dizziness
Apathy
Confusion
Mental disturbances (anxiety, depression, delirium, hallucination)
4. Other
Gynecomastia
Thrombocytopenia
Severe hyperkalemia
WPW, Wolff-Parkinson-White. (Adapted from Eichhorn EJ, et al. Prog Cardiovasc Dis 2002; 44: 251 – 266,39 with modifications and with permission from Elsevier. http://www.onlinepcd.com/article/S0033–0620(02)50002–5/abstract)

Circulation Journal Vol.81, April 2017
594 AONUMA K et al.
digoxin therapy and reduces the risk of ADRs.As different patients undergo TDM for different purposes,
the frequency of blood sampling should be determined individually. Serum digoxin concentrations should be determined whenever necessary, such as when ECG changes occur during long-term treatment with digoxin, when ADRs are suspected, or when a change in the patient’s condition may affect the pharmacokinetics or efficacy of digoxin.
As age-related changes in physiological functions may occur even in patients who respond to digoxin, have a stable condition, and may not change their treatment regimens, annual blood drug concentration monitoring is acceptable.
HTU14 What is the target blood concentration of digoxin?
Answer:Minimum effective concentrations should be targeted. Considering the safety and efficacy of digoxin therapy, it is appropriate to target (from 0.5 to) 1.5 ng/mL. For patients
with heart failure due to systolic dysfunction, it is preferable to target ≤0.9 ng/mL.
Commentary:It has been reported that the therapeutic range of digoxin is 0.5 to 2.0 ng/mL,2,38 based on the findings that the risk of ADRs (digitalis intoxication) increases at serum concen-trations of ≥2.0 ng/mL.44,56 A study in Japanese patients has indicated that the risk of gastrointestinal ADRs increases at digoxin concentrations of ≥1.5 ng/mL,57 while another study reported extracardiac ADRs did not developed at digoxin concentrations of <1.4 ng/mL.58 The purpose of blood concentration monitoring of digoxin is the prevention of ADRs, especially extracardiac ADRs, and digoxin should be administered at minimum effective concentrations. Based on the published studies, it is considered appropriate to target a blood digoxin concentration of (0.5 to) 1.5 ng/mL.59
In a post-hoc analysis of the DIG trial in patients with chronic heart failure and systolic dysfunction (LVEF ≤45%), the crude all-cause mortality rate was lower in male patients with lower serum digoxin concentrations (0.5 to 0.8 ng/mL) and higher in those with higher serum digoxin concentrations (≥1.2 ng/mL) than in those receiving placebo.49 An analysis of women with heart failure in the DIG trial demonstrated that lower serum digoxin concentrations (0.5 to 0.9 ng/mL) should be targeted to ensure the efficacy and safety of treatment.60 It is thus preferable to maintain serum digoxin concentrations at ≤0.9 ng/mL when this drug is administered to patients with chronic heart failure due to systolic dysfunction.
HTU15 Can we use digoxin concentrations during blood drug concentration monitoring of methyldigoxin?
Answer:Methyldigoxin, a substance that cross-reacts with digoxin immunoassays, is determined as digoxin in immunoassays. As digoxin concentrations determined with immunoassays represent the sum of concentrations of methyldigoxin and its metabolite digoxin, the results of digoxin immunoassays may be used in TDM of methyldigoxin in the clinical setting. When methyldigoxin is switched to digoxin or vice versa, TDM should be conducted to confirm that the
Figure 5. Change over time in serum digoxin concentrations during repeated doses of digoxin and in a steady state. Digoxin doses are indicated by arrows. (Adapted from Aronson JK, et al. BMJ 1992; 305: 1149 – 1152,44 with permission from BMJ Publishing Group Ltd.)
Figure 4. Serum concentration curve after digoxin or β-methyldigoxin adminis-tration for maintenance therapy. (Adapted from Miyashita H, et al. Jpn Circ J 1986; 50: 628 – 635,51 with modifications.)

Circulation Journal Vol.81, April 2017
595JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
serum digoxin concentration is within the target range.
Commentary:Serum digoxin concentrations are often determined with enzyme immunoassays (EIA) that show cross-reactions between digoxin and methyldigoxin. The sum of concen-trations of digoxin and methyldigoxin are determined as a digoxin concentration. HPLC or other appropriate assays should be used to determine accurate methyldigoxin concentrations. However, considering the absence of substantial differences between methyldigoxin and digoxin in terms of molecular weight and antibody crossreactivity, the sum of methyldigoxin and digoxin concentrations determined with EIA may be used instead of methyldigoxin concentrations in the clinical setting.
The dose should be carefully selected when methyldigoxin is replaced with digoxin or vice versa. As these two substances have different bioavailability, and their phar-macokinetic profiles may differ within and among indi-viduals, a fixed factor cannot be used to convert the dose from methyldigoxin to digoxin or vice versa. Blood drug concentrations should be determined when treatment is changed from methyldigoxin to digoxin or vice versa.
HTU16 Should physicians consider the possible effects of endogenous digoxin-like immunoreactive substances or drugs that have a chemical structure similar to digoxin on blood digoxin concentration monitoring?
Answer:When determined serum digoxin concentrations are higher than expected, the presence of digoxin-like immunoreactive substances (DLISs) should be considered. The patient should also be assessed for the presence/absence of signs/symptoms of digoxin intoxication, clinical features (renal dysfunction, liver disease, neonates, or pregnancy), and concomitant drug use (drugs that have a clinical structure similar to digoxin).
Commentary:Endogenous DLISs may be detected in neonates, pregnant women, patients with renal dysfunction, or patients with liver disease. Several studies have indicated that endogenous DLISs may increase blood digoxin concentrations deter-mined with enzyme immunoassays.61–63
The effect of endogenous or exogenous DLISs on the results of digoxin assays using blood samples differs among the assays used. Data on DLISs in the package insert for the assay used and references should be confirmed in advance.62,64,65 Blood digoxin concentration may differ among assays.66–68
HTU17 Does digitalis intoxication occur in relation to blood digoxin concentration?
Answer:A high blood digoxin concentration is a risk factor for digitalis intoxication, but digitalis intoxication does not always occur only in relation to blood digoxin concentra-tion. The risk of extracardiac signs/symptoms of digitalis intoxication increases at blood digoxin concentrations of ≥1.5 ng/mL.
Commentary:Digitalis intoxication causes cardiac symptoms and extra-
cardiac symptoms such as gastrointestinal symptoms, nervous symptoms, and visual disturbances (Table 3, see page 593).39 For decades it has been reported that the risk of digitalis intoxication is related to blood digoxin concen-tration, and that the incidence of digitalis intoxication is high among patients with high blood digoxin concentra-tions.41,69
It has been suggested that different signs and symptoms of digitalis intoxication develop at different ranges (thresh-olds) of blood digoxin concentrations. In addition to blood digoxin concentration, other risk factors such as age-related changes in physical activity and renal dysfunction, underlying heart disease, sinus dysfunction, and atrioven-tricular conduction disturbance, as well as exacerbating factors such as hypoxemia, hypokalemia, hypomagnesemia, and hypercalcemia may affect the occurrence of digitalis intoxication. The risk of digitalis intoxication cannot be explained only with serum digoxin concentrations. In studies in Japanese patients, the incidence of extracardiac symptoms of digitalis intoxication such as gastrointestinal symptoms increased in patients in whom blood digoxin concentration exceeded 1.5 ng/mL (Figure 6).57,58,70
2. Antimicrobial Drugs for the Treatment of Infective Endocarditis
CQ11 Does TDM of vancomycin help ensure effective treatment of infective endocarditis?
Answer:Confirming the range of blood drug concentrations appro-priate for each patient helps physicians prescribe the drug at an optimal dose and thereby avoid ADRs. TDM is particularly useful in adjusting the dose for patients who do not respond to vancomycin at the current dose, avoiding drug concentration-related ADRs, and assessing the efficacy of treatment when the patient’s condition changes.
Level of evidence: I and IIIGrade of recommendation: A
Figure 6. Serum digoxin concentrations and types and incidence rates of adverse drug reactions (ADRs) in Japanese patients. Assessment of patients with ADRs to digoxin in about 2,500 patients undergoing TDM of digoxin in a medical institution from 1988 to 1993. (Source: Ueno K, et al. Jpn J Hosp Pharm 1995; 21: 105 – 108.57)

Circulation Journal Vol.81, April 2017
596 AONUMA K et al.
Commentary:It has been reported that a lower vancomycin area under the concentration-time curve from 0 to 24 h (AUC24)/minimum inhibitory concentration (MIC) ratio is associated with higher attributable mortality among patients with methicillin-resistant Staphylococcus aureus (MRSA)-asso-ciated complicated bacteremia or infective endocarditis.71 As vegetation may reduce penetration of vancomycin into MRSA,72,73 it is considered that higher trough concentra-tions should be maintained in the treatment of infective endocarditis.73 The guidelines for the diagnosis and treat-ment of infective endocarditis published in the United Kingdom,74 and those in the United States75 recommend that trough serum vancomycin concentrations be maintained at 15–20 μg/mL.On the other hand, an initial trough concentration of ≥15 μg/mL is reported as a risk factor for nephrotoxicity.76
CQ12 Does TDM of aminoglycosides help ensure effective treatment of infective endocarditis?
Answer:Confirming the range of blood drug concentrations appro-priate for each patient helps physicians prescribe the drug at an optimal dose and thereby avoid adverse drug reactions (ADRs). TDM is especially useful in avoiding (trough) drug concentration-related renal dysfunction and assessing the efficacy of treatment when the patient’s condition changes.
Level of evidence: IIGrade of recommendation: B
Commentary:High trough concentrations and a large accumulated dose increase the risk of renal dysfunction due to aminoglyco-sides, and it has been reported that TDM helps reduce the incidence of ADRs to aminoglycosides.77 In the treatment of gram-positive bacterial infections, serum gentamysin concentration should target a trough concentration of ≤1 μg/mL and a peak concentration (Cpeak) of 3 to 5 μg/mL when the drug is given more than once a day.74
HTU18 When should blood samples be taken to monitor blood concentrations of vancomycin?
Answer:Typically, a trough sample within 30 minutes before the next dose should be taken. Routine measurement of peak concentrations is not recommended. For patients with intact renal function, blood samples for TDM should be taken on day 3 of treatment or thereafter, and then once a week. More frequent measurement may be necessary when renal function is unstable.
Commentary:The AUC/MIC ratio is a useful factor of clinical and bacteriological efficacy of vancomycin. However, as there is correlation between trough concentrations and AUC of vancomycin, trough concentrations in the steady state should be determined.75,78 Trough vancomycin concentra-tions should be determined during twice-daily treatment in patients with intact renal function, and during once-daily treatment in those with renal dysfunction. The dose for the treatment of infective endocarditis should be adjusted to
achieve a trough concentration of 15 to 20 μg/mL, which is higher than those for other indications. When renal function is intact, serum vancomycin concentrations reach a steady state in 3 days after the initiation of treatment.79 As the half-life of vancomycin is prolonged in patients with renal dysfunction,80,81 serum drug concentrations should be determined at later time points. Patients who receive vancomycin for a long period of time should be monitored carefully for renal function and changes in trough drug concentrations.
HTU19 When should blood samples for TDM of amino-glycosides be obtained?
Answer:Typically, a trough sample within 30 minutes before the next dose should be taken. The peak concentration at 1 hour after the initiation of intravenous administration should also be determined. For patients with intact renal function, blood samples for TDM should be taken on day 2 or 3 of treatment, and then once a week. More frequent measurement may be necessary when renal function is unstable.
Commentary:The peak concentration/MIC ratios are a useful factor of clinical and bacteriological efficacy of aminoglycosides.82 As there is a relationship between higher trough concentra-tions and the occurrence of nephrotoxicity,83 two blood samples should be obtained to determine trough and peak concentrations. A trough sample should be obtained within 30 minutes before the next dose. The peak concentration that represents drug concentration in the blood after the drug is distributed into tissues should be determined using a blood sample obtained 1 hour after the initiation of intravenous infusion.84 Blood samples should be obtained in the steady state.84 The first blood sample for TDM of an aminoglycoside drug may be obtained on day 2 of treat-ment, but it is practical to obtain it on day 3 as renal function is low in many patients.
HTU20 When should blood samples be taken to monitor blood concentrations of teicoplanin?
Answer:When blood teicoplanin concentration after the loading doses is obtained, a trough sample on day 4 after the initial treatment for 3 days should be obtained regardless of the level of renal function. When a trough teicoplanin concen-tration on the day after the initial treatment for 2 days is determined to confirm drug concentration in an early phase of treatment, a sample should be obtained at least 18 hours after the last dose. TDM should be conducted once a week thereafter. More frequent measurement may be necessary when renal function is unstable.
Commentary:As teicoplanin rarely causes drug concentration-related ADRs at the therapeutic range in the clinical setting, TDM of teicoplanin is conducted to confirm the onset of drug effects. For severe or complicated infections such as infec-tive endocarditis and bone and joint infections, clinicians should target a trough teicoplanin level of ≥20 μg/mL.85–87 During the first three days of treatment, teicoplanin should be administered according to the established protocol

