GUIDELINES FOR THE MANAGEMENT OF DYSPEPSIA AND GASTROESOPHAGEAL REFLUX …€¦ · suggesting...
16
PREFACE Acid peptic disorders have been with mankind for centuries but till date there exist numerous gaps in knowledge and controversies in the understanding of these conditions. Dyspepsia and gastroesophageal reflux disease (GERD) are the key acid-peptic disorders and account for over half of cases seen in gastroenterology practice. In her bid to provide the necessary leadership in the management of diseases of the gastrointestinal system in Nigeria, Society for Gastroenterology and Hepatology in Nigeria (SOGHIN) appointed a committee of 3 members and charged it with the responsibility of drawing up guidelines for the management of dyspepsia and GERD. The committee members promptly took up the challenge and approached the task by doing extensive literature search and critical review of identified articles. Similar guidelines published by other national professional societies were reviewed. The task was concluded with two meetings where the members had a very robust debate on the recommendations before coming up with this document. The peculiarities of our setting regarding culture, available resources and technology have been taken into consideration in making the recommendations. This guideline is the first of its kind in SOGHIN and indeed Nigeria. It is expected to serve as a guidance to doctors (non-gastroenterologists and gastroenterologists) in the evaluation and treatment of patients who present with dyspepsia and GERD. The recommendations should not be construed as establishing a legal standard of care or as encouraging any particular treatment. It is intended to indicate preferred approaches to dyspepsia and GERD as established by scientifically valid research and would be revised as necessary to accommodate the rapid improvements in knowledge. The committee members are immensely grateful to the Executive Council and all members of SOGHIN for the opportunity to serve. INTRODUCTION Dyspepsia is a clinical syndrome which comprises a series of symptoms that originate from the gastroduodenal region of the gastrointestinal tract. The symptoms may be episodic, recurrent or chronic and are often associated with eating, but this is not always the case. It classically presents as pain in the upper abdomen which is usually described as a burning sensation, heaviness or an ache. Other symptoms include a feeling of fullness, easy satiety after meals, anorexia, bloating, belching, nausea and vomiting. GUIDELINES FOR THE MANAGEMENT OF DYSPEPSIA AND GASTROESOPHAGEAL REFLUX DISEASE (GERD) GUIDELINES COMMITTEE Nwokediuku S 1 , Omuemu C 2 and Akere A 3 1 University of Nigeria Teaching Hospital, Enugu, Nigeria. 2 University of Benin Teaching Hospital, Benin City, Nigeria. 3 University College Hospital, Ibadan, Nigeria. Nigerian Journal of Gastroenterology and Hepatology Vol. 7, No.2 December, 2015 93-108 93
Transcript of GUIDELINES FOR THE MANAGEMENT OF DYSPEPSIA AND GASTROESOPHAGEAL REFLUX …€¦ · suggesting...

PREFACEAcid peptic disorders have been with mankindfor centuries but till date there exist numerousgaps in knowledge and controversies in theunderstanding of these conditions. Dyspepsia andgastroesophageal reflux disease (GERD) are thekey acid-peptic disorders and account for overhalf of cases seen in gastroenterology practice.
In her bid to provide the necessary leadership inthe management of diseases of thegastrointestinal system in Nigeria, Society forGastroenterology and Hepatology in Nigeria(SOGHIN) appointed a committee of 3 membersand charged it with the responsibility of drawingup guidelines for the management of dyspepsiaand GERD.
The committee members promptly took up thechallenge and approached the task by doingextensive literature search and critical review ofidentified articles. Similar guidelines published byother national professional societies werereviewed. The task was concluded with twomeetings where the members had a very robustdebate on the recommendations before comingup with this document. The peculiarities of oursetting regarding culture, available resources andtechnology have been taken into considerationin making the recommendations.
This guideline is the first of its kind in SOGHINand indeed Nigeria. It is expected to serve as aguidance to doctors (non-gastroenterologists andgastroenterologists) in the evaluation andtreatment of patients who present with dyspepsiaand GERD. The recommendations should not beconstrued as establishing a legal standard of careor as encouraging any particular treatment. It isintended to indicate preferred approaches todyspepsia and GERD as established byscientifically valid research and would be revisedas necessary to accommodate the rapidimprovements in knowledge.
The committee members are immensely gratefulto the Executive Council and all members ofSOGHIN for the opportunity to serve.
INTRODUCTIONDyspepsia is a clinical syndrome which comprises aseries of symptoms that originate from thegastroduodenal region of the gastrointestinal tract. Thesymptoms may be episodic, recurrent or chronic andare often associated with eating, but this is not alwaysthe case. It classically presents as pain in the upperabdomen which is usually described as a burningsensation, heaviness or an ache. Other symptomsinclude a feeling of fullness, easy satiety after meals,anorexia, bloating, belching, nausea and vomiting.
GUIDELINES FOR THE MANAGEMENT OFDYSPEPSIA AND GASTROESOPHAGEAL REFLUX
DISEASE (GERD)
GUIDELINES COMMITTEENwokediuku S1, Omuemu C2 and Akere A3
1 University of Nigeria Teaching Hospital, Enugu, Nigeria.2University of Benin Teaching Hospital, Benin City, Nigeria.
3University College Hospital, Ibadan, Nigeria.
Nigerian Journal of Gastroenterology and Hepatology Vol. 7, No.2 December, 2015 93-108
93