Circulation Journal Vol.81, April 2017
597JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
regardless of the level of renal function. On day 4 and thereafter, the dose should be adjusted according the patient’s renal function. Although the standard procedures for TDM of teicoplanin have not been established, many of the previous reports have described the trough concen-tration on day 4 of treatment. A blood sample should be taken at least 18 hours after the last dosing, when the distribution phase has been completed.84
3. Considerations for Special Patient Populations
▋3.1 Patients With Renal Dysfunction or on Hemodialysis
HTU21 How should blood drug concentration monitoring of antiarrhythmic drugs be conducted for patients with renal dysfunction or those on hemodialysis?
Answer:Disopyramide, cibenzoline, procainamide, pilsicainide, and sotalol are excreted mainly through the kidneys. Flecainide is also excreted through the kidney. A trough sample should be determined immediately before the next dose in the steady state. It takes a longer time to reach the steady state when renally excreted drugs are administered to this patient population.
Commentary:When renally excreted drugs are administered to patients with renal dysfunction or those on hemodialysis, the dose should be reduced or the dosing interval should be increased. Among antiarrhythmic drugs, pilsicainide, sotalol, ciben-zoline, procainamide, and disopyramide are excreted mainly through the kidneys, while flecainide is eliminated through the liver and kidneys.
When renally excreted drugs are administered to patients with renal dysfunction, physicians must consider the effects of the renal function on the pharmacokinetics of these drugs. When these drugs are given to patients on hemodi-alysis, physicians must also consider drug removal with hemodialysis, and the effect of hemodialysis on alpha-1-acid glycoprotein binding. However, drug concentrations in blood are obtained as the sum of concentrations of free drug molecules and protein-bound drug molecules, and it is difficult to delineate the biological fate of free drug molecules.
In order to confirm the efficacy of these drugs and the risk of ADRs, a trough sample should be obtained at a steady state that is achieved after 4 to 5 half-lives. Physicians should be aware that the half-life of renally excreted drugs prolongs as renal function decreases.
In general, drugs with a low protein binding rate (<80%) and a small volume of distribution (<1 L/kg) are removed by hemodialysis.88 As cibenzoline has a large volume of distribution (5 to 7 L/kg) and is not removed by hemodi-alysis, physicians should be aware of this fact when an initial administration strategy is planned. Drugs removed by hemodialysis should be administered after a hemodialysis session.
HTU22 How should blood drug concentration monitoring of digoxin be conducted for patients with renal dysfunction or those on hemodialysis?
Answer:A trough blood sample at 12 to 24 hours after dosing should be obtained at the steady state. When it is difficult to obtain a trough blood sample, it is preferable to obtain a blood sample in the elimination phase, that is at ≥6 hours after dosing. As digoxin is mainly excreted through the kidneys, administration plans should be made according to the patient’s renal function. As it takes 2 to 3 weeks to achieve the steady state level of digoxin in patients with end-stage renal disease or those on hemodialysis, blood samples for TDM should be obtained thereafter.
Commentary:As digoxin is a renally excreted drug with 70% of the dose excreted unchanged in the urine, the dose for patients with renal dysfunction should be adjusted according to the patient’s renal function. As the half-life of digoxin is prolonged in patients with renal dysfunction, it takes longer time to achieve a steady state. It is appropriate to obtain a blood sample after a week of treatment for patients with renal dysfunction, and after 2 to 3 weeks of treatment for patients with end-stage renal disease or those on hemodialysis.
Digoxin has a large volume of distribution of 4 to 8 L/kg in patients with intact renal function, and is distributed mainly in the skeletal muscle. The volume of distribution of digoxin decreases as renal dysfunction, but is still as large as 4 to 5 L/kg in patients with end-stage renal disease.89 Digoxin cannot be removed efficiently by any type of renal replacement therapy.90,91 Therefore, the initial administra-tion planning and TDM are important. In patients on hemodialysis, a blood sample for TDM should be obtained before a hemodialysis session. Patients who start a session in the morning should be instructed to take digoxin after the session in order to avoid blood sampling during the distribution phase.
Patients with renal dysfunction are prone to be affected by DLIS, and some immunoassays may cause false high values (see HTU16 [page 595]).92 The effects of P-glycopro-tein inhibitors and inducers on the pharmacokinetics of digoxin are similar between patients on hemodialysis and individuals with intact renal function.93
Dose Selection for Patients With Renal DysfunctionA leading principle in dose selection for patients with renal dysfunction is reducing the dose of “drugs of which unchanged compound or active metabolites are largely excreted in the urine”.
The Giusti-Hayton method has been used as a simple method to adjust the dose and/or dosage interval in patients with renal dysfunction (Figure 7).94 For example, when a patient with a creatinine clearance (CCr) of 30 mL/min receives digoxin (percentage of the dose excreted unchanged in the urine [fe]: 0.7) to obtain the effect equivalent to that obtained in patients with intact renal function (CCr: 120 mL/min) receiving digoxin at a dose of 0.125 mg once daily, the patient should receive the drug at a dose of 0.060 mg once daily, when he/she prefers a once-daily regimen. This adjusted dose is the product of the factor G (1 to 0.7 × (1 to 30/120) [nearly equal] 0.48) and the dose for those with intact renal function (0.125 mg).
When the dose adjustment is made by changing the dosing interval, the appropriate interval can be calculated as a quotient of the interval for those with intact renal function and the factor G (24 hours/0.48=50 hours). The

Circulation Journal Vol.81, April 2017
598 AONUMA K et al.
patient may receive digoxin at a dose of 0.125 mg every other day.
HTU23 How should TDM of vancomycin be conducted for patients with renal dysfunction or those on hemodialysis who are complicated with infective endocarditis?
Answer:In patients with renal dysfunction who are not undergoing hemodialysis, a trough concentration during 30 minutes before the next dose should be determined in principle. In patients on hemodialysis, a blood sample should be taken before a hemodialysis session, and an additional dose of vancomycin should be administered after the session. Routine measurement of peak vancomycin concentration is not recommended. As the time to achieve a steady state prolongs as renal function decreases, it takes 2 to 3 weeks to achieve the steady state in patients on hemodialysis. In order to shorten the time to achieve the steady state, an initial loading dose of vancomycin should be given at 15 to 20 mg/kg for patients with renal dysfunction, and at 25 to 30 mg/kg for those with severe renal dysfunction and those on hemodialysis.
Commentary:It has been reported that renal dysfunction may lead to decreased immunity, and that the incidence of infective endocarditis in patients on hemodialysis is 17-fold that in the general population,95 and that the outcome of infective endocarditis is poor in this patient population. As vanco-mycin is a renally excreted drug with 90% of the dose excreted unchanged in the urine, the dose should be adjusted according to the patient’s renal function. In the treatment of infective endocarditis, trough vancomycin concentrations should be maintained high at 15 to 20 μg/mL, which may impair the patient’s renal function. As vancomycin should be given for a long period of time in the treatment of infective endocarditis, TDM is necessary to continue the treatment safely and effectively.
As the time to achieve steady state concentrations of vancomycin prolongs as renal function decreases, it takes 2 to 3 weeks to achieve the steady state in patients on hemodialysis. In order to shorten the time to achieve the steady state, an initial loading dose of vancomycin should be given at 15 to 20 mg/kg for patients with renal dysfunction, and at 25 to 30 mg/kg for those with severe renal dysfunction and those on hemodialysis.
In patients with renal dysfunction who are not undergoing
hemodialysis, a trough concentration during 30 minutes before the next dose should be determined. In patients on hemodialysis, a blood sample should be taken before a hemodialysis session, and an additional dose of vancomycin should be administered after the session. In order to confirm that vancomycin concentrations are within the optimal range, TDM should be conducted in the first week of treatment. As a rebound in serum vancomycin concentra-tions occurs after hemodialysis, serum vancomycin concen-trations immediately after a hemodialysis session do not reflect the drug concentration within the target tissue.96
▋3.2 CirrhosisHTU24 How should blood drug concentration monitoring of antiarrhythmic drugs be conducted for patients with cirrhosis?
Answer:Cirrhosis delays the elimination of antiarrhythmic drugs that are metabolized extensively in the liver. As such, when these drugs are administered in patients with cirrhosis, dose reduction with blood concentration monitoring should be considered on the basis of the severity of hepatic dysfunc-tion. Careful consideration for dose reduction is especially essential for patients with severe cirrhosis of Child-Pugh class C.
Commentary:Cirrhosis delays the elimination of many antiarrhythmic drugs that are metabolized in the liver. Therefore, dose adjustment according to blood drug concentration moni-toring should be considered (Table 4). Flecainide clearance is 42% lower in patients with cirrhosis than in healthy volunteers, and the elimination half-life is prolonged by 5-fold.97 The reduction of propafenone clearance in patients with hepatic dysfunction is small (about 25%), but the elimination half-life is prolonged by 2.5-fold, and the bioavailability increases by 3.6-fold compared with healthy volunteers.98 Lidocaine clearance is 28 to 56% lower in patients with severe cirrhosis of Child-Pugh class C than in healthy volunteers, and the elimination half-life is prolonged by 2.6 to 4.2-fold.99–101 Mexiletine clearance is 28% lower in patients with advanced alcoholic cirrhosis than in healthy volunteers, and the elimination half-life is prolonged by about 3-fold.102 Since aprindine, amiodarone, and bepridil are eliminated mostly by hepatic metabolism, the clearance of these drugs may be delayed with the progression of cirrhosis. Blood drug concentration monitoring of these drugs is acceptable in patients with cirrhosis.
Blood concentrations of drugs that are eliminated by both hepatic metabolism and renal excretion may increase unexpectedly as the patients with cirrhosis develop renal dysfunction. Blood drug concentration monitoring is acceptable for such cases.
▋3.3 Thyroid DysfunctionHTU25 How should blood concentration monitoring of digoxin be conducted for patients with thyroid dysfunction?
Answer:Blood digoxin concentrations are low in patients with hyperthyroidism and high in those with hypothyroidism. For patients whose thyroid function decreased or increased
Figure 7. Treatment design for patients with renal dysfunction: The Giusti-Hayton method. (Source: Giusti DL, et al. Drug Intel Clin Pharm 1973; 7: 382 – 387.94)

Circulation Journal Vol.81, April 2017
599JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
during digoxin therapy, physicians should assess the efficacy of digoxin and determine blood digoxin concentrations to reconsider the administration plan.
Commentary:Several reports have described that blooddigoxin concen-trations are low in patients with hyperthyroidism and high in those with hypothyroidism.106–108 It has been reported that digoxin concentrations in blood are 14% lower in patients with hyperthyroidism and 35% higher in those with hypothyroidism as compared with those in the euthyroid state.107
It has also been reported that changes in digoxin concen-trations in blood associated with thyroid dysfunction disappear when thyroid function returns to normal (euthy-roid).107,108 It is therefore desirable that clinical evaluation and blood digoxin concentration monitoring should be conducted to reconsider the patient’s administrationplan not only when thyroid function decreases but also when it increases after treatment for thyroid conditions.
▋3.4 Elderly PatientsHTU26 How should blood drug concentration monitoring of antiarrhythmic drugs be conducted for elderly patients?
Answer:Physiological function declines with age, and reduced renal function (i.e., low glomerularfiltration rate) is especially common among elderly patients. Elderly patients with reduced renal function have lower renal clearance and longer half-lives of drugs excreted by the kidneys. In general, TDM using a blood sample obtained at the steady state is recommended. If possible, a trough blood sample or a blood sample during the elimination phase should be obtained. As elderly patients may respond to or have ADRs to antiarrhythmic drugs before achieving steady-state concen-trations, TDM at the onset of efficacy or ADRs may also
be beneficial. The initial dose should be set carefully.
Commentary:Physiological function in the elderly is lower than in younger people. As glomerular filtration rate and renal blood flow are low in elderly people, systemic clearance of drugs excreted by the kidenys, i.e., drugs with ≥50% of the dose excreted unchanged in the urine, is substantially lower in the elderly than younger people. As elderly patients have low clearance rates and longer half-lives of renally-excreted drugs, it takes a longer time to achieve steady-state concen-trations of these drugs (it generally takes 4-5 half-lives). Drug concentrations in blood may also be high. Accord-ingly, drug concentrations should be determined before steady-state concentrations to confirm whether drug concentrations are within the therapeutic range. When elderly patients are treated with antiarrhythmic drugs that are extensively excreted by the kidneys, the initial dose should be set carefully. A nomogram for digoxin therapy may help the physician determine the initial dose according to the patient’s renal function and age.
Elderly patients tend to have abrupt changes in patho-logical and physiological conditions, a reduction in total protein in blood, and dehydration, among others, which may affect the drug’s clearance and unbound drug fraction in blood. Blood drug concentration monitoringshould therefore be conducted in response to changes in the patient’s condition. The total drug concentration that represents the sum of free and protein-bound drug mole-cules, rather than the unbound drug fraction, may be used in TDM for these cases. However, physicians should be aware that an increase in free drug concentration due to a change in the unbound drug fraction may lead to a stronger response (or ADRs) even when the total drug concentration is within the therapeutic range.
HTU27 How should blood drug concentration monitoring of pilsicainide be conducted for elderly patients?
Table 4. Delayed Clearance of Hepatically-Metabolized Antiarrhythmic Drugs in Patients With Cirrhosis and Dose Adjustment
Drug Major enzymes Clearance in patients with cirrhosis Desirable dose
Quinidine CYP3A4 No change103,104 (The half-life is prolonged) No recommendations
Procainamide N-acetyltransferase No sufficient data No recommendations
Disopyramide CYP3A4 No sufficient data No recommendations
Aprindine CYP2D6 No data No recommendations
Mexiletine CYP2D6, 1A2 Reduced102 1/3
Lidocaine CYP3A4 Reduced99–101 1/3–1/2
Flecainide CYP2D6, 1A2 Reduced97 1/3–1/2
Propafenone CYP2D6 Reduced98 1/3–1/2
Amiodarone CYP3A4 No data No recommendations
Bepridil CYP2D6 No data No recommendations
Reference: Child-Pugh classification for severity of liver disease105
Score 1 2 3
Hepatic encephalopathy None Mild (Grade I–II) Coma (Grade III or severe)
Ascites Absent Slight Moderate
Serum bilirubin (mg/dL) <2.0 2.0–3.0 >3.0
Serum albumin (g/dL) >3.5 2.8–3.5 <2.8
Prolonged prothrombin time (sec) 1–4 4–6 >6
Child-Pugh classification. Class A: A total score of 5 to 6. Class B: A total score of 7 to 9. Class C: A total score of 10 to 15. (Adopted from Pugh RN, et al. Br J Surg 1973; 60: 646 – 649,105 with modifications.)