Gastroesophageal reflux disease (GERD) is also adisorder of the upper gastrointestinal tract. It resultswhen reflux of gastric contents across thegastroesophageal junction into the esophagus, pharynxor mouth leads to troublesome symptoms and/orcomplications. Its cardinal symptoms are heartburn andregurgitation. Sometimes the symptoms of dyspepsiaoverlap with those of GERD.
The nomenclature for dyspepsia is confusing. This islargely because some medical organizations include allupper gastrointestinal (UGI) symptoms in the termdyspepsia, then separate patients with symptomssuggesting gastro-esophageal reflux disease (GERD)for appropriate management, whereas othersrecognize the overlap in symptoms between the variouscauses of UGI symptoms but choose to separate thesymptoms suggesting GERD before applying the termdyspepsia. Both approaches recommend identifyingpatients whose symptoms suggest GERD andmanaging them as having reflux disease.However,emerging data suggest that excluding all patients withany heartburn or regurgitation from the diagnosis ofdyspepsia is over-simplistic and potentially misleading.Consequently, some experts are proposing the term“dyspepsia complex” to accommodate patients withdyspeptic and reflux symptoms particularly theirfunctional variants (functional dyspepsia and functionalheartburn). These experts are of the view that bothconditions may be part of one disease complex1Inthe Rome III criteria, patients presenting withsymptoms suggestive of GERD are isolated beforeapplying the term dyspepsia and this guideline is builton that format.
Dyspepsia is one of the most common disorders inmedicine, with affected patients seen on daily basisnot only by gastroenterologists, but also by physiciansin a variety of other fields. Most affected people donot seek medical care. Although the disorder does notaffect survival, it is responsible for substantial healthcare costs and significantly affects quality of life2-5.
Nigeria belongs to the group of poorer countries ofthe world where medical care is grossly inadequatewith high rates of infant mortalityand malnutrition,low life expectancy and high mortality from infectiousdiseases like malaria, tuberculosis and HIV/AIDS. Theprecarious nature of health care underscores the need
for a guideline for the management of this commongastrointestinal problem. This would ensure that limitedresources are neither overused, underused, nor misused.
This guideline is intended to be an educational deviceto provide information that may assist practitioners inproviding care to patients with dyspepsia. It is not arule and should not be construed as establishing a legalstandard of care or as encouraging any particulartreatment. It is intended to indicate preferredapproaches to medical problems as established byscientifically valid research. Clinical decisions in anyparticular case involves a complex analysis of thepatient’s condition and available courses of action.Therefore, clinical considerations may lead a physicianto take a course of action that varies from this guideline.This guideline may be revised as necessary toaccommodate improvements in knowledge,emergence of new data or other aspects of clinicalpractice.
Rationale for Guideline(1.) Provision of a relevant guide to the diagnosis
and management of dyspepsia and GERDfor primary care physicians andgastroenterologists.
(2.) Articulation of the experience and views ofNigerian experts on dyspepsia and GERD
(3.) Adaptation of global best practices in themanagement of dyspepsia and GERD toNigeria’s peculiar socio-economiccircumstances
(4.) Standardization of research among differentpractitioners in Nigeria
(5.) Facilitation of training and supervision ofhealth care providers
(6.) Judicious use of scarce resources for healthcare
(7.) Identification of areas that need furtherresearch.
DYSPEPSIADefinition:According to the Rome III criteria, dyspepsia is definedas one or more of the following symptoms(6)• Postprandial fullness• Early satiation• Epigastric pain• Epigastric burning
94
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

Postprandial fullnessis a feeling of prolongedpersistence of food in the stomach. Early satiation is afeeling that the stomach is overfilled soon after startingto eat, out of proportion to the size of the meal beingeaten, so that the meal cannot be finished. Epigastricpain refers to a subjective unpleasant sensation.Epigastric burning refers to an unpleasant sensationof heat.
Postprandial fullness and early satiation are meal relatedsymptoms and they described as postprandial distresssyndrome (PDS)while epigastric pain and epigastricburning are not necessarily meal related and theyconstitute epigastric pain syndrome(EPS).
Other symptoms commonly complained about bydyspeptic patients include bloating in the upperabdomen, nausea, vomiting and belching7.
Heartburn and/or regurgitation are excluded fromdiagnostic symptom criteria for dyspepsia since theyare suggestive of GERD. However, there is a highdegree of overlap between GERD and dyspepsia1.When such overlap occurs , the symptomaticclassification of the patient would be determined bythe predominant symptom.
UNINVESTIGATED DYSPEPSIAThis is a form of dyspepsia that has not been recentlyinvestigated by upper gastrointestinal endoscopy. Thisinvestigation is the standard requirement internationallyfor classifying dyspepsia into organic or functional.
1. For Nigerian patients with dyspepsia, stoolmicroscopy and culture, and abdominalultrasonography should be included becauseintestinal parasites and liver disease are relativelycommon.
Functional DyspepsiaAccording to Rome III criteria6, functional dyspepsia(FD) is defined as presence of at least one of thefollowing:
• Postprandial fullness• Early satiation• Epigastric pain• Epigastric burning
AND no evidence of structural disease that is likely toexplain the symptoms.
Note: Criteria must be fulfilled for the past three months,with symptom onset at least six months before diagnosis.
Functional dyspepsia accounts for over 60% ofdyspepsia in most parts of the world, including Nigeria8-11.
2. Functional dyspepsia can be diagnosed in apatient with dyspepsia if upper gastrointestinalendoscopy, stool examination and abdominalultrasonography fail to reveal a potential causefor the dyspepsia.
Organic Dyspepsia3. This is defined as dyspepsia which has been
investigated and a structural, systemic orbiochemical cause for the symptom revealed.The investigation should include uppergastrointestinal endoscopy, stool microscopy/culture and abdominal ultrasonography.
Causes of Organic Dyspepsia• Peptic ulcer disease• Reflux esophagitis• Gastric or esophageal cancer• Pancreatic cancer• Drugs• Gastroparesis• Hepatoma• Intestinal parasites (Giardia, Strongyloides• Infiltrative diseases of stomach (Crohn’sdisease, Sarcoidosis)• Metabolic disturbances (hypercalcemia,hyperkalemia)• Pancreatitis• Systemic disorders (Diabetes mellitus, thyroidand parathyroid diseases)
Drugs that Commonly Cause Dyspepsia• Non steroidal anti-inflammatory drugs• Cox-2 inhibitors• Bisphosphonates• Erythromycin• Tetracyclines• Iron• Potassium supplements
95
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

• Acarbose• Digitalis• Theophylline• Orlistat• Corticosteroids
EpidemiologyThe prevalence of dyspepsia varies considerablybetween different populations, either due to genuineepidemiological differences or varying definitions usedin different population studies. The rapid introductionof new diagnostic criteria for dyspepsia has made verydifficult or virtually impossible to compare prevalencerates from different periods or geographical regions12.
In studies using “upper abdominal pain” as thedefinition, the prevalence of uninvestigated dyspepsiahas varied between 7%-34.2%13-21. When a broaderdefinition of “upper abdominal symptoms” is usedto define dyspepsia, a 23%-45% prevalence isobserved22-29. A study in Nigeria carried out in 1996with this definition reported a prevalence of 45%29.
Globally, functional dyspepsia accounts for over 60%of patients with dyspepsia 1,11,30. There is a high degreeof overlap between FD and other functionalgastrointestinal disorders, namely functional heartburnand irritable bowel syndrome11,31-33.
Pathophysiology of Functional DyspepsiaFunctional is a very heterogeneous entity with multi -factorial pathophysiology. Putative mechanisms includealtered sensory and motor functions , hypersensitivityto mechanical gastric stimulation, impaired acidclearance and enhanced sensitivity, and visceralhypersensitivity. Other mechanisms includeHelicobacter pylori infection, low- grade inflammation,and genetic susceptibility 34-40.
MANAGEMENT4. A detailed history and thorough physical
examination are the first step in the evaluationof patients with dyspepsia.
History• Age of the patient is major determinant of the
management approach. Patients who are over 40years of age should undergo early endoscopy
• Patients with one or more “alarm features” shouldalso undergo early endoscopy. Alarm features arefeatures that raise a suspicion of malignantdisease(table).
Table: Alarm Features41
Unintended weight lossProgressive dysphagiaOdynophagiaPersistent vomitingAnorexiaAnaemiaFamily history of gastrointestinalmalignancyJaundice
Palpable Mass or Lymphadenopathy5. A dominant history of heartburn,
regurgitation or cough is suggestive ofGERD.
6. Non steroidal anti -inflammatory drug(NSAID) use raises the possibility of NSAID-induced dyspepsia or peptic ulcer disease. A number of other drugs can cause dyspepsia(Table 1)
7. Pain radiation to the back is suggestive of apancreatic lesion
8. Epigastric or right upper quadrant pain thatis severe, episodic and lasting more than 1 houris suggestive of cholelithiasis.
Physical ExaminationPhysical examination may be normal except forepigastric tenderness.
9. General examination should be conducted insearch of anaemia, lymphadenopathy, massesand other alarm features.
96
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

Guidelines for the Management of GERD
Esophageal Syndrom
es
Symptom
atic
Syndromes
Typical reflux syndrom
es(H
eartburn and
Regurgitation)
Reflux Chest Pain
Syndromes w
ithesophageal injury
Reflux esophagitis
Reflux stricture
Barrett’s esophagus
A
denocarcinoma
Established Association
Reflux cough
Reflux Laryngitis
Reflux A
sthma
Reflux dental erosions
Extra-esophageal
Syndromes
complications
Montreal D
efinition and Classification
GE
RD is a condition w
hich develops when the reflux of stom
ach contents causestroublesom
e symptom
s and/or
Proposed association
Sinusitis
Pulm
onary fibrosis
Pharyngitis
Recurrent otitis media
From: Vakil N
et al. Am J G
astroenterol 2006; 101: 1900 - 20
97Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015