Circulation Journal Vol.81, April 2017
600 AONUMA K et al.
Answer:A trough blood sample or a blood sample during the elimination phase should be obtained on day 4 or 5 of treatment or thereafter after achieving steady-state concen-trations. However, a sample should be taken earlier when the patient shows a strong response or possible ADRs to determine blood concentrations. When the dose is changed, a blood sample should be taken 4 or 5 days after the dose change or thereafter to determine whether drug concentra-tions are within the therapeutic range. When renal function is stable, changes in drug concentrations in blood depend on the dose.
Commentary:As pilsicainide is a drug excreted by the kidneys with about 90% of the dose excreted unchanged in the urine, the systemic clearance of the drug is affected substantially by renal function. As renal function is reduced in elderly patients, special care should be taken to develop adminis-tration plans for them. As pilsicainide has a short half-life (4 to 5 hours in healthy adults), pilsicainide concentrations in blood achieve the steady state in 2 to 3 days after the initiation of treatment. When pilsicainide is administered to elderly patients, it is important to set the initial dose carefully, and blood drug concentration monitoring during the initial phase of treatment. A nomogram for calculating the initial dose of pilsicainide has been developed on the basis of a population pharmacokinetics analysis, and should be used to set the initial dose for elderly patients (Figure 8).109,110
HTU28 How should blood drug concentration monitoring of digoxin be conducted for elderly patients?
Answer:A trough blood sample at 12 to 24 hours after dosing should be obtained from the patient at steady state. When it is difficult to obtain a trough blood sample, it is preferable to obtain a blood sample in the elimination phase, i.e., at ≥6 hours after dosing. As renal function is low in elderly patients, and it takes a longer period of time to achieve steady state drug concentrations, administration plans should be developed according to the patient’s renal func-tion. Drug concentrations in blood tend to be higher in
elderly patients with low body weight or low muscle mass.
Commentary:As elderly people tend to have reduced renal function and receive multiple drugs, and those with a fragile constitution have a reduction in muscle mass, blood concentrations of digoxin, adrug excreted by the kidneys, tends to be higher than in younger patients.111 Although the effects of aging on renal function and muscle mass differ among individuals, digoxin therapy should be planned individually according to the patient’s renal function, and the dose and dosing interval should be adjusted via TDM. Patients should be instructed to visit the clinic when they have nausea, anorexia, diarrhea, confusion, disorientation, visual impairment, and/or severe bradycardia, which suggest digoxin intoxication.
▋3.5 ChildrenHTU29 When antiarrhythmic drugs are administered to children, can physicians target blood drug concentrations similar to those for adults?
Answer:Although no reports have described blood drug concentra-tion monitoring of antiarrhythmic drugs in children, it is considered that target blood drug concentrations, i.e., therapeutic range, of these drugs are roughly similar between children and adults.
Commentary:Dosage regimens and reference therapeutic ranges of antiar-rhythmic drugs for children.- Lidocaine
Indications: Mainly indicated for the treatment of ven-tricular tachycardia (its effects on atrial muscle is small).Intravenous injection: 1 to 2 mg/kg, administer by slow intravenous injectionContinuous infusion: 1 to 3 mg/kg/hr (15 to 50 μg/kg/min)Reference therapeutic range: 1 to 5 μg/mL
After metabolized in the liver, 70% of the dose is excreted in the urine. The half-life is ≤2 hours in healthy individuals.
- MexiletineIndications: Mainly indicated for the treatment of ven-tricular tachycardia (its effects on atrial muscle is small), and long QT syndrome (especially LQT3).Intravenous injection: 2 to 3 mg/kg, administer by slow intravenous injectionContinuous infusion: 0.4 to 0.6 mg/kg/hrOral administration: 5 to 10 mg/kg/day, usually divided into 3 dosesReference therapeutic range: 0.5 to 2 μg/mL
After metabolized in the liver, the drug is excreted in the urine. The half-life is 10 hours in healthy individuals.
- DisopyramideIndications: Atrial arrhythmia, ventricular arrhythmia, and supraventricular tachycardia Intravenous injection: 1 to 2 mg/kg, inject intravenously over 5 to 20 minutes Oral administration: 5 to 10 mg/kg/dayReference therapeutic range: 2 to 4 μg/mL
Part of the dose is metabolized in the liver, the metab-olites and free disopyramide are excreted in the urine. Children need higher oral doses per body weight than adults to achieve effective disopyramide concentrations
Figure 8. A nomogram for calculating the initial dose of pilsicainide (mg/day) according to renal function. Males= (140–age)×body weight/(72×SCr). Females=the dose in males×0.85. CCr, creatinine clearance; SCr, serum creatinine level. (Adapted from Ueno K, et al. Pharma Medica 2003; 21: 165 – 171,109 with permission from Medical Review Co., Ltd.)

Circulation Journal Vol.81, April 2017
601JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
in blood.112 Because of its anticholinergic activity, diso-pyramide may increase ventricular rate during atrial tachycardia, worsen glaucoma, or cause dysuria, consti-pation, hypoglycemia, or agranulocytosis.
- PilsicainideIndications: Tachyarrhythmia (supraventricular and ventricular)Intravenous injection: 1 to 1.5 mg/kg, inject over 10 minutesOral administration: 2 mg/kg/dayReference therapeutic range: 0.2 to 0.9 μg/mL
Most of the dose is excreted unchanged in the urine. The half-life is about 4 hours in adults.
- FlecainideIndications: Tachyarrhythmia (paroxysmal atrial fibrilla-tion/flutter, paroxysmal supraventricular tachyarrhythmia, ventricular tachyarrhythmia)Intravenous injection: 1 to 2 mg/kg or 100 to 150 mg/m2, administer by slow intravenous injectionOral administration: 3 to 5 mg/kg/day. The daily dose may be divided into 2 doses for some children <1 year of age and those ≥12 years of age, but usually into 3 doses.
The use in children has been approved in Japan.Reference therapeutic range: 0.2 to 1 μg/mL
About a third of the dose is metabolized in the liver, and about two thirds of the dose are excreted unchanged into the urine. The half-life of oral flecainide is about 8 hours in children 1 to 12 years of age, and 11 hours in infants under 1 year of age and children ≥12 years of age.113
- PropranololIntravenous injection: 0.05 to 0.1 mg/kg, administer by slow intravenous injectionOral administration: 1 to 4 mg/kg/day, usually divided into 3 dosesReference therapeutic range: 0.05 to 0.1 μg/mL
- AmiodaroneIntravenous injection: Initiate the treatment with either the loading dose of 5 mg/kg over 30 minutes or ≤5 bolus doses of 1 mg/kg with ≥5 minute intervals. Maintain the treatment at a dose of 10 mg/kg/day.Oral administration: Initiate the treatment at a dose of 10 to 20 mg/kg (divided into 1 or 2 doses) for 1 to 2 weeks, and maintain the treatment at a dose of 5 to 10 mg/kg (divided into 1 or 2 doses).Reference therapeutic range: 0.5 to 1.0 μg/mL
- SotalolOral administration: Initiate the treatment at a dose of 1 to 2 mg/kg, increase the dose up to 6 mg/kg, divided into 2 doses. For children ≥2 years of age, initiate the treatment at 90 to 100 mg/body surface area (m2)/day, divided into 2 doses. The maximum dose is 250 mg/m2/day.Reference therapeutic range: ?
- BepridilIndications: Patients with persistent atrial fibrillation or ventricular tachyarrhythmia who are intolerable or do not respond to other antiarrhythmic drugs.Oral administration: 1 to 2 mg/kg/day, divided into 2 dosesReference therapeutic range: As patients may respond to bepridil at concentrations under the common therapeutic range, the treatment should be initiated at a low dose according to the patient’s condition.
Few reports have described the use of bepridil in infants. As bepridil blocks calcium channel, this drug should be considered contraindicated for neonates and young infants as in the case of verapamil.
HTU30 When digoxin is administered to children, can physicians target blood drug concentrations similar to those for adults?
Answer:It may be considered that the therapeutic range of digoxin is roughly similar between children and adults, but prema-ture babies and children with renal dysfunction should be treated at lower doses and need more frequent blood drug concentration monitoring sessions.
Commentary:Digoxin is used to slow atrioventricular conduction, and is indicated for the treatment of supraventricular arrhythmias, such as atrioventricular reciprocating tachycardia and atrioventricular nodal reentrant tachycardia. Digoxin is not appropriate for the treatment of atrioventricular block, Wolff-Parkinson-White (WPW) syndrome, or ventricular tachycardia. Digoxin has only limited benefits in the treatment of heart failure, and is rarely used as a first-line drug for heart failure.
Intravenous injection: For rapid digitalization, administer 0.04 mg/kg to infants and young children, or 0.03 mg/kg to school children. (A half of the dose is given at the first injection, and the remaining dose is divided into 2 or 3 doses by slow intravenous injections with an interval of 6 to 8 hours.)
Oral administration: Maintenance dose: 0.0075 to 0.01 mg/kg/day for infants and young children, 0.005 to 0.0075 mg/kg/day for school children, divided into 1 or 2 doses. The half-life is 20 hours in infants, and 40 hours in children (36 to 48 hours in adults).
Therapeutic range: 0.5 to 2.0ng/mL. As digoxin has a narrow therapeutic range, physicians should observe patients carefully for digitalis intoxication. When rapid digitalization is not necessary, it is safe to start the treatment at the maintenance dose. Patients should also be monitored for hypokalemia.
HTU31 When glycopeptides or aminoglycosides are administered to children with infective endocarditis, can physicians target blood drug concentrations similar to those for adults?
Answer:Children are treated with antimicrobial drugs according to the regimens recommended for adults. The therapeutic ranges of antimicrobial drugs in children may be considered identical to those in adults.
Commentary:The prognosis of infective endocarditis depends on factors including whether the patient is an infant, has a large vegetation (>20 mm), heart failure, or staphylococcal infection. The risk of ADRs to antimicrobial drugs listed in Tables 5 and 6 is low, and the results are favorable in many cases.114–116 Regular TDM sessions should be con-ducted for children receiving glycopeptides or aminogly-cosides to adjust the treatment regimen accordingly.117,118
Pharmacokinetics of Antimicrobial Drugs in Children and Treatment Planning- Vancomycin
Dose: 30 to 40 mg/kg/day, divided into 2 to 4 dosesThe usual dose should be 15 mg/kg every 8 hours for