10. Carnett sign should be elicited in all cases toexclude abdominal wall pain. This is done bytensing the muscles of anterior abdominalwall and demonstrating local tenderness(positive Carnett test)
Initial Laboratory Evaluation11. All dyspeptic patients should have the
following initial basic tests• Stool microscopy and culture• Abdominal ultrasonography
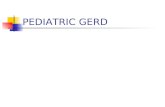
Further management would be determined by threefactors: age of patient, presence of alarm feature(s)and local prevalence of Helicobacter pylori infection.
12. Patients with a presumptive diagnosis ofGERD should receive PPI for 8 weeks
13. Patients on NSAID should discontinue andtake PPI for 8 weeks
14. Patients with alarm features or aged over 40yearsshould have early endoscopy andtreatment instituted as appropriate. Biopsy forHelicobacter pylori should be obtained anderadication therapy given to positive cases.
15. Patients without alarm features and ared”40years should be tested for H. pylori using ureabreath test or stool antigen test and positivecases subjected to eradication therapy(test and treat) because of the high prevalenceof H. pylori in Nigeria.
16. Those who continue to have symptoms aftereradication therapy should be treated with PPIfor 8 weeks.
17. Those who remain symptomatic after thiswould require endoscopy.
18. Patients whosesymptoms have lasted for over1 year without investigation may be offeredearly endoscopy.
There is evidence to show that there is improved patientsatisfaction and confidence following this line ofaction42.
Patients with Persistent SymptomsPatients who fail to respond to above strategy wouldneed the following additional actions:
19. Reassessment for type and severity ofpersisting symptoms
20. Adequacy of medication dosage andcompliance to treatment
21. Upper endoscopy, biopsy and testing for H.pylori. Histology should be used for thetesting if patient had not previously beentested and culture used if previously tested.Duodenal biopsy may also be done ifmalabsorbtion and anaemia are part ofpatient’s presentation.
22. Gastric emptying studies to rule outgastroparesis in patients with persistent nauseaand vomiting especially at risk patients likethose with diabetes mellitus.
23. Associated large bowel symptoms likediarrhea, constipation and flatulence areindications for colonoscopy.
24. Absence of any organic lesion supports adiagnosis of FD.
Treatment of Functional Dyspepsia (FD)25. General measures such as smaller, more
frequent meals, avoiding caffeine, alcohol,NSAIDs, fatty or spicy foods are usuallyemployed though there is little evidencesupporting their use(43). Patients should beencouraged to adopt these measures if theyexperience benefit from them.
26. Patients who have EPS- predominant FDshould be given PPI initially, followed ifnecessary by prokinetic agents.
27. Patients who have PDS-predominant FDshould receive prokinetic agents, followed ifnecessary by PPI.
28. Where there is a clear overlap of PDS andEPS, PPI and prokinetic drugs may becombined initially.
29. Patients who fail to respond to the steps statedabove should receive antidepressants oranxiolytics.
30. If symptoms persist, refer patient to agastroenterologist.
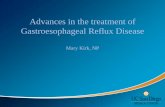
Gastroesophageal Reflux DiseaseGastroesophageal reflux disease (GERD) developswhen the reflux of gastric contents into the esophagusleads troublesome symptoms and/or complications1.Symptoms become troublesome when they adverselyaffect an individual’s wellbeing. Based on this definitionGERD can be classified into 2 syndromes(Figure 1).
98
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

99
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD
Fig 1: Algorithm
for managem
ent of univestigated dyspepsia

This definition is convenient for resource-poor settingsbecause it is patient-centred and symptom-driven, andallows the disease to be diagnosed in primary care onthe basis of symptoms alone, without additionaldeployment of scarce resources in investigations.
Heartburn and regurgitation are the characteristicsymptoms of GERD.
Heartburn is a burning sensation in the retrosternalarea. Regurgitation is the perception of flow ofrefluxed gastric content into the mouth orhypopharynx. Other features of GERD include chestpain, cough, voice changes, repeated need to clearthroat, asthmatic attacks, recurrent otitis media,abdominal pain and sleep disturbance.
EpidemiologyGastroesophageal reflux disease is the most commonupper gastrointestinal disease in the Western world,with 10-20% of the population experiencing weeklysymptoms2-4. Lower prevalence has been reported inAsia5,6. There are no population-based studies in Africaand indeed Nigeria. A questionnaire-based study ofmedical students in Nigeria showed a prevalence of26.3%7.
Risk factors for GERD include race8, sex9-11, age9-11,obesity12-14, alcohol consumption and hiatus hernia9,15,16,cigarette smoking17, and consumption of coffee andcola7. Other risk factors include connective tissuedisease18 and chronic obstructive airway disease19.Caucasians have higher risk of esophagitis and Barret’sesophagus. Males have higher risk of esophagitis andBarret’s esophagus. These complications also tend toincrease with increasing age. Pregnancy is a risk factorfor GERD. The prevalence of GERD is increasingglobally probably due to aging population, the obesityepidemic and associated changes in diet, physical activityand changes in sleep pattern20,21.
Drugs that may predispose to GERD includeanticholinergics, benzodiazepines, calcium channelblockers, dopamine, nicotine, nitrates, theophylline,estrogen, progesterone, glucagon and someprostaglandins.
PathophysiologyThe esophagus, lower esophageal sphincter (LES) andstomach can be likened to a simple plumbing circuit22.The esophagus functions as an anterograde pump, theLES as a valve, and the stomach as a reservoir. Theabnormalities that contribute to GERD can stem fromany component of the circuit. A dysfunctional LESallows reflux of large amounts of gastric juice. Delayedgastric emptying can increase volume and pressure inthe reservoir until the valve mechanism is overwhelmed,leading to GERD. Esophageal defense mechanismsinclude esophageal clearance and mucosal resistance.Esophageal clearance has a mechanical arm (esophagealperistalsis) and a chemical component(saliva) both ofwhich limit the amount of time the esophagus isexposed to refluxed gastric juice.
The three dominant pathophysiological mechanismscausing gastroesophageal junction incompetence are:transient lower esophageal sphincter relaxations(tLESRs), a hypotensive LES and anatomic disruptionof the gastroesophageal junction, often associated witha hiatal hernia. The dominant mechanism varies as afunction of disease severity with tLESR predominatingwith mild disease and mechanisms associated with LESdysfunction and hiatal hernia predominating with moresevere disease 23.
ClassificationNon erosive reflux disease (NERD): This is defined bypresence of troublesome reflux-associated symptomsand the absence of mucosal breaks at endoscopy. Thistype of GERD accounts for 60-70% of cases.
Erosive ref lux disease (ERD): This is def inedendoscopically by visible breaks of the distalesophageal mucosa.
Generally, symptom frequency and/or severity do notaccurately predict what the endoscopic findings wouldbe in an individual patient24-29. Patients with uppergastrointestinal symptoms , unrelated to reflux ofgastric contents are excluded from GERD.
Non erosive reflux disease is the more heterogeneoustype of GERD. Impedance-pH technology has helpedin defining the subgroups of NERD. All the subgroupshave negative upper endoscopy.
100
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

101
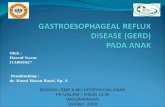
Fig.2: Algorithm
for managem
ent of functional dyspepsia
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

True NERD is characterized by abnormal esophagealacid exposure at impedance-pH monitoring.
Acid hypersensitive esophagus is characterized by normalesophageal acid exposure and positive symptomassociation to acid reflux at impedance-pH monitoring.
Nonacid hypersensitive esophagus is characterized by normalesophageal acid exposure and positive symptomassociation to non- acid reflux at impedance-pHmonitoring.
Functional heartburn is not part of NERD spectrum asthere is no underlying reflux of gastric contents. Thereis normal esophageal acid exposure, negative symptomassociation to any type of reflux at impedance-pHmonitoring and non-response to PPI.
Previously, patients with non-acid reflux were groupedunder functional heartburn if they failed to respondto PPI (Rome III). Impedance-pH technology hasmade it possible to isolate the non-acid hypersensitiveesophagus group which clearly falls under NERDbecause they exhibit positive symptom association toreflux, even though PPIs do not lead to ameliorationof the symptoms.
DiagnosisThere is no gold standard for the diagnosis of GERD.Modalities available to the clinician include history,radiology, upper gastrointestinal endoscopy, histology,PPI test and ambulatory pH monitoring (with orwithout impedance). An objective diagnostic tool withacceptable sensitivity and specificity remain an unmetneed for clinicians and researchers.
Heartburn and regurgitation are characteristicsymptoms of the typical reflux syndrome5.
1. In the absence of alarm features, the typicalreflux syndrome can be diagnosed on thebasis of characteristic symptomsaloneThis is consistent with the Montreal consensusand suites resource-limited settings1.
Alarm SymptomsThese are symptoms which raise a strong suspicionof malignant disease or complication. They include:
• Vomiting
• Gastrointestinal bleeding• Anemia• Abdominal mass• Unexplained weight loss• Progressive dysphagia
2. Radiology as a diagnostic tool is discouragedbecause of low sensitivity and specificity. It isuseless in the diagnosis of NERD.
3. Endoscopy has a high specificity. However,majority of GERD patients are actuallyendoscopy-negative (NERD).
4. The Los Angeles classification should be usedin the endoscopic characterization of refluxesophagitis.This model has gained genuine acceptanceover the last 20 years30-32.
5. Routinebiopsies from the distal esophagus arenot recommended specifically to diagnoseGERD.
6. Screening for Helicobacter pylori is notrecommended in GERD
7. Ambulatory pH monitoring is the bestmethod of evaluating NERD patients whodo not respond to PPI.
8. Multi-channel intraluminal impedancemonitoring with pH sensor (MII-pH) candetect all types of reflux, (including acidic,weakly acidic, and weakly alkaline)
9. Manometry has no place in the diagnosis ofGERD. Its use is limited to exclusion ofmotility disorders of the esophagus and inthe preoperative assessment of candidates foranti-reflux surgery. It may also localize the LESfor subsequent pH monitoring.
TREATMENTGoals of Treatment:
• Relief of symptoms• Healing of esophagitis• Prevention of recurrence• Prevention of complications
Lifestyle Modification10. Weight loss is recommended for GERD
patients who are overweight or obese11. Nocturnal symptoms are an indication for
head of bed elevation
102
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

12. Foods like chocolate, caffeine, alcohol, acidicand/or spicy food may be avoided if theyprecipitate/worsen patient’s symptoms.
Drugs13. PPI for 8 weeks is the preferred treatment
for healing of esophagitis and relief ofsymptoms.
14. PPIs are equally effective in erosive esophagitisand NERD.
A functional test is used to isolate patients with acidreflux, non acid reflux and functional heartburn33.
15. Patients who do not respond to PPI in properdosage and adequate duration should bereferred for evaluation.
16. Maintenance treatment is recommended forpatients in whom symptoms resume upondiscontinuation of PPI.
17. Bedtime H2-receptor antagonist therapy canbe added to daytime PPI therapy in selectedpatients with objective evidence of night-timeif needed.
18. Antacids and alginates may be used forsymptomatic relief but not for healing ofesophagitis.
APPROACH TO PATIENTS WITH GERDPatients who present with typical symptoms of GERD(heartburn and/or regurgitation) with or withoutatypical symptoms should be evaluated for thepresence of alarm symptoms.
19. The presence of alarm symptoms qualifiesthem for prompt endoscopy.
20. Those who do not have alarm symptomsshould receive PPI.
21. Lack of response warrants a search for otheretiologies with upper gastrointestinalendoscopy (for patients with typicalsymptoms) or other investigations inappropriate specialties depending on the natureof the atypical symptoms.
22. If no abnormality is found, pH-impedancemonitoring would be indicate; but where thisfacility is not available, further managementwill be determined by the predominant
symptom (heartburn or regurgitation), usingpain modulators and inhibitors of transientlower esophageal sphincter relaxation(figure2)
SURGERY23. Surgery is a treatment option but should not
be encouraged in centers without adequatefacilities, personnel and requisite experience inthe standard procedures.
24. Patients who do not respond to PPI are notcandidates for surgery.
25. Patients with erosive esophagitis do not requirepreoperative pH- monitoring.
26. Patients with NERD must have pH-monitoring prior to surgery.Surgical therapy is as effective as medicaltherapy when performed by competentsurgeons in carefully selected patients34.
ADVERSE EFFECTS OF PPI27. Adverse effects associated with short term use
include headache, diarrhea and dyspepsia,which occur in less than 2% of users and aregenerally mild. Chronic use of PPI has beenlinked to certain complications arising fromnutrient malabsorption and susceptibility toinfections (due to prolonged acid suppression)and drug-drug interaction.
28. Patients with known osteoporosis can remainon PPI except there are other risk factors forhip fracture.
29. PPI therapy may predispose to Clostridiumdifficile infection(35).
30. Community acquired pneumonia is arecognized risk of short-term PPI use, butnot long-term use(36)
31. Concomitant users of clopidogrel do notneed to alter their PPI therapy(37).
Extraesophageal Syndromes32. GERD may be associated with chronic
cough, chronic laryngitis and asthma(4,39,40).However, these associated extraesophagealconditions are often multifactorial.
103
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