Circulation Journal Vol.81, April 2017
602 AONUMA K et al.
children, 10 to 15 mg/kg every 12 hours for neonates <1 week of age, and 10 to 15 mg/kg every 8 hours for neonates 1 week to 1 month of age. TDM of vancomycin should be conducted on days 3 and 7 of treatment and weekly thereafter to adjust the dosage regimen.118–124
Target drug concentrations in blood: 25 to 40 μg/mL for peak concentrations, and 10 to 15 μg for trough concen-trations.
Trough vancomycin concentrations ranged from 10 to 15 μg/mL in children who received the drug at a dose of 60 mg/kg/day for the treatment of meninges. Although no prospective studies were conducted to assess the efficacy and safety of vancomycin in children, these concentrations are considered effective and safe in children.
Further studies should be carried out to confirm the efficacy and safety of vancomycin with regimens that achieve a trough concentration of 15 to 20 μg/mL, the target for adults.123
Half-life: About 2 hoursAs the clearance of vancomycin depends on renal func-
tion, the half-life of the drug varies among children in whom renal function develops differently with age. 6 to 10 hours in neonates; 4 hours in children 3 months to 3 years
of age; and 2 to 3 hours in children over 3 years of age.ADRs: It has been reported that the risk of auditory ADRs increases when peak concentrations range between 60 and 80 μg/mL, and that of ADRs related to renal tox-icity increases when trough concentrations are ≥20 μg/mL.
- TeicoplaninDose: Administer three doses of 10 mg/kg with 12-hour intervals, and infuse at a dose of 10 mg/kg/day thereafter. The dose should be infused over 30 minutes and should be adjusted according to teicoplanin concentrations in blood. Although a trough concentration of ≥15 μg/mL may not be maintained at this standard dose, there is no evidence on high-dose treatment with teicoplanin in chil-dren. Further studies are awaited.125–132 Neonates should be treated with an initial loading dose of 16 mg/kg fol-lowed by a maintenance dose of 8 mg/kg/day. The dose should be infused intravenously over at least 30 minutes.Elimination half-life: As the half-life is 50 hours, TDM should be conducted after 7 days of treatment. Target trough concentrations are ≥20 μg/mL (if possible 25 μg/mL). Although peak concentrations are not determined com-monly, a peak concentration of about 40 μg/mL should be obtained. The half-life of teicoplanin varies among chil-
Table 5. Antimicrobial Therapy for Infective Endocarditis
Causative organism
Antimicrobial agents
Treatment period
Streptococci 1. Penicillin G + gentamicin Penicillin G: 4 weeks
2. Ampicillin + gentamicin Ampicillin: 4 weeks
3. Ceftriaxone + gentamicin Ceftriaxone: 4 weeks
4. Vancomycin ± gentamicin Gentamicin: 2 weeks
Vancomycin: 4 weeks
Staphylococcus aureus (methicillin-sensitive)
1. Cefazolin ± gentamicin Cefazolin: 4–6 weeks
2. Vancomycin ± gentamicin Gentamicin: 2 weeks
Vancomycin: 4–6 weeks
Staphylococcus aureus (methicillin-resistant)
Vancomycin (or teicoplanin) ± gentamicin Vancomycin: 4–6 weeks
Gentamicin: 2 weeks
Enterococci 1. Ampicillin + gentamicin Ampicillin: 6 weeks
2. Vancomycin + gentamicin Gentamicin: 4–6 weeks
Vancomycin: 4–6 weeks
Gram-negative bactgeria (HACEK) Ceftriaxone ± gentamicin Ceftriaxone: 4 weeks
Gentamicin: 2 weeks
(Adapted from the Japanese Circulation Society. Guidelines for the prevention and treatment of infective endocarditis (JCS 2008),116 with modifications.)
Table 6. Antimicrobial Therapy for Infective Endocarditis of Unknown Etiology
Causative organisms
Antimicrobial agents
Treatment period
Postoperative cases with a negative blood culture result
Vancomycin ± gentamicin Vancomycin: 6–8 weeks
Gentamicin: 2 weeks
Non-postoperative cases with a negative blood culture result
Cefazolin + gentamicin ± penicillin G Cefazolin: 6–8 weeks
Gentamicin: 2 weeks
Penicillin G: 6–8 weeks
• Daily dose for children with normal renal function. Penicillin G: 200,000 to 300,000 U/kg/day, divided into 4–6 doses. Gentamicin: 3 mg/kg/day, divided into 3 doses. Vancomycin: 30 to
40 mg/kg/day, divided into 2 to 4 doses. Cefazolin: 100 mg/kg/day, divided into 4 doses. Ceftriaxone: 75 to 100 mg/kg/day, divided into 2 doses. Ampicillin: 200 to 300 mg/kg/day, divided into 4 doses.
(Adapted from the Japanese Circulation Society. Guidelines for the prevention and treatment of infective endocarditis (JCS 2008),116 with modifications.)

Circulation Journal Vol.81, April 2017
603JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
dren in whom renal function develops differently with age.ADRs: The incidence of ADRs to teicoplanin is relatively lower than that to vancomycin.
- Aminoglycosides (Gentamicin)Dose: 3 to 7.5 mg/kg/day, divided into 3 doses.
As the level of accumulation of aminoglycosides cor-relates with their toxicity and can be predicted from trough drug concentrations, patients receiving aminogly-cosides should be monitored for peak and trough concen-trations in blood from an early phase of treatment.118,133–136
Target concentrations in blood: Target concentrations are lower than in adults: 3 to 5 μg/mL for peak concentra-tions that are obtained at 1 hour after administration, and <1 μg/mL for trough (pre-dose) concentrations.Half-life: About 2 hours in children. 3 to 11.5 hours in neonates <1 week of age; 3 to 6 hours in neonates 1 week to 1 month of age; and 3 to 5 hours in infants [under 12 months of age]. As younger children have a longer half-life than older children, neonates are usually treated at a dose of 5 to 7.5 mg/kg every 24 hours.
After the first few days of treatment, blood urea nitrogen (BUN) and serum creatinine levels should be determined regularly to monitor for potential renal ADRs. The peak concentrations at 0.5 to 1 hour after administration should range between 5 and 10 μg/mL. Trough concen-trations immediately before the next dose should be tar-geted at <2 μg/mL. As trough concentrations over 2 μg/mL represent an accumulation of the drug, the dose should be
reduced to achieve a trough concentration of <2 μg/mL even when peak concentrations are not increased.
Once-daily treatment with aminoglycosides is conducted in adults and some children. Once-daily regimens are associated with peak aminoglycoside concentrations that are 2 to 3-fold those obtained with more frequent dosage regimens, and very low trough concentrations. As the bactericidal effects of aminoglycosides are concentration-dependent, once-daily regimens that can achieve higher concentrations in blood are more effective than more frequent dosage regimens. In adults, the incidence of nephrotoxicity of aminoglycosides is lower in once-daily dosing than in three-times-daily dosing, but clinical experience with once-daily dosing is limited in children.137
▋3.6 Women During Pregnancy and BreastfeedingCQ13 What are indications and precautions for the use of antiarrhythmic drugs in women during pregnancy and breastfeeding?
Answer:Only a limited number of reports have described TDM of antiarrhythmic drugs in women during pregnancy and breastfeeding. Physicians should monitor drug concentra-tions in blood and observe the patients carefully according to the therapeutic ranges of these drugs in adults. Table 7 summarizes the current findings as of 2015 on the use of
Table 7. Current Findings on the Use of Antiarrhythmic Drugs During Pregnancy or Breastfeeding (as of 2015)
Drugs ClassUse during pregnancy Use during breastfeeding
Briggs Placental transfer Briggs Hale Transfer
to milk
Procainamide I Limited human data No relevant animal data
⃝ Limited human data Probably compatible
L3 ⃝
Disopyramide I Human data suggest risk in 3rd trimeste
⃝ Limited human data Probably compatible
L2 ⃝
Quinidine I Compatible ⃝ Limited human data Probably compatible
L2 ⃝
Aprindine I No data No data No data No data No data
Lidocaine I Compatible ⃝ Limited human data Probably compatible
L2 ⃝
Pilsicainide hydrochloride
I No data No data No data No data No data
Propafenone I Limited human data Animal data suggest moderate risk
⃝ Limited human data Probably compatible
L2 ⃝
Mexiletine I Limited human data Animal data suggest low risk
⃝ Limited human data Probably compatible
L2 ⃝
Flecainide I Limited human data Animal data suggest moderate risk
⃝ Limited human data Probably compatible
L3 ⃝
Cibenzoline succinate I No data No data No data No data No data
Pirmenol I No data No data No data No data No data
Propranolol II Human data suggest risk in 2nd and 3rd trimesters
⃝ Limited human data Potential toxicity
L2 ⃝
Amiodarone III Human and animal data suggest risk ⃝ Contraindicated L5 ⃝Sotalol III Human data suggest risk in 2nd
and 3rd trimesters⃝ Limited human data
Potential toxicityL4 ⃝
Bepridil* IV No human data Animal data suggest low risk
No human data
No human data Probably compatible
L4 ⃝
Digoxin (methyldigoxin) Inotropic drugs Compatible ⃝ Compatible L2 ⃝Digitoxin Inotropic drugs Compatible ⃝ Compatible L3 ⃝
*As bepridil is no longer distributed in the United States as of 2014, the descriptions on this drug is based on the findings available in 2012. Bepridil is available in Japan.

Circulation Journal Vol.81, April 2017
604 AONUMA K et al.
antiarrhythmic drugs during pregnancy or breastfeeding.
Level of evidence: VGrade of recommendation: C1
Commentary:Physicians should consider the pharmacokinetic profile of the drug, as well as the increased circulating fluid volume, changes in vascular resistance and permeability, changes in hemodynamics including increased heart rate, and func-tional changes of visceral organs during pregnancy, and conduct TDM sessions more frequently in pregnant women. Data on placental drug transfer are important in considering potential adverse drug reactions or adverse events on the fetus and the efficacy of fetal therapy. The benefits and risks of using a particular drug during breastfeeding should be considered on the basis of the milk/plasma drug concen-tration ratio (M/P ratio), relative infant dose (RID), half-life, time to achieve the peak concentration, molecular weight (drugs with a molecular weight of <200 are readily excreted into the milk), and other pharmacokinetic param-eters of the drug, as well as the infant’s conditions such as premature birth, body weight, cardiovascular structure and function, the maturity and stability of visceral organs such as the kidneys, liver, and the nervous, metabolism, and blood coagulation systems, and the pathophysiology of the infant’s underlying disease, if present. The expected risks and benefits on the mother, fetus, and infant of using and not using antiarrhythmic drugs during pregnancy or breastfeeding must be explained to pregnant and breast-feeding women and their families to obtain their consent before starting or not starting treatment. As drug informa-tion may change over time, and different textbooks express different opinions, healthcare professionals should refer to current editions of standard textbooks such as Drugs in Pregnancy and Lactation138 and Medications and Mothers’ Milk,139 as well as guidelines published in Japan115,140,141
and information centers* in order to determine the use of drugs during pregnancy and breastfeeding in a compre-hensive manner.
*Japan Drug Information Institute in Pregnancy in the National Center for Child Health and Development: Breastfeeding and Medicationhttps://www.ncchd.go.jp/kusuri/lactation/index.html(National Institutes of Health; NIH): Drugs and Lactation Database (Lactmed)http://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm
4. Pharmacokinetic Profiles of Cardiovascular Drugs
Pharmacokinetic Profiles of Antiarrhythmic DrugsTable 8 summarizes the route of excretion and pharmaco-kinetic parameters of antiarrhythmic drugs.
5. Drug Interactions of Cardiovascular Drugs
During treatment with antiarrhythmic drugs, healthcare professionals should carefully observe for the following three types of drug interactions:(1) Interaction With Drugs That Prolong QT IntervalQT interval should be monitored during the use of the following drugs regardless of whether antiarrhythmic drugs are used concomitantly or not: vardenafil, moxifloxacin, toremifene, fingolimod, or others.(2) Pharmacodynamic Drug InteractionsDrugs that affect cardiac function such as beta-blockers should be used carefully [with antiarrhythmic drugs] as this combination may also prolong QT interval through a pharmacodynamic interaction.(3) Pharmacokinetic Drug InteractionsPharmacokinetic drug interactions may lead to adverse
Table 8. Major Route of Excretion and Pharmacokinetic Parameters of Antiarrhythmic Drugs
Generic name
Volume of distribution
(L/kg)
Protein binding rate (%)
Major route of excretion
Percentage of metabolites
(%)
CYP enzymes mainly
responsible for the
metabolism
Percentage of the dose
excreted unchanged in the urine (%)
Half-life (hr)
Reference therapeutic
range (μ/mL)
Amiodarone*1,*2 106 96 Liver 100 3A4, 2C8 <1 14–107 days*4 0.5–2(?)
Nifekalant 0.14 90 Liver 90– Conjugation 28–31 1–2 –*5
Lidocaine*1,*2 1–2 70 Liver 95– 3A4 <10 1–3 2–5
Quinidine 3 80–90 Liver 70–90 3A4 20 6–8 2–5
Aprindine*2 3 95–98 Liver 100 2D6 <1 1–2 days 0.25–1
Propafenone*1,*2 3.7 75–88 Liver 90– 2D6 3 3–5 0.05–1(?)
Bepridil*2 8 99 Liver 95– 2D6 <1 80 0.2–0.8
Mexiletine 5–12 70 Liver 90– 2D6, 1A2 6 10 0.5–2.0
Disopyramide 0.6 20–75 Liver/kidney 40–50 3A4 48 5–9 2–5
Flecainide 7–10 60 Liver/kidney 60 2D6 40 11–15 0.2–1
Procainamide*2 1.7–2.4 15 Liver/kidney 40–50 NAT*3 60 2–3 4–10
Pirmenol 1–1.5 80 Liver/kidney 35 3A4(?) 20–30 7–10 0.4–(?)
Cibenzoline 7 70 Kidney 35 2D6 55–62 5–6 0.2–0.8
Pilsicainide 1.5 35 Kidney 10 – 75–86 4–5 0.2–0.9
Sotalol 1.2–2.4 10 Kidney 0 – 75 7–11 ?*6
*1Producing active metabolites; *2non-linear excretion, *3N-acetyltransferase; *4about 13 hours after a single administration; *5Not determined in commercial laboratories; *6Not established in Japanese (adults). All drugs listed above other than nifekalant are covered with the specific therapeutic drug monitoring fees.

Circulation Journal Vol.81, April 2017
605JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
drug reactions due to an increase in drug concentrations in blood or loss of efficacy due to a decrease in drug concen-trations in blood. Table 2 (page 588) lists major enzymes that are involved in the metabolism of antiarrhythmic
drugs, and Table 9 summarizes drugs that affect blood concentrations of antiarrhythmic drugs in TDM.
Table 9. Drugs That Affects Blood Concentrations of Antiarrhythmic Drugs
Antiarrhythmic drugs
Drugs used concomitantly Effects Mechanisms of
drug interactions
Disopyramide Carbamazepine Decrease in blood concentration by about 50%142–144 Induction of drug-metabolizing enzymes
Rifampicin Decrease in blood concentration Induction of drug-metabolizing enzymes
Phenytoin Decrease in blood concentration Induction of drug-metabolizing enzymes
Erythromycin Occurrence of serious ADRs associated with QT prolongation145
Inhibition of drug-metabolizing enzymes
Clarithromycin Occurrence of serious ADRs associated with QT prolongation146
Inhibition of drug-metabolizing enzymes
Indinavir About 3-fold increase in drug concentration147 Inhibition of drug-metabolizing enzymes
Saquinavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Ritonavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Nelfinavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Mexiletine Rifampicin Decrease in blood concentration by about 50%148,149 Induction of drug-metabolizing enzymes
Phenytoin Decrease in blood concentration Induction of drug-metabolizing enzymes
Phenobarbital Decrease in blood concentration Induction of drug-metabolizing enzymes
Aprindine Amiodarone About 1.5-fold increase in blood concentration150 Inhibition of drug-metabolizing enzymes
Verapamil About 2-fold increase in blood concentration151 Inhibition of drug-metabolizing enzymes
Diltiazem About 2-fold increase in blood concentration152 Inhibition of drug-metabolizing enzymes
Pilsicainide Cetirizine Decrease in renal clearance by about 40%153 Inhibition of renal excretion
Flecainide Cimetidine About 1.3-fold increase in AUC154 Inhibition of drug-metabolizing enzymes
Amiodarone About 1.5-fold increase in blood concentration155 Inhibition of drug-metabolizing enzymes
Procainamide Amiodarone Reduce the dose of procainamide by about 20%156,157
Inhibition of renal excretion
Trimethoprim About 1.5-fold increase in blood concentration158,159 Inhibition of renal excretion
Ofloxacin About 1.2-fold increase in blood concentration160,161 Inhibition of renal excretion
Levofloxacin Increase in blood concentration Inhibition of renal excretion
Cimetidine About 1.3-fold increase in blood concentration162–164 Inhibition of renal excretion
Propafenone Cimetidine About 1.5-fold increase in blood concentration147 Inhibition of drug-metabolizing enzymes
Rifampicin Decrease in blood concentration165,166 Induction of drug-metabolizing enzymes
Amiodarone Possible increase in blood concentration147 Inhibition of drug-metabolizing enzymes
Quinidine Increase in blood concentration Inhibition of drug-metabolizing enzymes
Amiodarone Grapefruit juice About 2-fold increase in drug concentration167 Inhibition of drug-metabolizing enzymes (in the gastrointestinal tract)
Sotalol Magnesium/aluminum Decrease in blood concentration by about 30% when taken concomitantly
Inhibition of gastrointestinal absorption
These drugs should be taken 2 hours apart168
Bepridil Indinavir About 3-fold increase in blood concentration147 Inhibition of drug-metabolizing enzymes
Saquinavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Ritonavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Nelfinavir Increase in blood concentration Inhibition of drug-metabolizing enzymes
Quinidine Amiodarone Reduce the dose of quinidine by about 40%157,169–173 Inhibition of drug-metabolizing enzymes
Itraconazole 1.6-fold increase in blood concentration174 Inhibition of drug-metabolizing enzymes
Ketoconazole Increase in blood concentration171 Inhibition of drug-metabolizing enzymes
Erythromycin QT prolongation due to increase in blood concentration172
Inhibition of drug-metabolizing enzymes
Phenytoin Decrease in blood concentration by about 50%173,175 Induction of drug-metabolizing enzymes
Phenobarbital Decrease in blood concentration by about 50%176,177 Induction of drug-metabolizing enzymes
Rifampicin Decrease in blood concentration by about 50%178–180 Induction of drug-metabolizing enzymes
Carbamazepine Decrease in blood concentration by about 30%181 Induction of drug-metabolizing enzymes
Cimetidine About 1.2-fold increase in blood concentration182,183 Inhibition of drug-metabolizing enzymes
Fluvoxamine Decrease in hepatic clearance by 29–44%184 Inhibition of drug-metabolizing enzymes
AUC, area under the blood concentration time curve.

Circulation Journal Vol.81, April 2017
606 AONUMA K et al.
References 1. The Japanese Society of Clinical Pharmacology and Thera-
peutics, editor. Clinical Pharmacology & Therapeutics, 3rd edn. Tokyo: Igaku Shoin, 2011 (in Japanese).
2. Campbell TJ, Williams KM. Therapeutic drug monitoring: Antiarrhythmic drugs. Br J Clin Pharmacol 2001; 52(Suppl 1): 21S – 34S.
3. Boobis AR, Shiga T, Edwards RJ. Genetic polymorphisms and cardiovascular drug metabolism. In: Martin R Wilkins, editor. Cardiovascular pharmacogenetics. Springer-Verlag, 2003: 39 – 77.
4. Aronson JK, Hardmann M. ABC of monitoring drug therapy: Measuring plasma drug concentrations. BMJ 1992; 305: 1078 – 1080.
5. Ried LD, Horn JR, McKenna DA. Therapeutic drug monitoring reduces toxic drug reactions: A meta-analysis. Ther Drug Monit 1990; 12: 72 – 78.
6. Reynolds DJ, Aronson JK. ABC of monitoring drug therapy: Making the most of plasma drug concentration measurements. BMJ 1993; 306: 48 – 51.
7. Woosley RL. Role of plasma concentration monitoring in the evaluation of response to antiarrhythmic drugs. Am J Cardiol 1988; 62: 9H – 17H.
8. Tsuchishita Y, Itoh K, Mizokawa N, et al. Relationship between serum cibenzoline concentrations and hypoglycemia. Jpn J Ther Drug Monitor 2003; 20: 331 – 333.
9. Takada M, Shibakawa M. Efficacy of therapeutic drug moni-toring in prevention of hypoglycemia caused by cibenzoline. Eur J Clin Pharmacol 2001; 57: 695 – 700.
10. Tsuchishita Y, Fukumoto K, Kusumoto M, et al. Relationship between serum aprinndine concentration and neurologic side effects in Japanese. Biol Pharm Bull 2009; 32: 637 – 639.
11. Atkinson AJ Jr, Stec GP, Lertora JJ, et al. Impact of active metabolites on monitoring plasma concentrations of therapeutic drugs. Ther Drug Monit 1980; 2: 19 – 27.
11a. Romero K, Woosely RL. Arrhythmia and conductance distur-bances. In: Antman EM, Sabatine MS, editors. Cardiovascular therapeutics: A companion to Braunwald’s Heart Disease, 4th edn. Elsevier, 2013: 343 – 364.
12. Buxton ILO, Benet LZ. Pharmacokinetics: The dynamics of drug absorption, distribution, action, and elimination: Intro-duction. In: Brunton LL, Chabner BA, Knollmann BC, et al., editors. Goodman & Gilman’s the pharmacological basis of therapeutics, 12th edn. McGraw-Hill, 2011: 17 – 39.
13. Westfall TC, Westfall DP. Adrenergic agonists and antagonists. In: Brunton LL, Chabner BA, Knollmann BC, et al., editors. Goodman & Gilman’s the pharmacological basis of therapeutics, 12th edn. McGraw-Hill, 2011: 277 – 334.
14. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part I. Clin Pharmacokinet 2009; 48: 689 – 723.
15. Walle T, Webb JG, Bagwell EE, et al. Stereoselective delivery and actions of beta receptor antagonist. Biochem Pharmacol 1988; 37: 115 – 124.
16. Podrid PJ. Amiodarone: Reevaluation of an old drug. Ann Intern Med 1995; 122: 689 – 700.
17. Haffajee CI, Love JC, Canada AT, et al. Clinical pharmacoki-netics and efficacy of amiodarone for refractory tachyarrhyth-mias. Circulation 1983; 67: 1347 – 1355.
18. Stäubli M, Bircher J, Galeazzi RL, et al. Serum concentrations of amiodarone during long-term therapy: Relation to dose, efficacy and toxicity. Eur J Clin Pharmacol 1983; 24: 485 – 494.
19. Rotmensch HH, Belhassen B, Swanson BN, et al. Steady-state serum amiodarone concentrations: Relationships with antiar-rhythmic efficacy and toxicity. Ann Intern Med 1984; 101: 462 – 469.
20. Yamada Y, Shiga T, Matsuda N, et al. Incidence and predictors of pulmonary toxicity in Japanese patients receiving low-dose amiodarone. Circ J 2007; 71: 1610 – 1616.
21. Shiga T. Transition from intravenous amiodarone to oral maintenance therapy: Pharmacokinetic considerations. Jpn J Electrocardiology 2010; 30: 354 – 358 (in Japanese).
22. Yabek SM, Kato R, Singh BN. Effects of amiodarone and its metabolite, desethylamiodarone, on the electrophysiologic properties of isolated cardiac muscle. J Cardiovasc Pharmacol 1986; 8: 197 – 207.
23. Quaglino D, Ha HR, Duner E, et al. Effects of metabolites and analogs of amiodarone on alveolar macrophages: Structure-activity relationship. Am J Physiol Lung Cell Mol Physiol 2004; 287: L438 – L447.
24. Deleted in proof. 25. Wang T, Bergstrand RH, Thompson KA, et al. Concentration-
dependent pharmacologic properties of sotalol. Am J Cardiol 1986; 57: 1160 – 1165.
26. Drayer DE. Pharmacodynamic and pharmacokinetic differences between drug enantiomers in humans: An overview. Clin Pharmacol Ther 1986; 40: 125 – 133.
27. Drug interview form of Sotalol tablets, revised in April 2012. 28. Benet LZ. Pharmacokinetics and metabolism of bepridil. Am J
Cardiol 1985; 55: 8C – 13C. 29. Bepricor(R) Tablets 50 mg/Bepricor(R) Tablets 100 mg Drug
Interview Form. Revised in August, 2014 (9th edition) (in Japanese).
30. Sugi K, Kusano A, Noro M, et al. From bench to bedside of bepridil. Characteristics of pharmacokinetics of bepridil. Jpn J Electrocardiology 2007; 27: 30 – 35 (in Japanese).
31. Kurita T, Yasuda M, Nakazato Y, et al. From bench to bedside of bepridil: 8. Proarrhythmic effects and other adverse effects. Jpn J Electrocardiology 2007; 27: 61 – 73 (in Japanese).
32. Kamakura T, Yamada Y, Okamura E, et al. Optimal dose and blood concentration of bepridil in patients with arrhythmias. Jpn J Electrocardiology 2011; 31: 150 – 157 (in Japanese).
33. Shiga T, Suzuki A, Naganuma M, et al. Clinical outcome in paroxysmal or persistent atrial fibrillation patients receiving bepridil. Circ J 2011; 75: 1334 – 1342.
34. Miura S, Sumiyoshi M, Tsuchiya H, et al. The serum bepridil concentration as a safe rhythm control strategy in patients with atrial tachyarrhythmias. J Arrhythmia 2012; 28: 187 – 191.
35. Fukumoto K, Kasai H, Tsuchishita Y, et al. Population phar-macokinetics of bepridil in patients with atrial fibrillation. JPN J TDM 2012; 29: 77 – 82 (in Japanese).
36. Shiga T, Hashiguchi M, Naganuma M, et al. Contributing factors to the apparent clearance of bepridil in patients with paroxysmal or persistent atrial fibrillation: Analysis using a population pharmacokinetics method. Ther Drug Monitor 2013; 35: 367 – 373.
37. Ueno K, Fukumoto K. Summary of therapeutic drug monitoring (TDM) and pharmacokinetics of bepridil. Journal of Clinical Therapeutics & Medicines 2012; 28: 877 – 885 (in Japanese).
38. Sampson KJ, Kass RS. Anti-arrhythmic drugs. In: Brunton LL, Chabner BA, Knollmann BC, et al., editors. Goodman & Gilman’s the pharmacological basis of therapeutics, 12th edn. McGraw-Hill, 2011: 815 – 848.
39. Eichhorn EJ, Gheorghiade M. Digoxin. Prog Cardiovasc Dis 2002; 44: 251 – 266.
40. Beller GA, Smith TW, Abelmann WH, et al. Digitalis intoxica-tion: A prospective clinical study with serum level correlations. N Engl J Med 1971; 284: 989 – 997.
41. Ordog GJ, Benaron S, Bhasin V, et al. Serum digoxin levels and mortality in 5,100 patients. Ann Emerg Med 1987; 16: 32 – 39.
42. Koch-Weser J, Duhme DW, Greenblatt DJ. Influence of serum digoxin concentration measurements on frequency of digitoxicity. Clin Pharmacol Ther 1974; 16: 284 – 287.
43. Duhme DW, Greenblatt GJ, Koch-Weser J. Reduction of digoxin toxicity associated with measurements of serum levels: A report from the Boston Collaborative Drug Surveillance Program. Ann Intern Med 1976; 80: 516 – 519.
44. Aronson JK, Hardmann M. ABC of monitoring drug therapy. Digoxin. BMJ 1992; 305: 1149 – 1152.
45. Wing D, Duff HJ. Impact of a therapeutic drug monitoring program for digoxin. Arch Intern Med 1987; 147: 1405 – 1408.
46. Cañas F, Tanasijevic MJ, Na’luf N, et al. Evaluating the appro-priateness of digoxin level montoring. Arch Intern Med 1999; 159: 363 – 368.
47. Mordaini MR, Krähenbühl S, Schlienger RG. Appropriateness of digoxin level monitoring. Swiss Med Wkly 2002; 132: 506 – 512.
48. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med 1997; 336: 525 – 533.
49. Rathore SS, Curtis JP, Wang Y, et al. Association of serum digoxin concentration and outcomes in patients with heart failure. JAMA 2003; 289: 871 – 878.
50. Adams KF Jr, Ghali JK, Herbert Patterson J, et al. A perspective on re-evaluating digoxin’s role in the current management of patients with chronic systolic heart failure: Targeting serum concentration to reduce hospitalization and improve safety profile. Eur J Heart Fail 2014; 16: 483 – 493.
51. Miyashita H, Sato T, Tamura T, et al. The problems of digitalis therapy from the viewpoint of serum concentration with special