33. In the absence of heartburn or regurgitation,unexplained asthma and laryngitis are unlikelyto be related to GERD40-42.
34. A PPI trial is recommended to treatextraesophageal symptoms in patients whoalso have typical symptoms of GERD.
35. Medical and surgical treatment trials aimed atimproving presumed reflux cough, refluxlaryngitis, and reflux asthma syndromes bytreating GERD are associated with uncertainand inconsistent treatment effect.
36. Reflux monitoring should be consideredbefore a PPI trial in patients withextraesophageal symptoms who do not havetypical symptoms of GERD.
Refractory GERDVarious factors affect response to PPI in GERD,including symptom frequency and severity and PPIdosing regime (once or twice daily) and correctnessof diagnosis.Although there is no established consensusregarding the definition of refractory GERD in termsof symptom burden, degree of therapeutic responseand PPI dose at which failure occurs, it is reasonableto accept that refractory GERD is a patient-drivenphenomenon.
37. Patients with GERD are named refractory toPPI when they do not respond to PPI standarddose BID.Potential causes may be gastrointestinal orextra-gastrointestinal. The gastrointestinalcauses may or may not be reflux-related.
The main causes of reflux-related treatment failureinclude:(a.) Acid Reflux: These include incorrect medicationdose timing, medication non-compliance, residualpathological acid secretion, rapid PPI metabolism, ahypersecretory state, a significant anatomic abnormalitylike a large hiatal hernia, excess reflux during tLESRof defective esophageal mucosal barrier function.
(b.) Non Acid Reflux: from stomach or duodenume.g. bile
Reflux of normal amounts of weakly acidic or alkalinecontents into a hypersensitive esophagus
Approach to Patient with Refractory GERD:38. Optimize PPI therapy39. Upper endoscopy if symptoms are typical or
if dyspeptic symptomsalso present40. Assessment of other etiologies if
extraesophageal symptoms are present41. Ambulatory reflux monitoring42. Additional anti-reflux therapy for patients with
objective evidence of on-going reflux egsurgery, TLESR inhibitors like Baclofen.
Gastroesophageal Reflux Disease in PregnancyGastroesophageal reflux disease is common duringpregnancy, affecting as much as 80% of pregnantwomen in some populations43-45. Proposedmechanisms for this observation include reduced loweresophageal sphincter (LES) pressure probably due toincreased progesterone levels, abnormal gastricemptying and delayed small bowel transit43. Thecondition is usually short-lived and resolves afterdelivery and complications are rare43.
43. The preferred and safest initial treatment forGERD during pregnancy is l ifestylemodification through such measures asavoidance of food triggers, elevation of headof bed, avoidance of tight-fitting clothing andchewing gum, avoiding smoking, waiting for2-3 hours after the last meal before lying downand avoiding medications that can aggravatesymptoms.Chewing gum stimulates salivary glands tosecrete saliva which helps to neutralizeacid.Lifestyle modifications may control mildsymptoms, but drug therapy may be necessaryif symptoms are not relieved by thesemeasures.
44. If symptoms fail to abate on lifestylemodifications, calcium and magnesiumantacids are considered safe in pregnancy andmay be prescribed in recommended doses.Antacid use has not been shown to be unsafe,but there have been no controlled studies.46
Despite the limited data, experts have agreedthat antacids should be the f irstpharmacological treatment for heartburnduring pregnancy47. Antacids provide fast andeffective relief, and up to half of women willrequire only antacids to control GERD 43.High doses of aluminum-containing antacids
104
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

Fig. 3: Algorithm
for treatment of G
ERD
105
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