Circulation Journal Vol.81, April 2017
607JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
reference to the sampling time, to the overlapping range of serum concentration where intoxicated and non-intoxicated patients are located and to atrial fibrillation. Jpn Circ J 1986; 50: 628 – 635.
52. Winter ME. Digoxin. In: Winter ME, editor. Basic clinical pharmacokinetics, 5th edn. Lippincott Williams & Wilkins/Wolters Kluwer Health, 2010: 198 – 239.
53. Aronson JK. Clinical pharmacokinetics of digoxin. Clin Pharmacokinet 1980; 5: 137 – 149.
54. Hori R, Miyazaki K, Mizugaki M, et al. Estimation of popula-tion pharmacokinetic parameters in Japanese (1): Digoxin. JPN J TDM 1994; 11: 7 – 17 (in Japanese).
55. Kramer WG, Kolibash AJ, Lewis RP, et al. Pharmacokinetics of digoxin: Relationship between response intensity and pre-dicted compartmental drug levels in man. J Pharmacokinet Biopharm 1979; 7: 47 – 61.
56. Smith TW, Haber E. Digoxin intoxication: The relationship of clinical presentation to serum digoxin concentration. J Clin Invest 1970; 49: 2377 – 2386.
57. Ueno K, Uchimi Y, Ishida Y, et al. Effect of TDM on frequency of digoxin toxicity. Jpn J Hosp Pharm 1995; 21: 105 – 108 (in Japanese).
58. Miura T, Kojima R, Sugiura Y, et al. Effect of aging on the incidence of digoxin toxicity. Ann Pharmacother 2000; 34: 427 – 432.
59. Hauptman PJ, Kelly RA. Digitalis. Circulation 1999; 99: 1265 – 1270.
60. Adams KF Jr, Patterson JH, Gattis WA, et al. Relationship of serum digoxin concentration to mortality and morbidity in women in the Digitalis Investigation Group trial: A retrospective analysis. J Am Coll Cardiol 2005; 46: 497 – 504.
61. Stone JA, Soldin SJ. An update on digoxin. Clin Chem 1989; 35: 1326 – 1331.
62. Valdes R Jr. Endogenous digoxin-like immunoreactive factors: Impact on digoxin measurements and potential physiological implications. Clin Chem 1985; 31: 1525 – 1532.
63. Dasgupta A. Endogenous and exogenous digoxin-like immuno-reactive substances: Impact on therapeutic drug monitoring of digoxin. Am J Clin Pathol 2002; 118: 132 – 140.
64. Dasgupta A, Reyes MA. Effect of Brazilian, Indian, Siberian, Asian, and North American ginseng on serum digoxin measure-ment by immunoassays and binding of digoxin-like immunore-active components of ginseng with Fab fragment of antidigoxin antibody (Digibind). Am J Clin Pathol 2005; 124: 229 – 236.
65. Konno A, Terasawa Y, Aono H, et al. The cross-reactivity in digoxin TDM using dimension. Jpn J TDM 2005; 22: 113 – 114 (in Japanese).
66. Katagiri F, Sato N, Tsutsumi K, et al. Evaluation of the plasma drug concentrations by Aalternation of analytical method from TDx and atomic absorption spectrometric method to dimension Xpand. JPN J TDM 2007; 24: 34 – 39 (in Japanese).
67. Jones TE, Morris RG. Discordant results from “real-world” patient samples assayed for digoxin. Ann Pharmacother 2008; 42: 1797 – 1803.
68. Hermida-Cadahía EF, Calvo MM, Tutor JC. Interference of circulating endogenous antibodies on the Dimension® DGNA digoxin immunoassay: Elimination with a heterophilic blocking reagent. Clin Biochem 2010; 43: 1475 – 1477.
69. Smith TW, Haber E. Digitalis (third of four parts). N Engl J Med 1973; 289: 1063 – 1072.
70. Ueno K, Miyai K. Studies on the potentially toxic serum digoxin concentration in the Japanese. Jpn J Hosp Pharm 1991; 17: 34 – 37 (in Japanese).
71. Brown J, Brown K, Forrest A. Vancomycin AUC24/MIC ratio in patients with complicated bacteremia and infective endocar-ditis due to methicillin-resistant Staphylococcus aureus and its association with attributable mortality during hospitalization. Antimicrob Agents Chemother 2012; 56: 634 – 638.
72. Fernández Guerrero ML, González López JJ, Goyenechea A, et al. Endocarditis caused by Staphylococcus aureus: A reap-praisal of the epidemiologic, clinical, and pathologic manifesta-tions with analysis of factors determining outcome. Medicine (Baltimore) 2009; 88: 1 – 22.
73. Giuliano C, Haase KK, Hall R. Use of vancomycin pharmaco-kinetic-pharmacodynamic properties in the treatment of MRSA infections. Expert Rev Anti Infect Ther 2010; 8: 95 – 106.
74. Gould FK, Denning DW, Elliott TS, et al; Working Party of the British Society for Antimicrobial Chemotherapy. Guidelines for the diagnosis and antibiotic treatment of endocarditis in adults: A report of the Working Party of the British Society for
Antimicrobial Chemotherapy. J Antimicrob Chemother 2012; 67: 269 – 289.
75. Rybak M, Lomaestro B, Rotschafer JC, et al. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm 2009; 66: 82 – 98.
76. van Hal SJ, Paterson DL, Lodise TP. Systematic review and meta-analysis of vancomycin-induced nephrotoxicity associated with dosing schedules that maintain troughs between 15 and 20 milligrams per liter. Antimicrob Agents Chemother 2013; 57: 734 – 744.
77. Bartal C, Danon A, Schlaeffer F, et al. Pharmacokinetic dosing of aminoglycosides: A controlled trial. Am J Med 2003; 114: 194 – 198.
78. Andrés I, López R, Pou L, et al. Vancomycin monitoring: One or two serum levels? Ther Drug Monit 1997; 19: 614 – 619.
79. Nakashima M, Katagiri K, Oguma T. Phase I studies on vancomycin hydrochloride for injection. Jpn J Chemother 1992; 40: 210 – 224 (in Japanese).
80. Rodvold KA, Blum RA, Fischer JH, et al. Vancomycin phar-macokinetics in patients with various degrees of renal function. Antimicrob Agents Chemother 1988; 32: 848 – 852.
81. Yasuhara M, Iga T, Zenda H, et al. Population pharmacokinetics of vancomycin in Japanese adult patients. Ther Drug Monit 1998; 20: 139 – 148.
82. Blaser J, Stone BB, Groner MC, et al. Comparative study with enoxacin and netilmicin in a pharmacodynamic model to determine importance of ratio of antibiotic peak concentration to MIC for bactericidal activity and emergence of resistance. Antimicrob Agents Chemother 1987; 31: 1054 – 1060.
83. Streetman DS, Nafziger AN, Destache CJ, et al. Individualized pharmacokinetic monitoring results in less aminoglycoside-associated nephrotoxicity and fewer associated costs. Pharma-cotherapy 2001; 21: 443 – 451.
84. The Japanese Society of Chemotherapy Amtimicrobial TDM Guidelines Development Committee, the Japanese Society of Therapeutic Drug Monitoring TDM Guidelines Development Committee for Antimicrobial agents, eds. Guidelines for TDM of antimicrobial agents. Kyorinsha 2012 (in Japanese).
85. Wilson AP, Gaya H. Treatment of endocarditis with teicoplanin: A retrospective analysis of 104 cases. J Antimicrob Chemother 1996; 38: 507 – 521.
86. Leport C, Perronne C, Massip P, et al. Evaluation of teicoplanin for treatment of endocarditis caused by gram-positive cocci in 20 patients. Antimicrob Agents Chemother 1989; 33: 871 – 876.
87. Greenberg RN. Treatment of bone, joint, and vascular-access-associated gram-positive bacterial infections with teicoplanin. Antimicrob Agents Chemother 1990; 34: 2392 – 2397.
88. Hirata S, Izumi S, Furukubo T, et al. Factors influencing the removal rate of drugs by hemodialysis. JPN J TDM 2005; 22: 141 – 142 (in Japanese).
89. Kramer P. Digitalis pharmacokinetics and therapy with respect to impaired renal function. Klin Wochenschr 1977; 55: 1 – 11.
90. Hirata S, Izumi S, Furukubo T, et al. Factors influencing the removal rate of drugs by hemodialysis. J Jpn Soc Dial Ther 2004; 37: 1893 – 1900 (in Japanese).
91. Pancorbo S, Comty C. Digoxin pharmacokinetics in continuous peritoneal dialysis. Ann Intern Med 1980; 93: 639.
92. Fitzsimmons WE. Influence of assay methodologies and inter-ferences on the interpretation of digoxin concentrations. Drug Intell Clin Pharm 1986; 20: 538 – 542.
93. Hirata S, Izumi S, Furukubo T, et al. Interaction between clarithromycin and digoxin in patients with end stage renal disease. Int J Pharmacol Ther 2005; 43: 30 – 36.
94. Giusti DL, Hayton WL. Dosage regimen adjustments in renal impairment. Drug Intel Clin Pharm 1973; 7: 382 – 387.
95. Abbott KC, Agodoa LY. Hospitalizations for bacterial endocarditis after initiation of chronic dialysis in the United States. Nephron 2002; 91: 203 – 209.
96. Pollard TA, Lampasona V, Akkerman S, et al. Vancomycin redistribution: Dosing recommendations following high-flux hemodialysis. Kidney Int 1994; 45: 232 – 237.
97. McQuinn RL, Pentikäinen PJ, Chang SF, et al. Pharmacokinetics of flecainide in patients with cirrhosis of the liver. Clin Pharmacol Ther 1988; 44: 566 – 572.
98. Lee JT, Yee YG, Dorian P, et al. Influence of hepatic dysfunction on the pharmacokinetics of propafenone. J Clin Pharmacol 1987; 27: 384 – 389.