may increase aluminum levels in women andcause fetal harm43,47,48.
45. Acid suppressants (H2-receptor antagonistsand proton pump inhibitors) may be usedafter a careful risk-benefit analysis by thephysician.
Complications of GERDComplications of GERD include erosive esophagitis,stricture and Barrett’s esophagus. Barrett’s esophagusis the only complication of GERD with malignantpotential. It is associated with long duration ofsymptoms, age over 50 years, male sex and Caucasianrace. Barrett’s esophagus appears to be rare in Nigerianpatients.
RECOMMENDED AREAS FOR FURTHERRESEARCH
1. Population-based epidemiological studies ondyspepsia and GERD with emphasis onprevalence, age and gender distribution andclinical course.
2. Well-designed studies to determine the idealcut-off age for early endoscopy in dyspepticpatients.
3. Studies to determine the exact roles of rolesof PDS and EPS as well as the role ofsymptoms other than PDS and EPS indyspepsia and incorporation of such into thedefinition of dyspepsia. This is becausedifferences in culture and language mayengender differences in interpretation ofdyspeptic symptoms.
4. Similarly, heartburn may be influenced by thetype of reporting by the patients because ofsociocultural issues and lack of appropriateterminology in some local languages.
5. Studies to determine the significance of certainendoscopic findings that appear “flimsy” andconsidered insufficient to account forobserved dyspeptic symptoms.
6. Similarly, the significance of minimalesophagitis or esophageal lesions that fall belowLos Angeles Grade A needs to be elucidatedin Nigerian patients.
7. The role of Helicobacter pylori in Nigerianpatients with FD needs further study.
8. The usefulness of PPI in Nigerians with FDneeds to be elucidated.
9. This guideline should be revised on 4-yearlybasis as new knowledge emerges fromresearch.
REFERENCES1. Vakil N, Zanten S V, Kahrilas P, Deut J and
Jones R. Global Consensus Group. TheMontreal definition and classification ofgastroesophageal reflux disease: A GlobalEvidence-Based Consensus. Am J.Gastroenteol 2006; 101: 1900 – 1920.
2. Dent J, El-Serag HB, Wallander MA andJohansson S. Epidemiolog y ofgastroesophageal reflux disease: a systematicreview, Gut 2005,54 (5) ; 710 -717
3. Stanghellini V. Relationship between uppergastrointestinal symptoms and lifestyle,psychological factors and co-morbidity in thegeneral population: resul ts from theDomestic/International Gastroenterologysurveillance study (DIGEST), Scand J.Gastroenteral 1999 suppl, 231: 29 – 37.
4. Locke G 3 rd, Talley NJ, Fett SL et al.Prevalence and clinical spectrum ofgastroesophageal reflux: a population-basedstudy in Olmsted County, Minesota.Gastroenterology 1997; 112: 1448 – 1456.
5. Wong WM, Lai KC, Lam KF et al. Prevalence,clinical spectrum and health care utilization ofgastroesophageal reflux disease in a Chinesepopulation: a population-based study. AlimentPharmacol Ther 2003; 18(16) : 595 – 604.
6. Chen M, Xiong L, Chen H, Xu A, He L andHu P. Prevalence, risk factors, and impact ofgastroesophgeal reflux disease symtoms: apopulation – based study in South China.Scand J Gastroenterol 2005; 40(7): 759 -767.
7. Nwokediuko SC. Gastroesophageal refluxdisease: a population-based study.Gastroenterology Research 2009; 2: 152- 156.
8. Sharma P, Wani S, Romero Y, Johnson D,Hamilton F. Racial and geographic issues ingastroesophageal reflux disease. Am JGastroenterol 2008; 103 (11); 2669 – 2680.
106
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

9. Rosaida MS, Goh KL. Gastroesophagealreflux disease, reflux esophagitis and non-erosive reflux disease in a multi–racial Asianpopulation: a prospective, endoscopy–basedstudy. Eur J. Gastroentrol Hepatol 2004;16(5): 445 - 501
10. Hirakawa K, Adachi K, Amano K et al.Prevalence of non-ulcer dyspepsia in theJapanese population. J. Gastroentrol Hepatol1999; 14 (11): 1083 -1087.
11. Rajendra S, Kutty K and Karim N. Ethicdifferences in the prevalence of endoscopicesophagitis and Barrett’s esophagus; the longand short of it all. Dig Dis Sci 2004; 49(2):237 – 242.
12. El-Serag HB, Graham DY, Satia JA andRabeneck L. Obesity is an independent riskfactor for GERD symptoms and erosiveesophagitis. Am J Gastroenterol 2005; 100(6):1243 – 1250
13. Ayazi S and Crookes P Peyre C. Objectivedocumentation of the link between GERDand obesity. Ann J Gastroenterol 2007; 102;138 – 139.
14. Ayazi S, Hagen JA, Chan LS et al. Obesityand gastroesophageal reflux; quantifying theassociation between body mass index,esophageal acid exposure, and loweresophageal sphincter status in a large series ofpatients with reflux symptoms. J. GastrointestSurg 2009; 13(8): 1440 – 1447
15. Buttar NS and Falk GW. Pathogenesis ofgastroesophageal ref lux and Barrett’sesophagus. Mayo Clinc Proceedings 2001;76(2): 226 – 234.
16. Patti MG, Goldberg HI, Arcerito M, BortolasiL, Tong J and Way W. Hiatal hernia size affectslower esophageal sphincter function,esophageal acid exposure, and the degree ofmucosal injury. Am J Surg 1996; 171(1): 182– 186 .
17. Watanabe Y, Fujiwara, Shiba M et al. Cigarettesmoking and alcohol consumption associatedwith gastroesophageal reflux disease inJapanese men. Scand J. Gastroenterol 2003;38(8): 807 – 811.
18. Patti M G, Gasper WJ, Fisichella PM,Nipomnick I and Palazzo F. Gastroesophagealreflux disease and connective tissue disorders;pathophscology and implications for
treatment. J. Gastrointest Surg 2008; 12(11):1900 – 1906
19. Ruigomez A, Wallander MA, Johansson S andRodriguez LAG. Irritable bowel syndromeand gastroesophageal reflux disease in primarycare: is there a link? Dig Dis Sci 2009; 54(5):1079 1086.
20. El – Serag HB. Time trends ofgastroesophageal reflux disease; a systematicreview Gut 2005; 54(5): 710 – 717
21. Lewis JV. Editoral; Gastroesophageal refluxdisease and obesity. Southern Medical Journal2009; 102(10):995 – 996.
22. Stein HJ and De Meester TR. Outpatientphysiologic testing and surgical managementof foregut motility disorders. CurrentProblems in Surgery 1992; 29(&): 413 – 555
23. Barham CP, Gotley DC, Mills A andAnderson D. Precipitating causes of acidreflux episodes in ambulant patients withgastroesophegeal reflux disease. Gut 1995;36: 505 – 510
24. Thompson ABR, Barkun AN, Armstrong Det al. The prevalence of clinically significantupper gastrointestinal findings in primary carepatients with uninvestigated dyspepsia. TheCanadian adult dyspepsia empiric treatment-prompt endoscopy (CADET – PE) study.Aliment pharmacol Ther 2003; 17; 1481 –1491.
25. Rokkas T and Sladen GE. Ambulatoryesophageal pH recording in gastroesophagealreflux: relevance to the development ofesophagitis. Am J Gastroenterol 1988; 83:629 – 632.
26. Sarawat VA, Dhiman RK, Mishra A et al.Correlation of 24-hr esophageal pH patternswith clinical features and endoscopy ingastroesophageal reflux disease. Dig Dis Sci1994; 39: 199 – 205.
27. Eisen GM, Sandler RS, Murray S, et al. Therelationship between gastroesophageal refluxdisease and its complications with Barrett’sesophagus. AmJ Gastroenterol 1997; 92: 27– 31
28. El – Serag HB and Johansson JF. Risk factorsfor the severity of erosive esophagisits inHelicobacter pylori-negative patients with
107
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD

gastroesophygeal reflux disease. Scand J.Gastroenterol 2002; 39; 899 – 904
29. Avidan B, Sonnenberg A, Schnell TG et al.There are no reliable symptoms for erosiveesophagitis and Barrett’s esophagus:Endoscopic diagnosis is still essential. AlimentPharmacol Ther 2002; 16: 735 -742.
30. Armstrong D, Bennett JR, Blum Al et al. Theendoscopic assessment of esophagitis: aprogress report on observer agreement.Gastroenterology 1996; 111: 85 – 92.
31. Lundell LR, Dent J Bennett JR et al.Endoscopic assessment of esophatitis: clinicaland functional correlates and further validationof the Los Angeles classification. Gut 1999;45: 172 – 180.
32. Pandolfino JE, Vakil NB and Kahrilas PJ.Comparison of inter and intra-observerconsistency for grading of esophagitis byexpert and trainee endoscopists. GastrointestEndosc 2002; 56: 639 – 643.
33. Weijenborg et al. PPI therapy is equallyeffective in well-defined non-erosive refluxdisease and in reflux esophagitis: a meta-analysis. J Neurogastroentrol Motil 2012; 24:747 – e 350.
34. Galmiche JP, Hatlebakk J, Awoods S, Ell C,Fiocca R, Eklund S et al. Laparoscopicantireflux surgery vs Esomeprazole treatmentfor chronic GERD. The Lotus randomizedclinical trial. JAMA 2011; 305 (19): 1969 –1977.
35. Barishi C and Dupont HL. Systematic review:the use of proton pump inhibitors andincreased susceptibility to enteric infection.Aliment Pharmacol Ther 2011; 34: 12 – 1281.
36. Eom CS, Jeon CY, Lim JW et al. Use of acidsuppressive drugs and risk ofpneumonia: asystematic review and meta-analysis. CMAJ2001; 183: 310 – 319.
37. Gerson LB, McMahon D, Olkin I et al. Lackof significant interactions between clopidogreland proton pump inhibitor therapy: meta-analysis of existing literature. Dig Dis Sci 2012;57: 1304 – 1313
38. El-Serag HB and Sonnenberg A. Co-morbidoccurrence of laryngeal or pulmonary diseasewith esophagitis in United States military
veterans. Gastroenterology 1997; 113: 755 –760.
39. Gislason T, Janson C. Vermeire P et al.Respiratory symptoms and nocturnalgastroesophageal reflux: a population basedstudy of young adults in three Europeancountries. Chest 2002; 121: 158 – 163.
40. El-Serag HB, Lee P, Buchner A et al.Lansoprazole treatment of patients withchronic idiopathic laryngitis: a placebo-controlled trial. Am J Gastroenterol 2001;96:979 – 983.
41. Noordzij JP, Khidr A, Evans BA et al.Evaluation of Omeprazole in the treatmentof reflux laryngitis: A prospective, placebo-controlled, randomized double blind study.Laryngoscope 2001; 111: 2147 – 2151.
42. Vaezi MF, Richter JE, Stasney CR et al. Arandomized double-blind placebo-controlledstudy of acid suppression for the treatmentof suspected laryngopharyngeal reflux.Gastroenterology 2004; 126 (Suppl 2): A22.
43. Richter JE. The management of heartburn inpregnancy. Aliment Pharmacol Ther. 2005; 22:749-757.
44. Larson JD, Patatanian E, et al. Double-blind,placebo-controlled study of ranitidine forgastroesophageal reflux symptoms duringpregnancy. Obstet Gynecol. 1997; 90: 83-87.
45. Knudsen A, Lebech M and Hansen M. Uppergastrointestinal symptoms in the third trimesterof the normal pregnancy. Eur J ObstetReprod Biol. 1995; 60: 29-33.
46. Smal lwood RA, et a l. Safety of acid-suppressing drugs. Dig Dis Sci. 1995; 40(Suppl): 63S-80S.
47. Tytgat GN, Heading RC, et al. Contemporaryunderstanding and management of reflux andconstipation in the general population andpregnancy: a consensus meeting. AlimentPharmacol Ther. 2003; 18: 291-301.
48. Weberg R, Berstad A and Ladehaug B. AreAluminum-containing antacids duringpregnancy safe? Acta Pharmacol Toxicol.1986; 59(Suppl 7): 63-65
108
Nigerian Journal of Gastroenterology and Hepatology Vol.7 No. 2 December, 2015
Guidelines for the Management of GERD