Circulation Journal Vol.81, April 2017
608 AONUMA K et al.
99. Orlando R, Piccoli P, De Martin S, et al. Effect of the CYP3A4 inhibitor erythromycin on the pharmacokinetics of lidocaine and its pharmacologically active metabolites in subjects with normal and impaired liver function. Br J Clin Pharmacol 2003; 55: 86 – 93.
100. Orlando R, Piccoli P, De Martin S, et al. Cytochrome P450 1A2 is a major determinant of lidocaine metabolism in vivo: Effects of liver function. Clin Pharmacol Ther 2004; 75: 80 – 88.
101. Colli A, Buccino G, Cocciolo M, et al. Disposition of a flow-limited drug (lidocaine) and a metabolic capacity-limited drug (theophylline) in liver cirrhosis. Clin Pharmacol Ther 1988; 44: 642 – 649.
102. Pentikäinen PJ, Hietakorpi S, Halinen MO, et al. Cirrhosis of the liver markedly impairs the elimination of mexiletine. Eur J Clin Pharmacol 1986; 30: 83 – 88.
103. Kessler KM, Humphries WC Jr, Black M, et al. Quinidine pharmacokinetics in patients with cirrhosis or receiving pro-pranolol. Am Heart J 1978; 96: 627 – 635.
104. Debruyne D, Gram LF, Grollier G, et al. Quinidine disposition in relation to antipyrine elimination and debrisoquine phenotype in alcoholic patients with and without cirrhosis. Int J Clin Pharmacol Res 1989; 9: 319 – 325.
105. Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973; 60: 646 – 649.
106. O’Connor P, Feely J. Clinical pharmacokinetics and endocrine disorders: Therapeutic implications. Clin Pharmacokinet 1987; 13: 345 – 364.
107. Burk O, Brenner SS, Hofmann U, et al. The impact of thyroid disease on the regulation, expression, and function of ABCB1 (MDR1/ P glycoprotein) and consequences for the disposition of digoxin. Clin Pharmacol Ther 2010; 88: 685 – 694.
108. Shenfield GM, Thompson J, Horn DB. Plasma and urinary digoxin in thyroid dysfunction. Eur J Clin Pharmacol 1977; 12: 437 – 443.
109. Ueno K, Kawai M, Tanaka K, et al. Pharmacokinetics of pilsicainide and the development of a nomogram for adjusting loading doses of pilsicainide. Pharma Medica 2003; 21: 165 – 171 (in Japanese).
110. Fukumoto K, Tanemura M, Tsuchishita Y, et al. Effect of protein binding of pilsicainide on the pharmacokinetics. Drug Metab Pharmacokinet 2005; 20: 183 – 186.
111. Yukawa M, Yukawa E, Suematsu F, et al. Determination of digoxin clearance in Japanese elderly patients for optimization of drug therapy: A population pharmacokinetics analysis using nonlinear mixed-effects modelling. Drugs Aging 2011; 28: 831 – 841.
112. Baker EJ, Hayler AM, Curry PV, et al. Measurement of plasma disopyramide as a guide to paediatric use. Int J Cardiol 1986; 10: 65 – 69.
113. Perry JC, McQuinn RL, Smith RT Jr, et al. Flecainide acetate for resistant arrhythmias in the young: Efficacy and pharmaco-kinetics. J Am Coll Cardiol 1989; 14: 185 – 191.
114. Baddour LM, Wilson WR, Bayer AS, et al. Infective endocar-ditis: Diagnosis, antimicrobial therapy, and management of complications: A statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: Endorsed by the Infectious Diseases Society of America. Circulation 2005; 111: e394 – e434.
115. Guidelines for Diagnosis and Treatment of Cardiovascular Diseases (2010–2011 Joint Working Groups Report). Guide-lines for drug therapy in pediatric patients with cardiovascular diseases (JCS2012). Circ J 2014; 78: 507 – 533. http://www.j-circ.or.jp/guideline/pdf/JCS2012_sachi_h.pdf (in Japanese).
116. Guidelines for Diagnosis and Treatment of Cardiovascular Diseases (2007 Joint Working Groups Report). Guidelines for the prevention and treatment of infective endocarditis (JCS 2008). http://www.j-circ.or.jp/guideline/pdf/JCS2008_miyatake_h.pdf (in Japanese).
117. Kearns GL, Abdel-Rahman SM, Alander SW, et al. Develop-mental pharmacology--drug disposition, action, and therapy in infants and children. N Engl J Med 2003; 349: 1157 – 1167.
118. Bradley JS, Nelson JD. Nelson’s pediatric antimicrobial therapy, 19th edn. American Academy of Pediatrics, 2013.
119. Frymoyer A, Hersh AL, Benet LZ, et al. Current recommended dosing of vancomycin for children with invasive methicillin-resistant Staphylococcus aureus infections is inadequate.
Pediatr Infect Dis J 2009; 28: 398 – 402.120. Broome L, So TY. An evaluation of initial vancomycin dosing
in infants, children, and adolescents. Int J Pediatr 2011; 2011: 470364.
121. Kim DI, Im MS, Choi JH, et al. Therapeutic monitoring of vancomycin according to initial dosing regimen in pediatric patients. Korean J Pediatr 2010; 53: 1000 – 1005.
122. Eiland LS, English TM, Eiland EH 3rd. Assessment of vanco-mycin dosing and subsequent serum concentrations in pediatric patients. Ann Pharmacother 2011; 45: 582 – 589.
123. McKamy S, Hernandez E, Jahng M, et al. Incidence and risk factors influencing the development of vancomycin nephro-toxicity in children. J Pediatr 2011; 158: 422 – 426.
124. Yasuhara M, Iga T, Zenda H, et al. Population pharmacokinetics of vancomycin in Japanese pediatric patients. Ther Drug Monit 1998; 20: 612 – 618.
125. Sunakawa K, Nonoyama M, Iwai N, et al. Pharmacokinetic and clinical studies on teicoplanin for sepsis by methicillin-cephem resistant Staphyloccus aureus in the pediatric and neonate field. Jpn J Antibiot 2002; 55: 656 – 677 (in Japanese).
126. Sánchez A, López-Herce J, Cueto E, et al. Teicoplanin pharma-cokinetics in critically ill paediatric patients. J Antimicrob Chemother 1999; 44: 407 – 409.
127. Reed MD, Yamashita TS, Myers CM, et al. The pharmacoki-netics of teicoplanin in infants and children. J Antimicrob Chemother 1997; 39: 789 – 796.
128. Dufort G, Ventura C, Olivé T, et al. Teicoplanin pharmacoki-netics in pediatric patients. Pediatr Infect Dis J 1996; 15: 494 – 498.
129. Kobayashi M, Arima M, Kimura T, et al. Population pharma-cokinetics of teicoplanin in infants and children. Jpn J Chemother 2007; 55: 17 – 22 (in Japanese).
130. Kacet N, Dubos JP, Roussel-Delvallez M, et al. Teicoplanin and amikacin in neonates with staphylococcal infection. Pediatr Infect Dis J 1993; 12: 10 – 20.
131. Degraeuwe PL, Beuman GH, van Tiel FH, et al. Use of teico-planin in preterm neonates with staphylococcal late-onset neonatal sepsis. Biol Neonate 1998; 73: 287 – 294.
132. Fanos V, Kacet N, Mosconi G. A review of teicoplanin in the treatment of serious neonatal infections. Eur J Pediatr 1997; 156: 423 – 427.
133. Bartelink IH, Rademaker CM, Schobben AF, et al. Guidelines on paediatric dosing on the basis of developmental physiology and pharmacokinetic considerations. Clin Pharmacokinet 2006; 45: 1077 – 1097.
134. Murphy JE, Austin ML, Frye RF. Evaluation of gentamicin pharmacokinetics and dosing protocols in 195 neonates. Am J Health Syst Pharm 1998; 55: 2280 – 2288.
135. Knight JA, Davis EM, Manouilov K, et al. The effect of post-natal age on gentamicin pharmacokinetics in neonates. Pharma-cotherapy 2003; 23: 992 – 996.
136. Stolk LM, Degraeuwe PL, Nieman FH, et al. Population pharmacokinetics and relationship between demographic and clinical variables and pharmacokinetics of gentamicin in neonates. Ther Drug Monit 2002; 24: 527 – 531.
137. Best EJ, Gazarian M, Cohn R, et al. Once-daily gentamicin in infants and children: A prospective cohort study evaluating safety and the role of therapeutic drug monitoring in minimizing toxicity. Pediatr Infect Dis J 2011; 30: 827 – 832.
138. Briggs GG, Freeman RK. Drugs in pregnancy and lactation, 10th edn. Wolters Kluwer Health, 2015.
139. Hale WT, Rowe EH. Medications and mothers’ milk, 16th edn. Hale Publishing, 2014.
140. Ito S, Murashima A, eds. Drug treatment consultation: Preg-nancy and lactation, 2nd edition. Nanzando 2014 (in Japanese).
141. Guidelines for Diagnosis and Treatment of Cardiovascular Diseases (2009 Joint Working Groups Report). Guidelines for indication and management of pregnancy and delivery in women with heart disease (JCS 2010). http://www.j-circ.or.jp/guideline/pdf/JCS2010niwa.h.pdf.
142. Staum JM. Enzyme induction: Rifampin-disopyramide interac-tion. DICP 1990; 24: 701 – 703.
143. Aitio ML, Mansury L, Tala E, et al. The effect of enzyme induction on the metabolism of disopyramide in man. Br J Clin Pharmacol 1981; 11: 279 – 285.
144. Kessler JM, Keys PW, Stafford RW. Disopyramide and phenytoin interaction. Clin Pharm 1982; 1: 263 – 264.
145. Ragosta M, Weihl AC, Rosenfeld LE. Potentially fatal interac-tion between erythromycin and disopyramide. Am J Med 1989; 86: 465 – 466.

Circulation Journal Vol.81, April 2017
609JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
146. Iida H, Morita T, Suzuki E, et al. Hypoglycemia induced by interaction between clarithromycin and disopyramide. Jpn Heart J 1999; 40: 91 – 96.
147. Michalets EL. Update: Clinically significant cytochrome P-450 drug interactions. Pharmacotherapy 1998; 18: 84 – 112.
148. Pentikäinen PJ, Koivula IH, Hiltunen HA. Effect of rifampicin treatment on the kinetics of mexiletine. Eur J Clin Pharmacol 1982; 23: 261 – 266.
149. Begg EJ, Chinwah PM, Webb C, et al. Enhanced metabolism of mexiletine after phenytoin administration. Br J Clin Pharmacol 1982; 14: 219 – 223.
150. Southworth W, Friday KJ, Ruffy R. Possible amiodarone-aprindine interaction. Am Heart J 1982; 104: 323.
151. Hashimoto Y, Kuroda T, Konishi M, et al. The effects of verapamil on the gastrointestinal metabolism of aprindine. Jpn J Clin Pharmacol Ther 1995; 30: 571 – 580.
152. Kuroda T, Hashimoto Y, Konishi M, et al. Interaction between diltiazem and antiarrhythmic drugs: Aprindine and mexiletine. Jpn J Clin Pharmacol Ther 1994; 25: 569 – 575 (in Japanese).
153. Tsuruoka S, Ioka T, Wakaumi M, et al. Severe arrhythmia as a result of the interaction of cetirizine and pilsicainide in a patient with renal insufficiency: First case presentation showing compe-tition for excretion via renal multidrug resistance protein 1 and organic cation transporter 2. Clin Pharmacol Ther 2006; 79: 389 – 396.
154. Tjandra-Maga TB, van Hecken A, van Melle P, et al. Altered pharmacokinetics of oral flecainide by cimetidine. Br J Clin Pharmacol 1986; 22: 108 – 110.
155. Funck-Brentano C, Becquemont L, Kroemer HK, et al. Variable disposition kinetics and electrocardiographic effects of flecainide during repeated dosing in humans: Contribution of genetic factors, dose-dependent clearance, and interaction with amio-darone. Clin Pharmacol Ther 1994; 55: 256 – 269.
156. Windle J, Prystowsky EN, Miles WM, et al. Pharmacokinetic and electrophysiologic interactions of amiodarone and procain-amide. Clin Pharmacol Ther 1987; 41: 603 – 610.
157. Saal AK, Werner JA, Greene HL, et al. Effect of amiodarone on serum quinidine and procainamide levels. Am J Cardiol 1984; 53: 1264 – 1267.
158. Kosoglou T, Rocci ML Jr, Vlasses PH. Trimethoprim alters the disposition of procainamide and N-acetylprocainamide. Clin Pharmacol Ther 1988; 44: 467 – 477.
159. Vlasses PH, Kosoglou T, Chase SL, et al. Trimethoprim inhibi-tion of the renal clearance of procainamide and N-acetylpro-cainamide. Arch Intern Med 1989; 149: 1350 – 1353.
160. Martin DE, Shen J, Griener J, et al. Effects of ofloxacin on the pharmacokinetics and pharmacodynamics of procainamide. J Clin Pharmacol 1996; 36: 85 – 91.
161. Bauer LA, Black DJ, Lill JS, et al. Levofloxacin and ciprofloxacin decrease procainamide and N-acetylprocainamide renal clear-ances. Antimicrob Agents Chemother 2005; 49: 1649 – 1651.
162. Christian CD Jr, Meredith CG, Speeg KV Jr. Cimetidine inhibits renal procainamide clearance. Clin Pharmacol Ther 1984; 36: 221 – 227.
163. Bauer LA, Black D, Gensler A. Procainamide-cimetidine drug interaction in elderly male patients. J Am Geriatr Soc 1990; 38: 467 – 469.
164. Rodvold KA, Paloucek FP, Jung D, et al. Interaction of steady-
state procainamide with H2-receptor antagonists cimetidine and ranitidine. Ther Drug Monit 1987; 9: 378 – 383.
165. Dilger K, Greiner B, Fromm MF, et al. Consequences of rifam-picin treatment on propafenone disposition in extensive and poor metabolizers of CYP2D6. Pharmacogenetics 1999; 9: 551 – 559.
166. Castel JM, Cappiello E, Leopaldi D, et al. Rifampicin lowers plasma concentrations of propafenone and its antiarrhythmic effect. Br J Clin Pharmacol 1990; 30: 155 – 156.
167. Libersa CC, Brique SA, Motte KB, et al. Dramatic inhibition of amiodarone metabolism induced by grapefruit juice. Br J Clin Pharmacol 2000; 49: 373 – 378.
168. Läer S, Neumann J, Scholz H. Interaction between sotalol and an antacid preparation. Br J Clin Pharmacol 1997; 43: 269 – 272.
169. Tartini R, Kappenberger L, Steinbrunn W, et al. Dangerous interaction between amiodarone and quinidine. Lancet 1982; 1: 1327 – 1329.
170. Marcus FI. Drug interactions with amiodarone. Am Heart J 1983; 106: 924 – 930.
171. McNulty RM, Lazor JA, Sketch M. Transient increase in plasma quinidine concentrations during ketoconazole-quinidine therapy. Clin Pharm 1989; 8: 222 – 225.
172. Spinler SA, Cheng JW, Kindwall KE, et al. Possible inhibition of hepatic metabolism of quinidine by erythromycin. Clin Pharmacol Ther 1995; 57: 89 – 94.
173. Data JL, Wilkinson GR, Nies AS. Interaction of quinidine with anticonvulsant drugs. N Engl J Med 1976; 294: 699 – 702.
174. Kaukonen KM, Olkkola KT, Neuvonen PJ. Itraconazole increases plasma concentrations of quinidine. Clin Pharmacol Ther 1997; 62: 510 – 517.
175. Urbano AM. Phenytoin-quinidine interactions in a patient with recurrent ventricular tachyarrhythmias. N Engl J Med 1983; 308: 225.
176. Chapron DJ, Mumford D, Pitegoff GI. Apparent quinidine-induced digoxin toxicity after withdrawal of pentobarbital: A case of sequential drug interactions. Arch Intern Med 1979; 139: 363 – 365.
177. Rodgers GC, Blackman MS. Quinidine interaction with anti-convulsants. Drug Intell Clin Pharm 1983; 17: 819 – 820.
178. Twum-Barima Y, Carruthers SG. Quinidine-rifampin interac-tion. N Engl J Med 1981; 304: 1466 – 1469.
179. Bussey HI, Merritt GJ, Hill EG. The influence of rifampin on quinidine and digoxin. Arch Intern Med 1984; 144: 1021 – 1023.
180. Schwartz A, Brown JR. Quinidine-rifampin interaction. Am Heart J 1984; 107: 789 – 790.
181. Andreasen AH, Brøsen K, Damkier P. A comparative pharma-cokinetic study in healthy volunteers of the effect of carbam-azepine and oxcarbazepine on CYP3A4. Epilepsia 2007; 48: 490 – 496.
182. Hardy BG, Schentag JJ. Lack of effect of cimetidine on the metabolism of quinidine: Effect on renal clearance. Int J Clin Pharmacol Ther Toxicol 1988; 26: 388 – 391.
183. Hardy BG, Zador IT, Golden L, et al. Effect of cimetidine on the pharmacokinetics and pharmacodynamics of quinidine. Am J Cardiol 1983; 52: 172 – 175.
184. Damkier P, Hansen LL, Brøsen K. Effect of fluvoxamine on the pharmacokinetics of quinidine. Eur J Clin Pharmacol 1999; 55: 451 – 456.
Appendix 1Chair: •KazutakaAonuma,CardiovascularDivision,FacultyofMedicine,
University of Tsukuba (JCS) •Tsuyoshi Shiga, Department of Cardiology, Tokyo Women’s
Medical University (JSTDM)
Member: •Hirotsugu Atarashi, NipponMedical School Tama Nagayama
Hospital •KosukeDoki,DepartmentofPharmaceuticalSciences,Facultyof
Medicine, University of Tsukuba •Hirotoshi Echizen, Department of Pharmacotherapy, Meiji
Pharmaceutical University •NobuhisaHagiwara,DepartmentofCardiology,TokyoWomen’s
Medical University •JunichiHasegawa,DivisionofPharmacotherapeutics,Department
of Pathophysiological and Therapeutic Science, Faculty of Medicine, Tottori University
•Hideharu Hayashi, Department of Internal Medicine III,Hamamatsu University School of Medicine
•KenzoHirao,HeartRhythmCenter,TokyoMedicalandDentalUniversity
•FukikoIchida,ToyamaUniversityGraduateSchoolofMedicineand Pharmaceutical Science
•Takanori Ikeda, Division of Cardiovascular Medicine, TohoUniversity Faculty of Medicine
•Yorinobu Maeda, Department of Pharmacy, Chugoku RosaiHospital
•NaokiMatsumoto,DepartmentofPharmacology,St.MariannaUniversity School of Medicine
•Toshiyuki Sakaeda, Department of Pharmacokinetics, KyotoPharmaceutical University
•WataruShimizu,DepartmentofCardiovascularMedicine,NipponMedical School
•MitsuruSugawara,LaboratoryofPharmacokinetics,FacultyofPharmaceutical Sciences, Hokkaido University

Circulation Journal Vol.81, April 2017
610 AONUMA K et al.
•KyoichiTotsuka,KitatamaHospital •YoshimasaTsuchishita,DepartmentofPharmacy,MaizuruKyosai
Hospital •KazuyukiUeno,DepartmentofPharmaceuticalSciences,Niigata
University of Pharmacy and Applied Life Sciences •Eiichi Watanabe, Department of Cardiology, Fujita Health
University School of Medicine
Collaborators: •MasayukiHashiguchi, Division for Evaluation andAnalysis of
Drug Information, Faculty of Pharmacy, Keio University •SumioHirata,DepartmentofClinicalPharmacology,Kumamoto
University School of Pharmacy •HidefumiKasai,CertaraG.K. •YoshiakiMatsumoto,DepartmentofClinicalPharmacokinetics,
School of Pharmacy, Nihon University •AkihikoNogami,CardiovascularDivision,FacultyofMedicine,
University of Tsukuba •YukioSekiguchi,CardiovascularDivision,FacultyofMedicine,
University of Tsukuba •TokukoShinohara,DepartmentofPediatricCardiology,Tokyo
Women’s Medical University •Atsushi Sugiyama, Department of Pharmacology, Faculty of
Medicine, Toho University
•NaokataSumitomo,DepartmentofPediatricCardiology,SaitamaMedical University International Medical Center
•Atsushi Suzuki, Department of Cardiology, Tokyo Women’sMedical University
•Naohiko Takahashi, Department of Cardiology and ClinicalExamination, Faculty of Medicine, Oita University
•EijiYukawa,ChemistandPharmacist
Independent Assessment Committee: •MasatoHomma,DepartmentofPharmaceuticalSciences,Faculty
of Medicine, University of Tsukuba •Minoru Horie, Department of Cardiovascular and Respiratory
Medicine, Shiga University of Medical Science •HiroshiInoue,SaiseikaiToyamaHospital •HiroshiIto,DivisionofCardiovascularandRespiratoryMedicine,
Akita University Graduate School of Medicine •Takanori Miura, Center for Education and Clinical Research
Training, Anjo Kosei Hospital •TohruOhe,TheSakakibaraHeartInstituteofOkayama •Kimikazu Shinozaki, Department of Clinical Pharmacy and
Pharmacokinetics, Center for Clinical Pharmacy and Sciences, Kitasato University School of Pharmacy
•KazuhikoTanaka,KidneyCenter,ShirasagiHospital(The affiliations of the members are as of September 2015)
Appendix 2 Disclosure of Potential Conflicts of Interest (COI): Guidelines for Therapeutic Drug Monitoring of Cardiovascular Drugs
Author
Employer/leadership position (private
company)
Stake-holder
Patent royalty Honorarium
Payment for
manuscriptsResearch
grant
Scholarship (educational)
grant/endowed chair
Other rewards
Potential COI of the marital partner, first-degree family members, or
those who share income and property
Chair: Kazutaka Aonuma
MSDActelion
Pharmaceuticals JapanAstecAstellas PharmaOtsuka PharmaceuticalSt. Jude MedicalDaiichi SankyoTakeda PharmaceuticalMitsubishi Tanabe
PharmaTeijin PharmaDVxNippon Boehringer
IngelheimBayer YakuhinBristol-MyersBoston Scientific JapanTsukuba Memorial
HospitalChair: Tsuyoshi Shiga
Daiichi SankyoBristol-MyersToa Eiyo
Terumo EisaiDaiichi Sankyo
Member: Hirotsugu Atarashi
Daiichi SankyoBristol-Myers
Member: Takanori Ikeda
Mitsubishi Tanabe Pharma
Daiichi SankyoOno
PharmaceuticalBayer YakuhinBristol-MyersPfizer
Daiichi SankyoBristol-MyersMitsubishi Tanabe
PharmaNippon Boehringer
Ingelheim
Member: Hirotoshi Echizen
Kaken Pharmaceutical
Member: Toshiyuki Sakaeda
Taisho Toyama Pharmaceutical
Towa Pharmaceutical
(Appendix 2 continued the next page.)

Circulation Journal Vol.81, April 2017
611JCS/JSTDM Guidelines for Blood Concentration Monitoring of CV Therapeutic Drugs
Author
Employer/leadership position (private
company)
Stake-holder
Patent royalty Honorarium
Payment for
manuscriptsResearch
grant
Scholarship (educational)
grant/endowed chair
Other rewards
Potential COI of the marital partner, first-degree family members, or
those who share income and property
Member: Wataru Shimizu
SuzukenDia
Medical Net
Daiichi SankyoNippon
Boehringer Ingelheim
Bristol-MyersPfizerBayer YakuhinMitsubishi Tanabe
PharmaOno
Pharmaceutical
NTT Daiichi SankyoNippon Boehringer
IngelheimBayer YakuhinMSDOno PharmaceuticalOtsuka PharmaceuticalAstraZenecaMitsubishi Tanabe
PharmaEisai
Member: Kyoichi Totsuka
Toyama Chemical
Member: Nobuhisa Hagiwara
Nippon Boehringer Ingelheim
Bristol-Myers
Toa EiyoAstellas PharmaNippon Boehringer
IngelheimShionogiEisaiMitsubishi Tanabe
PharmaTakeda PharmaceuticalOtsuka PharmaceuticalDaiichi Sankyo
Member: Hideharu Hayashi
Genzyme JapanDaiichi Sankyo
Member: Kenzo Hirao
Bayer Yakuhin Bristol-Myers Daiichi Sankyo
Member: Naoki Matsumoto
Daiichi SankyoBayer Yakuhin
PfizerBristol-Myers
Member: Eiichi Watanabe
Biotronik Japan
Nippnon Boehringer Ingelheim
Pfizer
Takeda PharmaceuticalJapan LifelineMedtronic JapanBoston Scientific JapanBiotronik JapanSt. Jude MedicalDaiichi SankyoNippon Boehringer
IngelheimCollaborator: Atsushi Sugiyama
Otsuka Pharmaceutical
Fuji Micra
Collaborator: Yukio Sekiguchi
DVx St. Jude Medical
Collaborator: Naohiko Takahashi
Bristol-MyersPfizerMedtronic JapanBayer YakuhinDaiichi SankyoNippon Boeh-
ringer IngelheimMitsubishi Tanabe
PharmaTakeda Pharma-
ceutical
Takeda PharmaceuticalSumitomo Dainippon
PharmaDaiichi SankyoNippon Boehringer
IngelheimBayer YakuhinAstellas PharmaMitsubishi Tanabe
Pharma
Collaborator: Akihiko Nogami
Medtronic JapanSt. Jude Medical
Johnson & JohnsonMedtronic Japan
Collaborator: Yoshiaki Matsumoto
Chugai Pharmaceutical
(Appendix 2 continued the next page.)

Circulation Journal Vol.81, April 2017
612 AONUMA K et al.
Companies are listed only by name. No relevant COIs were declared by other members or collaborators.The following members and collaborators have no relevant COIs.Member: Fukiko Ichida, noneMember: Kazuyuki Ueno, noneMember: Mitsuru Sugawara, noneMember: Yoshimasa Tsuchishita, noneMember: Kosuke Doki, noneMember: Junichi Hasegawa, noneMember: Yorinobu Maeda, noneCollaborator: Hidefumi Kasai, noneCollaborator: Tokuko Shinohara, noneCollaborator: Atsushi Suzuki, noneCollaborator: Naokata Sumitomo, noneCollaborator: Masayuki Hashiguchi, noneCollaborator: Sumio Hirata, noneCollaborator: Eiji Yukawa, none